Deepak M. Sampathu MD, PhD Assistant Professor of Clinical Radiology University of Pennsylvania
|
|
|
- Morgan Griffin
- 5 years ago
- Views:
Transcription

1 Deepak M. Sampathu MD, PhD Assistant Professor of Clinical Radiology University of Pennsylvania
2 Objectives Recognize benign masses and masslike lesions of the neck and skull base Understand the imaging characteristics of benign masses and mass-like lesions of the neck and skull base on CT and MRI
3 Neck Masses By location: Midline/paramidline anterior neck Floor of mouth Submandibular space at angle of jaw Along lateral cervical nodal chain Posterior neck
4 Midline/paramidline anterior neck Thyroglossal duct cyst Laryngocele Dermoid/epidermoid cyst Venolymphatic malformation
5 Thyroglossal duct cyst Most common congenital neck mass Child / young adult Location Suprahyoid 20% At level of hyoid or infrahyoid 80% Painless fluctuant mass Risk of thyroid carcinoma Sistrunk procedure (Harnsberger, Handbook of Head and Neck Imaging, 1995)


6 Thyroglossal duct cyst

7 Thyroglossal duct cyst



8 Papillary carcinoma in TGDC


9 Epidermoid

10 Laryngocele Adulthood Enlarged laryngeal saccule Laryngeal saccule blind pouch arising from laryngeal ventricle Types: Internal External Mixed Laryngoscopy is critical (Harnsberger, Handbook of Head and Neck Imaging, 1995)

11 Laryngocele

12 Laryngocele
13 Floor of Mouth Ranula/Sialocele Abscess, Ludwig s angina Dermoid/ Epidermoid cyst Lymphatic malformation
14 Floor of Mouth Lesions (Vogl et al, AJR 1993)
15 Ranula Peak prevalance age years Pseudocyst in floor of mouth Submandibular duct obstruction Types Simple Plunging/Diving DDx: Sialocele - Ruptured SMD extravasates saliva into sublingual space


16 Simple ranula


17 Plunging Ranula

18 Plunging Ranula
19 Floor of Mouth Infection Clinical findings get history! Imaging findings dirty fat Thickening of platysma/skin Abscess: peripherally-enhancing collection Most common etiology: odontogenic Ludwig s angina: 5% fatality rate Mixed bacterial infection: aerobes/anaerobes Potential airway compromise


20 Infection - Ludwig angina



21 Dermoid
22 Dermoid/Epidermoid cyst Usually present at age Terminology Epidermoid: squamous epithelial lining Dermoid: squamous epithelial lining + skin appendages (sebaceous glands, hair follicles) [Teratoma: true neoplasm with tissue of one or more germ layers] Etiology: Trapped pouches of ectoderm or failure of ectoderm to separate from neural tube Dermoid: 5% malignant degeneration to SCCa
23 Dermoid/Epidermoid cyst Imaging characteristics Epidermoid CT: fluid attenuation MRI: hyper on T2, hypo on T1 Restricted diffusion Dermoid More variable on CT/MR Restricted diffusion

24 Dermoid/epidermoid


25 Presumed epidermoid
26 Lymphatic malformation lymphangioma, cystic hygroma ~50% present at birth or before age 5, do not spontaneously regress Slow-flow vascular malformation containing embryonic lymphatic sacs Can occur in any H&N space transspatial mass with fluid-fluid levels Venolymphatic malformation: venous and lymphatic elements in same mass


27 Lymphatic malformation


28 Lymphatic malformation
29 Submandibular space at angle of jaw 2 nd Branchial cleft cyst (DDx - Cystic/necrotic level IIA lymphadenopathy ) Plunging ranula/sialocele Abscess/Ludwig s angina Lymphatic malformation
30 Cystic/necrotic lymphadenopathy Infectious etiologies Mycobacterial Bacterial Neoplastic etiologies Squamous cell carcinoma Papillary thyroid carcinoma (lymphoma rarely cystic-appearing)
31 2 nd branchial cleft cyst Most common branchial apparatus anomaly Typically present at age subtypes based on location Classic is type 2: Posterior to submandibular gland Anteromedial to sternocleidomastoid muscle Lateral to carotid sheath

32 Branchial Apparatus (Ibrahim et al. Neurimag Clin N Amer 2012)

33 2 nd branchial cleft cyst

34 2 nd branchial cleft cyst

35 Lymphadenopathy R tonsillar SCCa

36 Metastatic lymphadenopathy from oropharyngeal SCCa

37 2 nd branchial cleft cyst
38 Cystic lesion at level 2A in adult Consider cancer until proven otherwise Increasing incidence of HPV-related squamous cell cancer in adults < age 40 Male>female, nonsmokers Occur in oropharynx Propensity for cystic adenopathy Primary tumor may be small FNA for workup (avoid open biopsy) If FNA inconclusive, some advocate for blind oropharyngeal biopsies/pet in workup
39 Along cervical nodal chain Suppurative or cystic/necrotic lymphadenopathy 2 nd /3 rd Branchial cleft cyst Paraganglioma Schwannoma


40 Suppurative Lymphadenitis
41 Carotid body paraganglioma Benign neuroendocrine neoplasm arising in paraganglionic tissue Slowly growing, painless, pulsatile mass Vascular mass splaying ICA and ECA salt and pepper appearance in larger tumors on T1WI: Salt = areas of high signal intensity Pepper = flow voids Intense rapid enhancement


42 Paragangliomas

43 Carotid body paraganglioma
44 Multiple paragangliomas Multiple gene mutations identified in familial and sporadic types SDH: succinate dehydrogenase gene RET protoongogene: multiple endocrine neoplasia (MEN) syndromes VHL gene: von Hippel-Lindau syndrome
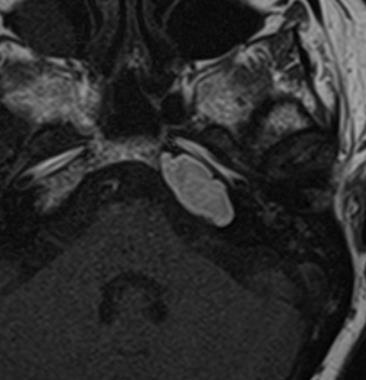
45 Carotid space schwannoma Benign tumor of Schwann cells that wrap around a nerve Clinical presentation: Typical: asymptomatic palpable mass if large, may cause dysphagia or occlusion of IJV Horner syndrome Hoarseness (vocal cord paralysis Imaging: lack of flow voids Dense uniform enhancement +/- intratumoral cysts



46 Schwannoma
47 Parotid space 1 st Branchial cleft cyst Parotid lymphoepithelial cyst/sialocele/sialectasis Lymphoepithelial lesions (bilateral and multiple, HIV or Sjogren) Warthin s tumor (bilateral parotid tails)
48 1 st branchial cleft cyst 1 st branchial arch extends from EAC, through parotid gland, to submandibular space Locations Adjacent to external auditory canal Intraparotid/periparotid CT/MR cannot differentiate from cystic parotid mass


49 1 st Branchial Cleft Cyst



50 Infected 1 st BCC
51 Benign Lymphoepithelial lesions in HIV Intraparotid May be: Cystic Mixed cystic/solid Solid (lymphadenopathy) DDx: Sjogren s Warthin s tumors


52 Lymphoepithelial Lesions
53 Posterior cervical space Cystic hygroma (very large lymphatic malformation presents at < 2-year-old) Lymphatic malformation (smaller lymphatic malformation presents at any age) Level 5 Cystic/necrotic lymphadenopathy 3 rd Branchial cleft cyst (posterior to the carotid, rare)

54 Lymphatic malformation




55 Lymphatic malformation

56 Infectious lymphadenopathy - bacterial
57 Skull Base Benign masses Anterior skull base Central skull base Posterior skull base (jugular foramen)
58 Anterior Skull Base Fibrous Dysplasia Cephalocele Meningioma
59 Fibrous Dysplasia Benign fibro-osseous lesion in which normal bone is replaced by weak osseous & fibrous tissue Classic appearance groundglass density on CT Variable enhancment of fibrous component



60 Fibrous Dysplasia

61 Fibrous Dysplasia
62 Cephalocele Cephalocele: general term for protrusion of intracranial contents through defect in calvarium or skull base Meningoencephalocele/encephalocele: Brain tissue, meninges, and CSF Meningocele: Meninges and CSF only CT: delineation of osseous defect MR: heterogeneous appearance reflecting brain tissue and CSF contents


63 Ethmoid meningoencephalocele
64 Meningioma Most common extra-axial intracranial neoplasm Typical meningioma WHO grade 1 (~70%) Atypical meningioma WHO grade 2 (~30%) Malignant meningioma WHO grade 3 (~1%) Well-circumscribed extra-axial mass with dural attachment Majority enhance homogeneously and intensely Necrosis, cysts, hemorrhage (8-23%) Calcifications (20-25%)




65 Meningioma
66 Central Skull Base Meningioma Pituitary Macroadenoma Chordoma Benign Fibrofatty lesion (arrested pneumatization) Cholesterol granuloma




67 Meningioma



68 Meningioma
69 Pituitary Macroadenoma Sellar mass without separate identifiable pituitary gland Most common suprasellar mass in adults superior extension of macroadenoma +/- mass effect on optic chiasm +/- cavernous sinus invasion Usually isointense with gray matter Most enhance heterogeneously


70 Pituitary Macroadenoma


71 Pituitary Macroadenoma
72 Chordoma Arises primitive notochord remnant Rare, locally aggressive Considered low-grade malignancy Local recurrence is common despite combined surgical and radiation therapy Imaging: destructive midline mass which is hyperintense on T2WI


73 Clival Chordoma




74 Clival chordoma
75 Cholesterol Granuloma Expansile lesion in petrous apex consisting of fibrosis and vascular proliferation Giant cell reaction to deposition of cholesterol crystals in air cells CT: sharply marginated, expansile lesion MR: high signal intensity on T1WI, no internal enhancement

76 Cholesterol Granuloma
77 Benign fibro-fatty lesion of sphenoid Synonym: arrested pneumatization of sphenoid Common incidental finding on imaging leave me alone lesion Nonexpansile lesion in sphenoid bone with sclerotic margins Internal fat attenuation is invariably present


78 Benign fibro-fatty lesion of sphenoid


79 Encephalocele in sphenoid siunus
80 Posterior Skull Base Lesions of jugular foramen: Paraganglioma Schwannoma Meningioma
81 Glomus jugulare paraganglioma Benign tumor arising from neural crest cells in/around jugular foramen CT: permeative bone destruction around jugular foramen MR: vascular mass




82 Glomus jugulare paraganglioma In-111 Octreoscan


83 Glomus jugulare paraganglioma
84 Jugular foramen schwannoma Benign neoplasm of differentiated Schwann cells around cranial nerve 9, 10, or 11 in jugular foramen CT: well marginated, expanded jugular foramen without permeative destruction MR: tubular or dumbell-shaped mass; no flow-voids Homogeneously enhancing except for cystic areas in larger lesions




85 Jugular foramen schwannoma



86 Jugular foramen schwannoma
87 Jugular foramen meningioma Mass arising from arachnoid meningothelial cap cells along cranial nerves 9-11 in jugular foramen CT: permeative/sclerotic margins MR: enhancing mass with dural tail(s), no flow voids


88 Jugular foramen menngioma
89 Objectives Recognize benign masses and masslike lesions of the neck and skull base Understand the imaging characteristics of benign masses and mass-like lesions of the neck and skull base on CT and MRI
90 Thanks
Cystic Head and Neck Lesions
 Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
 PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses CASE 1 Case 1 A 2
Case Studies in the Skull Base
 Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji
 Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
Congenital Neck Masses C. Stefan Kénel-Pierre, MD
 Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
PITUITARY PARASELLAR LESIONS. Kim Learned, MD
 PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
DISCLOSURES LEARNING OBJECTIVES WE WILL NOT DISCUSS. CSB: Birdseye View MESSAGE NAVIGATING THE SELLA AND CENTRAL SKULL BASE
 NAVIGATING THE SELLA AND CENTRAL SKULL BASE Christopher P. Hess, M.D., Ph.D. DISCLOSURES Research Support, General Electric SLIDES: http://www.radiology.ucsf.edu/research/meetings/rsna LEARNING OBJECTIVES
NAVIGATING THE SELLA AND CENTRAL SKULL BASE Christopher P. Hess, M.D., Ph.D. DISCLOSURES Research Support, General Electric SLIDES: http://www.radiology.ucsf.edu/research/meetings/rsna LEARNING OBJECTIVES
Neck lumps in children
 Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Imaging of Petrous Apex: Anatomy and Pathology
 University of Utah Head and Neck Conference 2018 Petrous apex Imaging of Petrous Apex: Anatomy and Pathology Philip Chapman MD University of Alabama, Birmingham Good News PAs tend to be symmetric A quick
University of Utah Head and Neck Conference 2018 Petrous apex Imaging of Petrous Apex: Anatomy and Pathology Philip Chapman MD University of Alabama, Birmingham Good News PAs tend to be symmetric A quick
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
SKULL BASE LESIONS THAT MAY MIMICK DISEASE
 SKULL BASE LESIONS THAT MAY MIMICK DISEASE AUTHORS: MYERS, TANDBERG, LORENZO UNIVERSITY OF NEW MEXICO DIAGNOSTIC RADIOLOGY Learning Objectives The participant will identify normal anatomic variants that
SKULL BASE LESIONS THAT MAY MIMICK DISEASE AUTHORS: MYERS, TANDBERG, LORENZO UNIVERSITY OF NEW MEXICO DIAGNOSTIC RADIOLOGY Learning Objectives The participant will identify normal anatomic variants that
INFECTION. HIV Infection DWI
 HIV Infection INFECTION DWI Fig Axial CT and MRI images show multiple enlarged lymph nodes in the neck as well as in the parotid gland bilaterally. These nodes were suppurative with positive diffusion.
HIV Infection INFECTION DWI Fig Axial CT and MRI images show multiple enlarged lymph nodes in the neck as well as in the parotid gland bilaterally. These nodes were suppurative with positive diffusion.
Neck mass Evaluation & Management OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY
 Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
RADIOLOGY TEACHING CONFERENCE
 RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
RADIOLOGY TEACHING CONFERENCE John Athas, MD Monica Tadros, MD Columbia University, College of Physicians & Surgeons Department of Otolaryngology- Head & Neck Surgery September 27, 2007 CT SCAN IMAGING
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Ultrasound Interpretation of Non-Thyroid Neck Pathology
 Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
HEAD & NECK SWELLINGS
 HEAD & NECK SWELLINGS EXCLUDING GOITRE FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS-HPE; PGDIP-BIOETHICS PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y MIDLINE SWELLINGS NECK SWELLINGS
HEAD & NECK SWELLINGS EXCLUDING GOITRE FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS-HPE; PGDIP-BIOETHICS PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y MIDLINE SWELLINGS NECK SWELLINGS
Imaging of Hearing Loss
 Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Cross sectional imaging of Intracranial cystic lesions Abdel Razek A
 Cross sectional imaging of Intracranial cystic lesions Abdel Razek A Department of Radiology. Mansoura Faculty of Medicine, Mansoura. Egypt. arazek@mans.edu.eg Introduction Intracranial cystic lesions
Cross sectional imaging of Intracranial cystic lesions Abdel Razek A Department of Radiology. Mansoura Faculty of Medicine, Mansoura. Egypt. arazek@mans.edu.eg Introduction Intracranial cystic lesions
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Endoscopic Assisted resection for congenital Midline Nasal Mass
 Endoscopic Assisted resection for congenital Midline Nasal Mass Ahmed Aly Ibrahim A.prof ORL Department Alexandria University Emad. A Magdy prof ORL Department Alexandria University Haytham Morsi,MD Mohammad
Endoscopic Assisted resection for congenital Midline Nasal Mass Ahmed Aly Ibrahim A.prof ORL Department Alexandria University Emad. A Magdy prof ORL Department Alexandria University Haytham Morsi,MD Mohammad
Case Studies in Sella/Parasellar Region. Child thirsty, increased urination. Imaging. Suprasellar Germ Cell Tumor (Germinoma) No Disclosures
 No Disclosures") Case Studies in Sella/Parasellar Region No Disclosures 2018 Head and Neck Imaging Conference Child thirsty, increased urination Suprasellar Germ Cell Tumor (Germinoma) Midline Pineal >> Suprasellar > Other
Case Studies in Sella/Parasellar Region No Disclosures 2018 Head and Neck Imaging Conference Child thirsty, increased urination Suprasellar Germ Cell Tumor (Germinoma) Midline Pineal >> Suprasellar > Other
Metastasis. 57 year old with progressive Headache and Right Sided Visual Loss
 Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Evaluation of Head and Neck Masses in Adults
 Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Radiologic Evaluation of Petrous Apex Masses. Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009
 Radiologic Evaluation of Petrous Apex Masses Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009 Roadmap Petrous Apex Anatomy Patient D.S.: Clinical Presentation Differential diagnosis of
Radiologic Evaluation of Petrous Apex Masses Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009 Roadmap Petrous Apex Anatomy Patient D.S.: Clinical Presentation Differential diagnosis of
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS. By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN
 LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN I. Objectives II. By the end of this presentation, the learner will be able
LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN I. Objectives II. By the end of this presentation, the learner will be able
Salivary ultrasound. Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK
 Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Salivary Gland Imaging. Mary Scanlon MD FACR October 2016
 Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Clinical evaluation. Imaging Surgical treatment
 Parapharyngeal Space Khalid adhussain AL-Qahtani a MD,MSc,FRCS(c) Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular Reconstruction, ti and
Parapharyngeal Space Khalid adhussain AL-Qahtani a MD,MSc,FRCS(c) Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular Reconstruction, ti and
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck
 "The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
"The Space Between Us:" A Radiographic Review of Common and Uncommon Pathologic Findings within the Deep Spaces of the Neck Poster No.: C-2457 Congress: ECR 2015 Type: Educational Exhibit Authors: A. K.
SALIVARY GLAND DISEASES. Omar alnoubani MD,MRCS
 SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
"Mummy what's this on my neck? - A pictorial review of paediatric neck masses"
 "Mummy what's this on my neck? - A pictorial review of paediatric neck masses" Poster No.: C-0405 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Farrugia, A. S. Gatt; Msida/MT Keywords: Education,
"Mummy what's this on my neck? - A pictorial review of paediatric neck masses" Poster No.: C-0405 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Farrugia, A. S. Gatt; Msida/MT Keywords: Education,
Advances In Orbital Neuropathology
 Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
Glomus Glomus tympanicum tumor 52. Mondini Mondini malformation 64
 5 2 2 A Key to Head and Neck Imaging 3 4 6 3 9 1 16 ossicular malformation 30 aberrant internal carotid artery, partial absence of internal carotid artery 34 jugular bulb variants 36 Bezold S acute otitis
5 2 2 A Key to Head and Neck Imaging 3 4 6 3 9 1 16 ossicular malformation 30 aberrant internal carotid artery, partial absence of internal carotid artery 34 jugular bulb variants 36 Bezold S acute otitis
MDCT and Ultrasound Evaluation of Primary Masses of Neck with Pathological Correlation
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. IX (September). 2016), PP 63-71 www.iosrjournals.org MDCT and Ultrasound Evaluation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. IX (September). 2016), PP 63-71 www.iosrjournals.org MDCT and Ultrasound Evaluation
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
The many faces of extranodal lymphoma
 The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
Posterior fossa tumors: clues to differential diagnosis with case-based review
 Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
1. What is the embryologic origin of the major salivary glands, and when do they develop? 2. What is the embryologic origin of minor salivary glands?
 Salivary Gland Chapters 37, 38, 39, 40 Shapiro 1. What is the embryologic origin of the major salivary glands, and when do they develop? Outpouchings of oral ectoderm in the 6th 8 th week 2. What is the
Salivary Gland Chapters 37, 38, 39, 40 Shapiro 1. What is the embryologic origin of the major salivary glands, and when do they develop? Outpouchings of oral ectoderm in the 6th 8 th week 2. What is the
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
THYROID & PARATHYROID. By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy
 THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Zubair W. Baloch, MD, PhD: Consultant for Veracyyte, INC Tarik M. Elsheikh, MD: Nothing to disclose
 Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
Cytology Works shop #8 Zubair W. Baloch, MD, PhD: Consultantt for Veracyte, INC Tarik M. Elsheik kh, MD: Nothing to disclose Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair
Imaging Work-Up of a Neck Mass - Adults & Children
 Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Thyroid gland. importance. relations and connections. external laryngeal nerves. malformations.
 Thyroid gland 1. Recognize and understand the coverings of the thyroid gland and their clinical importance. 2. Recognize and understand the main parts of the thyroid gland and their locations, relations
Thyroid gland 1. Recognize and understand the coverings of the thyroid gland and their clinical importance. 2. Recognize and understand the main parts of the thyroid gland and their locations, relations
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
C. Douglas Phillips MD FACR Director of Head and Neck Imaging Weill Cornell Medical College/NewYork-Presbyterian Hospital
 C. Douglas Phillips MD FACR Director of Head and Neck Imaging Weill Cornell Medical College/NewYork-Presbyterian Hospital Disclosures Neither I nor any family members have any pertinent financial relations
C. Douglas Phillips MD FACR Director of Head and Neck Imaging Weill Cornell Medical College/NewYork-Presbyterian Hospital Disclosures Neither I nor any family members have any pertinent financial relations
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
Where Has My Vision Gone? Evaluation of Sellar Lesions. Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008
 Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions
 CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
Index ... Moedder et al., Direct Diagnosis in Radiology. Head and Neck Imaging (ISBN ), 2008 Georg Thieme Verlag KG
, 2008 Georg Thieme Verlag KG") A abscess vs. branchial cleft cyst 204 cervical 214 216 vs. cervical hematoma 207 cervical prevertebral 138 140 epidural, intraoral 159 161 paralaryngeal, vs. laryngeal edema 134 parapharyngeal 115 117
A abscess vs. branchial cleft cyst 204 cervical 214 216 vs. cervical hematoma 207 cervical prevertebral 138 140 epidural, intraoral 159 161 paralaryngeal, vs. laryngeal edema 134 parapharyngeal 115 117
Pediatric Spine Tumors (and other masses)
") Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Head and Neck Image 頭頸部放射影像學
 Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
Head and Neck Image 頭頸部放射影像學 陳家媛 台北醫學大學 - 市立萬芳醫院 cychen@wanfang.gov.tw Normal Suprahyoid neck: the old way Nasopharynx Oropharynx Oral cavity Staging of SCC Spaces of Suprahyoid Neck: a New Way Deep
STATE OF THE ART MANAGEMENT of PARAGANGLIOMA. IFOS, Lima, 2018
 STATE OF THE ART MANAGEMENT of PARAGANGLIOMA IFOS, Lima, 2018 VINCENT C COUSINS ENT-Otoneurology Unit, The Alfred Hospital & Department of Surgery, Monash University MELBOURNE, AUSTRALIA PARAGANGLIOMAS
STATE OF THE ART MANAGEMENT of PARAGANGLIOMA IFOS, Lima, 2018 VINCENT C COUSINS ENT-Otoneurology Unit, The Alfred Hospital & Department of Surgery, Monash University MELBOURNE, AUSTRALIA PARAGANGLIOMAS
Traditional Approach. Pathways for Skull Base Pathology. Special Pathways Approach. 1. Traditional Approach. Central Skull Base. Anterior Skull Base
 Traditional Approach Pathways for Skull Base Pathology Anatomy Local Pathology Wade Wong DO FACR Professor of Radiology University of California, San Diego Special Pathways Approach Perineural Perivascular
Traditional Approach Pathways for Skull Base Pathology Anatomy Local Pathology Wade Wong DO FACR Professor of Radiology University of California, San Diego Special Pathways Approach Perineural Perivascular
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Evaluation and Management of Pediatric Neck masses
 Evaluation and Management of Pediatric Neck masses Steven T. Wright, M.D. Faculty Advisor: Ronald Deskin, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Evaluation and Management of Pediatric Neck masses Steven T. Wright, M.D. Faculty Advisor: Ronald Deskin, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Case Presentation. x year old African American male seen in Pediatric Surgery Clinic. History: NKDA
 Case Presentation ALIREZA SADEGHI MD Kings County Hospital Center University Hospital of Brooklyn Downstate Medical Center Division of Pediatric Surgery July 7 th 2006 Case Presentation x year old African
Case Presentation ALIREZA SADEGHI MD Kings County Hospital Center University Hospital of Brooklyn Downstate Medical Center Division of Pediatric Surgery July 7 th 2006 Case Presentation x year old African
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Spinal Neoplasms. First Things First!! Localize the Lesion!! Ependymomas. Common Intramedullary Lesions
 Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
Suprahyoid and Infrahyoid Neck Overview
 10 Imaging Approaches & Indications Neither CT nor MR is a perfect modality for imaging the extracranial H&N. MR is most useful in the suprahyoid neck (SHN) because it is less affected by oral cavity dental
10 Imaging Approaches & Indications Neither CT nor MR is a perfect modality for imaging the extracranial H&N. MR is most useful in the suprahyoid neck (SHN) because it is less affected by oral cavity dental
The Temporal Bone Anatomy & Pathology
 Department of Radiology University of California San Diego The Temporal Bone Anatomy & Pathology John R. Hesselink, M.D. Temporal Bone Axial View Temporal Bone Coronal View Longitudinal Fracture The Temporal
Department of Radiology University of California San Diego The Temporal Bone Anatomy & Pathology John R. Hesselink, M.D. Temporal Bone Axial View Temporal Bone Coronal View Longitudinal Fracture The Temporal
A CASE OF A Huge Submandibular Pleomorphic Adenoma
 ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 4 Number 2 S VERMA Citation S VERMA.. The Internet Journal of Head and Neck Surgery. 2009 Volume 4 Number 2. Abstract Pleomorphic adenoma
ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 4 Number 2 S VERMA Citation S VERMA.. The Internet Journal of Head and Neck Surgery. 2009 Volume 4 Number 2. Abstract Pleomorphic adenoma
Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis
 Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis Schwannomas (also called neurinomas or neurilemmomas) constitute the most common primary cranial nerve tumors. They are benign slow-growing
Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis Schwannomas (also called neurinomas or neurilemmomas) constitute the most common primary cranial nerve tumors. They are benign slow-growing
Role of imaging in RCC. Ultrasonography. Solid lesion. Cystic RCC. Solid RCC 31/08/60. From Diagnosis to Treatment: the Radiologist Perspective
 Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Workshop 2. Controversies and Diagnostic Challenges in Head and Neck Cytopathology. Zubair Baloch, MD,PhD. Veracyte, Inc: Consultant
 Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Workshop 2 Controversies and Diagnostic Challenges in Head and Neck Cytopathology Zubair Baloch, MD,PhD Veracyte, Inc: Consultant Tarik Elsheikh, MD There are no disclosures necessary. Controversies and
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass
 Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass Poster No.: C-1390 Congress: ECR 2015 Type: Educational Exhibit Authors: I. Candelaria, C. Figueira,
Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass Poster No.: C-1390 Congress: ECR 2015 Type: Educational Exhibit Authors: I. Candelaria, C. Figueira,
TABLES. Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class
 Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class") TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
Imaging the Spinal Cord & Intradural Disease
 Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Ectopic salivary tissue of the tonsil: a case report
 International Journal of Pediatric Otorhinolaryngology (2005) 69, 567 571 www.elsevier.com/locate/ijporl CASE REPORT Ectopic salivary tissue of the tonsil: a case report Jeffrey B. Wise a,b, Kriti Sehgal
International Journal of Pediatric Otorhinolaryngology (2005) 69, 567 571 www.elsevier.com/locate/ijporl CASE REPORT Ectopic salivary tissue of the tonsil: a case report Jeffrey B. Wise a,b, Kriti Sehgal
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Imaging Of Cystic Paravertebral Masses:
 Imaging Of Cystic Paravertebral Masses: Differential Diagnosis and Key Discriminators John P. Lichtenberger III, MD, Maj, USAF, MC Brent McCarragher, MD, CPT, USA John R. Dryden, MD, LT, USN P. Gabriel
Imaging Of Cystic Paravertebral Masses: Differential Diagnosis and Key Discriminators John P. Lichtenberger III, MD, Maj, USAF, MC Brent McCarragher, MD, CPT, USA John R. Dryden, MD, LT, USN P. Gabriel
Case Studies in CPA/IAC
 Outline Case Studies in CPA/IAC Atul K Mallik MD PhD Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA Case based review of cerebellopontine
Outline Case Studies in CPA/IAC Atul K Mallik MD PhD Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA Case based review of cerebellopontine
Cholesteatoma and Non-cholesteatomatous Inflammatory Disease. Cholesteatoma. Disclosures. Overview EAC. Cholesteatoma. None
 Disclosures Cholesteatoma and Non-cholesteatomatous Inflammatory Disease None Amy F Juliano, MD Staff Radiologist, Massachusetts Eye and Ear Infirmary Assistant Professor of Radiology, Harvard Medical
Disclosures Cholesteatoma and Non-cholesteatomatous Inflammatory Disease None Amy F Juliano, MD Staff Radiologist, Massachusetts Eye and Ear Infirmary Assistant Professor of Radiology, Harvard Medical
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Thyroglossal cyst our experience
 Volume 3 Issue 1 2013 ISSN: 2250-0359 Thyroglossal cyst our experience Balasubramanian Thiagarajan 1 Ulaganathan Venkatesan 2 Geetha Ramamoorthy 1 1 Stanley Medical College 2 Meenakshi Medical College
Volume 3 Issue 1 2013 ISSN: 2250-0359 Thyroglossal cyst our experience Balasubramanian Thiagarajan 1 Ulaganathan Venkatesan 2 Geetha Ramamoorthy 1 1 Stanley Medical College 2 Meenakshi Medical College
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
EXPERT DIFFERENTIAL DIAGNOSIS:
 EXPERT DIFFERENTIAL DIAGNOSIS: Sellar Region Anne G. Osborn, M.D. DISCLOSURE: Published RSNA 2008 SELLA, PITUITARY: Normal Gross, 3T Anatomy SELLA, PITUITARY: Anatomically-Based Differential Diagnoses
EXPERT DIFFERENTIAL DIAGNOSIS: Sellar Region Anne G. Osborn, M.D. DISCLOSURE: Published RSNA 2008 SELLA, PITUITARY: Normal Gross, 3T Anatomy SELLA, PITUITARY: Anatomically-Based Differential Diagnoses
Pediatric Spinal Anomalies
 Department of Radiology University of California San Diego Pediatric Spinal Anomalies John R. Hesselink, M.D. Spine Embryogenesis 1. Primitive streak 2. Proliferation of cells at primitive pit (Hensen's
Department of Radiology University of California San Diego Pediatric Spinal Anomalies John R. Hesselink, M.D. Spine Embryogenesis 1. Primitive streak 2. Proliferation of cells at primitive pit (Hensen's
IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT
 IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT Ramneet Wadi 1, Anil Kumar Shukla 2, Seetha Pramila V. V 3, Sabyasachi Basu 4, Sonam Sanjay 5 1Postgraduate Student, Department of Radiodiagnosis,
IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT Ramneet Wadi 1, Anil Kumar Shukla 2, Seetha Pramila V. V 3, Sabyasachi Basu 4, Sonam Sanjay 5 1Postgraduate Student, Department of Radiodiagnosis,
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Imaging: When to get MRI, CT or PET-CT?
 Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
04 Development of the Face and Neck. Development of the Face Development of the neck
 04 Development of the Face and Neck Development of the Face Development of the neck Development of the face Overview of facial development The fourth week ~ the twelfth week of prenatal development Between
04 Development of the Face and Neck Development of the Face Development of the neck Development of the face Overview of facial development The fourth week ~ the twelfth week of prenatal development Between
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Paraganglioma of the Skull Base. Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI
 Paraganglioma of the Skull Base Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI Case Presentation 63-year-old female presents with right-sided progressive conductive hearing loss for several
Paraganglioma of the Skull Base Ross Zeitlin, MD Medical College of Wisconsin Milwaukee, WI Case Presentation 63-year-old female presents with right-sided progressive conductive hearing loss for several
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Branchial Cleft and Pouch Anomalies
 Branchial Cleft and Pouch Anomalies Prof.Mohamed Hesham Alexandria Faculty of Medicine Alexandria, Egypt Emberyological Basis Branchial Clefts 1st 2nd Pinna EAC 3rd 4th 4th 6th Cervical sinus Branchial
Branchial Cleft and Pouch Anomalies Prof.Mohamed Hesham Alexandria Faculty of Medicine Alexandria, Egypt Emberyological Basis Branchial Clefts 1st 2nd Pinna EAC 3rd 4th 4th 6th Cervical sinus Branchial