Special Course Cytomorphology II : FNA Cytology
|
|
|
- Abraham Hill
- 6 years ago
- Views:
Transcription
1 Special Course Cytomorphology II : FNA Cytology Thyroid Richard M. DeMay, MD Lung Kristen A. Atkins, MD Salivary Glands William C. Faquin, MD, PhD Pancreas Gregg A. Staerkel, MD Disclosure information The speakers have no relationship that represents a possible conflict of interest with respect to the content of this presentation.
2 *-Thyroid Richard M. DeMay, MD Professor of Pathology Director of Cytopathology University of Chicago Objectives: *Learn diagnostic criteria for non-neoplastic lesions of the thyroid *Learn diagnostic criteria for follicular lesions of the thyroid *Learn diagnostic criteria for major forms of thyroid cancer Thyroid Cytology Made Easy There are only a few common, diagnostic categories in fine needle aspiration biopsy of the thyroid. These are: Granulomatous thyroiditis, a post-viral syndrome characterized by giant cells munching on colloid. If you see epithelioid giant cells, rule-out papillary carcinoma. Hashimoto thyroiditis, a classic autoimmune disease characterized by lymphocytes and oncocytes (Hürthle cells). 4 clues to chronic inflammation: lymphoid tangles, plasma cells, infiltration of lymphoid cells into groups of epithelial cells, and lymphoglandular bodies. Papillary carcinoma, characterized by papillary architecture, nuclear grooves and inclusions, and squamoid cytoplasm. Other clues: epithelioid giant cells, psammoma bodies, gummy colloid. Medullary carcinoma, a carcinoid tumor with amyloid stroma associated with calcitonin. The tumor cells are lymphoplasmacytoid or spindle shaped, with salt & pepper chromatin, fine metachromatic granules, and calcitonin expression. When it looks like a neoplasm, but you don t know what, consider medullary carcinoma. Anaplastic carcinoma, characterized by ugly giant and spindle, or epithelioid, tumor cells. When ugly tumor cells are present, exclude metastasis. Follicular Lesions The basic clues to diagnosis of follicular lesions are: the more colloid that is present in the sample, the more likely the lesion is benign and the more cells that are present, the more likely that the lesion is neoplastic. Using these two simple, low power observations, aspirates of follicular lesions can be divided into three categories or zones. Zone I, a colloid nodule (or benign thyroid nodule) is dominated by colloid, and cells are scant. At the other end of the spectrum, Zone III, a follicular nodule (or suspicious for follicular neoplasm) is dominated by cells and colloid is scant. Zone II, a cellular nodule (or follicular lesion of undetermined significance) falls in between. This categorization roughly separates goiters (mostly zone I, colloid nodules) from neoplasms (mostly zone III, follicular nodules).
 are nonneoplastic (ie, hyperplastic nodules in goiters or thyroiditis) and of the malignancies, up to 68% are papillary")


 epithelium usually correlates with goiter, rather than neoplasm.")
3 DeMay: Follicular Thyroid Lesions Colloid nodules have a very low risk of malignancy (<3%). Follicular nodules have a significant risk of malignancy (15%-30%). Note that a substantial number of follicular nodules (up to 35%) are nonneoplastic (ie, hyperplastic nodules in goiters or thyroiditis) and of the malignancies, up to 68% are papillary carcinomas, not follicular carcinomas. Next, an attempt is made to refine the distinction between goiters and neoplasms. Nodules in goiters are formed by degeneration and regeneration. Therefore, signs of these processes are practically part of the definition of the disease, nodular goiter. Cytologically, evidence of hemorrhage, fibrosis, cystic degeneration, stromal calcification, repair, cellular pleomorphism and types of cells, together with a wide range in follicular size, usually characterize nodules of goiters. Also, the cells tend to form uniform, honeycomb sheets. In contrast, neoplasms tend to form microfollicles. The nuclei tend to be uniform, though they may be enlarged. Nucleoli are infrequent. Atypical (but not frankly malignant-appearing) epithelium usually correlates with goiter, rather than neoplasm. Clues to follicular carcinoma include marked architectural abnormalities, such as crowded, irregular microfollicles and increased single cells, and marked cytologic atypia, such as nuclear enlargement and pleomorphism, abnormal chromatin, prominent or multiple nucleoli, atypical mitotic figures, and necrosis. 2
4 DeMay: Follicular Thyroid Lesions There are two forms of follicular carcinoma: a minimally invasive, minimally atypical, and minimally malignant form and a frankly invasive, frankly atypical, and frankly malignant form. The first type is difficult to recognize cytologically, but the second type is unlikely to be missed cytologically. The final step in evaluation of follicular lesions is to take a close look at the nuclei. Nuclear grooves, when extensive, or even a single bona fide intranuclear inclusion strongly suggests papillary carcinoma. A helpful sign is that follicular nuclei, even in neoplasms, tend to be round and smooth, like oranges. Papillary nuclei tend to be irregular, more like potatoes. The classic teaching is that follicular carcinoma comprises 15% to 20% of all thyroid malignancies and that zone III biopsies usually (80% to 90%) correlated with neoplasms, 20% to 30% of which were malignant. However, more recently, follicular carcinoma has apparently become rare (owing both to changes in definition and a true reduction related to adding iodized salt to the diet). Therefore, today, zone III biopsies are much less likely to be neoplastic, and <5% are malignant, assuming papillary carcinoma has been carefully excluded! Advanced Topics Hürthle cell lesions represent a mixed bag of entities, including goiters, thyroiditis, adenomas, and carcinomas. The common denominator is metaplastic (Hürthle cell or oncocytic) change. As usual, colloid, inflammation, and honeycomb sheets of cells favor a benign/nonneoplastic interpretation, while numerous microfollicles, diffuse atypia, high N/C ratios, and features of papillary carcinoma favor a neoplastic/malignant interpretation. However, any thyroid lesion comprised exclusively, or nearly exclusively or Hürthle cells is likely to be neoplastic, and if neoplastic, there is a significant risk (~33%) of malignancy. Poorly differentiated carcinoma includes insular and non-insular types. The diagnostic features are: 1. solid/trabecular/insular growth, 2. No nuclear features of papillary carcinoma, and 3. At least one of a. convoluted nuclei, b. increased mitotic activity, and c. necrosis. The tumor cells typically express thyroglobulin and TTF-1, but are negative for calcitonin. Thyroid sarcomas are extremely rare. Most sarcomas are actually anaplastic thyroid carcinoma. Note that both thyroglobulin and cytokeratin can be negative in anaplastic carcinoma. Metastases to the thyroid are not rare, but were formerly rarely diagnosed during life. However, the advent of FNA biopsy has increased the rate of antemortem diagnosis. Thyroid metastasis is a grave prognostic sign. Most of the cancers are poorly differentiated, unlike most primary thyroid carcinomas. Common sites of origin include: kidney, lung, breast, GI carcinomas; melanoma; and lymphoma. Graves disease is related to Hashimoto thyroiditis. The diagnosis is usually made based upon clinical and laboratory findings, not FNA biopsy. Occasionally, however, a patient with Graves disease will undergo FNA biopsy (usually to investigate a cold nodule). The cytologic findings in Graves disease include: high cellularity, pale watery colloid, flame and Hürthle cells, and inflammation, which may include granulomas. 3
5 DeMay: Follicular Thyroid Lesions Therapeutic effects, ie, owing to radiation or antithyroid medications, can cause marked cytologic atypia. However, this atypia is usually randomly distributed and mitoses are rare. Note that radiation is a risk factor for thyroid carcinoma, particularly papillary carcinoma. Dyshormonogenetic goiter refers to thyroid enlargement due to congenital hypothyroidism. Autosomal recessive enzyme defects in hormone synthesis cause the goiter. The FNA biopsy is highly cellular, with microfollicles, cytologic atypia, and scant colloid mimicking a neoplasm, and carcinoma may be favored. However, actual malignant change is rare in this condition. Pregnancy is associated with loss of iodine in the urine, leading to thyroid hyperplasia. Any preexisting nodularity will be accentuated. The FNA biopsy is highly cellular, with watery colloid, and flame cells. Papillary hyperplasia ( polsters ) may suggest papillary carcinoma and women of childbearing age are at risk of papillary carcinoma. Look for the usually features of papillary carcinoma, such as nuclear grooves and inclusions, as previously discussed. The Bethesda System Diagnostic Terminology and Morphologic Criteria A six tiered diagnostic system was suggested at the NCI conference. Briefly, the six categories are: Benign; Atypical; Follicular Neoplasm; Suspicious; Malignant; and Nondiagnostic. The categories also include an estimate of the risk of malignancy and management recommendations. I. Non-Diagnostic Nondiagnostic includes limited cellularity, absence of follicular cells, poor fixation, excessive blood, and poor cell preservation. The risk of malignancy is not applicable to this category. (Adequacy defined as at least 6 groups of at least 10 well preserved, well visualized follicular cells. II. Benign Benign includes colloid nodular disease (eg, nodular goiter, hyerplastic/adenomatoid nodule, macrofollicular adenoma) and thyroiditis (eg, acute thyroiditis, chronic lymphocytic thyroiditis). The risk of malignancy is low (<3%). III. Atypical Atypia is a heterogeneous category that includes atypical cells of undetermined significance (ACUS), follicular lesion of undetermined significance (FLUS), indeterminate follicular lesions, rule-out neoplasm, and cellular nodule. The cytologic findings are not convincingly benign, yet the degree of cellular or architectural atypia is not sufficient for an interpretation of Follicular Neoplasm or Suspicious for Malignancy. Some cases are placed in this category because the specimen was compromised (eg, low cellularity, poor fixation, obscuring blood). The use of this category is optional, but should be kept to a minimum (<7% of all thyroid FNA interpretations was arbitrarily chosen). The risk of malignancy is between 5% and 15%. 4
6 DeMay: Follicular Thyroid Lesions IV. (Suspicious for) Follicular Neoplasm (Specify if Hürthle cell type) Follicular neoplasm includes suggestive or suspicious of follicular neoplasm, microfollicular lesion, and follicular lesion/ follicular nodule. This category applies to follicular patterned lesions, including Hürthle cell lesions, lacking nuclear features of papillary carcinoma. The risk of malignancy is between 20% and 30%. Notes: Up to 35% are nonneoplastic; of malignancies, up to 68% are papillary carcinoma. V. Suspicious Suspicious for malignancy includes suspicious for papillary carcinoma (most commonly), suspicious for medullary carcinoma (material inadequate for calcitonin staining; recommend serum calcitonin to confirm), suspicious for other primary or metastatic malignancy, and suspicious for neoplasm due to lesion necrosis (anaplastic carcinoma). The risk of malignancy is 60% to 75%. VI. Malignant Malignant includes specimens diagnostic of malignancy. The type of malignancy, eg, papillary carcinoma, should be specified when possible. Risk of malignancy is 97-99%. Diagnosis Cancer Risk Management I. Nondiagnostic NA Rpt w/ US II. Benign <3% F U Clinically III. AUS ACUS, FLUS IV. Follicular Neoplasm* 5% 15% Rpt FNA 20% 30% Surgery V. Suspicious 60% 75% Surgery VI. Malignant 97% 99% Surgery * Specify if Hürthle cell type Final Topic: An Epidemic of Thyroid Cancer? 5
7 11/2/2010 Pulmonary Cytology Kristen Atkins, MD University of Virginia The speaker has no relationship that represents a possible conflict of interest with respect to the content of this presentation. Procurement of Tissue Bronchoscopic Brushings, EBUS, Washes, lavage FNA Thorocentesis for pleural fluid Accuracy of detecting malignancy 1 Sputum< multiple sputums<brushing Transbronchial FNA< percutaneous FNA 1



8 11/2/2010 Normal components Malignancies Primary and metastatic Benign neoplasms Infections Oh no! The pitfalls. 2


9 11/2/2010 Primary Malignancies Squamous Adenocarcinoma Bronchoalveolar carcinoma Small cell Carcinoid 3


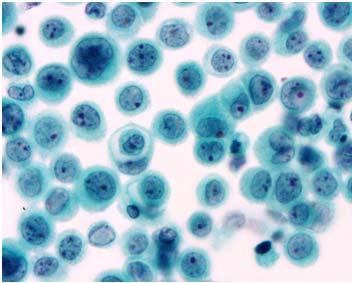
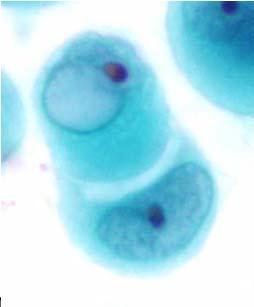
10 11/2/2010 Very blue Small Cell Carcinoma Nuclear streaking artifact Variability Single cell apoptosis Nuclear molding, chromatin pattern 4



11 11/2/2010 5



12 11/2/2010 BAC BAC VOLUME Columnar cells Inclusions, some atypia Not an outright diagnosis for cytology 6



13 11/2/2010 7



14 11/2/2010 BAC cytologic features Overlap with well-differentiated adenocarcinoma Columnar Enlarged nuclei (compared to internal control) Pseudonuclear inclusions, grooves Psammoma bodies Metastasis 8



15 11/2/2010 9




16 11/2/


17 11/2/




18 11/2/2010 Traumatic Numerous should spark viral possibility Ciliacytopthoria 12



19 11/2/2010 Peripheral Nodules Malignancies Metastases Benign neoplasms Mesothelioma Pleural fibrosis Chondroid Hamartoma 13




20 11/2/2010 Reactive Effusions Variable Cellularity Cell types: mesothelial cells, macrophages, inflammatory cells Architectural patterns: dispersed, papillary, sheets Mesothelial cells: Abundant cytoplasm, ruffled borders, vacuolization, nucleoli Microvilli Mesothelials, Breast, Pancreas, Stomach 14




21 11/2/2010 mesothelial like pattern of breast cancer 15
22 Special Course Cytomorphology II : FNA Cytology Salivary Glands William C. Faquin, MD, PhD Disclosure information The speaker has no relationship that represents a possible conflict of interest with respect to the content of this presentation.
23 Faquin - Salivary Gland FNA, Cytomorphology II: SALIVARY GLAND William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA
24 Faquin - Salivary Gland FNA, BACKGROUND TO SALIVARY GLAND CYTOLOGY Salivary gland cytology represents one of the most challenging areas of all of cytopathology owing to the wide range of lesions that can be encountered and the significant degree of overlap between some benign and malignant tumors. In approaching a salivary gland FNA, it is useful to apply an algorithmic approach by attempting to place the lesion into one of several different broad categories: GENERAL CATEGORIES FOR SALIVARY GLAND LESIONS: Matrix-containing tumors: e.g. pleomorphic adenoma and adenoid cystic carcinoma Basaloid neoplasms: e.g. basal cell adenoma Oncocytic lesions: e.g. oncocytoma and acinic cell carcinoma Mucinous cysts: e.g. low-grade mucoepidermoid carcinoma and mucocele High-grade carcinomas: e.g. salivary duct carcinom Lymphoid lesions: LESA and lymphoma Clear cell tumors: e.g. epithelial-myoepithelial carcinoma Spindle cell lesions: e.g. myoepithelioma RATIONALE AND INDICATIONS FOR SALIVARY GLAND FNAB: FNA is widely used at many institutions for the evaluation of salivary gland lesions. Overall, FNA is safe, cost-effective, and accurate. Most often, FNA acts as a guide for the clinician in assessing the need for surgical or other clinical intervention for any unexplained salivary gland mass. When surgery is indicated, results from the FNA can assist in the pre-operative strategy. The primary goal of salivary gland FNA is to place the diagnosis into 1 of 3 categories that will dictate management: Non-neoplastic lesions (e.g. chronic sialadenitis) may not require surgical intervention Benign tumors (e.g. pleomorphic adenoma) and low-grade malignancies are usually treated with limited surgery such as superficial parotidectomy with disease-free margins High-grade carcinomas are usually treated with radical surgery Facial nerve sacrifice may be necessary Lymph node neck dissection and neo-adjuvant therapy are often indicated ACCURACY Overall, FNA is fairly accurate in the assessment of salivary gland lesions. In recent studies, sensitivity and specificity for neoplasia is >90%. The distinction between benign and malignant neoplasms has a sensitivity of 80-90% and a specificity of >90%. Diagnostic accuracy is lower for rendering a specific diagnosis. High diagnostic accuracy for neoplastic versus non-neoplastic lesions High accuracy for low-grade versus high-grade lesions Variable accuracy depending upon the specific entity (e.g. high accuracy for tumors such as pleomorphic adenoma & Warthin tumor, but lower for tumors such as basal cell adenocarcinoma, solid adenoid cystic carcinoma, and epithelial-myoepithelial carcinoma) IMPORTANT!!! SAMPLE PREPARATION: Both Romanowsky-stained (Diff-Quik, Giemsa, MGG) and Papanicolaou stains are essential in the evaluation of most salivary gland lesions by FNA, especially those with matrix material. Air-dried Romanowsky-stained smears highlight diagnostically useful features of the matrix component that are poorly visualized in alcohol-fixed preparations of lesions such as pleomorphic adenoma, basal cell tumors, and adenoid cystic carcinoma. Romanowsky stains also aid in the evaluation of lymphoid lesions. Papanicolaou-stained smears are especially useful for


25 Faquin - Salivary Gland FNA, evaluating nuclear features and cytoplasmic differentiation. Yes, FNA of salivary glands can be done without both types of stains or even with thin-layer preparations, but depending upon the lesion, your diagnostic abilities may be limited. THE NORMAL SALIVARY GLAND ASPIRATE: Aspirates of normal salivary gland are comprised of groups of acinar cells, occasional ductal cells, and admixed adipose tissue. Acinar cells are usually present as cohesive polarized grape-like clusters with associated small inconspicuous tubules and small honeycomb sheets of cohesive ductal cells. Stripped nuclei from crushed acinar cells may be present in the background. The presence of normal salivary gland as the only cytologic finding warrants careful clinical correlation to exclude the possibility of a sampling error. Other explanations for normal-appearing salivary gland elements include a prominent but normal salivary gland, sialadenosis, and lipoma. Pitfall: A pitfall for the diagnosis of normal salivary gland tissue is mistaking it for acinic cell carcinoma (and vice versa). Cytologic Features of the Normal Salivary Gland Aspirate Serous and mucinous acinar cells in grapelike (lobular) clusters + background stripped nuclei Admixed small tubules and/or small sheets of ductal epithelium Adipose tissue Normal salivary gland showing ductal cells (left) and acinar cells BASIC SALIVARY GLAND TUMOR CYTOMORPHOLOGY: 1) MATRIX-CONTAINING TUMORS: The differential diagnosis of matrix-containing salivary gland tumors includes a number of entities, but the most common and clinically significant differential diagnosis is between pleomorphic adenoma and adenoid cystic carcinoma. Differential diagnosis of matrix-containing salivary gland tumors: Pleomorphic adenoma Adenoid cystic carcinoma Basal cell adenoma/adenocarcinoma Myoepithelioma Polymorphous low grade adenocarcinoma Epithelial-myoepithelial carcinoma




26 Faquin - Salivary Gland FNA, Pleomorphic Adenoma: Pleomorphic adenoma is the most common salivary gland tumor in both children and adults. Two-thirds of parotid tumors and 50% of all salivary gland tumors are pleomorphic adenomas. The most common site is the superficial parotid gland, often the tail of the gland at the angle of the jaw; occasionally, the latter are mistaken for a cervical lymph node. Approximately 50% of pleomorphic adenomas have been found to have specific gene rearrangements involving either the PLAG1 gene on chromosome 8q12 or the HMGA2 gene on chromosome 12q Cytologic features of pleomorphic adenoma: Cohesive epithelial cells in honeycomb groups Myoepithelial cells, often plasmacytoid or spindled Chondromyxoid matrix - fibrillary and bright magenta using Romanowsky stains The hallmark of pleomorphic adenoma in FNA specimens is its characteristic fibrillary matrix material. Pleomorphic adenomas are characterized by an admixture of cohesive epithelial cells, usually in a honeycomb pattern, and myoepithelial cells, that can have a variety of appearances including epithelioid, clear, spindled, and plasmacytoid. Unlike epithelial cells, myoepithelial cells are commonly found individually, embedded within matrix material, in loose clusters, or in larger, haphazardly arranged clusters. In my experience, pleomorphic adenomas are more often composed predominantly of myoepithelial cells, but epithelial-predominant lesions do occur and appear somewhat basaloid. In addition to the cellular component, there is a characteristic matrix material, best appreciated in air-dried Romanowsky-stained preparations where it has a fibrillary or "wet yarn" appearance. It stains pale green or colorless in Papanicolaou-stained preparations, and it has an intense magenta (metachromatic) color in Romanowsky stained smears. The distinctive fibrillary nature of the matrix material with its frayed, indistinct margins and embedded myoepithelial cells is characteristic enough to distinguish a pleomorphic adenoma from other lesions that may mimic it, especially adenoid cystic carcinoma. Pleomorphic adenoma Pap Stain Pleomorphic adenoma Diff-Quik Stain Some common pitfalls in diagnosing pleomorphic adenomas include: Cellular specimens with sparse or absent matrix material Lesions with focal adenoid cystic-like areas Lesions with focal cytologic atypia Lesions with metaplastic changes, especially squamous or mucinous features
 survival is poor.")



27 Faquin - Salivary Gland FNA, Adenoid Cystic Carcinoma: Adenoid cystic carcinomas represent 4-10% of all salivary gland neoplasms, usually occurring in middle-age women. Although the clinical course of adenoid cystic carcinoma is often protracted, longterm (15-20 year) survival is poor. Three histologic variants of adenoid cystic carcinoma are recognized and often present in combination: tubular, cribriform, and solid. Recognition of the solid pattern is important because of its more aggressive clinical course. The tendency of these tumors to invade nerves manifests itself clinically as a painful mass or as pain during the FNA, which should increase the clinical suspicion of malignancy. Cytologic features of adenoid cystic carcinoma: Variably sized, often large, three-dimensional hyaline matrix spheres and linear branching structures Matrix is acellular with sharp borders, and metachromatic Surrounding basaloid cells with dark angulated nuclei and variable nuclear atypia Adenoid cystic carcinoma Diff-Quik stain Adenoid cystic carcinoma Pap stain Aspirates of adenoid cystic carcinoma are classically comprised of acellular "cookie cutter-like" matrix spheres and tubules that are metachromatic in Romanowsky preparations and pale blue-green or colorless in Pap stains. The cellular component of adenoid cystic consists of small basaloid cells with angulated nuclei. The primary way that pleomorphic adenomas and adenoid cystic carcinomas are distinguished is based upon differences in their stroma. Romanowsky-stained preparations are essential for helping to make this distinction since it highlights the stromal features! Pleomorphic adenoma has fibrillar stroma with embedded cells, while adenoid cystic carcinoma has homogeneous acellular stroma in spheres and cylindrical shapes. 2) BASALOID TUMORS: This category is among the most difficult in salivary gland cytology, because there are several entities that have overlapping features. By basaloid, we mean that the cells have small dark nuclei and scant cytoplasm. In a majority of instances, the diagnosis of a basaloid tumor will be descriptive rather than specific. Importantly, the differential diagnosis includes basal cell adenoma, cellular pleomorphic adenoma, and solid adenoid cystic carcinoma. In some cases, these entities can look nearly identical, so beware! Differential diagnosis of basal cell tumors: Basal cell adenoma/adenocarcinoma Cellular pleomorphic adenoma Solid adenoid cystic carcinoma





28 Faquin - Salivary Gland FNA, Cytologic Features of the Membranous Subtype of Basal Cell Adenoma: While the diagnosis of most basaloid tumors of the salivary gland will be descriptive, there is one form of basal cell tumor that is distinctive: the membranous subtype of basal cell adenoma. The characteristic cytology of this entity is the presence of a thick acellular ribbon of homogeneous matrix material surrounding large clusters of bland basaloid cells (see Figure below). No other tumor in the salivary gland looks like this: Pitfall: Mistaking chronic sialadenitis for a basal cell tumor Beware of aspirates of chronic sialadenitis which can occasionally be mistaken for a basal cell tumor. Chronic sialadenitis does contain basaloid cells, but the aspirates are hypocellular in contrast to the cellular aspirates of most true basal cell tumors. In addition, chronic sialadenitis contains small angulated groups of basaloid cells in a background of mild chronic inflammation and fibrous tissue. Cytologic Features of Chronic Sialadenitis: Hypocellular Small angulated groups of basaloid cells Mild chronic inflammation Fibrous tissue, crystalloids, and stone fragments Hypocellular aspirate of chronic sialadenitis


29 Faquin - Salivary Gland FNA, ) ONCOCYTIC-APPEARING SALIVARY GLAND LESIONS: The differential diagnosis of oncocytic salivary gland tumors includes a variety of entities, but the most common differential diagnosis is between oncocytoma and acinic cell carcinoma. Acinic Cell Carcinoma vs Oncocytoma: Differential Diagnosis of Oncocytic Salivary Gland Tumors: Acinic cell carcinoma is the second most common salivary gland malignancy, representing approximately 4-6% of all salivary gland tumors and up to 17% of salivary gland malignancies. It is generally a low-grade tumor although high-grade forms do occur. Acinic cell carcinoma typically presents as a circumscribed, mobile, slowly-growing mass which occasionally is painful. Acinic cell carcinoma is best recognized in Diff-Quik stained specimens, which highlights its cytoplasmic vacuoles distinguishing the tumor cells from oncocytes of Warthin tumor and oncocytoma. Oncocytes of oncocytoma have homogeneously dense and granular cytoplasm that lacks vacuoles. Cytoplasmic zymogen granules in acinic cell carcinoma are PAS-positive diastase-resistant and negative for PTAH the opposite is true of oncocytomas. When acinic cell carcinomas show well-defined features of serous acinar differentiation, the tumor is easily recognized both cytologically and histologically. However, acinic cell carcinoma can show features of intercalated duct cells or of an adenocarcinoma, NOS, in which case, it is much more challenging to recognize the tumor specifically as acinic cell carcinoma. Cytologic features of acinic cell carcinoma: Oncocytoma Warthin tumor Acinic cell carcinoma Mucoepidermoid carcinoma, oncocytic variant Metastatic renal cell carcinoma Cellular smear of serous-type acinar cells Large polygonal cells with abundant finely vacuolated cytoplasm PAS+D resistant cytoplasmic zymogen granules Bland nuclear cytologic features Background stripped nuclei + lymphocytes Psammoma bodies may be seen Acinic Cell Carcinoma



 Oropharyngeal squamous cell carcinoma Sebaceous carcinoma (eyelid) Breast carcinoma Small cell carcinoma Metastatic renal cell carcinoma 4) CYSTIC AND MUCINOUS")
30 Faquin - Salivary Gland FNA, Oncocytoma: Aspirates have a clean background and groups Of oncocytes that lack cytoplasmic vacuoles. Warthin tumor is an example of a salivary gland tumor comprised of oncocytes in a background of lymphocytes and abundant granular background debris. Most aspirates of Warthin tumor are easily recognized and accurately diagnosed. Warthin tumor showing background debris, lymphocytes, and groups of oncocytes. In assessing an oncocytic lesion of the salivary gland, Diff-Quik stains for identification of cytoplasmic vacuoles is helpful, and sometimes, histochemical stains for intracellular mucin, PAS + diastase, and PTAH can be useful for narrowing the differential diagnosis. The differential diagnosis of metastatic renal cell carcinoma, raises the broader issue of metastatic disease in the head and neck region. The most common metastatic tumors encountered in periparotid and submandibular lymph nodes include: Cutaneous cancers (squamous cell carcinoma, melanoma, and Merkel cell carcinoma) Oropharyngeal squamous cell carcinoma Sebaceous carcinoma (eyelid) Breast carcinoma Small cell carcinoma Metastatic renal cell carcinoma 4) CYSTIC AND MUCINOUS SALIVARY GLAND LESIONS: The differential diagnosis of non-neoplastic and low-grade tumors where mucus-containing cells predominate includes a mucocele (a pseudocyst because it lacks an epithelial lining), ductal mucinous

31 Faquin - Salivary Gland FNA, metaplasia (mucus retention cyst) in sialolithiasis, mucinous metaplasia in Warthin tumor or pleomorphic adenoma, and low-grade mucoepidermoid carcinoma. Beware: The most important entity to consider in any salivary gland aspirate containing mucin is low grade mucoepidermoid carcinoma! The key to distinguishing low-grade mucoepidermoid carcinoma from benign mucinous cysts is to search for the characteristic 3 epithelial cell types, and especially the combination of mucus-containing epithelial cells and squamoid or intermediate cells within a group. Sometimes a definite diagnosis is not possible, especially when cell block material is not available or only cyst contents are aspirated.. Differential Diagnosis of mucinous cysts: Mucocele Mucus retention cyst Low-grade mucoepidermoid carcinoma Warthin s tumor with mucinous metaplasia Pleomorphic adenoma with mucinous metaplasia Low-grade mucoepidermoid carcinoma: Mucoepidermoid carcinoma is the most common salivary gland malignancy in children and adults and the most common malignancy of the major and minor salivary glands. The cytology of these tumors is variable depending upon the grade of the tumor, but low-grade forms are the most frequently encountered. Low-grade mucoepidermoid carcinoma is also the most common cause of a false-negative cytologic diagnosis, in part because the lesion is cystic and aspirates may yield only cyst contents, and partly because the epithelial cells are bland, and the mucin-containing cells can easily be misinterpreted as histiocytes or muciphages. Cytologically, low-grade mucoepidermoid carcinoma is characterized by a combination of 3 epithelial components: bland cohesive squamous cells, intermediate cells, and mucus cells in a background of cystic mucinous material. These lesions can be extremely challenging, and when possible, material for a cell block preparation should be obtained. The latter can be quite useful since ancillary marker stains for keratins and for intracellular mucin can help to solidify the diagnosis. Cytologic features of low-grade mucoepidermoid carcinoma: Mucus-containing epithelial cells Epidermoid cells (squamous features) Intermediate cells Mucinous background FNA of low grade mucoepidermoid carcinoma




32 Faquin - Salivary Gland FNA, Aspirates of mucoceles are hypocellular and contain histiocytes, mucinous background material, scattered inflammatory cells, and sometimes crystals. Mucocele containing muciphages in a mucoid background. 5) HIGH GRADE SALIVARY GLAND CANCERS: The differential diagnosis of high grade salivary gland cancers includes salivary duct carcinoma, high grade mucoepidermoid carcinoma, carcinoma ex pleomorphic adenoma, and metastatic disease. In some cases, it may be extremely difficult to distinguish salivary duct carcinoma from highgrade mucoepidermoid carcinoma and carcinoma ex pleomorphic adenoma, but clinical management tends to be similar for all of these cases. Distinction from distant metastasis is also difficult and depends on appropriate clinical information. Differential diagnosis of high grade salivary gland carcinomas Salivary duct carcinoma High grade mucoepidermoid carcinoma Carcinoma-ex-pleomorphic adenoma (malignant mixed tumor) Metastatic carcinoma Salivary Duct Carcinoma Salivary duct carcinoma is an uncommon, clinically aggressive malignancy that most commonly occurs in the parotid gland of older men. It resembles high-grade comedo-type ductal carcinoma of the breast. The cytologic features are those of a high-grade carcinoma. Cells are polygonal with moderate to abundant vacuolated cytoplasm, enlarged hyperchromatic nuclei with prominent nucleoli, and background necrosis. The cells are present in cohesive groups that may form sheets, papillae, and cribriform clusters. Cytologic features of salivary duct carcinoma: Overtly malignant cytology Polygonal cells with abundant vacuolated cytoplasm Prominent nucleoli Sheets, clusters, papillae, and cribriform groupings Background necrosis Salivary duct carcinoma


33 Faquin - Salivary Gland FNA, Carcinoma ex pleomorphic adenoma: Carcinoma ex pleomorphic adenoma (malignant mixed tumor) is a rare neoplasm. There are 3 types of malignant mixed tumor: metastasizing mixed tumor, carcinosarcoma, and carcinoma arising in a pleomorphic adenoma, the latter being the most common. When pleomorphic adenomas develop a malignant component, it is most commonly in the form of salivary duct carcinoma, although a variety of different salivary gland malignancies can arise, usually they are high-grade and clinically aggressive! Cytologic features of malignant pleomorphic adenoma: Carcinoma ex pleomorphic adenoma High-grade carcinoma (usually salivary duct carcinoma) juxtaposed with typical pleomorphic adenoma Metastasizing mixed tumor Indistinguishable from pleomorphic adenoma Carcinosarcoma Distinct, malignant epithelial and mesenchymal elements References: Carcinoma-ex-pleomorphic adenoma Abrams AM, Cornyn J, Scofield HH, Hansen LS. Acinic cell adenocarcinoma of the major salivary glands: a clinico-pathologic study of 77 cases. Cancer 1965; 18: Ali S. Acinic-cell carcinoma, papillary cystic variant: a diagnostic dilemma in salivary gland aspiration. Diagn Cytopathol 2002;27: Atula T, Klemi PJ, Donath K, Happonen RP, Joensuu H, Grenman R. Basal cell adenocarcinoma of the parotid gland: a case report and review of the literature. J.Laryngol.Otol. 1993; 107: Batsakis JG, Sneige N, el-naggar AK. Fine-needle aspiration of salivary glands: its utility and tissue effects [see comments]. Ann.Otol.Rhinol.Laryngol. 1992; 101: Brachtel, EF, Pilch BZ, Khettry U, Zembowicz A, Faquin WC. Fine needle aspiration biopsy of a cystic pleomorphic adenoma with extensive adnexa-like differentiation: Differential diagnostic pitfall with mucoepidermoid carcinoma. Diagn. Cytopathol. 2003;28: Brown D, Konzen B, Kashkari S. Fine needle aspiration of basal cell adenocarcinoma of salivary gland. Acta Cytol. 1994; 38:853a(Abstract) Cajulis RS, Gokaslan ST, Yu GH, Frias-Hidvegi D. Fine needle aspiration biopsy of the salivary glands. A five-year experience with emphasis on diagnostic pitfalls. Acta Cytol. 1997; 41: Chan MK, McGuire LJ, King W, Li AK, Lee JC. Cytodiagnosis of 112 salivary gland lesions. Correlation with histologic and frozen section diagnosis. Acta Cytol. 1992; 36: Cooper TL. Fine Needle Aspiration of the Head and Neck, Part A: Cytopathology of the salivary glands, neck, soft tissue, and skin. In: Pilch BZ., ed. Head and Neck Surgical Pathology. Philadelphia: Lippincott Williams & Wilkins, 2000: Dodd LG, Caraway NP, Luna MA, Byers RM. Myoepithelioma of the parotid. Report of a case initially examined by fine needle aspiration biopsy. Acta Cytol. 1994; 38: Droese M. Cytological diagnosis of sialadenosis, sialadenitis, and parotid cysts by fine-needle aspiration
34 Faquin - Salivary Gland FNA, biopsy. Adv.Otorhinolaryngol. 1981; 26:49-96: Elliott DD, Krane JF, Pitman MB, Pilch BZ, Faquin WC. Fine needle aspiration biopsy (FNAB) of salivary gland basal cell tumors. Mod.Pathol. 2001; 14:51a(Abstract) Ellis GL, Auclair PL. Tumors of the salivary glands. Washington, D.C.: Armed Forces Institute of Pathology, Elsheikh TM, Bernacki EG. Fine needle aspiration cytology of cellular pleomorphic adenoma. Acta Cytol. 1996; 40: Eneroth CM, Zajicek J. Aspiration biopsy of salivary gland tumors. II. Morphologic studies on smears and histologic sections from oncocytic tumors (45 cases of papillary cystadenoma lymphomatosum and 4 cases of oncocytoma). Acta Cytol. 1965; 9: Eneroth CM, Zajicek J. Aspiration biopsy of salivary gland tumors. III. Morphologic studies on smears and histologic sections from 368 mixed tumors. Acta Cytol. 1966; 10: Eneroth CM, Zajicek J. Aspiration biopsy of salivary gland tumors. IV. Morphologic studies on smears and histologic sections from 45 cases of adenoid cystic carcinoma. Acta Cytol. 1969; 13: Faquin WC, Powers CL. Salivary Gland Cytopathology. New York: Springer-Verlag, Faquin WC, Krane JF, Pilch BZ, Cooper TL. Fine needle aspiration of benign and malignant myoepithelial-predominant neoplasms of the parotid gland. Mod.Pathol. 2000; 13:33a(Abstract) Frable MA, Frable WJ. Fine-needle aspiration biopsy of salivary glands. Laryngoscope 1991; 101: Geisinger KR, Weidner N. Aspiration cytology of salivary glands. Semin.Diagn.Pathol. 1986; 3: Granger JK, Houn HY. Malignant mixed tumor (carcinosarcoma) of parotid gland diagnosed by fineneedle aspiration biopsy. Diagn.Cytopathol. 1991; 7: Heintz PW, Schmidt WA, Pommier RF, Vetto JT, DiTomasso JP. Submandibular gland carcinoma ex pleomorphic adenoma. Report of a case with cytologic features and diagnostic pitfalls. Acta Cytol. 1998; 42: Hood IC, Qizilbash AH, Salama SS, Alexopoulou I. Basal-cell adenoma of parotid. Difficulty of differentiation from adenoid cystic carcinoma on aspiration biopsy. Acta Cytol. 1983; 27: Jandu M, Webster K. The role of operator experience in fine needle aspiration cytology of head and neck masses. Int.J.Oral Maxillofac.Surg. 1999; 28: Kern SB. Necrosis of a Warthin's tumor following fine needle aspiration. Acta Cytol. 1988; 32: Klijanienko J, Vielh P. Fine-needle sample of salivary gland lesions. V: Cytology of 22 cases of acinic cell carcinoma with histologic correlation. Diagn.Cytopathol. 1997; 17: Klijanienko J, Vielh P. Fine-needle sampling of salivary gland lesions. III. Cytologic and histologic correlation of 75 cases of adenoid cystic carcinoma: review and experience at the Institut Curie with emphasis on cytologic pitfalls. Diagn.Cytopathol. 1997; 17: Klijanienko J, Vielh P. Fine-needle sampling of salivary gland lesions. IV. Review of 50 cases of mucoepidermoid carcinoma with histologic correlation. Diagn.Cytopathol. 1997; 17:92-8. Krane JF, Faquin WC. Salivary Glands. In: Cibas ES, Ducatman BS, ed. Cytology: Diagnostic Principles and Clinical Correlates. Philadelphia: W.B. Saunders Company, Kumar N, Kapila K, Verma K. Fine needle aspiration cytology of mucoepidermoid carcinoma. A diagnostic problem. Acta Cytol. 1991; 35: Layfield LJ, Glasgow BJ. Diagnosis of salivary gland tumors by fine-needle aspiration cytology: a review of clinical utility and pitfalls. Diagn.Cytopathol. 1991; 7: Layfield LJ, Gopez EV. Cystic lesions of the salivary glands: cytologic features in fine-needle aspiration biopsies. Diagn Cytopathol 2002;27: Lee SS, Cho KJ, Jang JJ, Ham EK. Differential diagnosis of adenoid cystic carcinoma from pleomorphic adenoma of the salivary gland on fine needle aspiration cytology. Acta Cytol. 1996; 40: Lussier C, Klijanienko J, Vielh P. Fine-needle aspiration of metastatic nonlymphomatous tumors to the major salivary glands: a clinicopathologic study of 40 cases cytologically diagnosed and histologically correlated. Cancer 2000.Dec.25.;90.(6.): : Mino M, Pilch BZ, Faquin WC. Expression of KIT (CD117) in neoplasms of the head and neck: An ancillary marker for adenoid cystic carcinoma. Mod. Pathol. 2003;16: Mooney EE, Dodd LG, Layfield LJ. Squamous cells in fine-needle aspiration biopsies of salivary gland lesions: potential pitfalls in cytologic diagnosis. Diagn.Cytopathol. 1996; 15: Spiro RH, Huvos AG, Strong EW. Acinic cell carcinoma of salivary origin. A clinicopathologic study of 67 cases. Cancer 1978; 41:
35 Faquin - Salivary Gland FNA, Stanley MW, Horwitz CA, Rollins SD, et al. Basal cell (monomorphic) and minimally pleomorphic adenomas of the salivary glands. Distinction from the solid (anaplastic) type of adenoid cystic carcinoma in fine-needle aspiration. Am.J.Clin.Pathol. 1996; 106: Watanabe K, Ono N, Saito K, Saito A, Suzuki T. Fine-needle aspiration cytology of polymorphous lowgrade adenocarcinoma of the tongue. Diagn.Cytopathol. 1999; 20:167-9.
36 Special Course Cytomorphology II : FNA Cytology Pancreas Gregg A. Staerkel, MD Disclosure information The speaker has no relationship that represents a possible conflict of interest with respect to the content of this presentation.
37 Fine Needle Aspiration of the Pancreas Gregg A. Staerkel, M.D. Fine-needle aspiration (FNA) has become the preferred method for evaluating a lesion of the pancreas suspected of being neoplastic in nature. The selection of FNA as a diagnostic tool has occurred because of radiologic technological advances. In addition, the utility of FNA has improved sensitivity/specificity for tumor detection while decreasing complications seen in traditionally performed biopsy procedures. Pancreatic Fine-Needle Aspiration: Prior to FNA, cutting needle or wedge biopsy and endoscopic exfoliative cytology were widely utilized. For the pancreas, cutting needle and wedge biopsies yield complications that include hemorrhage, fistula formation, pancreatitis and death in 5 to 20% of cases. Furthermore, obtaining representative tissue for histologic examination can be problematic in up to half of cases sampled. In addition, histologic tissues obtained for frozen section evaluation can yield a false positive rate of 3%. Although endoscopic exfoliative cytology is a relatively safe method for tissue acquisition, sensitivity rates are low, in the neighborhood of 50%. Reaching the level of a stricture for sampling can be difficult because of the small size of pancreatic ducts. The use of fine needle aspiration, in conjunction with computed tomography and ultrasonography, has maintained the reliability of diagnosing pancreatic carcinoma with specificity rates near 100%, while increasing sensitivity to 80 to 90%. Percutaneous computerized tomographic guided-fna is technically easier to use than percutaneous ultrasound as it is unaffected by gas within the bowels and excessive adipose tissue. However, the lack of real-time imaging increases procedure time. The arrival of endoscopic ultrasonography eliminates the prior mentioned problem with percutaneous ultrasound. It also allows for the evaluation of the primary pancreatic lesion and, if malignant, simultaneous staging of the disease. In addition, smaller lesions can be detected and/or biopsied in less time with real-time imaging. It should be noted that with any technique employed, overall accuracy increases with aspirator experience and with the availability of a cytopathologist for immediate specimen adequacy assessment. Major complications for FNA are reported at less than a tenth of one percent. The relative non-invasive detection of malignancy by fine needle aspiration causes little or no change in the performance status of the patient for subsequent surgery or chemoradiation.
38 Fine Needle Aspiration of the Pancreas I. Pancreas Aspiration II. III. Increased diagnostic accuracy and decreased rate of complications, (e.g. hemorrhage, pancreatitis, death), when compared to core needle or wedge biopsy Normal Pancreas A. Exocrine Tissue 1. Serous Acini a. Small cohesive, raspberry-like groups [Aggressive smears can disrupt groups giving impression of single cells (similar to cells of an islet cell tumor); recognition of the small nuclear sizes of these dispersed cells is key] b. Cell borders between cells, indistinct (margins of group, defined) c. Nucleus, eccentrically placed d. Nucleus, small, round to oval, smooth contour e. Chromatin, hyperchromatic, evenly distributed f. Nucleolus, small, inconspicuous g. Cytoplasm, granular and abundant (relative to size of nucleus) 2. Excretory Ducts a. Monolayer sheets 1) Uniform columnar to cuboidal cells 2) Cell borders between cells, indistinct to honeycombed (margins of group, defined) 3) Nucleus, round/oval, smooth contour, fine evenly distributed chromatin, indistinct nucleolus 4) Nuclear spacing uniform throughout cell fragment with minimal to no overlap b. Cylindrical tubular structures [Cellular composition, same as monolayer sheets (see above)] B. Endocrine Tissue [Not recognizable in cytology preparations due to sparse distribution and similarity to acinar cells that have been disrupted (special stains required)] Pancreatic FNA Contaminants A. Duodenum (approach to head lesions) 1. Flat sheets showing goblet cells (appear to have zone of clear cytoplasm around nucleus) spaced at regular intervals. 2. Three dimensional, elephant trunks, epithelial groups (represents the epithelial lining of villi) Page 1
39 3. Lamina propria fragments (recognized as stromal fragments containing inflammatory cells) B. Stomach (approach to body and tail lesions) 1. Flat sheets of columnar cells with diffuse mucinous cell features (can be confused with mucinous neoplasms since background mucin can also be present) 2. Gastric glands either do not aspirate or are not recognized and therefore interpreted as normal pancreatic ductal epithelium. C. Differentiation of benign pancreatic ductal epithelium and gastrointestinal epithelium. 1. B72.3 labeling -Benign pancreatic ductal epithelium: negative -Gastrointestinal contamination: goblet cells with strong, coarse granular pattern and other epithelial cells with finely granular, punctuate, perinuclear distribution 2. Mucin expression -normal duodenum MUC1 - MUC2 + MUC5AC - MUC6 + -non-neoplastic pancreas MUC1 + MUC2 MUC5AC - MUC6 + IV. Reactive Pancreas (Pancreatitis) [Related to biliary tract disease, excessive alcohol intake and trauma] A. Acinar Tissue [Similar in appearance to normal pancreas (see above)] B. Ductal Tissue Atypia seen can cause confusion with malignancy, features to note: 1. Nuclear enlargement, relatively uniform throughout cells of the same fragment, with minimal nuclear overlap 2. Sizes of nuclei (total nuclear volume), within the same fragment, do not show differences of 4:1 or greater 3. Nuclear contours remain round/oval 4. Nucleoli may be prominent 5. Mitotic activity, infrequent 6. Necrotic debris, histiocytes and acute inflammatory cells can be seen Page 2
40 V. Tumors A. Non-neoplastic Cysts 1. Congenital [Less than 5 cm., low cuboidal to no epithelium with fibrous connective tissue wall, filled with mucoid or serous fluid] a. Scant epithelium with features similar to those described under Normal Pancreas/Excretory Ducts/Monolayer sheets (see above) b. Proteinaceous background 2. Pseudocyst [5-10cm., fluid collection secondary to inflammation, necrosis or hemorrhage (history of pancreatitis), located adjacent to tail of pancreas, no lining cells (fibrous connective tissue only), filled with serous/turbid fluid high amylase, normal CEA and viscosity less than serum (separates from cystic neoplasms)] a. No epithelium, although mesothelium may be inadvertently obtained b. Variable amounts of mixed inflammatory cells, fibroblasts and granular debris B. Benign Neoplasms 1. Serous Cystadenoma [synonyms: microcystic adenoma and glycogenrich adenoma; serous oligocystic adenoma (large cysts present)] [Elderly female (F/M:3/1) individuals (mean age 66), frequently large, multicystic, involving head of pancreas, central scar, sun burst type calcifications on CT scan, clear fluid, sponge-like, vascular tumor (post contrast media enhancement, mucinous tumors do not)] a. Few cuboidal cells and small groups in monolayers b. Clear cytoplasm (glycogen) c. Honeycomb pattern d. Nucleus, round/oval, smooth contour, fine evenly dispersed chromatin, inconspicuous nucleolus e. PAS stain positive, not diastase resistant indicating glycogen and not mucin 2. Lymphoepithelial Cyst [Typically found incidentally or large in size, greater than 5 cm, when abdominal pain is complaint, peripancreatic, 80% occur in men] a. Anucleated squamous cells (ghost-like looking sometimes) b. Granular amorphous debris in background (looks like necrotic debris grossly when placed on slides; +/- cholesterol crystals) c. Lymphoid component sparse or not recognized (due to size of lesion, lymphoid component is stretched thin, needle passes quickly through) Page 3
41 3. Solid-Pseudopapillary Tumor (Synonym: Solid and Papillary Epithelial Neoplasm) [Adolescent girls and young women (F/M: 9/1, mean age 28), usually discovered incidentally or during pregnancy or after trauma, tail of pancreas, greater than 10 cm., encapsulated, lesion is solid however cells furthest from small vessels are acantholytic-like and drop out of histologic sections creating a pseudopapillary pattern with cystic spaces] a. Slender papillary fronds b. Small cells c. Nucleus, round/oval, smooth contour, fine evenly dispersed chromatin, inconspicuous nucleolus d. Globules of myxoid material among cells (Pap: pale blue; Diff- Quik: reddish) e. Electron microscopy shows no neuroendocrine granules (helps distinguish from islet cell tumor which has cytologic similarity) f. Immunoperoxidase stains for B-catenin, CD56, CD10, alpha-1- antitrypsin and vimentin are positive, pan-keratin can be positive in 1/3 of cases and synaptophysin can be focally positive, chromogranin is negative C. Mucinous Lesions 1. Pancreatic intraepithelial neoplasia (PanIN) - in-situ lesion, thought to give rise to invasive ductal carcinomas Entity is not knowingly aspirated as they are clinically not detectable grossly not visible (typically <0.5 cm) with no visible mucin Classification - Normal: epithelium is low columnar with amphophilic cytoplasm and no mucinous cell changes, cellular crowding or nuclear atypia - Pan IN-1A: mucinous metaplasia, lesion is flat composed of tall columnar cells with basally oriented nuclei and supranuclear mucin - PanIN-1B: same as PanIN-1A plus micropapillary to papillary or basally pseudostratified architecture - Pan1N-2: mostly papillary, but, can be flat with nuclear abnormalities (enlargement, hyperchromasia, crowding, pseudostratification +/or loss of polarity); rare, non-atypical, nonapical mitoses - PanIN-3: micropapillary to papillary, only rarely flat with greater nuclear abnormality than PanIN-2; mitoses may be atypical and apical, cribriforming, budding off of small cell groups into lumen Page 4
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Salivary gland cytology. Salivary gland cytology. Triage helps the clinician. Salivary gland tumors. Diagnostic difficulties
 Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
Salivary gland cytology Salivary Gland Cytology Pınar Fırat, MD Professor of Pathology İ.U. İstanbul Faculty of Medicine Çapa, İstanbul It is a reliable diagnostic test However, definitive subclassification
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION
 Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology
 Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Ben Witt, MD University of Utah/ARUP Laboratories Assistant Professor of Anatomic Pathology Review some of the more common cytodiagnoses of the Head and Neck Establish an approach to some of the diagnostic
Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma:
 SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Pleomorphic Adenoma: Cytologic Variations and Potential Diagnostic Pitfalls
 Pleomorphic Adenoma: Cytologic Variations and Potential Diagnostic Pitfalls Uma Handa, M.D., Neerja Dhingra, M.D., D.N.B.,* Rajan Chopra, M.D., and Harsh Mohan, M.D., M.N.A.M.S., F.I.C.P. The diverse morphological
Pleomorphic Adenoma: Cytologic Variations and Potential Diagnostic Pitfalls Uma Handa, M.D., Neerja Dhingra, M.D., D.N.B.,* Rajan Chopra, M.D., and Harsh Mohan, M.D., M.N.A.M.S., F.I.C.P. The diverse morphological
Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls
 Original Research Article DOI: 10.18231/2394-6792.2017.0102 Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls Vaneet Kaur Sandhu 1,*, Navtej
Original Research Article DOI: 10.18231/2394-6792.2017.0102 Cytomorphological spectrum of pleomorphic adenoma with emphasis on differential diagnosis and diagnostic pitfalls Vaneet Kaur Sandhu 1,*, Navtej
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Salivary gland Workshop Trondheim 31th may 2012
 Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Salivary gland Workshop Trondheim 31th may 2012 Peter Jebsen cytopathologist Oslo University Hospital Rikshospitalet Anna Bofin ass. Professor St. Olavs Hospital, Trondheim Drying artifacts Lymfocytes
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
ORIGINAL ARTICLE. Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population
 ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
ORIGINAL ARTICLE Fine-Needle Aspiration Biopsy of Salivary Gland Lesions in a Selected Patient Population Erik G. Cohen, MD; Snehal G. Patel, MD; Oscar Lin, MD; Jay O. Boyle, MD; Dennis H. Kraus, MD; Bhuvanesh
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors
 An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA An Integrated
An Integrated Cytologic and Histologic Approach to the Diagnosis of Salivary Gland Tumors W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Boston, MA An Integrated
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
The Korean Journal of Cytopathology 15(1) : 60-64, 2004
 : 60-64, 2004") 15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Thyroid Cytopathology: Weighing In The Bethesda System
 Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
encapsulated thyroid nodule with a follicular architecture and some form of atypia. The problem is when to diagnose
 Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS
 NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
NODULAR CYSTIC HIDRADENOMA OVER THE GLUTEAL REGION: A RARE CYTOMORPHOLOGICAL DIAGNOSIS Abstract: The primary as well as metastatic tumours of the skin can be diagnosed by fine needle aspiration cytology
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Fine needle aspiration cytology of salivary gland lesions with histopathological correlation - A two year study
 Original article Fine needle aspiration cytology of salivary gland lesions with histopathological correlation - A two year study Tessy PJ, Jayalekshmy PS, Cicy PJ, Usha Poothiode Department of Pathology,
Original article Fine needle aspiration cytology of salivary gland lesions with histopathological correlation - A two year study Tessy PJ, Jayalekshmy PS, Cicy PJ, Usha Poothiode Department of Pathology,
Cytomorphological study of major salivary gland lesions: a 5-year experience at a tertiary care center
 Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
Original article Cytomorphological study of major salivary gland lesions: a 5year experience at a tertiary care center Aruna S, Prathiksha Pai, Shreekant K. Kittur Department of Pathology, Belagavi Institute
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Case #1. Ed Stelow, MD University of Virginia
 Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung
 Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung masses. Specimen shown is from a tap of the pleural effusion.
Case 1. Slide 1 History: 65 year old male presents with bilateral pleural effusions, a 40 pack year smoking history and peripheral and hilar lung masses. Specimen shown is from a tap of the pleural effusion.
Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on?
 Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on? RITU NAYAR, MD PROFESSOR & VICE CHAIR OF PATHOLOGY NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DIRECTOR OF CYTOPATHOLOGY,
Thyroid Cytopathology: What s New and What s Old That We Don t All Agree on? RITU NAYAR, MD PROFESSOR & VICE CHAIR OF PATHOLOGY NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DIRECTOR OF CYTOPATHOLOGY,
Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland
 The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
The Korean Journal of Pathology 2013; 47: 481-485 CASE STUDY Fine-Needle Aspiration Cytology of Low-Grade Cribriform Cystadenocarcinoma with Many Psammoma Bodies of the Salivary Gland Ji Yun Jeong Dongbin
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Case # year old man with a 2 cm right kidney mass
 Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
3/22/2017. Disclosure of Relevant Financial Relationships. Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Pathology Slides. [Pathology]
![Pathology Slides. [Pathology]](/thumbs/94/120604575.jpg "Pathology Slides. [Pathology]") Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Almost any suspected tumor can be aspirated easily and safely. Some masses are more risky to aspirate including:
 DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
DOES THIS PATIENT HAVE CANCER? USING IN-HOUSE CYTOLOGY TO HELP YOU MAKE THIS DIAGNOSIS. Joyce Obradovich, DVM, Diplomate, ACVIM (Oncology) Animal Cancer & Imaging Center, Canton, Michigan Almost every
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
LGM International, Inc.
 Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Liqui-PREP TM Cytology Atlas Preface The following pictures are examples with descriptions of cytology slides processed with the Liqui-PREP TM System.. The descriptions are reviewed by Pathologists. It
Departments of Pathology and *Otorhinolaryngology, Faculty of Medicine, University of Malaya, Kuala Lumpur
 Malaysian J Pathol 2002; 24(2) : 107-112 CASE REPORT Papillary cystic type of acinic cell carcinoma of parotid: fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia
Malaysian J Pathol 2002; 24(2) : 107-112 CASE REPORT Papillary cystic type of acinic cell carcinoma of parotid: fine needle aspiration cytological features of a high grade variant with oncocytic metaplasia
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
International Journal of Pharma and Bio Sciences CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY.
 Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 CHROMOPHOBE VARIANT OF RENAL CELL CARCINOMA MASQUARDING AS RENAL ONCOCYTOMA ON CYTOLOGY. DR.MAMATHA K*, DR. ARAKERI
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Pancreatic malignant tumors are the fifth leading cause of cancerrelated
 44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
Enterprise Interest None
 Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Oncocytic carcinoma: A rare malignancy of the parotid gland
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Oncocytic carcinoma: A rare malignancy of the parotid gland K Mardi, J Sharma Citation K Mardi, J Sharma.. The Internet Journal of Pathology.
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
FNA Biopsy of Salivary Gland
 FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
FNA Biopsy of Salivary Gland Richard M. DeMay, MD Professor of Pathology Director of Cytopathology The University of Chicago Objective: To describe the use of FNA Bx to diagnose salivary gland lesions
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Normal Morphology. Anatomic Considerations. Normal Urothelial Histology and Cytology
 1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
1 Normal Morphology Anatomic Considerations The urinary tract can be divided into three regions: the kidney; the calyces, pelves and ureters (upper collecting system or upper tract); and the bladder and
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Role of fine needle aspiration cytology and cytohistopathological co-relation in thyroid lesions: experience at a tertiary care centre of North India
 International Journal of Research in Medical Sciences Chandra S et al. Int J Res Med Sci. 2016 Oct;4(10):4552-4556 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163328
International Journal of Research in Medical Sciences Chandra S et al. Int J Res Med Sci. 2016 Oct;4(10):4552-4556 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163328
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for