Hyperurikaemie - nur Gicht oderauch kardio-renales Risiko?
|
|
|
- Eugenia Eaton
- 5 years ago
- Views:
Transcription





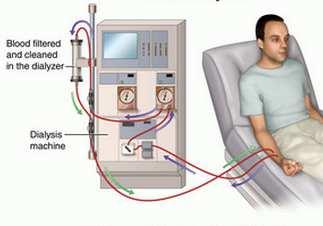
1 9. November 2017 Hyperurikaemie - nur Gicht oderauch kardio-renales Risiko? PD Dr. Bernhard Hess Innere Medizin & Nephrologie NierensteinZentrum Zürich Hirslanden Kliniken Im Park & Hirslanden, Zürich Konsiliararzt Nephrologie, Kantonsspital, Baden / AG



2 Hyperurikamie-das Zipperlein!? B. Hess 11/2017
 LS/OA LS/OA & Allopurinol PGC 51.9 56.7 50.1 mmhg sbp 126.4 143.3 121.8 mmhg systemic/intrarenal hypertension& glom.")
3 Hyperuricemia& cardio-renal risk Animal experiments: male Sprague Dawley rats fed 2% oxonic acid (OA) on low salt diet (LS) mild hyperuricemia kidney biopsies after 5 weeks: afferent glomerular arterioles LS (control) LS/OA LS/OA & Allopurinol PGC mmhg sbp mmhg systemic/intrarenal hypertension& glom. arteriolopathy in hyperuricemic animals, abolished by allopurinol B. Hess 11/2017 (adapted from Sanchez-Lozada LG et al., Am J Physiol Renal Physiol 283: F1105-F1110, 2002)
4 Rats -hyperuricemia& atherosclerosis Uric acid in VSMC cultures(rats) Platelet-derived growth factor (A &C chains) Tissue Angiotensin II - attenuated by ACE-I & ARBs Oxidative stress NO bioavailability VSMC proliferation/ hypertrophy ATHEROSCLEROSIS B. Hess 11/2017 (adaptred from Corry DB et al., J Hypertens 26: , 2008)
5 Hyperuricemiaand hypertension $ Meta-Analysis: - 18 prospective cohort studies subjects -endpoint: incident hypertension (GraysonPC et al. Arthritis Care Res 63: , 2011) B. Hess 11/2017
 Multidetector computed tomography (3 mm slices, reconstruction interval 1.")
6 Hyperuricemia& coronary artery calcification Cross-sectional retrospective study : Check-up in 4884 South Koreans, excluded: <20/>80 years, CAD, gout, nephrolithiasis, medications altering S-UA 4188 subjects (2559 males, 1629 females) Multidetector computed tomography (3 mm slices, reconstruction interval 1.5 mm) coronary artery calcium(cac) scores CAC group1:cac score 0 = calcium absent CAC group2:cac score CAC group3:cac score >300 Multivariate-adjusted associations between S-uric acid and CAC scores (adjustedfor age, sex, diabetesmellitus, hypertension, smoking, sbp, BMI, CRP, Hb, WBC, egfr, glucose, lipids) B. Hess 11/2017 (from Kim H et al., Medicine 2017 Apr; 96(14):e6565. doi: /MD
,never-treatedstage 1 hypertension, S-uric acid > 356 µmol/l.randomization : Allopurinol 2 x 200 mg/d vs. placebo 4 weeks B.")
7 Hyperuricemiaand CV disease-allopurinolin hypertensiveadolescents 30 adolescents (11-17 yrs.),never-treatedstage 1 hypertension, S-uric acid > 356 µmol/l.randomization : Allopurinol 2 x 200 mg/d vs. placebo 4 weeks B. Hess 4/2017 (adapted from Feig DI et al., JAMA 300: , 2008)
8 Hyperuricemia& CV disease-allopurinol effectson LV mass& endothelialdysfunctionin CKD - RCT 67 elderly patients, CKD stage 3, LV hypertrophy, randomization: allopurinol 300 mg/d vs.placebo on top of other medication (not different between groups), 9 months, 53 finished study (27 A, 26 P). NO differencein sbp & dbp at 9 months. S-UA:Allopurinol 440 to 260 µmol/l, Placebo 420 to 440 µmol/l (p < ) Left ventricular mass index Flow-mediated dilation brachial artery B. Hess 11/2017 (from Kao MP et al., J Am Soc Nephrol 22: , 2011)
9 Uric acid lowering: effects on Renin-Angiotensinsystem and ambulatory blood pressure - RCT Double-blind placebo-controlled trial adults, BMI >25 kg/m 2, meanserumua 6.1 mg/dl(363 µmol/l) 62% white, male/female1 : 1 Excluded: hypertension, CAD, egfr < 60, malignancy, liver disease Randomization: 8 weeks treatment with - Placebo (n = 53, 45 completedstudy) - Allopurinol (n =49, 35 completed study) - Probenecid(n = 47, 40 completedstudy) Primary endpoints: systemic and kidney-specific RAS-activity NO differences between groups despite significant uric acid lowering in both treatment arms vs. placebo NO changes in plasma renin and angiotensin II Secondary endpoints: mean 24h-BP, awake/asleep BP, night dipping NO changes, NO differences between groups B. Hess 11/2017 (from McMullan CJ et al., Clin J Am Soc Nephrol 12: , 2017)
 trial of allopurinol (up to 600 mg daily) versus no treatment in a 1:1 ratio, added to usual")
10 Multicentre, prospective, randomised, openlabel, blinded end point trial of the efficacy of allopurinol therapy in improving cardiovascular outcomes in patients with ischaemic heart disease: the ALL-HEART study Multicentre, controlled, prospective, randomised, open-label blinded end point (PROBE) trial of allopurinol (up to 600 mg daily) versus no treatment in a 1:1 ratio, added to usual care, in 5215 patients aged 60 years and over with ischemic heart disease(scotland & GB). The primary outcome is the composite of non-fatal myocardial infarction, non-fatal stroke or cardiovascular death. The study is event-driven and results are expected after B. Hess 4/2017(fromMackenzieIS et al., BMJ Open.2016 Sep 8;6(9):e doi: /bmjopen
11 SUMMARY -Hyperuricemia& CV disease There is clinical evidence that hyperuricemia. increases BP / induces systemic arterial hypertension in adolescents, but not in adults (different pathophysiology?) is associated with coronary artery calcification causes vascular hypertrophy / endothelial dysfunction (reduced flow-mediated dilation) modestly increases left ventricular mass index Xanthine oxidase inhibition is able to reduce blood pressure in adolescents can attenuate endothelial dysfunction in adolescents and adults is able to reduce LV mass index in elderly adults B. Hess 11/2017

12 Hyperuricemia& chronickidneydisease - epidemiology Vienna Health Screening Project, healthy volunteers, mean follow-up 7.4 years, followup examinations, egfr calculated by MDRD formula Statistics : Adjustmentsfor age, gender, waist circumference, mean arterial BP, antihypertensives, blood glucose, blood lipids, baseline egfr Primary outcome/results: developmentof CKD stage3 (egfr< 60) in relationtoserumuricacid(s-ua) at baseline: - Normal reference: S-UA < 7.0 mg/dl (< 416 µmol/l) OR Sligthlyelevated: S-UA mg/dl ( µmol/l) - Elevated: S-UA >9.0 mg/dl (>530 µmol/l) B. Hess 4/2017 (modified from Obermayr RP et al., J Am Soc Nephrol 19: , 2008) OR 1.74 OR 3.12
13 new CKD 3 B. Hess 4/2017 (modified from Obermayr RP et al., J Am Soc Nephrol 19: , 2008) Hyperuricemia& chronickidneydisease(2)
14 Allopurinol & chronickidneydisease - randomizedevidence Stable clinical condition-- egfr< 60 ml/min/1.73 m 2 (MDRD formula) -- Stable CKD (MDRD) 100 mg/d 24 months B. Hess 4/2017 (modified from Coicoechea M et al., Clin J Am Soc Nephrol 5: , 2010)
15 Allopurinol & chronickidneydisease - randomizedevidence(2) B. Hess 4/2017 (modified from Coicoechea M et al., Clin J Am Soc Nephrol 5: , 2010)
 Meta-analysis - 4 RCTs included -")
16 Renoprotection-allopurinolvs. febuxostat Literature search - 49 full-text articles - 45 excluded(no RCTs, conference papers, no adequate outcome, duplication) Meta-analysis - 4 RCTs included - Endpoints : S-creatinine egfr Albuminuria S-uric acid B. Hess 11/2017 (adapted from Kim S et al, Kidney Res Clin Pract 36: , 2017)
17 Allopurinol & chronickidneydisease - the field evidence Retrospectivecohortstudy: Medicaredata (U.S.), 5% randomsample, age>65 years, newlytreatedwithallopurinol(e.g. filledallopurinolprescriptionafter 183 dayswithoutprescription) Main outcome : 1 st occurrence of renal failure (ICD-9) during follow-up Predictors : allopurinol dose, durationof allopurinol use Multivariate adjustments: - age, gender, race, Charlson-Romano comorbidity index - Medications: β blockers, ACE inhibitors, statins, diuretics, allopurinol Cohortcharacteristics: allopurinol treatments without history of renal failure(baseline) - Follow-up: 8314 episodes with incident renal failure, without B. Hess 4/2017 (modified from Singh JA & Yu S, Ann Rheum Dis 76: , 2017)
18 Allopurinol & chronickidneydisease - the field evidence(2) Hazard ratio for incident renal failure Hazard ratio for incident renal failure days days >1-2 years > 2 years Allopurinol dose (mg/d) Duration Allopurinol B. Hess 4/2017 (modified from Singh JA & Yu S, Ann Rheum Dis 76: , 2017)

19 KONKLUSIONEN 1. Hyperurikaemie ist nicht einfach Gicht 2. Evidenz (exp./klin. Studien) für Hyperurikaemie als... CV Risikofaktor : Endothelschaden/-dysfunktion, VSMC Proliferation, BD und Renin bei Adoleszenten, LVH bei älteren Erwachsenen ABER: nur kleine Studien, grosse randomisierte, placebo-kontrollierte Studien fehlen renaler Risikofaktor: gute epidemiologische Evidenz, Harnsäure-Effekt durch Hypertonie verstärkt ABER: grosse randomisierte, placebo-kontrollierte Studien fehlen 3. Harnsäuresenkung mit Xanthinoxidase-Hemmern kann CV und renales Risiko senken, unabhängig von andern RF zeigt in höheren Dosen und über längere Therapiedauer whs. mehr Benefit, ABER: keine randomisierte, placebo-kontrollierte Studien B. Hess 11/2017
Dr. Mehmet Kanbay Department of Medicine Division of Nephrology Istanbul Medeniyet University School of Medicine Istanbul, Turkey.
 The uric acid dilemma: causal risk factor for hypertension and CKD or mere bystander? Mehmet Kanbay, Istanbul, Turkey Chairs: Anton H. van den Meiracker, Rotterdam, The Netherlands Claudia R.C. Van Roeyen,
The uric acid dilemma: causal risk factor for hypertension and CKD or mere bystander? Mehmet Kanbay, Istanbul, Turkey Chairs: Anton H. van den Meiracker, Rotterdam, The Netherlands Claudia R.C. Van Roeyen,
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey
 THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey Chairs: Gerjan Navis, Groningen, The Netherlands Kamil Serdengecti, Istanbul, Turkey Dr. M. Kanbay Division of Nephrology
THE ROLE OF URIC ACID IN THE PROGRESSION OF CKD Mehmet Kanbay, Istanbul, Turkey Chairs: Gerjan Navis, Groningen, The Netherlands Kamil Serdengecti, Istanbul, Turkey Dr. M. Kanbay Division of Nephrology
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease
 Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Allopurinol reduces left ventricular hypertrophy and endothelial dysfunction in patients with chronic kidney disease Michelle P Kao, Donald S Ang, Steve Gandy, Chim C Lang, Allan D Struthers Division of
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Fructose, Uric Acid and Hypertension in Children and Adolescents
 Fructose, Uric Acid and Hypertension in Children and Adolescents Daniel I. Feig, MD, PhD, MS Director, Division of Nephrology Department of Pediatrics University of Alabama, Birmingham Topics for Discussion
Fructose, Uric Acid and Hypertension in Children and Adolescents Daniel I. Feig, MD, PhD, MS Director, Division of Nephrology Department of Pediatrics University of Alabama, Birmingham Topics for Discussion
Insidie del binomio iperuricemia e rischio CV
 Insidie del binomio iperuricemia e rischio CV Claudio Borghi, FESC, FAHA Department of Medical and Surgical Sciences University of Bologna, Bologna, Italy Claudio Borghi Potential conflicts of interest
Insidie del binomio iperuricemia e rischio CV Claudio Borghi, FESC, FAHA Department of Medical and Surgical Sciences University of Bologna, Bologna, Italy Claudio Borghi Potential conflicts of interest
CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial)
") CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial) William B. White, MD for the CARES Investigators Calhoun Cardiology Center University
CARDIOVASCULAR SAFETY OF FEBUXOSTAT OR ALLOPURINOL IN PATIENTS WITH GOUT AND CARDIOVASCULAR DISEASE (The CARES Trial) William B. White, MD for the CARES Investigators Calhoun Cardiology Center University
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Estrogens vs Testosterone for cardiovascular health and longevity
 Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Warum verirrt sich Kalzium in die Gefässeund fehlt im Knochen?
 Osteoporose Zentrum Zimmerberg (OZZ) NierensteinZentrum Zürich Warum verirrt sich Kalzium in die Gefässeund fehlt im Knochen? PD Dr. Bernhard Hess Innere Medizin & Nephrologie Kliniken Im Park & Hirslanden,
Osteoporose Zentrum Zimmerberg (OZZ) NierensteinZentrum Zürich Warum verirrt sich Kalzium in die Gefässeund fehlt im Knochen? PD Dr. Bernhard Hess Innere Medizin & Nephrologie Kliniken Im Park & Hirslanden,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Stadien der Progression bei CKD
 Stadien der Progression bei CKD Complications Normal Increased risk Damage GFR Kidney failure CKD death Screening for CKD risk factors CKD risk reduction; Screening for CKD Diagnosis & treatment; Treat
Stadien der Progression bei CKD Complications Normal Increased risk Damage GFR Kidney failure CKD death Screening for CKD risk factors CKD risk reduction; Screening for CKD Diagnosis & treatment; Treat
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS
 GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
GALECTIN-3 PREDICTS LONG TERM CARDIOVASCULAR DEATH IN HIGH-RISK CORONARY ARTERY DISEASE PATIENTS Table of Contents List of authors pag 2 Supplemental figure I pag 3 Supplemental figure II pag 4 Supplemental
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm
 Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm Department of Cardiology Keiji Inoue Akira Ueoka, Naoki Maruyama, Yoshiaki Shimoda, Eigo Kishita,
Clinical Significance of Aldosterone Levels and Low Grade Inflammation in Patients with Coronary Vasospasm Department of Cardiology Keiji Inoue Akira Ueoka, Naoki Maruyama, Yoshiaki Shimoda, Eigo Kishita,
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Supplementary Online Content
 Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
Correlation of novel cardiac marker
 Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Cardiovascular Diseases in CKD
 1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography
 Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography Hyo Eun Park 1, Eun-Ju Chun 2, Sang-Il Choi 2, Soyeon Ahn 2, Hyung-Kwan Kim 3,
Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography Hyo Eun Park 1, Eun-Ju Chun 2, Sang-Il Choi 2, Soyeon Ahn 2, Hyung-Kwan Kim 3,
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Association between arterial stiffness and cardiovascular risk factors in a pediatric population
 + Association between arterial stiffness and cardiovascular risk factors in a pediatric population Maria Perticone Department of Experimental and Clinical Medicine University Magna Graecia of Catanzaro
+ Association between arterial stiffness and cardiovascular risk factors in a pediatric population Maria Perticone Department of Experimental and Clinical Medicine University Magna Graecia of Catanzaro
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Cardiovascular Complications Of Chronic Kidney Disease. Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen
 Cardiovascular Complications Of Chronic Kidney Disease Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen Markers of kidney dysfunction Raised Albumin / Creatinine
Cardiovascular Complications Of Chronic Kidney Disease Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen Markers of kidney dysfunction Raised Albumin / Creatinine
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Uricemia nei pazienti a. fattore o marker di rischio? Claudio Borghi, FESC, FAHA Dipartimento di Scienze Mediche e Chirurgiche Università di Bologna
 Uricemia nei pazienti a rischio CV: fattore o marker di rischio? Claudio Borghi, FESC, FAHA Dipartimento di Scienze Mediche e Chirurgiche Università di Bologna R.Magritte: La reproducion interdite Urate
Uricemia nei pazienti a rischio CV: fattore o marker di rischio? Claudio Borghi, FESC, FAHA Dipartimento di Scienze Mediche e Chirurgiche Università di Bologna R.Magritte: La reproducion interdite Urate
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
SUPPLEMENTARY DATA. Supplementary Figure S1. Cohort definition flow chart.
 Supplementary Figure S1. Cohort definition flow chart. Supplementary Table S1. Baseline characteristics of study population grouped according to having developed incident CKD during the follow-up or not
Supplementary Figure S1. Cohort definition flow chart. Supplementary Table S1. Baseline characteristics of study population grouped according to having developed incident CKD during the follow-up or not
CHALLENGES OF HYPERTENSION IN THE COALFACE
 CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
CHALLENGES OF HYPERTENSION IN THE COALFACE Y VERIAVA CENTRE FOR RURAL HEALTH SCHOOL OF CLINICAL MEDICINE FACULTY OF HEALTH SCIENCES UNIVERSITY OF WITWATERSRAND SYSTOLIC AND DIASTOLIC BLOOD PRESSURES (BP)
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Statins in the elderly : Is there a rationale?
 Statins in the elderly : Is there a rationale? Pr B Boland After a communication by Dr. Manfred Gogol EAMA, Sion, June, 2006 1 RCTs with Statins Meta-Analysis, 1999 182 abstracts or research papers 29
Statins in the elderly : Is there a rationale? Pr B Boland After a communication by Dr. Manfred Gogol EAMA, Sion, June, 2006 1 RCTs with Statins Meta-Analysis, 1999 182 abstracts or research papers 29
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Lucia Cea Soriano 1, Saga Johansson 2, Bergur Stefansson 2 and Luis A García Rodríguez 1*
 Cea Soriano et al. Cardiovascular Diabetology (2015) 14:38 DOI 10.1186/s12933-015-0204-5 CARDIO VASCULAR DIABETOLOGY ORIGINAL INVESTIGATION Open Access Cardiovascular events and all-cause mortality in
Cea Soriano et al. Cardiovascular Diabetology (2015) 14:38 DOI 10.1186/s12933-015-0204-5 CARDIO VASCULAR DIABETOLOGY ORIGINAL INVESTIGATION Open Access Cardiovascular events and all-cause mortality in
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
THE IMPACT OF CCB AND RAS INHIBITOR COMBINATION THERAPY TO PREVENT CKD INCIDENCE IN HYPERTENSION AND ADVANCED ATHEROSCLEROSIS
 THE IMPACT OF CCB AND RAS INHIBITOR COMBINATION THERAPY TO PREVENT CKD INCIDENCE IN HYPERTENSION AND ADVANCED ATHEROSCLEROSIS Daisuke MAEBUCHI, Yasuyuki SHIRAISHI, Hiroaki TANAKA, Yumiko INUI, Makoto TAKEI,
THE IMPACT OF CCB AND RAS INHIBITOR COMBINATION THERAPY TO PREVENT CKD INCIDENCE IN HYPERTENSION AND ADVANCED ATHEROSCLEROSIS Daisuke MAEBUCHI, Yasuyuki SHIRAISHI, Hiroaki TANAKA, Yumiko INUI, Makoto TAKEI,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National