Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
|
|
|
- Sherman Arnold
- 5 years ago
- Views:
Transcription
1 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
2
3
4 Prevention Tight glucose control reduces the development of diabetic nephropathy
5 Progression Of Complications In Type 1 Diabetics With Intensive And Conventional Treatment (DCCT) - Primary Prevention Complications Conventional Therapy Intensive Therapy Risk Reduction Rate/100 patient-year % (95% CI) Urinary Alb (mg/24hr) > (2-56) > ( ) Clinical Nephropathy at 5 years (24-87) The Diabetes Control And Complications Trial Research Group, NEJM 1993
6 Progression Of Complications In Type 1 Diabetics With Intensive And Conventional Treatment (DCCT) -Secondary Prevention Complications Conventional Therapy Intensive Therapy Risk Reduction Rate/100 patient-year % (95% CI) Urinary Alb (mg/24hr) > (21-58) > (18-76) Clinical Nephropathy at 5 years (29-73) The Diabetes Control And Complications Trial Research Group, NEJM 1993
7 UKPDS Prospective randomized trial in type II diabetics Selected newly diagnosed Type II DM with little or no prexisting renal complications Compared the effect of intensive therapy and conventional therapy on development of complications.
8 UKPDS Patients on the intensive therapy arm were treated with a sulphonylurea, or if needed insulin was added, to keep fasting blood glucose <7mmo/l Conventional therapy was started with diet, and a sulphonylurea added to keep fasting blood glucose <15mmol/l. Patients followed up 10 years
9 Effect of Intensive Therapy And Conventional Therapy On Renal End Points At Nine Years In Type 2 DM with Normoalbuminuria Intensive (FG <7) Conventional (FG<15) p RR for intensive (99% CI) Microalbuminuria < ( ) Proteinuria ( ) Doubling of serum creatinine < ( ) UK Prospective Diabetes Study Group, Lancet 1998
10 Prevention Blood pressure control reduces the development of microvascular disease in diabetics

11 Tight BP control reduces microvascular events Tight : 144/82 mm Hg achieved Less: 154/72 mmhg achieved ight blood pressure control and risk of macrovascular and icrovascular complications in type 2 diabetes: UKPDS 38. K Prospective Diabetes Study Group UK Prospective Diabetes Study Group, BMJ 1998;317:

12 Tight BP control reduces microvascular events ight blood pressure control and risk of macrovascular and icrovascular complications in type 2 diabetes: UKPDS 38. K Prospective Diabetes Study Group UK Prospective Diabetes Study Group, BMJ 1998;317:
13 Tight Blood Pressure Control Confers CV Benefits in Diabetic Patients The benefits of lowering BP in the UKPDS were greater than those achieved through glycemic control 0 Stroke Any DM endpoint DM death Microvascular complications Reduction in Risk (%) DM=diabetes mellitus FPG=fasting plasma glucose *P<0.05. * * Tight glucose control (FPG < 107 mg/dl) * Tight BP control (150/85 mmhg) * UKPDS 35. BMJ. 2000;321: ; UKPDS 38. BMJ. 1998;317:
14 Screening Screening for albuminuria should begin 5 years after the diagnosis of type 1 diabetes It should be done immediately after the diagnosis of type 2 diabetes. Screening for albuminuria should be done annually
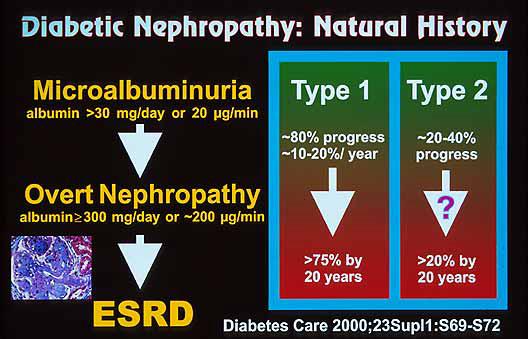
15 ABNORMAL ALBUMIN EXCRETION Timed (ug/min) 24 hour (mg/day) Alb/Cr (mg/gm) Normal <20 <30 <30 Microalbuminuria Macroalbuminuria >200 >300 >300 Microalbuminuria needs to be persistent over 6 months
16 Screening Serum creatinine should be done annually and the GFR estimated Cockcroft Gault equation (Age/weight/cr) MDRD formula (Age, creatinine)
17 Renal insufficiency in the absence of albuminuria and retinopathy among adults with type 2 diabetes mellitus 3 rd NHNES; > 40 yrs, T2 DM; Survey 13% of type 2 DM with CRI (MDRD) DR 28% Microalbuminuria 45% Macroalbuminuria 19% 30% of CRI with neither DR nor albuminuria Kramer HJ et al; JAMA 2003; 289;
18 Detection of Microalbuminuria
19 Impact of Blood Pressure Reduction on Mortality in Diabetes Trial Conventional care Intensive care Risk reduction P-value UKPDS 154/87 144/82 32% HOT 144/85 140/81 66% Mortality endpoints are: UK Prospective Diabetes Study (UKPDS) diabetes related deaths Hypertension Optimal Treatment (HOT) Study cardiovascular deaths in diabetics Turner RC, et al. BMJ. 1998;317: Hansson L, et al. Lancet. 1998;351:
20 Drug choices in the non-albuminuric hypertensive diabetic patient Blood pressure control reduces cardiovascular events Initial drug choices include Angotensin converting enzyme inhibitors Angiotensin receptor blockers Beta blockers Diuretics Calcium channel blockers
21 ABCD: Effect of blood pressure control on diabetic microvascular complications in patients with hypertension and type 2 diabetes. 470 hypertensive diabetics DBP> 90 2 x 2; nislodipine vs enalapril; Intensive versus moderate 5 year follow up Intensive BP 132/78 vs Mod 138/76 Results GFR decline no difference Normo to Micro: 25% vs 18 % (p 0.20 ns) Micro to Macro: 16 % vs 25% (p 0.28 ns) Estacio RO et al; Diabetes Care 2000; 23; Suppl 2 B 54-64
22 Blood Pressure Target The blood pressure target in all diabetics should be less than 130/80 Diabetics with proteinuria in excess of 1 gram should attempt to achieve values of less than 125/75 mm Hg
23 COURSE OF GFR, ALBUMINURIA, MEAN ARTERIAL BLOOD PRESSURE IN 9 IDDM PATIENTS TREATED WITH ANTIHYPERTENSIVES 125 MAP (mmhg) GFR (ml/min/1.73m2) Albuminuria (ug/min) years Parving HH et al; Am J Kidney Dis Jul;22(1):188-95
24 GFR (ml/min/year) Meta Analysis: Lower Mean BP Results in Slower Rates of Decline in GFR in Diabetics and Non-Diabetics MAP (mmhg) /85 140/90 r = 0.69; P < 0.05 Untreated HTN Parving HH, et al. Br Med J Moschio G, et al. N Engl J Med Viberti GC, et al. JAMA Bakris GL, et al. Kidney Int Klahr S, et al. N Eng J. Med Bakris GL. Hypertension Hebert L, et al. Kidney Int The GISEN Group. Lancet Lebovitz H, et al. Kidney Int Bakris GL, et al. Am J Kidney Dis. 2000;36(3): Reprinted by permission, Harcourt Inc. Slide Source HypertensionOnline
25 Mean glomerular filtration rate (GFR) decline and achieved follow-up blood pressure in study B* GFR 13-24; n = 255 Peterson, J. C. et. al. Ann Intern Med 1995;123:
26 Mean glomerular filtration rate (GFR) decline and achieved follow-up blood pressure in study A* GFR 22-55ml/min; n = 585 Peterson, J. C. et. al. Ann Intern Med 1995;123:
27 Combination Therapy Needed to Achieve Target SBP Goals Trial/SBP Achieved UKPDS (144 mm Hg) RENAAL(141 mm Hg) ALLHAT (138 mm Hg) IDNT HOT (138 mm Hg) (138 mm Hg) INVEST (133 mm Hg) ABCD MDRD AASK (132 mm Hg) (132 mm Hg) (128 mm Hg) Number of BP Medications Bakris GL et al. Am J Kidney Dis. 2000;36:
28 Drug choices in early nephropathy The initial therapy of choice should include and ACE inhibitor or an ARB
29 Drug Choices in Type 1 diabetics with overt nephropathy In the presence of overt nephropathy in type 1 diabetes, there is evidence that an ACE inhbitor can retard the progression of otherwise progressive renal disease
30 ACE-I Is More Renoprotective Than Conventional Therapy in Type 1 Diabetes % with doubling of baseline creatinine Baseline creatinine >1.5 mg/dl & overt proteinuria Placebo n=202 P<.001 Captopril n= Placebo BP achieved /80-84; Captopril BP achieved 128/134/77-82 Years of follow-up 50% ollaborative Study Group Trial Lewis EJ, et al. N Engl J Med. 1993;329(20):
31 Drug choices in type 2 diabetics with overt nephropathy In type 2 diabetes with overt nephropathy, either an ACE inhibitor or an ARB may be used to retard the progression of renal disease.
32 Long-Term Benefits of ACE Inhibition in Normotensive Type 2 Diabetics With Microalbuminuria Proteinuria (mg/24 h) Placebo (n=45) * ** *** *** Enalapril Percentage of initial value 100/creatinine Enalapril (n=49) * * Placebo Years *p<0.05; **p<0.01; p<0.02; ***p< Years Ravid et al. Ann Intern med. 1993; 118(8):
33 ARBs Can Reduce Diabetic Renal Disease Progression 30 RENAAL 30 IDNT Doubling of serum creatinine concentration (% of patients) p = rr 25% p = rr 20% p < rr 23% 0 Losartan Placebo 0 Irbesartan Amlodipine Placebo n = 1513; 3.45 years n = 1715; 2.6 years Brenner et al. N Engl J Med 2001;345: ; Lewis et al. N Engl J Med 2001;345:
34 IRMA II Irbesartan vs Placebo Primary Endpoint at 2 Years Total # of Progression to Nephropathy Patients n % Unadjusted Risk Reduction P Value Adjusted* Risk Reduction P Value 300 mg Irbesartan % < % < mg Irbesartan % % 0.05 Placebo For irbesartan vs placebo (the significance level for the primary endpoint was 0.025) *Hazard ratios were adjusted for baseline level of microalbuminuria and blood pressure achieved during the study Parving HH, et al. N Engl J Med. 2001;345(12):
35 IRMA II Change in Urinary Albumin Excretion* % change in urinary albumin excretion Placebo 150 mg of irbesartan 300 mg of irbesartan Months of Follow-up *P<0.001 for difference between both irbesartan groups and placebo Parving HH, et al. N Engl J Med. 2001;345(12):
36 Incidence of Diabetic Nephropathy (%) Placebo (n) Irbesartan 150 mg (n) Irbesartan 300 mg IRMA II Incidence of Progression to Diabetic Nephropathy P<0.001 for difference between 300 mg irbesartan group and placebo Placebo Months of Follow-up 150 mg of irbesartan 300 mg of irbesartan % % 5.2% Parving HH, et al. N Engl J Med. 2001;345(12):
37 Drug Choices in type 2 diabetics with early nephropathy Both an ARB and ACE inhibitor demonstrate similar benefit in reducing a decline in the GFR
38 Inclusion criteria 250 patients Inclusion criteria Male or female, years Type 2 diabetes (onset >40 years) on diet ± OHA or insulin ACE inhibitor for 3 months (ACE inhibitor tolerant) Mild-to-moderate hypertension (BP 180/95 mmhg) Barnett et al. N Engl J Med 2004;351: Normal gross renal morphology 12 months
39 Outcomes Primary endpoint Change in GFR after 5 years Secondary endpoints Changes in GFR after 1, 2, 3 and 4 years Changes in UAER and serum creatinine after 1, 2, 3, 4 and 5 years Incidence of clinical events Barnett et al. N Engl J Med 2004;351: (end-stage renal disease, myocardial infarction,
40 Barnett et al. N Engl J Med 2004;351: ARB vs ACE inhibitors in type 2 diabetes and incipient nephropathy Total GFR p = NS Change in GFR Telmisartan Enalapril 0 ml/min/1.73m Telmisartan Enalapril ml/min/1.73m p = NS Baseline After 5 years *All patients, LOCF; 250 patients; 5 years follow up p = NS, telmisartan vs enalapril
41 Drug choices in type 2 diabetics with overt nephropathy In type 2 diabetes with overt nephropathy, either an ACE inhibitor or an ARB may be used to retard the progression of renal disease.
42 Problems of use of ACE inhibitors Hyperkalaemia Acute renal failure with underlying bilateral renal artery stenosis
43 SBP (mmhg) Impact of ACE-I I on BP and GFR: Acute and Chronic Effects * * * GFR ml/min/1.73m * * 125 Baseline 1 Month *P<0.05 compared to baseline 5.6 Yrs Month off ACE-I +Clonidine Bakris GL, Weir MR. Arch Intern Med. 2000;160(5): American Medical Association 60 Baseline 1 Month 5.6 Yrs Month off ACE-I +Clonidine Slide Source HypertensionOnline
44 Recommended Practices The serum creatinine and potassium should be checked within 4 weeks of initiation of treatment to detect any rise in the serum creatinine of hyperkalaemia
45 The effect of dietary protein restriction on the progression of diabetic and nondiabetic renal diseases: a meta-analysis. Jan 1996 to Dec studies IDDM; 5 studies non DM CRF End points: Death and reduce GFR decline FU (mths) Study Size OR IDDM 9 to [ ] Non DM 18 to [ ] Pedrini MT et al; Ann Intern med 1996; 124:
46 Other measures: low protein diet Type 1 diabetics with overt nephropathy should be maintained on a low protein diet of 0.8gram / kg/ day of protein
47 Clinical Targets Therapy should aim to reduce albuminuria as much as possible, and its is reasonable to aim for a urinary protein levels to less than 1 gram per day or at least 50% of the pre treatment value
48 Recommended nephrology consultation Decline in renal function Difficulties in hyperkalaemia Atypical features eg haematuria, casts, renal bruits Difficult blood pressure control Heavy proteinuria (in excess of 3 gm/day) Absence of retinopathy
49 Summary
50 Prevention Tight glucose control reduces the development of diabetic nephropathy
51 Prevention Blood pressure control reduces the development of microvascular disease in diabetics
52 Screening Screening for albuminuria should begin 5 years after the diagnosis of type 1 diabetes It should be done immediately after the diagnosis of type 2 diabetes. Screening for albuminuria should be done annually
53 Screening Serum creatinine should be done annually and the GFR estimated Cockcroft Gault equation (Age/weight/cr) MDRD formula (Age, creatinine)
54 Blood Pressure Target The blood pressure target in all diabetics should be less than 130/80 Diabetics with proteinuria in excess of 1 gram should attempt to achieve values of less than 125/75 mm Hg
55 Drug Choices in Type 1 diabetics with overt nephropathy In the presence of overt nephropathy in type 1 diabetes, there is evidence that an ACE inhbitor can retard the progression of otherwise progressive renal disease
56 Drug choices in type 2 diabetics with overt nephropathy In type 2 diabetes with overt nephropathy, either an ACE inhibitor or an ARB may be used to retard the progression of renal disease.
57 Other measures: low protein diet Type 1 diabetics with overt nephropathy should be maintained on a low protein diet of 0.8gram / kg/ day of protein
58 Clinical Targets Therapy should aim to reduce albuminuria as much as possible, and its is reasonable to aim for a urinary protein levels to less than 1 gram per day or at least 50% of the pre treatment value
59 Recommended nephrology consultation Decline in renal function Difficulties in hyperkalaemia Atypical features eg haematuria, casts, renal bruits Difficult blood pressure control Heavy proteinuria (in excess of 3 gm/day) Absence of retinopathy
Firenze 22 settembre 2007
 Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
Istituto di di medicina dello sport di di Firenze AMES Prevenzione cardiovascolare e cambiamenti negli stili di vita Firenze 22 settembre 2007 Orientamenti attuali per un intervento farmacologico e non
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence?
 Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Diabetic Nephropathy 2009
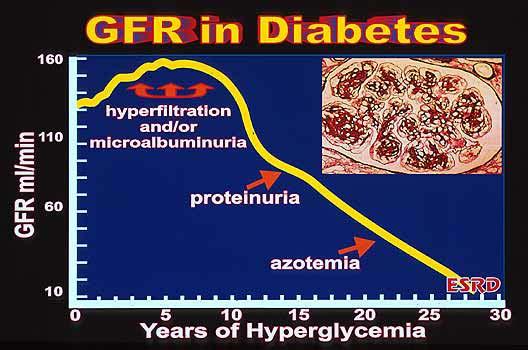
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Prevention and management of chronic kidney disease in type 2 diabetes
 162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
162..194 NEPHROLOGY 2010; 15, S162 S194 doi:10.1111/j.1440-1797.2010.01240.x Prevention and management of chronic kidney disease in type 2 diabetes Date written: April 2009nep_1240 Final submission: April
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Diabetes has become the most common
 P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
Risk factors associated with the development of overt nephropathy in type 2 diabetes patients: A 12 years observational study
 Indian J Med Res 136, July 2012, pp 46-53 Risk factors associated with the development of overt nephropathy in type 2 diabetes patients: A 12 years observational study Vijay Viswanathan, Priyanka Tilak
Indian J Med Res 136, July 2012, pp 46-53 Risk factors associated with the development of overt nephropathy in type 2 diabetes patients: A 12 years observational study Vijay Viswanathan, Priyanka Tilak
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers. Robert D. Toto, MD
 R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
University of Groningen. Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste
 University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
For more information about how to cite these materials visit
 Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Diabetes has become the most common
 P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
P O S I T I O N S T A T E M E N T Diabetic Nephropathy AMERICAN DIABETES ASSOCIATION Diabetes has become the most common single cause of end-stage renal disease (ESRD) in the U.S. and Europe; this is due
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Management of Hypertension in Diabetic Nephropathy: How Low Should We Go?
 Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Review Advances in CKD 216 Published online: January 15, 216 Management of Hypertension in Diabetic Nephropathy: How Low Should We Go? Hillel Sternlicht George L. Bakris Department of Medicine, Section
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Keywords albuminuria, hypertension, nephropathy, proteinuria
 Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Should proteinuria reduction be the criterion for antihypertensive drug selection for patients with kidney disease? Rigas G. Kalaitzidis and George L. Bakris Department of Medicine, Hypertensive Diseases
Does renin angiotensin system blockade deserve preferred status over other anti-hypertensive medications for the treatment of people with diabetes?
 Editorial Page 1 of 6 Does renin angiotensin system blockade deserve preferred status over other anti-hypertensive medications for the treatment of people with diabetes? Joshua I. Barzilay 1, Paul K. Whelton
Editorial Page 1 of 6 Does renin angiotensin system blockade deserve preferred status over other anti-hypertensive medications for the treatment of people with diabetes? Joshua I. Barzilay 1, Paul K. Whelton
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Solving Slowing Progressive Renal Disease
 Focus on CME at Memorial University of Newfoundland Solving Slowing Progressive Risk factors and treatment strategies for patients with kidney and cardiovascular disease overlap. Thus, evaluating renal
Focus on CME at Memorial University of Newfoundland Solving Slowing Progressive Risk factors and treatment strategies for patients with kidney and cardiovascular disease overlap. Thus, evaluating renal
The retinal renin-angiotensin system: implications for therapy in diabetic retinopathy
 (2002) 16, S42 S46 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh : implications for therapy in diabetic retinopathy AK Sjølie 1 and N Chaturvedi 2 1 Department
(2002) 16, S42 S46 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh : implications for therapy in diabetic retinopathy AK Sjølie 1 and N Chaturvedi 2 1 Department
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
KDIGO conference on high CV risk associated with CKD. The role of BP in CKD stage 1-4
 KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
KDIGO conference on high CV risk associated with CKD The role of BP in CKD stage 1-4 Johannes Mann, MD & Catherine Clase, MB BChir Friedrich Alexander University, Erlangen-Nuremberg Munich General Hospitals,
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
E.Ritz Heidelberg (Germany)
") Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Chronic kidney disease-what can you do and when to refer?
 Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor Treatment in Diabetic Nephropathy GUIDELINES
 ACE Inhibitor Treatment in Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All patients with Type 1 or Type 2 diabetes mellitus complicated
ACE Inhibitor Treatment in Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All patients with Type 1 or Type 2 diabetes mellitus complicated
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine
 Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD)
") 13 : 6 RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) Abstract: Chronic Kidney Disease (CKD) is common, harmful and treatable. It is worldwide public health problem, with several adverse outcomes;
13 : 6 RETARDING PROGRESSION OF CHRONIC KIDNEY DISEASE (CKD) Abstract: Chronic Kidney Disease (CKD) is common, harmful and treatable. It is worldwide public health problem, with several adverse outcomes;
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Low-Dose Candesartan Cilexetil Prevents Early Kidney Damage in Type 2 Diabetic Patients with Mildly Elevated Blood Pressure
 453 Original Article Low-Dose Candesartan Cilexetil Prevents Early Kidney Damage in Type 2 Diabetic Patients with Mildly Elevated Blood Pressure Satoru MURAYAMA, Tsutomu HIRANO, Taro SAKAUE, Kenta OKADA,
453 Original Article Low-Dose Candesartan Cilexetil Prevents Early Kidney Damage in Type 2 Diabetic Patients with Mildly Elevated Blood Pressure Satoru MURAYAMA, Tsutomu HIRANO, Taro SAKAUE, Kenta OKADA,
The Heart and the Kidney
 1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
Educational and behavioral interventions hitherto published
 Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,
Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,