Azathioprine-associated Interstitial Pneumonitis
|
|
|
- Winfred Snow
- 6 years ago
- Views:
Transcription

1 Azathioprineassociated Interstitial Pneumonitis CARLOS W. M. BEDROSSIAN, M.D., AND BARRY KAHAN, M.D., PH.D. JEFFREY SUSSMAN, M.D., RICHARD H. CONKLIN, PH.D., M.D. Seven renal allograft recipients taking azathioprine (Imuran ) for immunosuppression developed bilateral pulmonary infiltrates and a falling p0 2 that did not respond to antibiotic therapy. lung biopsies revealed changes ranging from diffuse alveolar damage (DAD) to usual interstitial pneumonia () culminating in pulmonary fibrosis. There was no evidence of immune deposits, eosinophilia, vasculitis, granulomas, or microorganisms by cultures and appropriate stains. Following discontinuance of Imuran, the two cases with DAD revealed a significant clearing of the lung infiltrates, whereas four of five patients with died while suffering from respiratordependent ARDS. Biopsies showing hyaline membranes, intraalveolar edema and cuboidalization of alveolar epithelium were associated with total doses from 2,850 to 4,355 mg, whereas atypical epithelial hyperplasia, reorganization of distal air spaces, and fibrosis were noted in cases receiving from 5,600 to 28,625 mg of azathioprine. Ultrastructural changes were indistinguishable from those induced by other drugs causing pulmonary toxicity. In three cases atypical epithelial cells were detected cytologically in brushing specimens and appeared identical to those noted in the lung biopsies. Our findings are consistent with the view that azathioprine should be added to the list of agents capable of causing direct, dosedependent pulmonary toxicity. Accordingly, drugassociated diffuse interstitial pulmonary disease should enter the differential diagnosis of a lung infiltrate that develops in renal transplant patients receiving Imuran. (Key words: Imuran; Drug toxicity; Interstitial pneumonitis; Pneumotoxic drugs) Am J Clin Pathol 1984; 82: AZATHIOPRINE (Imuran ; Burroughs Wellcome, Research Triangle Park, NC) is a potent immunosuppressive drug used primarily as an antiproliferative agent to prevent rejection after renal transplantation. Other indications for use of the drug include chronic inflammatory bowel diseases such as ulcerative colitis and regional enteritis and the collagen vascular diseases systemic lupus erythematosus and rheumatoid arthritis. 7 More recently, the drug also has been utilized in the treatment of chronic active hepatitis, glomerulonephritis, and a variety of hematologic and nonhematologic disorders. Complications of azathioprine therapy consist chiefly of hepatotoxicity, bone marrow suppression, and opportunistic infection. Pulmonary toxicity generally is not recognized as a side effect, even though two isolated case Received October 3, 1983; received revised manuscript and accepted for publication November 16, Address reprint requests to Dr. Bedrossian: Department of Pathology, St. Louis University School of Medicine, 1402 S. Grand Blvd., St. Louis, Missouri Department of Pathology, Vanderbilt University School/VA Medical Center, Nashville, Tennessee, and Transplant Division, Department of Surgery, University of Texas Medical School, Houston, Texas reports have implicated azathioprine in the development of interstitial lung disease. 8 " The present study reports seven cases of interstitial lung disease that developed in renal transplant recipients during immunosuppressive therapy with azathioprine. No infectious agents or other etiologic factors could be identified to account for the pulmonary changes; furthermore, the pathologic changes suggest drug toxicity. Materials and Methods All available clinical and pathologic data including chest roentgenograms were reviewed from seven renal transplant patients receiving azathioprine. An openlung biopsy was obtained in six of the seven cases from which viral, mycoplasma, Legionella, aerobic, anaerobic, AFB and fungal cultures were obtained. In the remaining case, a transbronchial biopsy was available for examination. Bronchial washings and brushings available in three cases and imprint smears from the openlung biopsies were stained with Papanicolaou, hematoxylin and eosin, Toluidine blue, AFB, and Gomori's methenamine silver stains. Formalinfixed lung tissue was embedded in paraffin, sectioned and stained with hematoxylin and eosin, periodic acidschiff, Masson's trichrome, AFB, and Gomori's methenamine silver stains. Small cubes of glutaraldehyde fixed lung tissue were postfixed in osmium tetraoxide, embedded in epoxy resin, thinsectioned in an ultramicrotome, and stained with lead citrate and uranyl acetate. Results Clinical and pathological data in seven patients who developed interstitial lung disease during immunosuppressive therapy with azathioprine are summarized in Table 1. All patients had received a cadaveric renal allograft prior to the development of lowgrade fever, an abnormal chest xray, and a falling p0 2, despite therapy with broadspectrum antibiotics. The chest xray abnormalities consisted of infiltrates that were diffuse and bi Downloaded from 148
2 vol. 82.No. 2 AZATHIOPRINE PNEUMONITIS 149 Table 1. Clinical and Pathologic Data on Seven Cadaveric Renal Allograft Recipients Treated with Azathioprine Distribution of Total Prednisone Consolidation Imuran Dose at Bx Patient/Age/Sex Chest xray Dose (mg) (mg/day) Type of Bx 1/74/M 2/51/M 3/42/F 4/49/F 5/41/F 6/40/F 7/31/M Left Lower Lobe Left Lung , , No. Days After Transplant Transbronchial 130 Bx Pathology DAD DAD Outcome Died two days after biopsy. Autopsy showed superimposed bronchopneumonia and cerebral hemorrhage. Died one day after biopsy. Consolidation did not clear after discontinuance of azathioprine. Consolidation did not clear following discontinuance of azathioprine. Died 30 days post biopsy. Autopsy showed disseminated Aspergillus. Consolidation cleared on discontinuance of azathioprine: alive and well y/i years later. Consolidation cleared following discontinuance of azathioprine and institution of Cytoxan; alive and well four years later. Consolidation cleared following discontinuance of azathioprine and institution of Cytoxan; died one year postbiopsy. Died two days after biopsy. lateral in five patients and diffuse but more severe on one side in the other two patients. No parenchymal cavities, pleural effusions, or focal lesions were noted in any of the cases. Total doses of azathioprine administered before the onset of the infiltrate ranged from 2,850 mg to mg. The infiltrate developed from 35 to 229 days following transplantation and disappeared spontaneously in one patient (patient 4) when azathioprine therapy was discontinued. In two additional patients (patients 5 and 6) the infiltrate disappeared when azathioprine was discontinued and Cytoxan (Mead Johnson, Evansville, IN) was instituted. In four patients (patients 1, 2, 3, and 7) the p0 2 never improved, the infiltrates progressed, and the patients expired despite supportive therapy with a respirator. Results of cultures obtained from the openlung biopsies were negative in all cases. Histopathology lung biopsies in six of the cases revealed changes varying from diffuse alveolar damage (DAD) to usual Table 2. Pulmonary Histopathologic Changes in Seven Patients Receiving Azathioprine Patient Hyaline Membranes _ Intraalveolar Edema _ Cuboidal Hyperplasia Interstitial Fibrosis Atypical Epithelial Cells _ Downloaded from

3 150 BEDROSSIAN ET AL. Downloaded from AJ.C.P. August 1984
. FIG. 2 (lower).")
. interstitial pneumonia () (Table 2).")
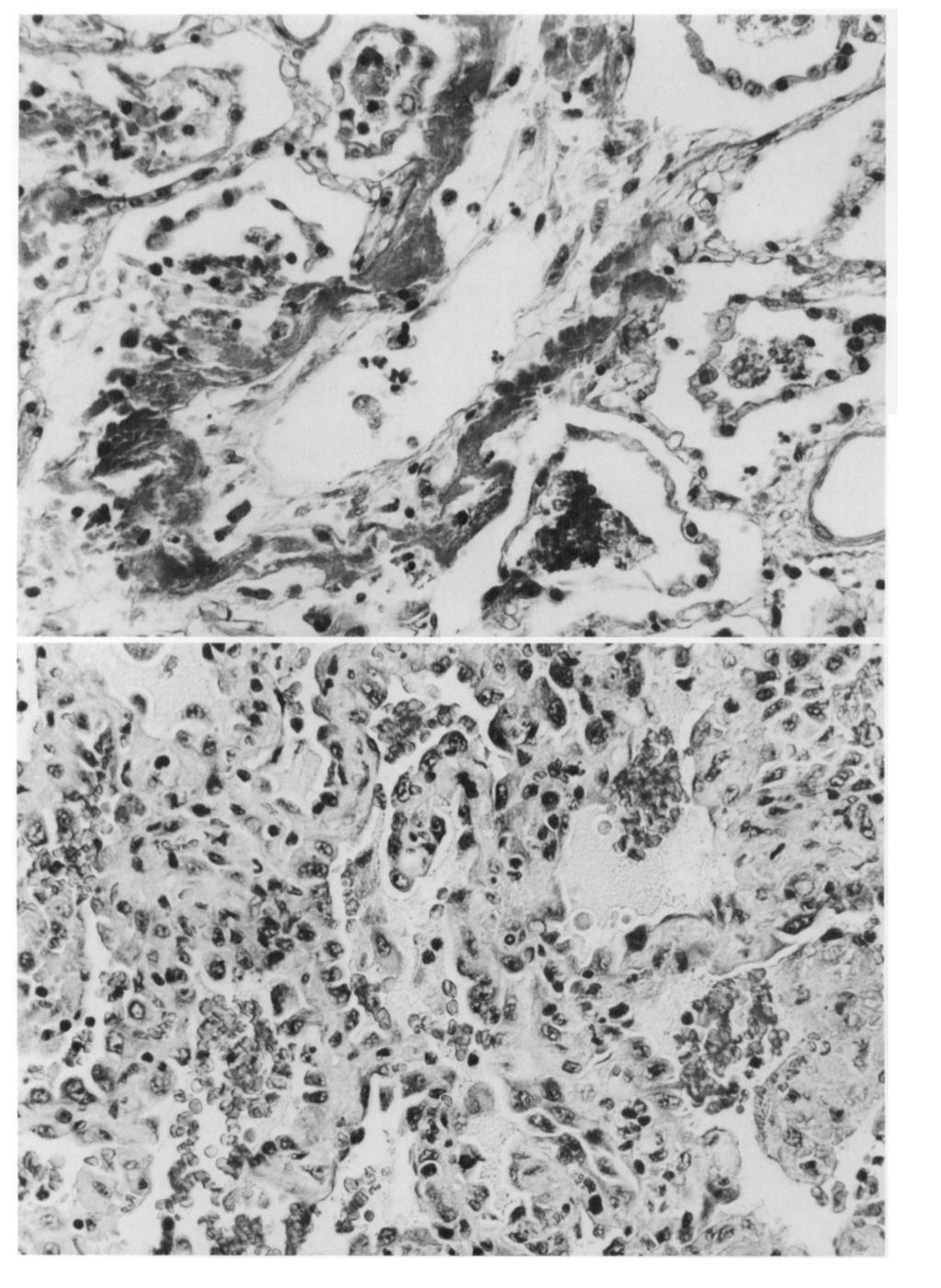
4 Vol. 82 No. 2 AZATHIOPR1NE PNEUMONITIS 151 FIG. 1 (upper). lung biopsy from 49yearold woman who received 4,355 mg azathiopnne. Note interstitial edema, prominent intraalveolar hyaline membranes, and rows of cuboidal cells lining alveoli. Hematoxylin and eosin (X400). FIG. 2 (lower). This is an openlung biopsy in a 42yearold woman who received a total of 28,625 mg of azathiopnne. There is reorganization of distal air spaces, edema,fibrosis,and proliferation of atypical epithelial cells. Hematoxylin and eosin (X400). interstitial pneumonia () (Table 2). DAD was characterized by hyaline membranes, intraalveolar edema, and cuboidalization of alveolar epithelium (Fig. 1). Features of were reorganization of distal air spaces, atypical epithelial hyperplasia, and varying degrees of fibrosis (Fig. 2). No cytoplasmic or intranuclear viral inclusions were seen in any of the cases. The special stains for microorganisms were negative in all cases. There was no evidence of eosinophilia, granulomas, or vasculitis. Acute inflammatory cellular infilrate was not prominent in any of the cases. In one patient (patient 7) transbronchial biopsy showed collapse of air spaces, atypical epithelial hyperplasia, and fibrosis, consistent with. Cytopathology Bronchial washings and brushings in three cases revealed atypical epithelial cells similar to those lining the reorganized distal air spaces in the biopsies. The cytologic characteristics of these cells were better appreciated in the imprint smears prepared from the biopsies and consisted of a crescentic shape, granular cytoplasm without pigmentation, atypical nuclei and prominent nucleoli (Fig. 3). No inclusion bodies were noted in any of the cytologic preparations. Ultrastructure Electron microscopic examination was performed on all six openlung biopsies (Table 3). Electron micrographs revealed intraalveolar edema, fibrin accumulation, air spaces lined predominantly by type II alveolar pneumonocytes, and a marked paucity of type I cells (Fig. 4). The type II cells showed bizarre shapes, prominent 1ammelar bodies, blunted microvilli, and partial extrusion of osmiophilic material. No viral particles were seen. Type FIG. 3. Imprint smear of lung biopsy from same patient as Figure 2. Note atypical cells with crescent shape, nuclei from prominent nucleoli and granular cytoplasm without inclusions. Papanicolaou (X800). Downloaded from

.")
5 152 BEDROSSIAN ET AL. AJ.C.P. August 1984 Table 3. Electron Microscopy in Six Cases of Azathioprineassociated Interstitial Pneumonitis Patient Blebs in Type I Cells Alveolar Edema Fibrin Accumulation I cells, when present, showed minimal bleb formation, whereas endothelial cells appeared intact. The basement membranes did not contain immune deposits. The interstitium showed fibrosis, more pronounced in cases of usual interstitial pneumonia (Fig. 5). Bizarre Type II Cells Collagen/ Fibroblasts Immunopathology Material for immunofluorescence was available in three of six openlung biopies. They were stained with antisera against IgG, IgM, C3, albumin, and fibrinogen. A small ' ' i,, ",. "' FIG. 4. Electron micrograph of lung biopsy from same patient as Figures 2 and 3. Note crescentshaped Type II cells lining alveoli and free in the lumen, with prominent lamellar bodies. Lead citrate and uranyl acetate (X 12,000). Downloaded from
. amount of fibrinogen was noted within alveolar spaces.")

6 AZATHIOPR1NE PNEUMONITIS Vol. 82 No FIG. 5. Another area from same biopsy as Figure 2. The interstitium shows increased collagen,fibroblastsand a macrophage. The basement membranes remain intact. Lead citrate and uranyl acetate (X20.000). amount of fibrinogen was noted within alveolar spaces. However, no staining was noted with the other antisera within epithelial or endothelial alveolar wall basement membranes. Discussion In the transplant patient, pulmonary infections are the most common cause of pulmonary failure and an abnormal chest xray.6 Infections can be of viral, bacterial, fungal or protozoal origin.9 The least recognized cause of respiratory failure in the allograft recipient is toxicity due to the immunosuppressive agent itself. To our knowledge, only two previous case reports have appeared in the literature relating instances of Imuran Downloaded from associated pulmonary toxicity. The first case was a 20yearold man who developed a reticular infiltrate on the chest xray accompanied by bloodgas evidence of restrictive lung disease.8 He had received up to 150 mg/ day of cyclophosphamide over a threemonth period prior to therapy with azathioprine. The second was a 24yearold woman who developed a similar pattern on the chest xray without prior treatment with any known pneumotoxic medication. This second case came to biopsy, which revealed interstitial pulmonary fibrosis with features very similar to those seen in our patients.'' The seven cases reported here all had clinical and pathologic features consistent with azathioprine pulmonary toxicity. All patients developed hypoxia, lowgrade fever, and abnormal chest roentograms following cadav

7 154 BEDROSSIAN ET AL. A.J.C.P. August 1984 eric renal allografts and histologically showed varying degrees of hyaline membranes, intraalveolar edema, atypical hyperplasia of alveolar lining cells, and interstitial fibrosis. All cases were submitted to careful microbiologic cultures and thorough histopathologic examination for viruses, bacteria, and fungi resulting in no significant positive findings. Two patients receiving the lower doses of azathioprine (patients 4, 5) were classified as having diffuse alveolar damage and had a definite better prognosis. In one patient (patient 4) radiographic consolidation cleared following discontinuance of azathioprine. In the other patient (patient 5) discontinuance of azathioprine followed by treatment with Cytoxan was accompanied by clearing of the consolidation. One patient who also received low total dose (patient 6) had on the lung biopsy but had significant clinical improvement when azathioprine was discontinued and Cytoxan instituted. This patient died one year after biopsy. No autopsy was performed. Patients receiving higher doses (patients 1,2,3 and 7) were classified as having usual interstitial pneumonia and all showed some degree of interstitial fibrosis. Three patients (patients 1, 2, and 7) died one to two days after biopsy. Only one case came to autopsy which revealed and superimposed bronchopneumonia. One patient (patient 3) died 30 days after biopsy. In this patient, consolidation did not improve following discontinuance of azathioprine, and death was due to disseminated aspergillosis, which, at autopsy was noted in addition to. In human subjects the diagnosis of druginduced pulmonary toxicity is based on clinical history of drug exposure and absence of other known causative agents. 12 Diffuse interstitial pulmonary disease is by far the most frequent type of lung pathology induced by drugs.' The lesion can be reproduced experimentally by the administration of some of the drugs clinically implicated in pulmonary toxicity. 2,5 The pulmonary alterations, as noted in tissue biopsies, appear to be mediated either by direct, dosedependent toxicity or an allergic mechanism. None of our cases revealed immune deposits as observed in examples of druginduced lung disease believed to occur on an allergic basis. 10 On the other hand, ultrastructural evidence of epithelial damage in the absence of endothelial involvement is indistinguishable from that of previous cases of dosedependent pulmonary drug toxicity examined by electron microscopy. 3 In three of our patients atypical epithelial cells were seen in cytologic specimens at the time abnormalities appeared on chest radiographs. This occurrence also has been noted previously during drug therapy accompanied by pulmonary side effects. 4 These findings suggest that cytology can be useful in monitoring patients receiving potential pneumotoxic drugs. Although the evidence is circumstantial, our findings support the view that azathioprine is capable of causing dosedependent pulmonary toxicity. Broader recognition of this complication and discontinuance of azathioprine in patients who develop acute pulmonary failure in the absence of infection could prevent progression of pulmonary damage in such cases. Addendum. Since the acceptance of our manuscript, another case report of interstitial pneumonitis secondary to azathioprine in a renal transplant patient has appeared in the literature. The lung biopsy changes described by D. J. S. Carmiachel and associates (Thorax 1983; 38: ) are virtually identical to the ones noted in our patients who received the higher doses of Imuran. References 1. Bedrossian CWM: Pathology of druginduced lung diseases. Sem Resp Med 1982;4: Bedrossian CWM, Greenberg SD, Yawn D, O'Neal RM: Experimentally induced bleomycin sulphate pulmonary toxicity. Arch Pathol Lab Med 1977; 101: Bedrossian CWM, Luna MA, MacKay B, Lichtiger B: Ultrastructure of Bleomycin pulmonary toxicity. Cancer 1973; 32: Bedrossian CWM, Corey BJ: Abnormal sputum cytopathology during chemotherapy with Bleomycin. Acta Cytol 1978; 22: Gould VE, Miller S: Sclerosing alveolitis induced by ciclyphosphamide. Am J Pathol 1975; 81: Huertas VE, Port FK, Rozas VV, Niederhuber JE: Pneumonia in recipients of renal allografts. Arch Surg 1976; 111: Rossman M, Bestino J: Axathioprine. Ann Intern Med 1973; 79: Rubin G, Baume P, Vandenberg R: Azathioprine and acute restrictive lung disease. Austr NZ J Med 1972; 3: Rubin RH, Wolfson JS, Cosimi AB, TolkorT NE: Infection in the renal transplant recipient. Am J Med 1981; 70: Smith WR, Dearden LC, McRae DM: Deposits of immunoglobulin and complement in the pulmonary tissue of patients with "heroin lung." Chest 1978;73: Weisenburger DD: Interstitial pneumonitis associated with azathioprine therapy. Am J Clin Pathol 1978; 69: Weiss RR, Muggia FM: Cytotoxic druginduced pulmonary disease: Update Am J Med 1980; 68: Downloaded from
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Open Lung Biopsy for Diffuse Infiltrative Lung Disease
 Open Lung Biopsy for Diffuse Infiltrative Lung Disease Vijay Chechani, MD, Rodney J. Landreneau, MD, and Shabbir S. Shaikh, MD Division of Pulmonary Medicine, Department of Medicine, and Division of Cardiothoracic
Open Lung Biopsy for Diffuse Infiltrative Lung Disease Vijay Chechani, MD, Rodney J. Landreneau, MD, and Shabbir S. Shaikh, MD Division of Pulmonary Medicine, Department of Medicine, and Division of Cardiothoracic
The Acute Vasculitis of Wegener's Granulomatosis in Renal Biopsies
 The Acute Vasculitis of Wegener's Granulomatosis in Renal Biopsies RICHARD. NOVAK, M.D., RICHARD G. CHRISTIANSEN, M.D., AND EWALD T. SORENSEN, M.D. The kidney biopsy specimens fromfivepatients with Wegener's
The Acute Vasculitis of Wegener's Granulomatosis in Renal Biopsies RICHARD. NOVAK, M.D., RICHARD G. CHRISTIANSEN, M.D., AND EWALD T. SORENSEN, M.D. The kidney biopsy specimens fromfivepatients with Wegener's
Case 4 History. 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar
 Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology
 Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology G. BERRY SCHUMANN, M.D., LAWRENCE J. PALMIERI, B.S., C.T.(ASCP), AND DAVID B. JONES, M.D. Schumann, G. Berry, Palmieri, Lawrence
Differentiation of Renal Tubular Epithelium in Renal Transplantation Cytology G. BERRY SCHUMANN, M.D., LAWRENCE J. PALMIERI, B.S., C.T.(ASCP), AND DAVID B. JONES, M.D. Schumann, G. Berry, Palmieri, Lawrence
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nitrofurantoin-Induced Lung Toxicity
 Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
Non-neoplastic Lung Disease II
 Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Light and electron microscopical studies of focal glomerular sclerosis
 J. clin. Path., 1971, 24, 846-850 Light and electron microscopical studies of focal glomerular sclerosis A. H. NAGI, F. ALEXANDER, AND R. LANNIGAN From the Department of Pathology, Queen's University of
J. clin. Path., 1971, 24, 846-850 Light and electron microscopical studies of focal glomerular sclerosis A. H. NAGI, F. ALEXANDER, AND R. LANNIGAN From the Department of Pathology, Queen's University of
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Antibody-Mediated Rejection in the Lung Allograft. Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305
 Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Organizing Pneumonia And Diffuse Alveolar Damage: An Incidental Finding In An Immunocompromised Patient By EBUS-FNA
 ISPUB.COM The Internet Journal of Pathology Volume 17 Number 1 Organizing Pneumonia And Diffuse Alveolar Damage: An Incidental Finding In An Immunocompromised Patient By EBUS-FNA B Lowenthal, F Hasteh
ISPUB.COM The Internet Journal of Pathology Volume 17 Number 1 Organizing Pneumonia And Diffuse Alveolar Damage: An Incidental Finding In An Immunocompromised Patient By EBUS-FNA B Lowenthal, F Hasteh
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia)
 (Lynne S. Garcia)") PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia) A 46-year-old man with AIDS was admitted to the hospital for complaints of a persisting fever and dry cough. A chest radiograph showed bilateral
PARASITOLOGY CASE HISTORY 10 (HISTOLOGY) (Lynne S. Garcia) A 46-year-old man with AIDS was admitted to the hospital for complaints of a persisting fever and dry cough. A chest radiograph showed bilateral
New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma
 July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
LADIS Case of the Month
 November 2018 LADIS Case of the Month Drs Valentin Janvier and Brieuc Cossic Hospital for Animals and Animal Health Diagnostic Center Signalment and presenting complaint 13 year old Thoroughbred gelding
November 2018 LADIS Case of the Month Drs Valentin Janvier and Brieuc Cossic Hospital for Animals and Animal Health Diagnostic Center Signalment and presenting complaint 13 year old Thoroughbred gelding
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Inflammation class 2. Inflammation part 2. Rheumatic fever RF. Rheumatic fever - pathogenesis. Hypersensitivity reactions. Rheumatic fever RF
 Inflammation class 2 Inflammation part 2 Rheumatic endocarditis Pneumocystis carinii pneumonia Cytomegalic pneumonia Aspergillosis Actinomycosis Rheumatic fever RF An acute, immunologically mediated multisystem
Inflammation class 2 Inflammation part 2 Rheumatic endocarditis Pneumocystis carinii pneumonia Cytomegalic pneumonia Aspergillosis Actinomycosis Rheumatic fever RF An acute, immunologically mediated multisystem
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
NONE OVERVIEW FINANCIAL DISCLOSURES UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF (UIP) FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP
 FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP") UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
Radiologic findings of drug-induced lung disease
 Radiologic findings of drug-induced lung disease Poster No.: P-0115 Congress: ESTI 2015 Type: Educational Poster Authors: A. I. C. Santos, A. F. Roque, R. Mamede, L. Oliveira, T. Saldanha; Lisbon/PT Keywords:
Radiologic findings of drug-induced lung disease Poster No.: P-0115 Congress: ESTI 2015 Type: Educational Poster Authors: A. I. C. Santos, A. F. Roque, R. Mamede, L. Oliveira, T. Saldanha; Lisbon/PT Keywords:
Radiation Pneumonitis Joseph Junewick, MD FACR
 Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
A 72-year-old male with worsening interstitial infiltrates and respiratory failure
 A 72-year-old male with worsening interstitial infiltrates and respiratory failure Case report On November 24, 2004, a 72-year-old male was admitted to the medical intensive care unit (ICU) with a history
A 72-year-old male with worsening interstitial infiltrates and respiratory failure Case report On November 24, 2004, a 72-year-old male was admitted to the medical intensive care unit (ICU) with a history
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Examination of the light microscopic slide of renal biopsy specimens by utilizing Low-vacuum scanning electron microscope
 SCIENTIFIC INSTRUMENT NEWS 2017 Vol. 9 SEPTEMBER Technical magazine of Electron Microscope and Analytical Instruments. Article Examination of the light microscopic slide of renal biopsy specimens by utilizing
SCIENTIFIC INSTRUMENT NEWS 2017 Vol. 9 SEPTEMBER Technical magazine of Electron Microscope and Analytical Instruments. Article Examination of the light microscopic slide of renal biopsy specimens by utilizing
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Déjà vu all over again
 Disclosures Déjà vu all over again None Jonathan Singer MD MS University of California, San Francisco HPI 49 y/o woman presents for lung transplant evaluation for Hypersensitivity Pneumonitis Exposures:
Disclosures Déjà vu all over again None Jonathan Singer MD MS University of California, San Francisco HPI 49 y/o woman presents for lung transplant evaluation for Hypersensitivity Pneumonitis Exposures:
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Pulmonary Vascular Disease in Systemic Lupus Erythematosus
 Pulmonary Vascular Disease in Systemic Lupus Erythematosus A. OLUSEGUN FAYEMI, M.D.* Department of Pathology, The Mount Sinai School of Medicine of the City University of New York, New York, New York 129
Pulmonary Vascular Disease in Systemic Lupus Erythematosus A. OLUSEGUN FAYEMI, M.D.* Department of Pathology, The Mount Sinai School of Medicine of the City University of New York, New York, New York 129
Imaging Cancer Treatment Complications in the Chest
 Imaging Cancer Treatment Complications in the Chest Michelle S. Ginsberg, MD Objectives Imaging Cancer Treatment Complications in the Chest To understand the mechanisms of action of different classes of
Imaging Cancer Treatment Complications in the Chest Michelle S. Ginsberg, MD Objectives Imaging Cancer Treatment Complications in the Chest To understand the mechanisms of action of different classes of
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Bronkhorst colloquium Interstitiële longziekten. Katrien Grünberg, klinisch patholoog
 Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
Part I Study Questions
 Part I Study Questions 1. A 59-year-old man with a history of pulmonary embolism diagnosed 2 years ago and treated with warfarin for 6 months is evaluated for progressive dyspnea and bilateral lower extremity
Part I Study Questions 1. A 59-year-old man with a history of pulmonary embolism diagnosed 2 years ago and treated with warfarin for 6 months is evaluated for progressive dyspnea and bilateral lower extremity
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentation: S.A is 25 years old. Referred to a gastroentrologist because of abdominal pain and bloody diarrhea in the last few weeks.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentation: S.A is 25 years old. Referred to a gastroentrologist because of abdominal pain and bloody diarrhea in the last few weeks.
Using the Ch6diak-Higashi Marker
 A Study of the Origin of Pulmonary Macrophages Using the Ch6diak-Higashi Marker Kent J. Johnson, MD, Peter A. Ward, MD, Gary Striker, MD, and Robin Kunkel, MS Using bone marrow reconstitution techniques
A Study of the Origin of Pulmonary Macrophages Using the Ch6diak-Higashi Marker Kent J. Johnson, MD, Peter A. Ward, MD, Gary Striker, MD, and Robin Kunkel, MS Using bone marrow reconstitution techniques
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Pathology lab 4 DONE BY : MORAD ABU QAMAR
 Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Pathology lab 4 DONE BY : MORAD ABU QAMAR Chronic interstitial inflammation, lung Certain etiologic agents such as viruses are more likely to lead to chronic inflammation, as seen here in the lung of a
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
2046: Fungal Infection Pre-Infusion Data
 2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
Radiological Imaging of Drug-Induced Pulmonary Lesions
 Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Cryptogenic Organising Pneumonia As The Initial Presenting Manifestation of SLE
 BMH Medical Journal 2015;2(3):79-83 Case Report Cryptogenic Organising Pneumonia As The Initial Presenting Manifestation of SLE Neena Mampilly MD, G Manoj MD, Binoy J Paul MD, PhD, DNB, FRCP Baby Memorial
BMH Medical Journal 2015;2(3):79-83 Case Report Cryptogenic Organising Pneumonia As The Initial Presenting Manifestation of SLE Neena Mampilly MD, G Manoj MD, Binoy J Paul MD, PhD, DNB, FRCP Baby Memorial
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Slide 120, Lobar Pneumonia. Slide 120, Lobar Pneumonia. Slide 172, Interstitial Pneumonia. Slide 172, Interstitial Pneumonia. 53 Year-Old Smoker
 Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
Slide 120, Lobar Pneumonia Slide 120, Lobar Pneumonia Slide 172, Interstitial Pneumonia Slide 172, Interstitial Pneumonia 53 Year-Old Smoker Emphysema Pink puffer Barrel chest Hyperinflation Trapped air
NEPHROTIC SYNDROME OF ACQUIRED SYPHILIS-A MORPHOLOGICAL AND ULTRASTRUCTURAL STUDY
 NEPHROTIC SYNDROME OF ACQUIRED SYPHILIS-A MORPHOLOGICAL AND ULTRASTRUCTURAL STUDY Abstract Pages with reference to book, From 3 To 7 A.H. Nagi, I.A. Naveed, A. Rashid ( Department of Pathology, Allama
NEPHROTIC SYNDROME OF ACQUIRED SYPHILIS-A MORPHOLOGICAL AND ULTRASTRUCTURAL STUDY Abstract Pages with reference to book, From 3 To 7 A.H. Nagi, I.A. Naveed, A. Rashid ( Department of Pathology, Allama
ARDS during Neutropenia. D Mokart DAR IPC GRRRRROH 2010
 ARDS during Neutropenia D Mokart DAR IPC GRRRRROH 2010 Definitions Neutropenia is a decrease in circulating neutrophil white cells in the peripheral blood. neutrophil count of 1,000 1,500 cells/ml = mild
ARDS during Neutropenia D Mokart DAR IPC GRRRRROH 2010 Definitions Neutropenia is a decrease in circulating neutrophil white cells in the peripheral blood. neutrophil count of 1,000 1,500 cells/ml = mild
Introduction. 23 rd Annual Seminar in Pathology. FLUIDS, Part 1. Pittsburgh, PA Gladwyn Leiman UVMMC, VT
 23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
23 rd Annual Seminar in Pathology Pittsburgh, PA Gladwyn Leiman UVMMC, VT FLUIDS, Part 1 "Blue walls", Claudia Hansen, 2009 Introduction o Challenging to everyone o Almost any benign or malignant process
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Chapter 8. Other Important Tests and Procedures. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 8 Other Important Tests and Procedures 1 Introduction Additional important diagnostic studies include: Sputum examination Skin tests Endoscopic examination Lung biopsy Thoracentesis Hematology,
Chapter 8 Other Important Tests and Procedures 1 Introduction Additional important diagnostic studies include: Sputum examination Skin tests Endoscopic examination Lung biopsy Thoracentesis Hematology,
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
HISTO-PHYSIOLOGY HISTO-PHYSIOLOGY HISTO-PHYSIOLOGY. 09-Mar-15. Dr. Muhammad Tariq Javed. RESPIRATORY SYSTEM Lec-1
 RESPIRATORY SYSTEM Lec-1 Dr. Muhammad Tariq Javed Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: http://www.geocities.ws/mtjaved 1 2 Conducting
RESPIRATORY SYSTEM Lec-1 Dr. Muhammad Tariq Javed Professor Department of Pathology, University of Agriculture, Faisalabad. Email: mtjaved@uaf.edu.pk Web: http://www.geocities.ws/mtjaved 1 2 Conducting
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Periodic Acid-Schiff-Light Green Stain to Detect Glomerular Protein Deposits by Routine Light Microscopy
 Periodic Acid-Schiff-Light Green Stain to Detect Glomerular Protein Deposits by Routine Light Microscopy CHARLES N. GAMBLE, M.D. Department of Pathology, Sutter Memorial Hospital, Sacramento, California
Periodic Acid-Schiff-Light Green Stain to Detect Glomerular Protein Deposits by Routine Light Microscopy CHARLES N. GAMBLE, M.D. Department of Pathology, Sutter Memorial Hospital, Sacramento, California
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Pneumocystis Pneumonia. Dr. Pradeep kumar II yr Pulmonary Medicine
 Pneumocystis Pneumonia Dr. Pradeep kumar II yr Pulmonary Medicine PNEUMOCYSTIS CARINII PNEUMONIA Pneumocystis carinii pneumonia (PCP), is commonly termed Pneumocystis jiroveci pneumonia, is the 2 nd most
Pneumocystis Pneumonia Dr. Pradeep kumar II yr Pulmonary Medicine PNEUMOCYSTIS CARINII PNEUMONIA Pneumocystis carinii pneumonia (PCP), is commonly termed Pneumocystis jiroveci pneumonia, is the 2 nd most
Interstitial Inflammation
 Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
Nonspecific Interstitial Pneumonitis: A Common Cause of Pulmonary Disease in the Acquired Immunodeficiency Syndrome
 Nonspecific Interstitial Pneumonitis: A Common Cause of Pulmonary Disease in the Acquired Immunodeficiency Syndrome ANTHONY F. SUFFREDINI, M.D.; FREDERICK P. OGNIBENE, M.D.; ERNEST E. LACK, M.D.; J. THAYER
Nonspecific Interstitial Pneumonitis: A Common Cause of Pulmonary Disease in the Acquired Immunodeficiency Syndrome ANTHONY F. SUFFREDINI, M.D.; FREDERICK P. OGNIBENE, M.D.; ERNEST E. LACK, M.D.; J. THAYER
DRUG INDUCED LUNG DISEASES
 DRUG INDUCED LUNG DISEASES CHEMOTHERAPEUTIC AGENTS 1. CYTOTOXIC ANTIBIOTICS 2. ALKYLATING AGENTS 3. ANTIMETABOLITES 4. BIOLOGIC RESPONSE MODIFIERS CYTOTXIC ANTIBIOTICS BLEOMYCIN 1.CHRONIC PNEUMONITIS/
DRUG INDUCED LUNG DISEASES CHEMOTHERAPEUTIC AGENTS 1. CYTOTOXIC ANTIBIOTICS 2. ALKYLATING AGENTS 3. ANTIMETABOLITES 4. BIOLOGIC RESPONSE MODIFIERS CYTOTXIC ANTIBIOTICS BLEOMYCIN 1.CHRONIC PNEUMONITIS/
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
CHRONIC INFLAMMATION
 CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
Atlas of Stains. Special Stains on Artisan Link Pro
 Atlas of Stains Special Stains on Artisan Link Pro Intended use Routinely processed samples (paraffin-embedded) may be used. The preferred fixative is neutral buffered formalin. The clinical interpretation
Atlas of Stains Special Stains on Artisan Link Pro Intended use Routinely processed samples (paraffin-embedded) may be used. The preferred fixative is neutral buffered formalin. The clinical interpretation
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference. Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2
 June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host
 Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Thin-Section CT Findings in 32 Immunocompromised Patients with Cytomegalovirus Pneumonia Who Do Not Have AIDS
 Tomás Franquet 1,2 Kyung S. Lee 3 Nestor L. Müller 1 Received January 27, 2003; accepted after revision April 21, 2003. 1 Department of Radiology, Vancouver Hospital and Health Sciences Center and University
Tomás Franquet 1,2 Kyung S. Lee 3 Nestor L. Müller 1 Received January 27, 2003; accepted after revision April 21, 2003. 1 Department of Radiology, Vancouver Hospital and Health Sciences Center and University
Reparatory system 18 lectures Heyam Awad
 Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Study of systemic fungal infections in renal transplant recipients
 Original Research Article Study of systemic fungal infections in renal transplant recipients N.D. Srinivasaprasad 1*, G. Chandramohan 1, M. Edwin Fernando 2 1 DM (Nephrology), Assistant Professor, 2 DM
Original Research Article Study of systemic fungal infections in renal transplant recipients N.D. Srinivasaprasad 1*, G. Chandramohan 1, M. Edwin Fernando 2 1 DM (Nephrology), Assistant Professor, 2 DM
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection. Masoud Mardani M.D,FIDSA
 Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Mammary Nodular Hyperplasia in Intact R hesus Monkeys
 Vet. Path. 10: 130-134 (1973) Mammary Nodular Hyperplasia in Intact R hesus Monkeys L. W NELSON and L. D. SHOTT Department of Pathology and Toxicology, Mead Johnson Research Center, Evansville, Ind., and
Vet. Path. 10: 130-134 (1973) Mammary Nodular Hyperplasia in Intact R hesus Monkeys L. W NELSON and L. D. SHOTT Department of Pathology and Toxicology, Mead Johnson Research Center, Evansville, Ind., and
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish