Lung Transplant Case Presentation
|
|
|
- Melina Hopkins
- 5 years ago
- Views:
Transcription


1 Lung Transplant Case Presentation Errol L. Bush, MD Assistant Professor of Surgery Heart and Lung Transplantation UCSF Medical Center Update in Advanced Lung Disease May 9, 2015 LP 47y F never smoker w/ LAM at age 19 Bilateral pneumothorax Left tetracycline pleurodesis 1986 R talc pleurodesis 2000 PRA % Class I, 74% Class II % Class I, 63% Class II 1

2 LP 47y F never smoker w/ LAM at age 19 Bilateral pneumothorax Left tetracycline pleurodesis 1986 R talc pleurodesis 2000 PRA % Class I, 74% Class II % Class I, 63% Class II Bilateral lung transplant w/o bypass 2 hours lysisof adhesions Extrapleural pneumonectomies 3U PRBC 2




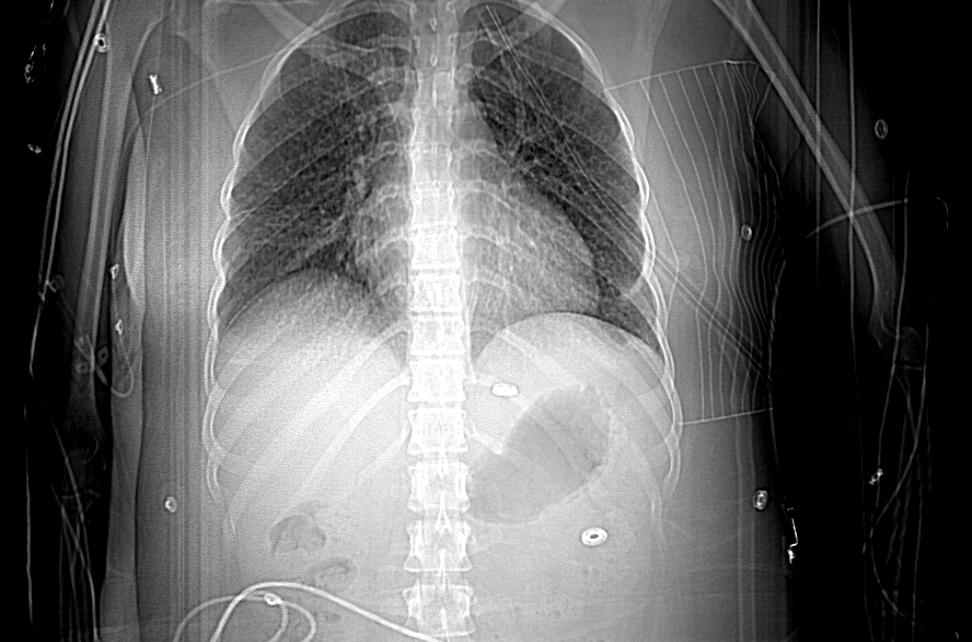
3 Chest tube placed CT chest 3



4 Chest tube placed CT chest VATS lung BX LAM d/c home after 2 weeks, on home O2 2 weeks later Desaturations -> ER 4




5 5


6 2 weeks later Desaturations -> ER Transferred to tertiary center Tachypnea->AMS w/ hypoxia and hypercarbia Intubated 12 minspea arrest L needle decompression with chest tube Improved hemodynamics R chest tube 2 weeks later Desaturations -> ER Transferred to tertiary center Tachypnea->AMS w/ hypoxia and hypercarbia Intubated 12 mins PEA arrest L needle decompression with chest tube Improved hemodynamics R chest tube D/c Home after 3 week hospitalization and heimlech valve Oxygen 4L at rest, 6L for ambulation Expedited transplant evaluation mostly complete 2 weeks later Home: extreme SOB, intermittent hypoxia. Found on the sidewalk tachypneic, hypoxic, and tachycardicto 140s and brought straight to ER. 6



7 Secondary Spontaneous Pneumothorax Pneumothorax that occurs as a complication of underlying lung disease Most commonly Chronic obstructive pulmonary disease, cystic fibrosis, primary or metastatic lung malignancy, and necrotizing pneumonia 70% COPD 50 percent likelihood of recurrent SSP over three years among patients with a SSP due to COPD 7



8 Treatment Hospitalization Underlying lung disease increases the risk for an adverse outcome Supplemental Oxygen Stabilization with pleural drainage Referral to Lung transplant center Further therapy? 18y F with cystic fibrosis and SSPx 10d air leak EBV placed Tube removed in 5 days d/c home 3 days later, recurrent PTx Lung transplant 1 month following EBV 8


9 Thank you 9
10 CL 48y M Peruvian immigrant aquarium cleaner with acute hypoxic respiratory failure Recently hospitalized for mycobacterial facial cellulitis and left lower lobe pneumonia Six months earlier had facial cellulitis Soft tissue only by MRI, despite abx T-4m noted cough and SOB CXR w/ LLL pneumonia, Moxifloxacin» Only facial improvement, added minocycline T-2m daily fevers, pulmonary process worsens T-1m hospitalized, VATS bx Organizing pneumonia w/ acute lung injury and fibrosis» Steroids, Abs CL Next Steps? 48y M Peruvian immigrant aquarium cleaner with acute hypoxic respiratory failure Recently hospitalized for mycobacterial facial cellulitis and left lower lobe pneumonia Six months earlier had facial cellulitis Soft tissue only by MRI, despite abx T-4m noted cough and SOB CXR w/ LLL pneumonia, Moxifloxacin» Only facial improvement, added minocycline T-2m daily fevers, pulmonary process worsens T-1m hospitalized, VATS bx Organizing pneumonia w/ acute lung injury and fibrosis» Steroids, Abs 10

11 CL continued 48y M Peruvian immigrant aquarium cleaner with acute hypoxic respiratory failure F/u pulmonologist: hypoxic, SOB, significant weight loss 2 week hospitalization 2L NC -> NRB Failed high dose steroids, cellcept» Intubation Oscillator» Oxygen saturations only in 80s Now what? Admission CXR CL 48y M w/ DAD/AIP txfrom CPMC on VA ECMO 6/8 Concern: drug-induced DAD in setting of 3 drug therapy for mycobacterial skin infxn vs cryptogenic organizing PNA. RIJ->R CFA VA ECMO 6/14/10 RIJ->LCFV VV ECMO Agitation w/ neuro checks -> flow disturbances 6/18 RIJ->PA VV ECMO Chest left open 6/20 RA->PA tunneled VV ECMO w/ chest closure?6/22 RIJ/RCFV to RCFA VA ECMO 6/25 weight bearing; listed for lung transplant 7/5 BOLT on CPB 7/12 Washout for R empyema 7/22 dysphagia, continue TF 8/2 tx floor 8/12 tracheostomy closure 8/17 perc GJ and passed swallow, but no motivation 8/20 d/c home 9/30 L groin seroma evacuation 11
12 WJ 64y M with IPF and hypoxemic failure Planned outpatient appointment later in week ED Progressive dyspnea, multiple ED visits SpO290% on 8LPM and 70s with exertion ABG 7.46/36/51 on 8L high flow BiPAPand HFNC 15 L/min No infections or heart failure Solumedrol, levaquin, spiriva, budesonide, nebs, PPI admitted 8/27 SpO2 low 80's on HFNC 15L ->supplemental NRB Exam BP 118/79, HR 107, T 36.4, SpO % on 25L HFNC and NRB 100% A&OX3 Spoke four to five word sentences Moderate distress, rapid and abdominal breathing to the mid 30 s, desaturatedwith any movement or talking. ABG 7.47/39/158 on high flow 25L and NRB Transferred to ICU Intubated/Paralyzed 9/5 Course 9/6 Perc Trach Awakened from sedation and paralytics were weaned off. Minimal exertion caused desaturations to the 60s with poor recovery PA pressure 61/21 (34) on swan NO did not reduce the PA pressure on swan Hypoxemia and respiratory instability requiring urgent ECMO 9/11 BOLT 12

13 13
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Management of Respiratory Failure: The Surgical Perspective. When Traditional Respiratory Support Techniques fail. ARDS: Evidence Based Practice
 Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Correspondence should be addressed to Haris Kalatoudis;
 Hindawi Case Reports in Critical Care Volume 2017, Article ID 3092457, 4 pages https://doi.org/10.1155/2017/3092457 Case Report Bronchopleural Fistula Resolution with Endobronchial Valve Placement and
Hindawi Case Reports in Critical Care Volume 2017, Article ID 3092457, 4 pages https://doi.org/10.1155/2017/3092457 Case Report Bronchopleural Fistula Resolution with Endobronchial Valve Placement and
The diagnosis and management of pneumothorax
 Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
MRSA pneumonia mucus plug burden and the difficult airway
 Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
Case report Crit Care Shock (2016) 19:54-58 MRSA pneumonia mucus plug burden and the difficult airway Ann Tsung, Brian T. Wessman An 80-year-old female with a past medical history of chronic obstructive
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong
 Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
Working in partnership Quality Care Innovation lead clinician for integrated respiratory service georges ng* man kwong chest physician pronounced ning qualified 1990 chief clinical information officer
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Original Research. Mummadi, Srinivas; Pack, Sasheen; Hahn, Peter
 The Official Journal of the International Society of Pleural Diseases Original Research The Use of Bronchoscopic Oxygen Insufflation to Isolate Persistent Air Leaks in Secondary Pneumothorax Due to COPD
The Official Journal of the International Society of Pleural Diseases Original Research The Use of Bronchoscopic Oxygen Insufflation to Isolate Persistent Air Leaks in Secondary Pneumothorax Due to COPD
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
SURGERY FOR GIANT BULLOUS EMPHYSEMA
 SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Systems differ in their ability to deliver optimal humidification
 Average Absolute Humidity (mg H 2 O/L) Systems differ in their ability to deliver optimal humidification 45 Flows Tested 40 35 30 Optiflow Airvo 2 Vapotherm Vapotherm 5 L/min 10L/min 20L/min 30L/min 40L/min
Average Absolute Humidity (mg H 2 O/L) Systems differ in their ability to deliver optimal humidification 45 Flows Tested 40 35 30 Optiflow Airvo 2 Vapotherm Vapotherm 5 L/min 10L/min 20L/min 30L/min 40L/min
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
The Crashing Pediatric Patient: Stopping the Fall
 The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
Surgical Complication, or Not, That Is the Question
 Surgical Complication, or Not, That Is the Question Adriane Martin, DO, FACOS, CCDS Vice President Enjoin This is the Full Title of a Session Eads, TN 1 Learning Objectives At the completion of this educational
Surgical Complication, or Not, That Is the Question Adriane Martin, DO, FACOS, CCDS Vice President Enjoin This is the Full Title of a Session Eads, TN 1 Learning Objectives At the completion of this educational
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Pneumothorax and Chest Tube Problems
 Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
Pneumothorax and Chest Tube Problems Pneumothorax Definition Air accumulation in the pleural space with secondary lung collapse Sources Visceral pleura Ruptured esophagus Chest wall defect Gas-forming
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Respiratory Care and Organ Donation
 Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
BASIC CRITICAL CARE OF THE PATIENT. Hannelisa Callisen PA C February 2017
 BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Overview Definition of NIV and AHF
 Overview Definition of NIV and AHF NIV related changes in mortality NIV related patient benefits Clinical summary and cases NIV in AHF in Switzerland, a short questionaire Definition of NIV and AHF AHF=
Overview Definition of NIV and AHF NIV related changes in mortality NIV related patient benefits Clinical summary and cases NIV in AHF in Switzerland, a short questionaire Definition of NIV and AHF AHF=
Top Tips for Pleural Disease in 2012
 Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
Top Tips for Pleural Disease in 2012 The unilateral pleural effusion on the Post Take Ward Round Pleural Effusion on CXR Bedside ultrasound + Pleural aspirate Empyema Nil evidence infection Admit IV antibiotics
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
The Role of ECMO in Thoracic Surgery. Matthew Hartwig, MD
 The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS
 Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS SpR Training Day 07.07.14 Dr Alex West Consultant Chest/Pleural Physician Guy s and St Thomas Hospital Medical Thoracoscopy? No Just
Medical Thoracoscopy When to Choose Over a General Anaesthetic VATS SpR Training Day 07.07.14 Dr Alex West Consultant Chest/Pleural Physician Guy s and St Thomas Hospital Medical Thoracoscopy? No Just
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Central Sleep Apnea Problem Based Learning Module
 Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
Central Sleep Apnea Problem Based Learning Module Vidya Krishnan, and Sutapa Mukherjee for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee 2015 Case Section I A 75 year old
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
Chris Cameron Clinical pharmacologist & General Physician CCDHB. Oxygen- A prescribing Blindspot?
 Chris Cameron Clinical pharmacologist & General Physician CCDHB Oxygen- A prescribing Blindspot? Ms J, 70yo Lives with partner, who has a recent diagnosis of breast cancer Works 3 days a week Weight 46kg
Chris Cameron Clinical pharmacologist & General Physician CCDHB Oxygen- A prescribing Blindspot? Ms J, 70yo Lives with partner, who has a recent diagnosis of breast cancer Works 3 days a week Weight 46kg
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Living with rare lung disease LYMPHANGIOLEIOMYOMATOSIS (LAM): The Patient Perspective. Gill Hollis, Edinburgh January 2010
: The Patient Perspective. Gill Hollis, Edinburgh January 2010") Living with rare lung disease LYMPHANGIOLEIOMYOMATOSIS (LAM): The Patient Perspective Gill Hollis, Edinburgh January 2010 LAM Basics Disease of the lungs and lymphatics Affects women Causes progressive
Living with rare lung disease LYMPHANGIOLEIOMYOMATOSIS (LAM): The Patient Perspective Gill Hollis, Edinburgh January 2010 LAM Basics Disease of the lungs and lymphatics Affects women Causes progressive
Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600
 Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
Indications for prolongation of ECMO into the early postoperative period in lung transplantation How we do it
 Indications for prolongation of ECMO into the early postoperative period in lung transplantation How we do it W Klepetko, MD Professor of Thoracic Surgery HEAD: DIVISION OF THORACIC SURGERY MEDICAL UNIVERSITY
Indications for prolongation of ECMO into the early postoperative period in lung transplantation How we do it W Klepetko, MD Professor of Thoracic Surgery HEAD: DIVISION OF THORACIC SURGERY MEDICAL UNIVERSITY
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Candidate. Within the 8 minutes you are required to do the following:
 Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Where do we come from?
 Interdisciplinary Decision-Making with Patients Requiring Tracheostomy and Carrie Windhorst MS CCC-SLP Cheryl Wagoner MS CCC-SLP Ricque Harth MEd CCC-SLP Where do we come from? Welcome to Madonna Rehabilitation
Interdisciplinary Decision-Making with Patients Requiring Tracheostomy and Carrie Windhorst MS CCC-SLP Cheryl Wagoner MS CCC-SLP Ricque Harth MEd CCC-SLP Where do we come from? Welcome to Madonna Rehabilitation
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด
 Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
S and secondary spontaneous pneumothorax. Primary
 Secondary Spontaneous Pneumothorax Fumihiro Tanaka, MD, Masatoshi Itoh, MD, Hiroshi Esaki, MD, Jun Isobe, MD, Youichiro Ueno, MD, and Ritsuko Inoue, MD Department of Thoracic and Cardiovascular Surgery,
Secondary Spontaneous Pneumothorax Fumihiro Tanaka, MD, Masatoshi Itoh, MD, Hiroshi Esaki, MD, Jun Isobe, MD, Youichiro Ueno, MD, and Ritsuko Inoue, MD Department of Thoracic and Cardiovascular Surgery,
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Sleep and Neuromuscular Disease. Sharon De Cruz, MD Tisha Wang, MD
 Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis. Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine
 Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Wheezy? Easy Peasy! The Emergent Management of Asthma & Bronchiolitis Maneesha Agarwal MD Assistant Professor of Pediatrics & Emergency Medicine Asthma Defined National Asthma Education and Prevention
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Tracheostomy Sim Course
 Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD?
 Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Long Term Support for Respiratory Failure: VV ECMO or Oxygenated RVAD? Mechanical Circulatory Support Symposium 2018 (Houston, TX) Charles Hoopes, MD Professor of Surgery University of Alabama (Birmingham)
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions