What we will talk about
|
|
|
- Nathan Warren
- 5 years ago
- Views:
Transcription


1 Surgical Neuropathology: Avoiding pitfalls at frozen section and Immunochemistry that really helps Arizona Society of Pathologists Fall 2013 Stephen W. Coons MD Barrow Neurological Institute Beauregard Mason Dixon Georgia What we will talk about Artifacts Use of smears How to look at smears and FS Sampling issues: Next to Immunochemistry for neuropathology Abscess v GBM Tumor v Demyelinating Recurrence v Treatment effect Meningioma and SFT 1



2 Cautery artifact Freeze artifact 2
 Interpretation: Does it smear well?")





3 Principles of the smear/crush preparation Amount: 1mm 3 Never more than 1/3 of biopsy Goal: Lineage/cell population(s) Interpretation: Does it smear well? Yes = brain No = fibrous (e.g. meningioma, schwannoma) Are their processes? Yes Astrocytes No Oligodendrocytes, epithelial, etc. Single cells? Yes Glial/Brain Clusters Epithelial, meningothelial Predominant population? Does it belong? Atypia? Look at the background Necrosis, hemorrhage, inflammation, neuropil, etc. Don t try to do too much Cellularity hard to predict Account for everything! Don t ignore the naked nuclei because you see some cells with processes White matter Smears easily/well Predominant population of small round nuclei w/ even chromatin Granulo-fibrillary background with vague linear orientation Smears easily/well Smooth to wispy granulofibrillary background with diffuse distribution Gray matter Mixed population of small round nuclei, larger ovoid nuclei and large round nuclei 3


 Typical brain")
 or")



4 Astrocytic processes Identification of the presence or absence of glial/ astrocytic processes is one of most important observations in smear/crush preparations. Astrocytic (+) v nonastrocytic ( ) tumors Gliosis (seen here) Typical brain granulofibrillary pale background with mixed cell populations (gray matter) or oligodendrocytepredominant (white matter) Scattered cells with larger ovoid nuclei and numerous obvious processes extending from eosinophilic cell body Glial processes - Astrocytomas Most cells have prominent dense/solid eosinophilic processes. May be bipolar, unipolar With or without prominent cell body 4








5 Oligodendroglioma No processes Predominant population of monotonous round-to-oval nuclei without processes Background is typical granulo-fibrillary matrix of white matter These are NOT glial processes: pale not strongly eosinophilic Wispy or granulofibrillary, not dense/solid Test our new skills 5






6 Anaplastic astrocytoma Smear: Although not as widespread or prominent as our examples, some cells had definite solid eosinophilic processes. Frozen section: Markedly hypercellular population of diffusely distributed atypical cells. And again 6





7 Oligodendroglioma Smear: Round cells without processes. Cells are larger than background oligodendrocytes and with more open nuclei Frozen section: Diffuse moderately hypercellular proliferation/infiltrate in a background of preserved parenchyma Predominant population matches the smear Processes or Stretched cell body? Non-glial tumors with a fibrous stroma will occasional smear well, particularly when the tumor is highly cellular (less stroma). In this setting, the smear process will stretch the cell body cytoplasm in a pattern that mimics glial processes. Although sometimes tricky, this differentiation is critical to determining tumor lineage particularly in cases with obscuring artifacts on the sections. Glial processes: dense strongly eosinophilic Cytoplasm/cell body: Pale, wispy. May have railroad track dual densities along edges 7





8 Smear/Crush prep Meningioma Variable cohesive pattern Stretched cell bodies; no processes Variable mixed population of epithelioid and spindle cells Epithelioid cells in nests/lobules Small whorled nests (prepsammoma body?) Crush-smear prerp Schwannoma Rarely smears well very fibrous Spindle cells Fascicular pattern may be obvious Overlap with fibrous predominant meningioma Schwannoma usually more fibrous Meningioma usually has a few epithleioid cells 8




9 Meningioma v Schwannoma Meningioma Lobules and fascicles in fibrous stroma Collagen bundles often discrete Nests/whorls/psammoma bodies Schwannoma Fascicles throughout Fibrous stroma is diffuse not discrete Verocay (like) bodies if lucky Metastasis Crush/smear prep Clusters of cells, usually epithelioid May be obviously cohesive (or not) Lack fibrillary processes Beware of stretched cytoplasm Beware of admixed reactive astrocytes Naked nuclei At edge of tumor, reactive changes may predominate Small numbers of tumor cells may be ignored, especially if crushed naked nuclei Account for everything 9




10 Metastasis Metastatic non-small cell carcinoma Cohesive nests Expansive interface with brain Metastasis Small cell carcinoma Neuroendocrine/small cell tumors may raggedly infiltrate from a densely cellular core. Limited extent of invasion Tendency to form short cords Cytology may be indistinguishable from small anaplastic astrocytes Hopefully, the smear had enough processes! 10





 in children.")


11 Avoiding a smear prep trap on small cell tumors Cerebellar granule cells are easy to mistake for a small cell malignancy, either metastatic neuroendocrine carcinoma in adults or medulloblastoma (here) in children. Granule cells have smooth round contours and are appreciably smaller than malignant cells (about the size of RBCs). 11


12 Sampling issues- Pathology There is no way to know if the sample chosen for the smear prep is representative In the examples at right, using either end would give the same correct result (matching the FS) In the example at the top, the results would be different and in fact neither would match the frozen section = GBM + = = + 12

13 It s worth the risk + = Suspicious for astrocytoma; more tissue requested Note that the risk of a non-correlating smear and section or of failing to make a definitive diagnosis is minimal if the surgeon provides an appropriately representative biopsy! Sampling - Surgeon We talked about sampling issues that are created in the lab. Some are created by the surgeon but that is why we got the tissue: to find out what it is for sure. Biopsies next to the lesion typically require more time than lesional samples and have the added bonus of finding a way to tell the neurosurgeon that he/she missed. Some biopsies are lesional but misleading. 13




14 Glioblastoma Cellular tumor + Necrotizing inflammation Necrosis in GBM can occurs from vascular injury leading to infarction. May involve tumor and/or brain Just like ordinary infarcts, sometimes massive PMN infiltrates occur at 1-2 days Not a problem if both are present, BUT Abscess Sometimes that nemesis Sampling rears its ugly head and you just get a lot of necrosis and neutrophils Nothing to indicate this is not an ordinary abscess So this conversation takes place 14

.")


15 Abscess?GBM Pathologist: We ve got marked necrotizing inflammation looks like an abscess Neurosurgeon: No way! This is a tumor (you idiot). Pathologist (In a firm calm voice): Yeah that happens sometimes with acute tumor necrosis. Just send me some tissue from a viable area. Neurosurgeon: OK (Wow! This pathologist really knows what they are doing!) Glioblastoma The new biopsy does in fact have cellular tumor. The surgeon is happy and has a newfound respect for pathologists (I can dream). 15






16 Perineuronal satellitosis Recurrent tumor v radiation effect A frequent biopsy question as new enhancing lesions on MRI can reflect either recurrent tumor or radiationinduced vascular injury. Recurrent tumors are usually characterized by the presence of cellular tumor. Mitoses are strong evidence or actively growing recurrent neoplasm. This pattern is diagnostic even if there are changes of recurrence elsewhere. 16






17 Recurrent infiltrating The other pattern of unqualified recurrence involves infiltrating diffuse growth. This will be less cellular but the background will be relatively normal brain. In fact, were it not for the history, this pattern be indistinguishable from the infiltrating edge of a primary glioma. Diffuse necrosis At the other extreme is the biopsy that shows diffuse necrosis or minimal semi-viable tumor. Whereas this is also identical to the necrotic centers of untreated glioblastomas, the history of a new or enlarging lesion on MRI indicates that it represents treatment effect. In cases at either extreme, the answer is easy but as we shall see, that is not always the case. 17







18 A side note on types of necrosis Brain tumor necrosis is described as either Infarct-type or (pseudo)palisading. In primary/untreated tumors they have the same significance. Infarct necrosis may be due to RT or spontaneous/intrinsic. However, by convention, pseudopalisading necrosis is considered spontaneous/ intrinsic. In this regard, the presence of palisading necrosisindicates recurrent tumor. Typical RT changes: Gliosis, edema & vascular fibrosis Typical changes associated with RT include: Edema and gliosis in various proportions and severity. The astrocytes often demonstrate reactive or radiation induced atypia. Vascular changes including hyaline fibrosis, loss of endothelial cells, fibrinoid degeneration and even thrombosis. 18




19 Parenchymal infarcts Small circumscribed foci of severe edema with axonal loss or overt necrosis represent microvascular infarcts due to radiation vascular injury (the mechanism of clinical radiation necrosis ). They are distinguished from tumor necrosis by the lack of ghost outlines of cellular tumor (parenchymal architecture may be apparent) and the surrounding background of normal or reactive brain. A very specific indicator of treatment effect. Individual Tumor Cells The cells seen here are too bizarre to be radiation-induced atypia in reactive astrocytes so they are almost certainly tumor cells. There are always residual tumor cells in treated gliomas whether you see them or not or they are in the biopsy or not. ITC are NOT recurrent tumor. In a background of reactive changes, they are most likely residual senescent tumor cells. 19
 gliomas Large")

.")

20 Macrophages A few individual macrophage are scattered throughout (high grade) gliomas Large numbers are only rarely seen and clusters, parenchymal or perivascular, are so exceptional as to seriously challenge a diagnosis of recurrent tumor (or of tumor at all). As seen here, they are all but diagnostic of treatment effect over recurrence.??? As newly minted experts, what do you think? Recurrent? Treatment? 20




21 ??? How about this one? Recurrent? Treatment??? Sometimes there is no right answer I have gone back and forth on these cases from when I first saw them to when I put the pictures in the talk. 21


22 Recurrent v treatment Next-to-last word Mild hypercellularity Scattered atypical cells Edema Scattered small cells Scattered reactive appearing astrocytes Vascular changes Would favor treatment but not straightforward unless the surgeon gave you the history that they were looking for recurrent metastatic carcinoma RT can cause a lot of atypia Lack of Hx can cause a lot of confusion Recurrent tumor or treatment? Extremes cellular tumor or diffuse necrosis easy but Milieu Scattered atypical cells in a healthy-appearing stroma suggests tumor Scattered atypical cells in a background of macrophages and necrosis suggests treatment allow a few more atypical cells here Macrophages are your friends Clustered macrophages are almost never seen in gliomas Parenchymal infarcts are specific for treatment effect Individual tumor cells does not mean recurrence There are always tumor cells left behind; eventually the treatment will always fail and the tumor will recur unless the patient dies first from the treatment itself, a heart attack, a car accident. The answer is often BOTH The patient did receive treatment for an incurable tumor. There will (almost) always be some treatment-related changes and the tumor will recur Remember the question is really Has the treatment failed/is the tumor winning? Definite cellular or infiltrating tumor indicates treatment failure even in a preponderant background of treatment effect The answer is sometimes a shrug. How many atypical cells do you need to call it cellular? Sometimes pathology doesn t have the right answer pick a side and comment that the case is borderline/not definitive/or whatever term you prefer for equivocation That s why tumor boards were created 22






23 Inflammatory/reactive tumor-like lesions Multiple sclerosis Permanent sections usually straightforward White matter Circumscribed v diffusely infiltrative Reactive astrocytes though often atypical Macrophages in clusters parenchymal & perivascular Myelin loss with relative axonal preservation Multiple sclerosis Frozen sections often not straightforward Hypercellular and edematous white matter Reactive astrocytes though often atypical Atypia is clue because of low number Small mononuclear cells account for most of hypercellularity 23





24 Multiple sclerosis At low power circumscribed pattern often apparent if biopsy big enough At higher power, mononuclear cells are seen to be macrophages in clusters - parenchymal & perivascular Inflammatory/Reactive v Tumor Hypercellular gray and white matter Obvious astrocytes with some atypia Cells with round nuclei?mononuclear Cells with slender elongate/oblong nuclei w/o obvious processes/ cytoplasm 24


25 Inflammatory/Reactive v Tumor Changes primarily in gray matter White matter less cellular edema and a few astrocytes Round and slender oblong nuclei both diffusely distributed and clustered around vessels or neurons Distribution suggests inflammatory Lymphocytes and microglia/histiocytes Inflammatory/Reactive v Tumor Cell number Overall By type Cell type Astrocytes Mononuclear cells Microglia v astrocyte MACROPHAGE Clustered macrophages are almost never seen in tumor Cell/Lesion distribution Diffuse WM Tumor Circumscribed WM MS Grey matter - Inflammatory Perivascular - Inflammatory No organisms on biopsy but autopsy confirmed Balmuthia/Acanthamoeba meningoencephalitis 25






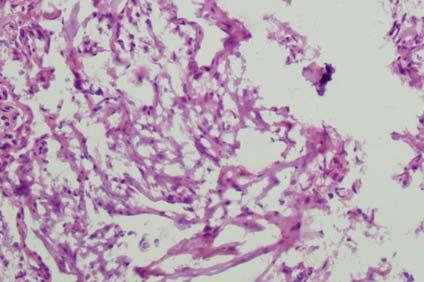
26 Atypical) Meningioma v Hemangiopericytoma/SFT (Atypical) Meningioma v Hemangiopericytoma/SFT 26








27 (Atypical) Meningioma EMA + 27


")



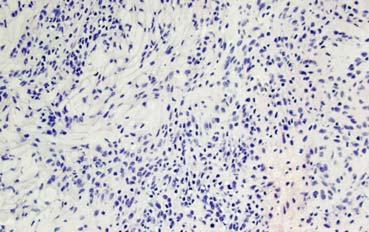
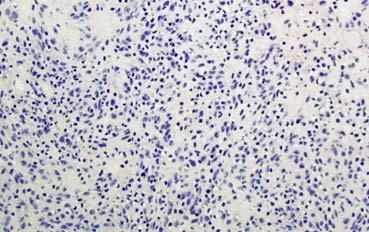
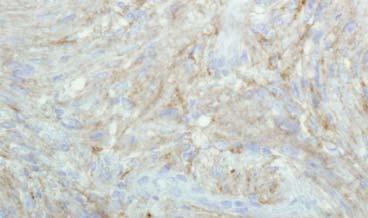
28 CD34 highlights only blood vessels Bcl2 (shown) Inflmmatory cells + CD99 Reticulin limited to blood vessels Hemangiopericytoma/SFT CD





29 CD99 + Bcl2 + Rich reticulin network EMA Hemangiopericytoma/SFT Invasive, aggressive tumors that almost always recur Grading based primarily on proliferative activity which correlates with cellularity and atypia Timing of recurrence, not if At FS, any time you see an I think it s a meningioma, but it s atypical, funny, worrisome consider HPC/SFT Operative management the same Surgeons often recognize tumor is more invasive may ask if it is atypical or an HPC Old name: Angioblastic meningioma based on high number of atypical microvessels. Not currently used but still causes confusion 29



30 Angiomatous meningioma Highly vascular, poorly cellular Cell loss and collapse leads to approximation of hyalized blood vessels More vessels than tumor cells Degenerative/involutional change (Almost) always grade I Hard to be aggressive and degenerative at the same time Closely related to microcystic meningioma Similar cell loss but mucopolysaccharide-rich edema fills the space so less collapse Angiomatous meningioma Hyalinized closey approximated vessels Few residual tumor cells Degenerative atypia common often pronounced 30
31 IMMUNOHISTOCHEMISTRY THAT ACTUALLY HELPS Lineage IHC Essential S100 GFAP Synaptophysin Neu-N Specialized/Limited Beta-tubulin MAP-2 Nestin CD-133 EMA CD34 CD99 BCL-2 Cam 5.2 NOT AE1/3 31
32 Glioma IHC α-internexin Cathepsin B EGFR/EGFR viii ch 7 IDH1 INI-1 MGMT O6 methyl guanine methytransferase Nestin p16 p53 PDGFR PTEN PI3K/Akt YKL-40 Glioma IHC that actually helps α-internexin High correlation with 1p 19q codeletion Usefulness as surrogate? p53 IDH1 INI-1 RTK/ATRT Valuable/limited 32

 of normally transient protein >50% diffuse astrocytomas Rare in oligodendrogliomas Antibody")
33 IDH1 and p53 IDH1 Most common mutation in diffuse gliomas 75%? Initial tumorigenic mutation IDH2 mutationa less common Antibody is specific to mutated gene Highly sensitive 100% specific for diffuse glioma (Oligo/Astro) p53 Widely expressed tumor suppresser gene/pathway p53 mutation or other defect in p53 pathway leads to accumulation (mutant or wild type) of normally transient protein >50% diffuse astrocytomas Rare in oligodendrogliomas Antibody detects both wild type and mutant Oligo v Astro Oligo classic Astrocytoma 33









34 Oligo v Astro Oligo not so classic Astrocytoma Oligo v Astro IDH1 + P53 - IDH1 + P






35 Oligodendroglioma v mimics Oligodendroglioma DNT Oligodendroglioma v mimics Oligodendroglioma DNT 35





36 Diffuse astrocytoma v mimics Diffuse astrocytoma Pilocytic astrocytoma Diffuse astrocytoma v mimics Diffuse astrocytoma Pilocytic astrocytoma 36


37 Diffuse astrocytoma v mimics Diffuse astrocytoma Pilocytic astrocytoma Diffuse astrocytoma v mimics Diffuse astrocytoma Reactive/Inflammatory 37
38 What we covered FS challenges: Artifacts & Neurosurgeons Smear/Crush Preparation: Friend or foe Glioblastoma?Abscess Recurrent?/Treatment?/??? Tumor v Inflammatory (MS): Beware of Macrophages Meningioma/SFT/Hemangiopericytoma IHC: IDH1!!! 38
Five Most Common Problems in Surgical Neuropathology
 Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
BAH1 - Primary Glioblastoma
 BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Cerebral Parenchymal Lesions: I. Metastatic Neoplasms
 Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
SUPPLEMENTARY INFORMATION
 VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
Wedge Biopsy for Diffuse Lung Diseases
 Chapter VI Wedge Biopsy for Diffuse Lung Diseases Wedge biopsy via thoracoscopic biopsy or open lung biopsy is occasionally performed to obtain tissue for the diagnosis of a diffuse lung disease. A wedge
Chapter VI Wedge Biopsy for Diffuse Lung Diseases Wedge biopsy via thoracoscopic biopsy or open lung biopsy is occasionally performed to obtain tissue for the diagnosis of a diffuse lung disease. A wedge
Pleomorphic Xanthoastrocytoma
 Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas
 The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
SPECIAL SLIDE SEMINAR CASE 3
 SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
Chapter 1 Introduction
 Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Chapter 1 Introduction Men think epilepsy divine, merely because they do not understand it. But if they called everything divine which they do not understand, why, there would be no end to divine things.
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Lách
 Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Understanding general brain tumor pathology, Part I: The basics. Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky
 Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
I have no conflicts of interest in relation to this presentation. Vogel FS & Burger PC 3/28/2016
 IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Intraoperative Cytology of CNS Lesions
 1 Intraoperative Cytology of CNS Lesions Matthew A Zarka, M.D. Director of Cytopathology Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Scottsdale, Arizona Gregory S. Moes, M.D. Department
1 Intraoperative Cytology of CNS Lesions Matthew A Zarka, M.D. Director of Cytopathology Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Scottsdale, Arizona Gregory S. Moes, M.D. Department
USCAP Neuropathology. Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC
 USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
WSC , Conference 9, Case 1. Tissue from a nyala.
 WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
WSC 2009-2010, Conference 9, Case 1. Tissue from a nyala. MICROSCOPIC DESCRIPTION: Heart, atrium (1 pt.): Approximately 40% of the atrial myocardium is replaced by areas of fibrous connective tissue (1
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Immunohistochemical Staining for Claudin-1 Can Help Distinguish Meningiomas From Histologic Mimics
 Anatomic Pathology / CLAUDIN-1 IN MENINGIOMAS Immunohistochemical Staining for Claudin-1 Can Help Distinguish Meningiomas From Histologic Mimics Hejin P. Hahn, MD, PhD, Elizabeth A. Bundock, MD, PhD, and
Anatomic Pathology / CLAUDIN-1 IN MENINGIOMAS Immunohistochemical Staining for Claudin-1 Can Help Distinguish Meningiomas From Histologic Mimics Hejin P. Hahn, MD, PhD, Elizabeth A. Bundock, MD, PhD, and
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal,
 Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Hello and welcome to Patient Power sponsored by Northwestern Memorial Hospital. I'm Andrew Schorr.
 Brain Tumor Clinical Trials Webcast November 22, 2011 Sean Grimm, M.D. Please remember the opinions expressed on Patient Power are not necessarily the views of Northwestern Memorial Hospital, its medical
Brain Tumor Clinical Trials Webcast November 22, 2011 Sean Grimm, M.D. Please remember the opinions expressed on Patient Power are not necessarily the views of Northwestern Memorial Hospital, its medical
Review of the AP Part II Practical Examination. Dr David Clift Co Chief Examiner
 Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Review of the AP Part II Practical Examination Dr David Clift Co Chief Examiner General Remarks The part II practical examination involved 15 cases which were presented with sufficient clinical data to
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad
 Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma
 AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Brain Microanatomy: Artifacts, Neoplastic Lesions and Utilization of Special Stains
 1 Brain Microanatomy: Artifacts, Neoplastic Lesions and Utilization of Special Stains Current Standard for CNS Evaluation in Rodent Toxicity Studies ESTP Congress in Ghent, Belgium 12 September 2013 Robert
1 Brain Microanatomy: Artifacts, Neoplastic Lesions and Utilization of Special Stains Current Standard for CNS Evaluation in Rodent Toxicity Studies ESTP Congress in Ghent, Belgium 12 September 2013 Robert
WHO 2016 CNS Tumor Classification Update. DISCLOSURES (Arie Perry, MD) PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology
 PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology") WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
Case # year old man with a 2 cm right kidney mass
 Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Case # 4. 52 year old man with a 2 cm right kidney mass Figure 1 Figure 2 Figure 3 Figure 4 Diagnosis: Negative/Non-diagnostic Normal kidney tissue Fine needle aspiration (FNA) of the kidney is performed
Advances In Orbital Neuropathology
 Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
2. Subependymal giant cell astrocytoma:
 I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
PLEOMORPHIC ADENOMA ( BENIGN MIXED TUMOR )
") ( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
( BENIGN MIXED TUMOR ) Grossly, the tumor is freely movable, solid, sometimes lobulated and occasionally cystic. If recurrent, multinodular masses are common. Histologically, within a fibrous capsule,
Infections. Meningitis- leptomenings (usually bakterial)
") Neuropathology Neuropathology Cerebral Edema, raised intracranial pressure, Herniatio Malformations, Developmental Diseases Perinatal Brain Injury Trauma Cerebrovascular Diseases Infections Transmissible
Neuropathology Neuropathology Cerebral Edema, raised intracranial pressure, Herniatio Malformations, Developmental Diseases Perinatal Brain Injury Trauma Cerebrovascular Diseases Infections Transmissible
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
GUT-C 11/30/2017. Debasmita Das, M.D. PGY-1 Danbury Hospital
 GUT-C 11/30/2017 Debasmita Das, M.D. PGY-1 Danbury Hospital CLINICAL SUMMARY 8/2017 59 year old female Presented to the ED with 1 month history of general malaise, fever and weight loss PMH: Significant
GUT-C 11/30/2017 Debasmita Das, M.D. PGY-1 Danbury Hospital CLINICAL SUMMARY 8/2017 59 year old female Presented to the ED with 1 month history of general malaise, fever and weight loss PMH: Significant
Avian Pathology. Bacterial diseases: histo slides. ECVP-ESVP Summer School 2012 Frédérique NGUYEN
 Avian Pathology Bacterial diseases: histo slides ECVP-ESVP Summer School 2012 Frédérique NGUYEN Bacterial diseases: histo slides B1. Turkey. Organs? Morphologic diagnosis? Special procedure? B2. Hen. Organ?
Avian Pathology Bacterial diseases: histo slides ECVP-ESVP Summer School 2012 Frédérique NGUYEN Bacterial diseases: histo slides B1. Turkey. Organs? Morphologic diagnosis? Special procedure? B2. Hen. Organ?
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Cellular Pathology. Histopathology Lab #2 (web) Paul Hanna Jan 2018
 Paul Hanna Jan 2018") Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
Cellular Pathology Histopathology Lab #2 (web) Paul Hanna Jan 2018 Slide #91 Clinical History: a necropsy was performed on an aged cat the gross pathological changes included: widespread subcutaneous edema
Mousa. Israa Ayed. Abdullah AlZibdeh. 0 P a g e
 1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
Mesenchymal Tumors MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE)
") MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Mesenchymal Tumors Focus on Vascular Tumors Benign and
MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Mesenchymal Tumors Focus on Vascular Tumors Benign and
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Histopathology: healing
 Histopathology: healing These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information that
Histopathology: healing These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information that
Disclosure. Case. Mixed Tumors of the Uterine Corpus and Cervix. I have nothing to disclose
 Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Neuropathology Inflammation, Infection, Demyelination in the CNS
 Neuropathology Inflammation, Infection, Demyelination in the CNS PathoBasic 2016-09-20 Jürgen Hench Inflammation in the CNS inflammation generally as a reaction against pathogen, substance, necrotic, or
Neuropathology Inflammation, Infection, Demyelination in the CNS PathoBasic 2016-09-20 Jürgen Hench Inflammation in the CNS inflammation generally as a reaction against pathogen, substance, necrotic, or
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Morphological features and genetic alterations
 Morphological features and genetic alterations Tutor : Audrey Rousseau Caget Lise: Université d Angers Iorio Vittoria: Seconda Università degli studi di Napoli Manaila Roxana: Iuliu Hatieganu University
Morphological features and genetic alterations Tutor : Audrey Rousseau Caget Lise: Université d Angers Iorio Vittoria: Seconda Università degli studi di Napoli Manaila Roxana: Iuliu Hatieganu University
Mesenchymal Tumors. Cavernous Hemangioma (CH) VASCULAR TUMORS MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE)
 VASCULAR TUMORS MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE)") Mesenchymal Tumors MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Focus on Vascular Tumors Benign and
Mesenchymal Tumors MESENCHYMAL TUMORS OF THE LIVER: WHAT S NEW AND UNUSUAL (MY PERSPECTIVE) CURRENT ISSUES IN ANATOMIC PATHOLOGY MAY 23, 2014 Linda Ferrell, MD, UCSF Focus on Vascular Tumors Benign and
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
NEURORADIOLOGY DIL part 5
 NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP)
") Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
Cellular Neurothekeoma
 Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
2015 Descriptive Vet Path Course. Histo Exam #3 KEY
 2015 Descriptive Vet Path Course Histo Exam #3 KEY Test 3, Slide 1 Tissue from a guinea pig. MORPHOLOGIC DIAGNOSIS: Heart: Multifocally and randomly (1 pt), within the left and right ventricular myocardium
2015 Descriptive Vet Path Course Histo Exam #3 KEY Test 3, Slide 1 Tissue from a guinea pig. MORPHOLOGIC DIAGNOSIS: Heart: Multifocally and randomly (1 pt), within the left and right ventricular myocardium
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Histopathology plays an important role in the neurosurgical
 J Neurosurg 116:854 860, 2012 In vivo intraoperative confocal microscopy for real-time histopathological imaging of brain tumors Clinical article Jennifer Eschbacher, M.D., 2 Nikolay L. Martirosyan, M.D.,
J Neurosurg 116:854 860, 2012 In vivo intraoperative confocal microscopy for real-time histopathological imaging of brain tumors Clinical article Jennifer Eschbacher, M.D., 2 Nikolay L. Martirosyan, M.D.,
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Common Artifacts That Impede Reliable Interpretation and Cause Misdiagnosis
 Gregory N. Fuller, MD, PhD Department of Pathology The University of Texas M.D. Anderson Cancer Center Common Artifacts That Impede Reliable Interpretation and Cause Misdiagnosis Introduction A large number
Gregory N. Fuller, MD, PhD Department of Pathology The University of Texas M.D. Anderson Cancer Center Common Artifacts That Impede Reliable Interpretation and Cause Misdiagnosis Introduction A large number