Radiation Dose Response LQ model, RBE, LET, OER, TCP & NTCP
|
|
|
- Albert Sanders
- 5 years ago
- Views:
Transcription
1 Radiation Dose Response LQ model, RBE, LET, OER, TCP & NTCP SK Shrivastava et al. Department of Radiation Oncology Tata Memorial Hospital, Parel, Mumbai


2 Radiotherapeutic Paradigm The basic goal of Radiotherapy- Kill the enemy (TUMOUR) but prevent collateral damage (NORMAL TISSUES). 2
3 TUMOUR CONTROL AND NORMAL TISSUE COMPLICATIONS Repair of sublethal damage Redistribution Repopulation Reoxygenation Radiosensitivity Total dose Overall treatment time Fraction size Radiation technique Type of radiation Sensitisation or protection 3
4 What we want to achieve NTCP 50 TCP 25 Delivered dose
5 Level of damage Tumour + Sensitizer Tumour Normal tissue + protector Normal tissue Dose (Gy) 5

 T 0.11 N 0.24 No.")
6 The early days. Coutard s experiment 1934 Strandqvist s curves 1944 Ellis Nominal Standard Dose Total dose = (NSD) T 0.11 N 0.24 No. of fractions N Overall treatment time T 6
7 Linear Quadratic Model Mechanistically based model Calculates radio-therapeutic iso-effect doses for different fractionation schemes 7
8 Assumptions Basic lesion which is responsible for radiation induced cell death is the di-centric exchange type chromosomal aberration. Equal dose fractions are equally effective, independent of the preceding or following dose fractions. Complete repair between two fractions. 8
9 Type A damage Type B damage Always lethal Not always lethal Amount of damage is always proportional to dose. For instantaneous exposures, the amount of damage is always proportional to square dose. Amount of damage is independent of dose rate and exposure time. Amount of damage is additionally dependent on dose-rate and exposure time. For any given dose, as exposure time increases, the amount of Type B damage is reduced. 9




10 Two component of cell killing by radiation, one dependent by the dose and the other one proportional to the square of the dose -cell survival curve is continuously bending α and β = Constant. S = Survival, D = Dose. 10
11 α/β Ratio Defines the dose at which cell killing by linear and quadratic components are equal. 1 αcomponent α/β ratio is thus the measure of how soon the survival curve begins to bend over significantly. Survival 0.1 α = 0.1, β = 0.06 βcomponent 0.01 Late responding tissue have low α/β ratio and early responding tissue have more α/β ratio Dose (Gy) 11
12 Dose Response Relationship Tumor & early responding tissues. Large α/β. αdominates at low doses. Survival Fraction Late responding tissues. Low α/β. βdominates at low doses. Dose 12
13 PARAMETERS α/β ratio Dose Response Curve Isoeffect Curve Shape Dose fractionation Acutely Responding Normal tissues & Tumors High Gy Steep Shallow Less sensitive Late Responding normal Tissues Low 1-6 Gy Shallow Steep Marked sparing 13
14 α/β VALUES FOR EARLY AND LATE REACTING TISSUES TISSUE α/βvalue EARLY REACTIONS SKIN (DESQUAMATION) 9 12 JEJUNUM COLON 8 13 TESTIS TUMOR BED (45 DAYS) LATE REACTIONS SPINAL CARD (CERVICAL) LUMBAR COLON (WEIGHT LOSS) KIDNEY (PIG) LUNG (LD 50 ) 2 6 LUNG (BREATING RATE) BLADDER (FUNCTION)
15 α/β VALUES FOR HUMAN TUMORS HUMAN TUMORS α/βvalue HEAD AND NECK 14.5 VOCAL CARD 13 OROPHARYNX 16 BUCCAL MUCOSA 6.6 TONCIL 7.2 MASOPHARYNX 16 SKIN 8.5 MELANOMA 0.6 LIPOSARCOMA 0.4 SKIN (EARLY REACTIONS) 8 12 ORAL MUCOSA (EARLY REACTIONS) 8 15 SKIN (LATE REACTIONS) MUSCLE/VASCULATURE/CARTILATURE 3.5 SPINAL CARD < 3.3 LUNG <
16 Use of the LQ model in external beam radiotherapy: Calculate equivalent fractionation schemes Comparing different fractionation schemes Correcting treatment gaps Changing overall treatment time Changing time interval between dose fractions Changing dose per fraction Re-irradiation Double trouble Allowance for tumour proliferation 16
17 Biological Effective Dose (BED) Allow for the quantitative assessment of the biological effects associated with different patterns of radiation delivery. Is a measure of the biological dose delivered to a tumour or organ. The theoretical dose, which, if delivered in infinitely small fractions, would produce the same biological endpoint as that under consideration BED is a measure of effect in units of Gy x, where the suffix x indicates the value of α/β assumed in the calculation. 17
18 Derivation of BED formula E = αd + βd 2. = α nd +β nd 2 = n (αd + βd 2 ) = nd (α + βd) = α (nd) (1+ d/α/β) E / α = nd (1+ d/α/β) BED = Total dose X Relative effectiveness. nd = total dose 1+d/α/β= relative effectiveness 18
19 Calculating Isoeffective relationship Describe range of fractionations schedules that are isoeffective D 2 α/β + d 1 D 1 = α/β + d 2 D 1 = initial known total dose, d 1 = initial dose / fraction D 2 = total dose to be calculated for new dose schedule d 2 = new dose / fraction 19
20 EQUIVALENT EFFECTIVE DOSE (EQD) Simple way of calculating isoeffective relationship is To convert into equivalent dose in 2 Gy fraction EQD2 EQD2 = D d + α/β 2 + α/β 20
21 Example We want to change current practice of palliative radiotherapy in advanced head neck cancer from 40Gy/16# to 4Gy/# due to logistic reason Excluding late effects from calculation What would be total dose needed to achieve same effective dose to that of current practice. 21
22 Let us suppose D1=40Gy d1=2.5gy D2=? And d2= 4Gy. We want D1 and D2 isoeffective thus, BED equation can be modified to D2/D1 = d1 + α/β /d2 + α/β D2/D1 = d1 + 10/d D2/40 = /4+10 D2 = 40 X12.5 / 14 = Gy. 22
23 Comparison of different fractionation schemes Different fractionation schemes can be compared by comparing their BED for acute and late effects This is obviously only valid for one tissue/tumour type with one set of alpha, beta values 23
24 Clinical examples. Comparison of various treatment schedules for head neck cancer. For calculation purpose for early effect and tumor (10 Gy), late effect (2Gy). Treatment 1(conventional) = 70Gy/35#/ 7 1#/day, 2Gy/#. Treatment 2 (Hyperfractionation) = 80.5Gy 2# /day, 1.15Gy/#. Treatment 3 (Conco boost) = 54Gy/30#/6weeks 1.8Gy/# with conc boost 18Gy/12#, 1.5Gy/3 during same period. Treatment 4 (CHART) = 3#/day, 1.5Gy/# 24
25 Treatment 1(conventional) = 70Gy/35#/ 7 1#/day, 2Gy/#. - Early effect BED = nd (1+ d/ α/β) = 70 (1 + 2/10) = 70 (1.2) = Late effects = 70 (1+ 2/2) =
26 Using the formula we will see that.. Arm Early Late Conventional Hyper# Conco Boost CHART
27 Allowance for tumour proliferation An alternative to put time scale in BED formulae. Crude method based on the assumption that rate of cellular proliferation remains constant throughout the overall treatment time. N = N 0 e λt N = number of clonogens at time t. N0 = initial clonogens. λ = constant = / T pot. Thus after modification BED = nd (1+ d/α/β) (0.693/ α) (t / Tpot) 27
28 Arm Early Effect Proli. correction Corrected dose for time Conventional Hyper# Conco Boost CHART
29 Double trouble Dosimetric hotspots receive not only higher total dose but also higher dose per fraction Withers called it double trouble Biological effect of a hotspot is relatively more Important for late effects than for tumour control 29
30 Unplanned gaps in treatment Gaps negative therapeutic effect (strongest for sq.ca. of head & neck, uterine cervix) Options - accelerating treatment after gap - hyper fractionation - delivering remaining in hypofractionated dose/fr 30
31 Example Pt of colorectal ca planned to receive RT 5Fraction of 5 Gy from Monday to Friday, no Treatment on Wednesday.. Planned to deliver isoeffective tumour dose by increasing size of last 2 #. α/β =10 Gy for colorectal Gy 31
32 EQD 2 = = Gy EQD 2 (New) = 2x x x * x + 10 = x = * 12 2x x 225 = 0 x = -b+ b2 4ac = -20+ (20) a 2*2 =
33 Limitations of LQ model The LQ model from which the BED concept is derived does not intrinsically include an allowance for the volume effect. The methods for assessing volume effects are complex (e.g. integrated BED, EUD, NTCP and TCP) Limitation for reirradiation. Applies best within dose range of 2-8 Gy /# application beyond that is not established 33
34 Inaccuracy due to incorrect estimation of α/β Important in tissues with low α/β Since curve is steep, wide variation of SF with little change in dose/# So any in accuracy in α/β estimation leads to amplified differences in isoeffective dose prediction No application to treatment given in single dose per fraction Lacks time factor 34
35 Time Dose Parameters Time dose parameters determining normal tissue tolerance are: Total dose. Overall duration of treatment. Size of dose per fraction. Frequency of dose fractionation. Size of dose per fraction and fractionation frequency determine the rate of dose accumulation. Intensity of acute reaction depends upon rate of cell kill & cell survival through proliferation of surviving stem cells which, depends on dose accumulation. At the peak of acute reaction, further irradiation will not increase the intensity of acute reaction, but will increase the time to heal. 35
36 Time Dose Parameters Late reaction occurs in tissues with slow cellular turnover like mature connective tissue and parenchymal cells of organs. Eg. Spinal Cord. No depletion of cells in late reacting tissues even if full course of RT is complete. Hence overall Rx time as well as dose accumulation has little role in severity of late reaction. Instead severity of late reaction is dominated by size of dose per fraction and interfraction interval. Time interval is necessary for complete repair of sublethal damage. Recommended time interval is at least six hours. As overall treatment time increases the probability of tumor control decreases / isoeffective dose for tumor control increases. 36


37 The era of IMRT. Target and critical organ 37




38 38
39 Do the DVH parameters really predict the tumour control and normal tissue complications? This led to the development of more probabilistic models predicting tumour control or normal tissue complication probabilities. They essentially aimed at making plan evaluation easier between two close High Precision plans. 39



40 TCP TCP NTCP 61.30% NTCP 14.91% 40
41 TumourControl Probability The probability of uncomplicated tumor control (P UTC ): P UTC =TCP(1-NTCP) 41
42 Normal Tissue Complication Probability These models aim to predict the probability of a complication as a function of the dose or biologically equivalent dose and volume 42
43 Normal Tissue Complication Probability Functionally, the whole organ does not fail if some part of it is destroyed Withers suggested that the tolerance of tissues depends on the ability of the remaining clonogenic cells to maintain a sufficient number of mature cells suitably structured to maintain organ function 43
44 Normal tissue complication probability Organ function depend upon the aggregation of cells into functional sub-units ( FSUs ) FSUs in an organ can be organized in series or parallel Series: gastrointestinal tract and spinal cord, damage in one portion of the organ may produce total organ fail Parallel: lung or kidney, function is often maintained since the undamaged part operates independently from the damage part 44
45 Normal tissue complication probability Volume dependence A lot to a little or a little to a lot? Whether it is better to give a lot to a little as unconventional treatment, or a little to a lot as in 3D and IMRT 45
46 Models for NTCP Homogeneous dose distribution Empirical model Probit model : Lyman (1985) Logistic model Tissue architecture model Inhomogeneous dose distribution Effective dose method : Lyman and Wolbarst (1987) Effective volume method : Kutcher and Burman (1989) Integral probability model : Schultheiss et al. (1983) 46
47 Probit model (Lyman) NTCP v = V / Vref t = ( D TD TD 50 = 1/ 2π ( v) = 50 TD t ( v)) /( m TD 50 (1) v exp( t n 50 2 / 2) dt ( v)) TD 50 (1) : the tolerance dose for reference volume irradiation m : the steepness slope of the dose response curve V ref : the reference volume n : tissue-specific parameter 47
48 Tolerance Data: Emami et al., 1991 Lung Vol 1/3 2/3 3/3 TD 5/ TD 50/ TD 5/5 is the dose to the partial organ that would have a 5 % probability of complication in 5 years. TD 50/5 is the dose to the partial organ that would have a 50 % probability of complication in 5 years. 48
49 Fitting of Tolerance Data: Burman et al., 1991 Lung, brainstem, optic nerve organ n m TD50 end point Lung Pneumonitis Brainstem necrosis/infarction Optic nerve blindness TD 5/5 TD 50/5 organ 1/3 2/3 1 1/3 2/3 1 Lung (fitted data) Brainstem (fitted data) Optic nerve (fitted data)
50 NTCP vs. dose, fixed partial irradiated volume 2/3 NTCP 3/3 2/3 1/3 NTCP 3/3 1/3 dose dose Large volume effect, n 1.0 small volume effect, n
51 Logistic model NTCP( D,1) = 1+ 1 ( D 50 / D) k γ 50 D 50 : the dose resulting in a 50% complication probability for some specified complication or end point k : 4γ 50 D 50 (γ 50 : slope of D 50 ) D 50 51
52 Effective dose method ) ).( / ( 1) ( ) ).( / ( ) ).( / ( ' 1 1 ' 3 ' ' ' 2 N N N N N N D D V V D D step N D D V V D D D D V V D D + = + = + = M 52 D N Lyman model or logistic model From Lyman et al. 1987
 Lyman model or logistic model From Kutcher et al.")
53 Effective volume method V eff = i V i ( D i / D 1/ n max ) Lyman model or logistic model From Kutcher et al




54 54
55 Disadvantages of NTCP models Lymen s model only applies to fractional volumes receiving uniform doses. In practice it is never the case. Modern systems describes dose to an organ in terms of DVH. DVH needs to be transformed into into a single point dose: Method 1: DVH is transformed into an equivalent dose given to the whole volume Method 2: DVH is transformed into a fractional volume that received the maximum dose in DVH (ASSUMTION: Each fractional volume will follow the same dose-volume relationship as the whole organ). Use of NTCP in clinical decision making is highly controversial. 55
56 Dose is not the most important. Two identical doses may not produce identical responses due to other modifying factors 1.Physical factors Linear energy transfer Relative biologic effectiveness Fractionation & protraction 2. Biological factors Oxygen Effect-Oxygen enhancement ratio Age Recovery Chemical Agents 56



57 OER: Oxygen Enhancement Ratio Definition 57
58 OER for sparsely ionizing radiation (i.e., x-rays) for a synchronous cell population: OER varies from according to cell cycle phase S phase: 2.9 G2 and M phases: 2.3 G1 phase: 2.6 for an asynchronous cell population: OER varies according to radiation dose 58
59 OER & radiation sensitivity for radiation of low ionizing density (i.e x-rays): OER for radiation of intermediate ionizing density (i.e., neutrons): OER is 1.6 and is much smaller than for x-rays. for densely ionizing radiation (i.e., α-particles): OER is 1 that is, there is no oxygen effect Palcic et al Rad Res
60 OER for X-RAYS at low doses(i.e., < 200 cgy) OER ~ 2.5 rationale cells in G1, G2, or M phase are more radiosensitive than cells in S phase OER tends to be lower for cells in G1, G2, or M phase than cells in S phase therefore, at low doses, cells in radiosensitive phases constitute most of the killed cells, and OER is low. at high doses(i.e., > 200 cgy) OER ~ rationale: at high doses, an increasing proportion of radioresistant cells are killed, and OER is therefore observed to increase 60
61 OER & LET Oxygen effect is large for sparsly ionizing radiation e.g X-rays Oxygen effect is absent for densly ionizing radiation. Oxygen effect is Intermmediate for neutrons. 61 according to radiation type: OER decreases as LET increases
62 LET: Linear Energy Transfer Definition: introduced by Zirkle Energy deposited per unit of track length of soft tissue. LET = de/dl Where: de is the average energy locally imparted to the medium by a charged particle of a specified energy in traversing a distance of length dl. Units: KeV/um What LET tells us is that the number of ionization events increase as the LET increases and decrease as the LET decreases Track average = equal track length Energy average = equal energy increments. 62
63 LET Microdosimetry Sparsely ionizing: x-rays, gamma rays. Densly ionizing: Alfa particles, protons, neutrons A measure of average ionization density. LOW LET HIGH LET 63

64 LET The specific ionization of low LET radiation such as x-rays and gamma rays do not create ion pairs close together. The specific ionization of particulate radiations (e.g. alpha particles) is high as ionization occurs more frequently and at closer intervals along the radiation's path. 64
65 LET As the energy of a photon of electromagnetic radiation increases its LET decreases, for example a 25-MeV photon will impart a LET of approximately 0.2 kev/μm. X-rays and gamma rays are highly penetrating radiations as such do not easily give up their energy and are considered low LET radiations. Less penetrating radiations such as particulate radiation, photoelectrons, alpha particles, and beta radiation are high LET radiations. so LET is inversely proportional to energy and range of travel 65
66 RBE &LET (phenomenon of overkill effect) X-rays 100 kev/u 200 kev/u * * 20 A DNA * * * RBE LOW LET Optimal LET Densly ionizing HIGH LET LET 66



67 Initial DNA damage from an alfa- particle, measured by histone H2AX accumulation 67
68 LET Measure of the rate at which energy is transferred from ionizing radiation to tissue. Another way of expressing radiation quality & determining the value of the tissue weighting factor (WT) A simple way to indicate the quality of radiation. 68

69 Effect of varying LET on surviving fraction 69
70 Rationale of High LET beams (1) Hypoxiccells -are very resistant to low-let radiation -less resistant to high-let radiation (2) Slowly proliferating cells in the Go or G1 phase resistant to low-let radiation but not so resistant to high-let (3) Repair of sub lethal damage -Less repair of sub-lethal damage after high-let radiation, -high-let treatments resemble large dose-per-fraction of X rays. Jack F. Fowler International Journal of Radiation Applications and Instrumentation. Part D. Nuclear Tracks and Radiation Measurements, Volume 16, Issues 2-3, 1989, Pages
71 High-LET Neutrons Heavy ions Light ions Protons 71

72 High-LET radiation enhanced apoptosis but not necrosis regardless of p53 status. Takahashi A, Matsumoto H, Yuki K, et al. IJROBP 2004;60:
73 RBE: Relative Biological Effectiveness RBE : Dose of standard Radiation to produce a given effect Dose of test radiation to produce the same effect Standard radiation, by convention, is X-radiation in the 200- to 250-kVp range or 60Co gamma rays For diagnostic X-rays, RBE = 1 73
74 Factors which influence the RBE RBE depends upon: radiation dose (dose per fraction),dose rate radiation quality (LET) RBE increases with increase in LET up to a maximum at ~100keV /micron, and thereafter decreases due to the overkill effect. biological system or endpoint conditions, e.g. oxygenation 74
75 Effect of dose and dose per fraction on the RBE 75
76 Dependence of RBE on the type of cell irradiated In general, cells which exhibit large shoulders in their X-ray survival curves will show large RBEs for neutrons. Conversely, cells with little, if any, shoulder will have low RBE s for nutrons But there are exceptions, due to the different interaction mechanisms between low- and high-let radiations e.g. cell-cycle effect. 76
77 Dependence of RBE on type of cell irradiated 77
78 Applications of RBE in Radiation Protection Radiation Weighting Factor (WR) Equivalent Dose = dose x WR where WR is a rounded value of the RBE. A rounded (approximate) RBE needs to be used to cover all biological systems, doses, and endpoints. 78
79 Relationship Between LET & RBE LET & RBE Type of Radiation LET RBE 25-MV x-rays Less efficient cell kill Optimu m LET over kill 60Co X-rays MeV electrons Diagnostic X-rays MeV protons Fast Neutrons MeV alpha particles



80 Relation between LET, RBE & OER 80
81 LET for proton, carbon and neon ions along their path For carbon ions the maximum RBE is in the tumour region, neon ions produce an overkill-effect inside the target volume where the Bragg maximum is situated. The density of the red colour indicates the increased RBE for carbon LET Bragg maximum RBE~0 neon ions carbon ions high RBE region for carbon ions RBE~1 protons depth 81
")
82 Particle Therapy First proposed the use of protons and heavier ions for therapy in 1946 Robert Wilson (March 4, 1914 January 16, 2000) 82
83 Protons - positively charged particles hydrogen atom electrical field separated into protons and electrons protons vacuum tube in LA & proton energy boosted to about 7 MV proton beam synchrotron accelerated 70 to 250 MeV enough energy to place at any depth beam passes series of magnets shape, focus, and direct the beam to patient 83
84 Accelerators for High RBE Radiations Two types of accelerators : cyclotron or a synchrotron Cyclotrons fixed energy, higher energy 250 MeV Synchrotron varied energies, usually in the range of MeV 84
85 SOBP Individual Bragg peaks too narrow to use Summed up and spread out (SOBP) to a useful plateau 85

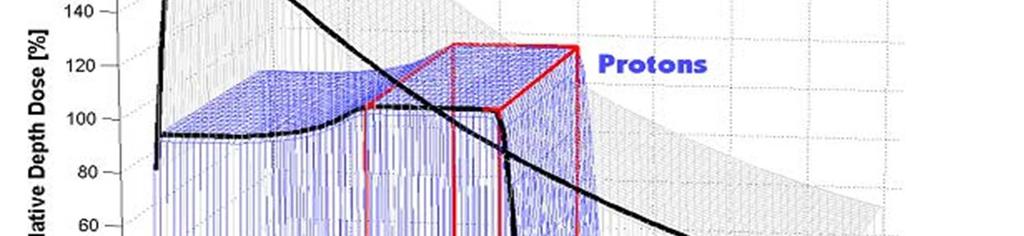

86 SOBP 86
87 Useful applications of the proton beam 1) Zero dose beyond the Bragg peak. -Stop the beam in front of sensitive healthy structures. Eye tumours 2) Low integral dose outside of the target volume. -Treatment of large tumours by reducing the dose burden outside the target volume and give more dose to the target. 3) Protons are charged particles. --Magnetic deflection of the beam - active dynamic scanning of the beam. -For treatment of tumours with complex geometrical shape - conformal therapy. 87


88 Photon beam displaying exit dose Proton beam displaying how dose stops 88
89 Example of DVH in Ca NPX Zahra Taheri-Kadkhoda 89 Radiation Oncology 2008, 3:4
90 Tumors considered for proton therapy High doses of radiations for control Located near sensitive normal tissues 90
91 Heavy Ion therapy 91
92 Biological aspects-carbon Major advantage - increased biological effectiveness in the Bragg peak region so in the tumor volume Increased effectiveness specific microscopic dose deposition pattern Photons deposit energy randomly and homogeneously Charged particles narrow region around the particle trajectory Very localized & concentrated energy Increased effectiveness 92
93 Lateral Scattering Lateral scattering more important than longitudinal straggling carbon broadening is < 1 mm up to depth 20 cm Protons 2 mm depth > 7 cm. Lateral scattering for protons > photons Deep-seated tumors precisely with carbon ions Superficial tumors (eye) satisfactory with protons 93
94 proton photon carbon Comparison of the lateral scattering of photon, proton and carbon beams as function of the penetration depth Weyrather Clinical Oncology (2003) 15: S23 S28 94
95 Clinical Evidence Protons Ions as Carbon, He Neutrons 95
96 Proton Beam Therapy 96
97 Proton Beam: Clinical Implications Uveal (choroidal) melanoma. Skull base tumors Spinal cord tumors Chordoma. Prostate cancer. Pituitary tumor. Acoustic neuromas. Paranasal sinus & Nasopharynx. Others AVM. 97

 110")
98 Summary of Clinical Evidence M. Lodge et al. / Radiotherapy and Oncology 83 (2007)
99 Neutron Therapy 99
100 Neutron Therapy Neutrons first were introduced without proper experimental data on sole basis that lower OER Since biological effect not taken into consideration major set back due very severe late reaction. Later on RBE concept taken into consideration Production -Deuterium Tritium generators. -Paricle Accelerators Bombarding particles Deuterons, proton. Target material Usually beryllium. Depth dose data same as photons 100
101 Isodose distributions for 8 MV X-ray and p(66)/be neutron 101
102 Interactions No charge but with high LET, RBE value. Indirectly ionizing. Two mechanism - Recoiling with hydrogen or heavy nucleus of element. - Nuclear disintegration. 102
103 Indications for fast neutron therapy Region Base of skull Tumour Chordomas Chondrosarcomas Head and neck Salivary gland tumours Paranasal sinus tumours Chest and abdomen Breast tumours Pelvis Prostate tumours (T3, T4) Uterine sarcomas Chordomas Chondrosarcomas Trunk and extremities Osteosarcomas Malignant melamonas STS Soft tissue sarcomas D.T.L. Jones, A. Wambersie / Nuclear Instruments and Methods in Physics Research A 580 (2007)
104 Neutrons: Advantage only in few selected tumors Salivary gland. Prostate cancer. STS. Head and neck malignancies (Advanced). NSCLC. Breast 104
105 Salivary gland Based on strong radiobiological rationale given by Batterman et al Salivary gland tumor has RBE ~ 8 as compare to other late effect (3-3.5) 20Gy of neutrons are equivalent to 160Gy at tumor site, 60Gy at normal tissue level Therapeutic gain factor for salivary gland tumor is
106 RCT RTOG/MRC trial Accrual stopped as 2 year data showed strong trend towards neutron Followed up 10 yr Improved local control in neutron arm 56% Vs 17%. P=0.009 No difference in long term survival due to distant mets. 106
107 Prostate cancer 2 RCT. RTOG* compared mixed beam with photon alone in locally advanced cases. -91 pt.. -At 10 yr F/U LRC 70% vs 58%(p=0.03), survival 46% vs 29% (p=0.04). -No difference in toxicity! *Am J Cli onco 1993,16,
108 2 nd RCT NTCWG Russell et al.* 172 pt. Fast Neutron vs photon. No difference in survival. *IJROBP 1993,28,47 108
109 Drawbacks Enormous cost involved. (~US $100m) More complex and bulky equipment necessary to accelerate particles. Stringent quality assurance needed. No long term data available to consider late effects of treatment. Dose tolerance for various organs are not available. 109
110 Conclusions Advances in radiation physics and better understanding of tumour biology allows us to plan more complex yet safe radiation therapy. This will lead to better tumour control and reduction in normal tissue toxicity thus improving the therapeutic ratio. Young Generation - : Undertake clinical trials to validate the radiobiological concepts. Develop models to individualize Radiotherapy based on tumour kinetics. 110




111 ThankYou Varanasi, April 23,
TFY4315 STRÅLINGSBIOFYSIKK
 Norges teknisk-naturvitenskaplige universitet Institutt for fysikk EKSAMENSOPPGÅVER med løysingsforslag Examination papers with solution proposals TFY4315 STRÅLINGSBIOFYSIKK Biophysics of Ionizing Radiation
Norges teknisk-naturvitenskaplige universitet Institutt for fysikk EKSAMENSOPPGÅVER med løysingsforslag Examination papers with solution proposals TFY4315 STRÅLINGSBIOFYSIKK Biophysics of Ionizing Radiation
Proton and heavy ion radiotherapy: Effect of LET
 Proton and heavy ion radiotherapy: Effect of LET As a low LET particle traverses a DNA molecule, ionizations are far apart and double strand breaks are rare With high LET particles, ionizations are closer
Proton and heavy ion radiotherapy: Effect of LET As a low LET particle traverses a DNA molecule, ionizations are far apart and double strand breaks are rare With high LET particles, ionizations are closer
Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation.
 Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
COMPARISON OF RADIOBIOLOGICAL EFFECTS OF CARBON IONS TO PROTONS ON A RESISTANT HUMAN MELANOMA CELL LINE
 COMPARISON OF RADIOBIOLOGICAL EFFECTS OF CARBON IONS TO PROTONS ON A RESISTANT HUMAN MELANOMA CELL LINE I. Petrovi a, A. Risti -Fira a, L. Kori anac a, J. Požega a, F. Di Rosa b, P. Cirrone b and G. Cuttone
COMPARISON OF RADIOBIOLOGICAL EFFECTS OF CARBON IONS TO PROTONS ON A RESISTANT HUMAN MELANOMA CELL LINE I. Petrovi a, A. Risti -Fira a, L. Kori anac a, J. Požega a, F. Di Rosa b, P. Cirrone b and G. Cuttone
LET, RBE and Damage to DNA
 LET, RBE and Damage to DNA Linear Energy Transfer (LET) When is stopping power not equal to LET? Stopping power (-de/dx) gives the energy lost by a charged particle in a medium. LET gives the energy absorbed
LET, RBE and Damage to DNA Linear Energy Transfer (LET) When is stopping power not equal to LET? Stopping power (-de/dx) gives the energy lost by a charged particle in a medium. LET gives the energy absorbed
HEAVY PARTICLE THERAPY
 HEAVY PARTICLE THERAPY DR. G.V. GIRI KIDWAI MEMORIAL INSTITUTE OF ONCOLOGY ICRO 2012 BHATINDA HEAVY PARTICLES USED IN A EFFORT TO IMPROVE TUMOR CONTROL, THAT DO NOT RESPOND TO PHOTONS OR ELECTRONS BETTER
HEAVY PARTICLE THERAPY DR. G.V. GIRI KIDWAI MEMORIAL INSTITUTE OF ONCOLOGY ICRO 2012 BHATINDA HEAVY PARTICLES USED IN A EFFORT TO IMPROVE TUMOR CONTROL, THAT DO NOT RESPOND TO PHOTONS OR ELECTRONS BETTER
The Radiation Biology of Dose Fractionation: Determinants of Effect
 The Radiation Biology of Dose Fractionation: Determinants of Effect E. Day Werts, Ph.D. Department of Radiation Oncology West Penn Allegheny Radiation Oncology Network Allegheny General Hospital Historical
The Radiation Biology of Dose Fractionation: Determinants of Effect E. Day Werts, Ph.D. Department of Radiation Oncology West Penn Allegheny Radiation Oncology Network Allegheny General Hospital Historical
CHAPTER TWO MECHANISMS OF RADIATION EFFECTS
 10-2 densely ionizing radiation CHAPTER TWO MECHANISMS OF RADIATION EFFECTS 2.0 INTRODUCTION Cell survival curves describe the relationship between the fractional survival, S, of a population of radiated
10-2 densely ionizing radiation CHAPTER TWO MECHANISMS OF RADIATION EFFECTS 2.0 INTRODUCTION Cell survival curves describe the relationship between the fractional survival, S, of a population of radiated
Nuclear Data for Radiation Therapy
 Symposium on Nuclear Data 2004 Nov. 12, 2004 @ JAERI, Tokai Nuclear Data for Radiation Therapy ~from macroscopic to microscopic~ Naruhiro Matsufuji, Yuki Kase and Tatsuaki Kanai National Institute of Radiological
Symposium on Nuclear Data 2004 Nov. 12, 2004 @ JAERI, Tokai Nuclear Data for Radiation Therapy ~from macroscopic to microscopic~ Naruhiro Matsufuji, Yuki Kase and Tatsuaki Kanai National Institute of Radiological
Radiobiology of fractionated treatments: the classical approach and the 4 Rs. Vischioni Barbara MD, PhD Centro Nazionale Adroterapia Oncologica
 Radiobiology of fractionated treatments: the classical approach and the 4 Rs Vischioni Barbara MD, PhD Centro Nazionale Adroterapia Oncologica Radiobiology It is fundamental in radiation oncology Radiobiology
Radiobiology of fractionated treatments: the classical approach and the 4 Rs Vischioni Barbara MD, PhD Centro Nazionale Adroterapia Oncologica Radiobiology It is fundamental in radiation oncology Radiobiology
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Peak temperature ratio of TLD glow curves to investigate the spatial variation of LET in a clinical proton beam
 Peak temperature ratio of TLD glow curves to investigate the spatial variation of LET in a clinical proton beam University of Chicago CDH Proton Center LET study C. Reft 1, H. Ramirez 2 and M. Pankuch
Peak temperature ratio of TLD glow curves to investigate the spatial variation of LET in a clinical proton beam University of Chicago CDH Proton Center LET study C. Reft 1, H. Ramirez 2 and M. Pankuch
7/16/2009. An overview of classical radiobiology. Radiobiology and the cell kill paradigm. 1. Repair: Radiation cell killing. Radiation cell killing
 tcp 0.8 0.4 0.3 0.2 0.1 55 65 75 group 4 7/16/2009 An overview of classical radiobiology 5 or 6 R s of radiobiology and their impacts on treatments R Impact/exploitable effect 35 45 55 1. Repair Fractionation
tcp 0.8 0.4 0.3 0.2 0.1 55 65 75 group 4 7/16/2009 An overview of classical radiobiology 5 or 6 R s of radiobiology and their impacts on treatments R Impact/exploitable effect 35 45 55 1. Repair Fractionation
BASIC CLINICAL RADIOBIOLOGY
 INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
INT6062: Strengthening Capacity for Cervical Cancer Control through Improvement of Diagnosis and Treatment BASIC CLINICAL RADIOBIOLOGY Alfredo Polo MD, PhD Applied Radiation Biology and Radiotherapy Section
Chapter 14 Basic Radiobiology
 Chapter 14 Basic Radiobiology This set of 88 slides is based on Chapter 14 authored by N. Suntharalingam, E.B. Podgorsak, J.H. Hendry of the IAEA publication (ISBN 92-0-107304-6): Radiation Oncology Physics:
Chapter 14 Basic Radiobiology This set of 88 slides is based on Chapter 14 authored by N. Suntharalingam, E.B. Podgorsak, J.H. Hendry of the IAEA publication (ISBN 92-0-107304-6): Radiation Oncology Physics:
The Four R s. Repair Reoxygenation Repopulation Redistribution. The Radiobiology of Small Fraction Numbers. The Radiobiology of Small Fraction Numbers
 The Radiobiology of Small Fraction Numbers David J. Brenner, PhD, DSc Center for Radiological Research Columbia University Medical Center djb3@columbia.edu The Radiobiology of Small Fraction Numbers 1.
The Radiobiology of Small Fraction Numbers David J. Brenner, PhD, DSc Center for Radiological Research Columbia University Medical Center djb3@columbia.edu The Radiobiology of Small Fraction Numbers 1.
Fractionation: why did we ever fractionate? The Multiple Fractions School won! Survival curves: normal vs cancer cells
 1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
Chapter 4: The Physics and Biophysiology of Radiation Therapy. George E. Laramore
 Chapter 4: The Physics and Biophysiology of Radiation Therapy George E. Laramore The use of ionizing radiation in medicine dates back almost to the very date of its discovery. In 1895 Wilhelm Roentgen
Chapter 4: The Physics and Biophysiology of Radiation Therapy George E. Laramore The use of ionizing radiation in medicine dates back almost to the very date of its discovery. In 1895 Wilhelm Roentgen
Cell Survival vs Irradiation dose
 What have we learned from Radiation Treatment, and what I think will be the next generation ion therapy accelerators? S.Y. Lee, Department of Physics, Indiana University Cell Survival vs Irradiation dose
What have we learned from Radiation Treatment, and what I think will be the next generation ion therapy accelerators? S.Y. Lee, Department of Physics, Indiana University Cell Survival vs Irradiation dose
Therapeutic Medical Physics. Stephen J. Amadon Jr., Ph.D., DABR
 Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
PRINCIPLES and PRACTICE of RADIATION ONCOLOGY. Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology
 PRINCIPLES and PRACTICE of RADIATION ONCOLOGY Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology OUTLINE Physical basis Biological basis History of radiation therapy Treatment planning Technology
PRINCIPLES and PRACTICE of RADIATION ONCOLOGY Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology OUTLINE Physical basis Biological basis History of radiation therapy Treatment planning Technology
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Assistant Professor Department of Therapeutic Radiology Yale University School of Medicine
 A Mechanism-Based Approach to Predict Relative Biological i Effectiveness and the Effects of Tumor Hypoxia in Charged Particle Radiotherapy David J. Carlson, Ph.D. Assistant Professor Department of Therapeutic
A Mechanism-Based Approach to Predict Relative Biological i Effectiveness and the Effects of Tumor Hypoxia in Charged Particle Radiotherapy David J. Carlson, Ph.D. Assistant Professor Department of Therapeutic
Radiation qualities in carbon-ion radiotherapy at NIRS/HIMAC
 Radiation qualities in carbon-ion radiotherapy at NIRS/ Shunsuke YONAI Radiological Protection Section Research Center for Charged Particle Therapy National Institute of Radiological Sciences (NIRS) E-mail:
Radiation qualities in carbon-ion radiotherapy at NIRS/ Shunsuke YONAI Radiological Protection Section Research Center for Charged Particle Therapy National Institute of Radiological Sciences (NIRS) E-mail:
Radiation Oncology. Initial Certification Qualifying (Computer-based) Examination: Study Guide for Radiation and Cancer Biology
 Examination: Study Guide for Radiation and Cancer Biology") Radiation Oncology Initial Certification Qualifying (Computer-based) Examination: Study Guide for Radiation and Cancer Biology This exam tests your knowledge of the principles of cancer and radiation biology
Radiation Oncology Initial Certification Qualifying (Computer-based) Examination: Study Guide for Radiation and Cancer Biology This exam tests your knowledge of the principles of cancer and radiation biology
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: charged_particle_radiotherapy 3/12/96 5/2017 5/2018 5/2017 Description of Procedure or Service Charged-particle
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: charged_particle_radiotherapy 3/12/96 5/2017 5/2018 5/2017 Description of Procedure or Service Charged-particle
The Promise and Pitfalls of Mechanistic Modeling in Radiation Oncology
 The Promise and Pitfalls of Mechanistic Modeling in Radiation Oncology Robert D. Stewart, Ph.D. Associate Professor of Radiation Oncology University of Washington School of Medicine Department of Radiation
The Promise and Pitfalls of Mechanistic Modeling in Radiation Oncology Robert D. Stewart, Ph.D. Associate Professor of Radiation Oncology University of Washington School of Medicine Department of Radiation
Therapeutic ratio - An Overview. Past Present Future Prof Ramesh S Bilimaga
 Therapeutic ratio - An Overview Past Present Future Prof Ramesh S Bilimaga Radiation Oncology Discipline of human medicine concerned with the generation, conservation and dissemination of knowledge concerning
Therapeutic ratio - An Overview Past Present Future Prof Ramesh S Bilimaga Radiation Oncology Discipline of human medicine concerned with the generation, conservation and dissemination of knowledge concerning
Biological Optimization of Hadrontherapy. Uwe Oelfke
 4/2/2012 page 1 Biological Optimization of Hadrontherapy Uwe Oelfke DKFZ Heidelberg (E040) Im Neuenheimer Feld 280 69120 Heidelberg, Germany u.oelfke@dkfz.de 4/2/2012 page 2 Contents Introduction and General
4/2/2012 page 1 Biological Optimization of Hadrontherapy Uwe Oelfke DKFZ Heidelberg (E040) Im Neuenheimer Feld 280 69120 Heidelberg, Germany u.oelfke@dkfz.de 4/2/2012 page 2 Contents Introduction and General
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
New Thinking on Fractionation in Radiotherapy
 New Thinking on Fractionation in Radiotherapy Alan E. Nahum Visiting Professor, Physics dept., Liverpool university, UK alan_e_nahum@yahoo.co.uk 1 An honorarium is provided by Accuray for this presentation
New Thinking on Fractionation in Radiotherapy Alan E. Nahum Visiting Professor, Physics dept., Liverpool university, UK alan_e_nahum@yahoo.co.uk 1 An honorarium is provided by Accuray for this presentation
Neutrons. ρ σ. where. Neutrons act like photons in the sense that they are attenuated as. Unlike photons, neutrons interact via the strong interaction
 Neutrons Neutrons act like photons in the sense that they are attenuated as I = I 0 e μx where Unlike photons, neutrons interact via the strong interaction μ = The cross sections are much smaller than
Neutrons Neutrons act like photons in the sense that they are attenuated as I = I 0 e μx where Unlike photons, neutrons interact via the strong interaction μ = The cross sections are much smaller than
Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization*
 Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization* Barry W. Wessels, Ph.D 1 ; Amilia G. Di Dia, PhD 2 ;Yiran Zheng, PhD 1 Marta Cremonesi, PhD 2 1 University Hospitals
Isoeffective Dose Specification of Normal Liver in Yttrium-90 Microsphere Radioembolization* Barry W. Wessels, Ph.D 1 ; Amilia G. Di Dia, PhD 2 ;Yiran Zheng, PhD 1 Marta Cremonesi, PhD 2 1 University Hospitals
Neutron Radiotherapy: Past, Present, and Future Directions
 Neutron Radiotherapy: Past, Present, and Future Directions Theodore L. Phillips Lecture -- 2014 George E. Laramore Ph.D., M.D. NONE Conflicts of Interest Peter Wootton Professor of Radiation Oncology University
Neutron Radiotherapy: Past, Present, and Future Directions Theodore L. Phillips Lecture -- 2014 George E. Laramore Ph.D., M.D. NONE Conflicts of Interest Peter Wootton Professor of Radiation Oncology University
Radiation Damage Comparison between Intensity Modulated Radiotherapy (IMRT) and Field-in-field (FIF) Technique In Breast Cancer Treatments
 and Field-in-field (FIF) Technique In Breast Cancer Treatments") Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
Radiobiological Models in Brachytherapy Planning and Evaluation
 Therapy Educational Course (TH-C-108, 10:30-11:25 am): Radiobiological Models in Brachytherapy Planning and Evaluation Zhe (Jay) Chen, PhD & David J. Carlson, PhD Department of Therapeutic Radiology S
Therapy Educational Course (TH-C-108, 10:30-11:25 am): Radiobiological Models in Brachytherapy Planning and Evaluation Zhe (Jay) Chen, PhD & David J. Carlson, PhD Department of Therapeutic Radiology S
Determination and Use of Radiobiological Response Parameters in Radiation Therapy Optimization. Panayiotis Mavroidis
 Determination and Use of Radiobiological Response Parameters in Radiation Therapy Optimization Panayiotis Mavroidis Division of Medical Radiation Physics Department of Oncology-Pathology Karolinska Institutet
Determination and Use of Radiobiological Response Parameters in Radiation Therapy Optimization Panayiotis Mavroidis Division of Medical Radiation Physics Department of Oncology-Pathology Karolinska Institutet
Modelling the induction of cell death and chromosome damage by therapeutic protons
 Modelling the induction of cell death and chromosome damage by therapeutic protons M.P. Carante 1,2 and F. Ballarini 1,2, * 1 University of Pavia, Physics Department, Pavia, Italy 2 INFN, Sezione di Pavia,
Modelling the induction of cell death and chromosome damage by therapeutic protons M.P. Carante 1,2 and F. Ballarini 1,2, * 1 University of Pavia, Physics Department, Pavia, Italy 2 INFN, Sezione di Pavia,
Status of H 1 and C 12
 Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Status of H 1 and C 12 Herman Suit No Conflict of Interest 1 Goal of a New Treatment Modality Tumor Control Probability or No in Complication Rate 2 Truism No Advantage to: any Patient for any Radiation
Biological Effects of Ionizing Radiation & Commonly Used Radiation Units
 INAYA MEDICAL COLLEGE (IMC) RAD 232 - LECTURE 2 & 3 Biological Effects of Ionizing Radiation & Commonly Used Radiation Units DR. MOHAMMED MOSTAFA EMAM How does radiation injure people? - High energy radiation
INAYA MEDICAL COLLEGE (IMC) RAD 232 - LECTURE 2 & 3 Biological Effects of Ionizing Radiation & Commonly Used Radiation Units DR. MOHAMMED MOSTAFA EMAM How does radiation injure people? - High energy radiation
What is radiation quality?
 What is radiation quality? Dudley T Goodhead Medical Research Council, UK DoReMi Radiation Quality workshop Brussels. 9-10 July 2013 What is radiation quality? Let s start at the very beginning. A very
What is radiation quality? Dudley T Goodhead Medical Research Council, UK DoReMi Radiation Quality workshop Brussels. 9-10 July 2013 What is radiation quality? Let s start at the very beginning. A very
III. Proton-therapytherapy. Rome SB - 5/5 1
 Outline Introduction: an historical review I Applications in medical diagnostics Particle accelerators for medicine Applications in conventional radiation therapy II III IV Hadrontherapy, the frontier
Outline Introduction: an historical review I Applications in medical diagnostics Particle accelerators for medicine Applications in conventional radiation therapy II III IV Hadrontherapy, the frontier
Radiobiological modelling applied to Unsealed Source (radio) Therapy
 Therapy") Radiobiological modelling applied to Unsealed Source (radio) Therapy Alan E. Nahum Physics Department Clatterbridge Cancer Centre NHS Foundation Trust Bebington, Wirral CH63 4JY UK alan.nahum@clatterbridgecc.nhs.uk
Radiobiological modelling applied to Unsealed Source (radio) Therapy Alan E. Nahum Physics Department Clatterbridge Cancer Centre NHS Foundation Trust Bebington, Wirral CH63 4JY UK alan.nahum@clatterbridgecc.nhs.uk
Chapter 7. What is Radiation Biology? Ionizing Radiation. Energy Transfer Determinants 09/21/2014
 Chapter 7 Molecular & Cellular Radiation Biology What is Radiation Biology? A branch of biology concerned with how ionizing radiation effects living systems. Biological damage that occurs from different
Chapter 7 Molecular & Cellular Radiation Biology What is Radiation Biology? A branch of biology concerned with how ionizing radiation effects living systems. Biological damage that occurs from different
Treatment Planning (Protons vs. Photons)
") Treatment Planning Treatment Planning (Protons vs. Photons) Acquisition of imaging data Delineation of regions of interest Selection of beam directions Dose calculation Optimization of the plan Hounsfield
Treatment Planning Treatment Planning (Protons vs. Photons) Acquisition of imaging data Delineation of regions of interest Selection of beam directions Dose calculation Optimization of the plan Hounsfield
Clinical Applications of Brachytherapy Radiobiology. Radiobiology is Essential
 Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
Risk of secondary cancer induced by radiotherapy
 Risk of secondary cancer induced by radiotherapy Iuliana Toma-Dasu Medical Radiation Physics Stockholm University and Karolinska Institutet Radiation - the two-edged sword Risk of secondary cancer induced
Risk of secondary cancer induced by radiotherapy Iuliana Toma-Dasu Medical Radiation Physics Stockholm University and Karolinska Institutet Radiation - the two-edged sword Risk of secondary cancer induced
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Characterization and implementation of Pencil Beam Scanning proton therapy techniques: from spot scanning to continuous scanning
 Characterization and implementation of Pencil Beam Scanning proton therapy techniques: from spot scanning to continuous scanning Supervisors Prof. V. Patera PhD R. Van Roermund Candidate Annalisa Patriarca
Characterization and implementation of Pencil Beam Scanning proton therapy techniques: from spot scanning to continuous scanning Supervisors Prof. V. Patera PhD R. Van Roermund Candidate Annalisa Patriarca
Nature of Radiation and DNA damage
 Nature of Radiation and DNA damage Index 1. What is radiation? 2. Ionizing Radiation 3. Interaction of Gamma-radiation with Matter 4. Radiobiology 5. Direct and Indirect action of radiation 6. Steps of
Nature of Radiation and DNA damage Index 1. What is radiation? 2. Ionizing Radiation 3. Interaction of Gamma-radiation with Matter 4. Radiobiology 5. Direct and Indirect action of radiation 6. Steps of
Clinical considerations of RBE in proton therapy
 Clinical considerations of RBE in proton therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Why do we need the RBE
Clinical considerations of RBE in proton therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Why do we need the RBE
PTCOG 46. Educational Workshop Session IV. Head & Neck CLINICAL. J. Mizoe (NIRS, Japan)
") PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
Biological Indices for IMRT Evaluation and Optimization
 Biological Indices for IMRT Evaluation and Optimization Ellen D. Yorke Memorial Sloan-Kettering Cancer Center 1 9 8 7 6 5 4 3 2 1 Why biological indices? Dose distributions, DVHssurrogates for outcome
Biological Indices for IMRT Evaluation and Optimization Ellen D. Yorke Memorial Sloan-Kettering Cancer Center 1 9 8 7 6 5 4 3 2 1 Why biological indices? Dose distributions, DVHssurrogates for outcome
Biological Effects of Ionizing Radiation & Commonly Used Radiation Units
 INAYA MEDICAL COLLEGE (IMC) RAD 232 - LECTURE 3, 4 & 5 Biological Effects of Ionizing Radiation & Commonly Used Radiation Units DR. MOHAMMED MOSTAFA EMAM How does radiation injure people? - High energy
INAYA MEDICAL COLLEGE (IMC) RAD 232 - LECTURE 3, 4 & 5 Biological Effects of Ionizing Radiation & Commonly Used Radiation Units DR. MOHAMMED MOSTAFA EMAM How does radiation injure people? - High energy
Radiobiological Characterization of Clinical Proton and Carbon-Ion Beams
 Proceedings of the CAS-CERN Accelerator School: Accelerators for Medical Applications, Vösendorf, Austria, 26 May 5 June 2015, edited by R. Bailey, CERN Yellow Reports: School Proceedings, Vol. 1/2017,
Proceedings of the CAS-CERN Accelerator School: Accelerators for Medical Applications, Vösendorf, Austria, 26 May 5 June 2015, edited by R. Bailey, CERN Yellow Reports: School Proceedings, Vol. 1/2017,
Radiobiological principles of brachytherapy
 Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
UNC-Duke Biology Course for Residents Fall
 UNC-Duke Biology Course for Residents Fall 2018 1 UNC-Duke Biology Course for Residents Fall 2018 2 UNC-Duke Biology Course for Residents Fall 2018 3 UNC-Duke Biology Course for Residents Fall 2018 4 UNC-Duke
UNC-Duke Biology Course for Residents Fall 2018 1 UNC-Duke Biology Course for Residents Fall 2018 2 UNC-Duke Biology Course for Residents Fall 2018 3 UNC-Duke Biology Course for Residents Fall 2018 4 UNC-Duke
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
The temporal pattern of dose delivery in external beam radiotherapy
 University of Wollongong Research Online University of Wollongong Thesis Collection University of Wollongong Thesis Collections 2012 The temporal pattern of dose delivery in external beam radiotherapy
University of Wollongong Research Online University of Wollongong Thesis Collection University of Wollongong Thesis Collections 2012 The temporal pattern of dose delivery in external beam radiotherapy
PRINCIPLES OF RADIATION ONCOLOGY
 PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
MEDICAL MANAGEMENT POLICY
 PAGE: 1 of 8 This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage, the employer/member summary
PAGE: 1 of 8 This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage, the employer/member summary
Biological Effects of Radiation
 Radiation and Radioisotope Applications EPFL Doctoral Course PY-031 Biological Effects of Radiation Lecture 09 Rafael Macian 23.11.06 EPFL Doctoral Course PY-031: Radioisotope and Radiation Applications
Radiation and Radioisotope Applications EPFL Doctoral Course PY-031 Biological Effects of Radiation Lecture 09 Rafael Macian 23.11.06 EPFL Doctoral Course PY-031: Radioisotope and Radiation Applications
Side effects of radiotherapy.
 Side effects of radiotherapy. Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl Basics Techniques: Radiation type:
Side effects of radiotherapy. Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl Basics Techniques: Radiation type:
Hampton University Proton Therapy Institute
 Hampton University Proton Therapy Institute Brief introduction to proton therapy technology, its advances and Hampton University Proton Therapy Institute Vahagn Nazaryan, Ph.D. Executive Director, HUPTI
Hampton University Proton Therapy Institute Brief introduction to proton therapy technology, its advances and Hampton University Proton Therapy Institute Vahagn Nazaryan, Ph.D. Executive Director, HUPTI
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
La ricerca e la terapia in adroterapia-2. R.Orecchia / P. Fossati
 La ricerca e la terapia in adroterapia-2 R.Orecchia / P. Fossati Dose (Gy) = energy (joule) / mass (kg) One degree of fever (from 37.5 to 38.5 ) > 4000 Gy RT small dose big damage Photons : Dose Resposne
La ricerca e la terapia in adroterapia-2 R.Orecchia / P. Fossati Dose (Gy) = energy (joule) / mass (kg) One degree of fever (from 37.5 to 38.5 ) > 4000 Gy RT small dose big damage Photons : Dose Resposne
Figure 1.1 PHITS geometry for PTB irradiations with: broad beam, upper panel; mono energetic beams, lower panel. Pictures of the setups and of the
 Figure 1.1 PHITS geometry for PTB irradiations with: broad beam, upper panel; mono energetic beams, lower panel. Pictures of the setups and of the PMMA ring holder with 7 containers are also shown. Relative
Figure 1.1 PHITS geometry for PTB irradiations with: broad beam, upper panel; mono energetic beams, lower panel. Pictures of the setups and of the PMMA ring holder with 7 containers are also shown. Relative
HDR Applicators and Dosimetry*
 HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
HDR Applicators and Dosimetry* Jason Rownd, MS Medical College of Wisconsin *with a too much radiobiology Objectives Review the radiobiology of brachytherapy-linear quadratic model. Understand how to convert
RADIOBIOLOIGCALLY BASED TREATMENT PLANNING: THE NEXT FRONTIER. Teddy LaMaster, MS
 RADIOBIOLOIGCALLY BASED TREATMENT PLANNING: THE NEXT FRONTIER Teddy LaMaster, MS RADIOBIOLOGY Radiobiology is the interaction between ionizing radiation and living things. Varies for different cells, organs,
RADIOBIOLOIGCALLY BASED TREATMENT PLANNING: THE NEXT FRONTIER Teddy LaMaster, MS RADIOBIOLOGY Radiobiology is the interaction between ionizing radiation and living things. Varies for different cells, organs,
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015)
") PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
Ion Beam Therapy should we prioritise research on helium beams?
 Ion Beam Therapy should we prioritise research on helium beams? Stuart Green Medical Physics University Hospital Birmingham NHS Trust Follow-up from the EUCARD2 workshop, ION Beam Therapy: Clinical, Scientific
Ion Beam Therapy should we prioritise research on helium beams? Stuart Green Medical Physics University Hospital Birmingham NHS Trust Follow-up from the EUCARD2 workshop, ION Beam Therapy: Clinical, Scientific
Introduction to Radiation Biology
 Introduction to Radiation Biology Survey of Clinical Radiation Oncology Outline Ionizing radiation Development of radiobiological damage Cell cycle Cell survival curves Tissue response and fractionation
Introduction to Radiation Biology Survey of Clinical Radiation Oncology Outline Ionizing radiation Development of radiobiological damage Cell cycle Cell survival curves Tissue response and fractionation
University of Patras. School of Medicine Department of Medical Physics. MSc Thesis
 University of Patras School of Medicine Department of Medical Physics MSc Thesis Evaluation of dose-response models and determination of several radiobiological parameters. By Koussi Evanthia Serial Number:
University of Patras School of Medicine Department of Medical Physics MSc Thesis Evaluation of dose-response models and determination of several radiobiological parameters. By Koussi Evanthia Serial Number:
4.1.1 Dose distributions LKB effective volume or mean liver dose? The critical volume model TUMOUR CONTROL...
 1 CONTENTS 1 INTRODUCTION... 3 1.1 STEREOTACTIC BODY RADIATION THERAPY (SBRT)... 3 1.1.1 The development of SBRT... 3 1.1.2 The technique of SBRT... 4 1.1.3 Hypofractionation and inhomogeneous dose distribution...
1 CONTENTS 1 INTRODUCTION... 3 1.1 STEREOTACTIC BODY RADIATION THERAPY (SBRT)... 3 1.1.1 The development of SBRT... 3 1.1.2 The technique of SBRT... 4 1.1.3 Hypofractionation and inhomogeneous dose distribution...
Overview of Clinical and Research Activities at Georgetown University Hospital
 Overview of Clinical and Research Activities at Georgetown University Hospital Dalong Pang, Ph.D. Department of Radiation Medicine Georgetown University Hospital Clinical Operation Two Varian linear accelerators
Overview of Clinical and Research Activities at Georgetown University Hospital Dalong Pang, Ph.D. Department of Radiation Medicine Georgetown University Hospital Clinical Operation Two Varian linear accelerators
Hypofractionation and positioning in breast cancer radiation. John Hardie, M.D., Ph.D. November 2016
 Hypofractionation and positioning in breast cancer radiation John Hardie, M.D., Ph.D. November 2016 At McFarland/MGMC we treat early stage breast cancer with 42.4 Gy in 16 fractions, in the prone position.
Hypofractionation and positioning in breast cancer radiation John Hardie, M.D., Ph.D. November 2016 At McFarland/MGMC we treat early stage breast cancer with 42.4 Gy in 16 fractions, in the prone position.
Dosimetric Uncertainties and Normal Tissue Tolerance. Ellen D Yorke Memorial Sloan Kettering Cancer Center New York City
 Dosimetric Uncertainties and Normal Tissue Tolerance Ellen D Yorke Memorial Sloan Kettering Cancer Center New York City Traditional accuracy/precision goal is to deliver external beam radiation therapy
Dosimetric Uncertainties and Normal Tissue Tolerance Ellen D Yorke Memorial Sloan Kettering Cancer Center New York City Traditional accuracy/precision goal is to deliver external beam radiation therapy
Multi-Ion Analysis of RBE using the Microdosimetric Kinetic Model
 Multi-Ion Analysis of RBE using the Microdosimetric Kinetic Model Council of Ionizing Radiation Measurements and Standards (CIRMS) March 28 th, 2017 Michael P. Butkus 1,2 Todd S. Palmer 2 1 Yale School
Multi-Ion Analysis of RBE using the Microdosimetric Kinetic Model Council of Ionizing Radiation Measurements and Standards (CIRMS) March 28 th, 2017 Michael P. Butkus 1,2 Todd S. Palmer 2 1 Yale School
Post-Lumpectomy Radiation Techniques and Toxicities
 Post-Lumpectomy Radiation Techniques and Toxicities Laura Willson, MD Abbott Northwestern Hospital Dept. of Radiation Oncology February 2, 2019 Learning Objectives How radiation therapy works Standard
Post-Lumpectomy Radiation Techniques and Toxicities Laura Willson, MD Abbott Northwestern Hospital Dept. of Radiation Oncology February 2, 2019 Learning Objectives How radiation therapy works Standard
Today, I will present the second of the two lectures on neutron interactions.
 Today, I will present the second of the two lectures on neutron interactions. 1 The main goal of this lecture is to tell you a little about clinical neutron therapy, first with fast neutron beams, and
Today, I will present the second of the two lectures on neutron interactions. 1 The main goal of this lecture is to tell you a little about clinical neutron therapy, first with fast neutron beams, and
ACR TXIT TM EXAM OUTLINE
 ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
ISOEFFECT CALCULATION IN HDR BRACHYTHERAPY (BASIC CLINICAL RADIOBIOLOGY)
") ISOEFFECT CALCULATION IN HDR BRACHYTHERAPY (BASIC CLINICAL RADIOBIOLOGY) Alfredo Polo MD, PhD Division of Human Health International Atomic Energy Agency TYPES OF BRACHYTHERAPY PROCEDURES (ICRU REPORT
ISOEFFECT CALCULATION IN HDR BRACHYTHERAPY (BASIC CLINICAL RADIOBIOLOGY) Alfredo Polo MD, PhD Division of Human Health International Atomic Energy Agency TYPES OF BRACHYTHERAPY PROCEDURES (ICRU REPORT
BIOLOGICAL EFFECTS OF
 BIOLOGICAL EFFECTS OF RADIATION Natural Sources of Radiation Natural background radiation comes from three sources: Cosmic Radiation Terrestrial Radiation Internal Radiation 2 Natural Sources of Radiation
BIOLOGICAL EFFECTS OF RADIATION Natural Sources of Radiation Natural background radiation comes from three sources: Cosmic Radiation Terrestrial Radiation Internal Radiation 2 Natural Sources of Radiation
Proton Therapy Dosimetry & Clinical Implementation. Baldev Patyal, Ph.D., Chief Medical Physicist Department of Radiation Medicine
 Proton Therapy Dosimetry & Clinical Implementation Baldev Patyal, Ph.D., Chief Medical Physicist Department of Radiation Medicine Outline» Proton Therapy Basics» Why Proton Therapy? (Dosimetric Superiority)»
Proton Therapy Dosimetry & Clinical Implementation Baldev Patyal, Ph.D., Chief Medical Physicist Department of Radiation Medicine Outline» Proton Therapy Basics» Why Proton Therapy? (Dosimetric Superiority)»
Role of protons, heavy ions and BNCT in brain tumors
 Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
Progress of Heavy Ion Therapy
 Progress of Heavy Ion Therapy Fuminori Soga Division of Accelerator Physics and Engineering, National Institute of Radiological Sciences, 4-9-1 Anagawa. Inage-ku, Chiba 263-8555, Japan 1. Introduction
Progress of Heavy Ion Therapy Fuminori Soga Division of Accelerator Physics and Engineering, National Institute of Radiological Sciences, 4-9-1 Anagawa. Inage-ku, Chiba 263-8555, Japan 1. Introduction
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Risk of a second cancer after radiotherapy
 Risk of a second cancer after radiotherapy Francesco d Errico University of Pisa, Italy Yale University, USA Medical radiological procedures worldwide 2.5 billion diagnostic radiological examinations 78%
Risk of a second cancer after radiotherapy Francesco d Errico University of Pisa, Italy Yale University, USA Medical radiological procedures worldwide 2.5 billion diagnostic radiological examinations 78%
The Impact of Cobalt-60 Source Age on Biologically Effective Dose in Gamma Knife Thalamotomy
 The Impact of Cobalt-60 Source Age on Biologically Effective Dose in Gamma Knife Thalamotomy BH Kann, JB Yu, J Bond, C Loiselle, VL Chiang, RS Bindra, JL Gerrard, DJ Carlson Leksell Gamma Knife Society
The Impact of Cobalt-60 Source Age on Biologically Effective Dose in Gamma Knife Thalamotomy BH Kann, JB Yu, J Bond, C Loiselle, VL Chiang, RS Bindra, JL Gerrard, DJ Carlson Leksell Gamma Knife Society
Spinal cord response to altered fractionation and re-irradiation: Radiobiological considerations and role of bioeffect models
 Original Article Free full text available from www.cancerjournal.net Spinal cord response to altered fractionation and re-irradiation: Radiobiological considerations and role of bioeffect models ABSTRACT
Original Article Free full text available from www.cancerjournal.net Spinal cord response to altered fractionation and re-irradiation: Radiobiological considerations and role of bioeffect models ABSTRACT
Scoring of linear energy transfer (LET) for calculation of biological dose in proton therapy
 for calculation of biological dose in proton therapy") Scoring of linear energy transfer (LET) for calculation of biological dose in proton therapy And why biological calculation should be done within FLUKA Eivind Rørvik May 11, 216 Eivind Rørvik 4th Fluka
Scoring of linear energy transfer (LET) for calculation of biological dose in proton therapy And why biological calculation should be done within FLUKA Eivind Rørvik May 11, 216 Eivind Rørvik 4th Fluka
Radiation Therapy 2013 The Role of Protons. Bob Gaston, D.O.
 Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
Radiation Therapy 2013 The Role of Protons Bob Gaston, D.O. Disclosures Oklahoma ProCure Treatment Center Radiation Medicine Associates Goal of Radiation Therapy Increase the Therapeutic Ratio Therapeutic
8/3/2016. Clinical Significance of RBE Variations in Proton Therapy. Why RBE (relative biological effectiveness)?
?") 8//06 Clinical Significance of Variations in Proton Therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Introduction
8//06 Clinical Significance of Variations in Proton Therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Introduction
Modelling of Biological Processes
 Modelling of Biological Processes WHAT HAPPENS AFTER EARLY MOLECULAR DAMAGE? Stephen McMahon Queen s University, Belfast, Northern Ireland 3 rd August 2016 1 Do we need biology? The Linear-quadratic relationship
Modelling of Biological Processes WHAT HAPPENS AFTER EARLY MOLECULAR DAMAGE? Stephen McMahon Queen s University, Belfast, Northern Ireland 3 rd August 2016 1 Do we need biology? The Linear-quadratic relationship
ProtonTherapy: A ballistic that will benefit patients? Pr. Xavier Geets MIRO Lab, IREC UCL Radiotherapy Dept. CUSL, Belgium
 ProtonTherapy: A ballistic that will benefit patients? Pr. Xavier Geets MIRO Lab, IREC UCL Radiotherapy Dept. CUSL, Belgium Proton Therapy, a swissknife The balistic advantage of protons P PHOTON THERAPY
ProtonTherapy: A ballistic that will benefit patients? Pr. Xavier Geets MIRO Lab, IREC UCL Radiotherapy Dept. CUSL, Belgium Proton Therapy, a swissknife The balistic advantage of protons P PHOTON THERAPY
Dose escalation in permanent brachytherapy for prostate cancer: dosimetric and biological considerations*
 INSTITUTE OF PHYSICS PUBLISHING Phys. Med. Biol. 48 (2003) 2753 2765 PHYSICS IN MEDICINE AND BIOLOGY PII: S0031-9155(03)62377-8 Dose escalation in permanent brachytherapy for prostate cancer: dosimetric
INSTITUTE OF PHYSICS PUBLISHING Phys. Med. Biol. 48 (2003) 2753 2765 PHYSICS IN MEDICINE AND BIOLOGY PII: S0031-9155(03)62377-8 Dose escalation in permanent brachytherapy for prostate cancer: dosimetric
Proceedings of the Eleventh International Conference on Cyclotrons and their Applications, Tokyo, Japan
 FAST NEUTRONS AND PROTONS IN CANCER TREATMENT WITH THE MEDICAL CYCLOTRON AT NIRS H.Tsunemoto and S. Morita National Institute of Radiol ogical Sci ences 9-1, Anagawa 4- chome, Chiba-shi 260, JAPAN SUMMERY
FAST NEUTRONS AND PROTONS IN CANCER TREATMENT WITH THE MEDICAL CYCLOTRON AT NIRS H.Tsunemoto and S. Morita National Institute of Radiol ogical Sci ences 9-1, Anagawa 4- chome, Chiba-shi 260, JAPAN SUMMERY
Physical Bases : Which Isotopes?
 Physical Bases : Which Isotopes? S. Gnesin Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland 1/53 Theranostic Bruxelles, 2 Octobrer 2017 Theranostic : use of diagnostic
Physical Bases : Which Isotopes? S. Gnesin Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland 1/53 Theranostic Bruxelles, 2 Octobrer 2017 Theranostic : use of diagnostic
The dependence of optimal fractionation schemes on the spatial dose distribution
 The dependence of optimal fractionation schemes on the spatial dose distribution Jan Unkelbach 1, David Craft 1, Ehsan Salari 1, Jagdish Ramakrishnan 1,2, Thomas Bortfeld 1 1 Department of Radiation Oncology,
The dependence of optimal fractionation schemes on the spatial dose distribution Jan Unkelbach 1, David Craft 1, Ehsan Salari 1, Jagdish Ramakrishnan 1,2, Thomas Bortfeld 1 1 Department of Radiation Oncology,