Kathleen R. Fink, MD Virginia Mason Medical Center. 6 th Nordic Emergency Radiology Course 2017
|
|
|
- Darleen Allen
- 6 years ago
- Views:
Transcription

1 Kathleen R. Fink, MD Virginia Mason Medical Center 6 th Nordic Emergency Radiology Course 2017
2 Disclosure My spouse receives research salary support from: Guerbet
3 Outline Acute neck and back pain Acute spine entities: Vascular Inflammatory Neoplasm
4 Acute back and neck pain
5 Acute back pain: Who to image? Low back pain: Imaging generally not recommended if there are no red flags Radiculopathy: Most acute radiculopathies improve with conservative care, thus waiting 6 weeks or more prior to imaging is reasonable Many acutely herniated disks resolve with time Low Back Pain: Evidence-Based Neuroimaging in Evidence-Based Neuroimaging Diagnosis and Treatment. New York: Springer p
6 Red Flags: Trauma Unexplained weight loss Age > 50 years, especially women, and males with osteoporosis or compression fracture Unexplained fever, history of infection Prolonged corticosteroid use, osteoporosis Focal neurological deficits with progressive or disabling symptoms, cauda equina syndrome Duration longer than 6 weeks Prior surgery Immunosuppression, diabetes History of malignancy Intravenous drug abuse ACR appropriateness criteria: Low Back Pain acr.org accessed April Jarvik et al. JAMA. 2015;313(11): doi: /jama


7 39 year old with left low back pain, left foot numbness, weakness and tingling. 2 nd ER visit.

8 MR obtained for clinical worsening.
9 Disk herniation Left L4-5 disk extrusion Compresses the left L5 nerve root in the lateral recess Nerve edema But is imaging indicated?


10 47 year old with acute right greater than left leg pain and urinary incontinence



11 Cauda Equina syndrome Syndrome: Saddle Anesthesia Urinary retention Severe or progressive deficit in lower extremities. **Not radiculopathy** Neurosurgical emergency: Better outcome, particularly of bowel and bladder dysfunction, with early decompression.
 Fever, weight loss, etc.")
12 Acute neck pain Like low back pain, many people experience neck pain. Many cases resolve within 6 weeks. Red flags: Trauma Rhematoid arthritis or Downs (risk of atlantoaxial subluxation) Fever, weight loss, etc. Upper motor neuron signs (myelopathy) Age <20 or >50 Associated chest pain or signs of myocardial infarction Stroke symptoms (carotid or vertebral artery dissection),cohen 2015 Mayo Clinic Proceedings 90 (2):
13 Vascular

14 70 year old critically ill man, acute weakness and sensory loss

15 Cord infarct Slightly expanded cord Increased T2/STIR signal Axial: gray matter involved May enhance DWI sequence may help MRA not helpful anterior spinal artery too small to see.

16 Cord infarct: causes Atherosclerosis Thoracoabdominal aneurysm Aortic surgery Systemic hypotension Dissection Coagulopathy
17 29 year old with LLE weakness, progressed to inability to walk.
18

19 Cord hemorrhage Low T1 and T2 indicating hemorrhage. Cord edema throughout spine No enhancing lesion Spinal angiogram negative DDx: Dural arteriovenous fistula/malformation Cavernous malformation Hemorrhagic mass lesion No underlying cause in this case (spontaneous hemorrhage)

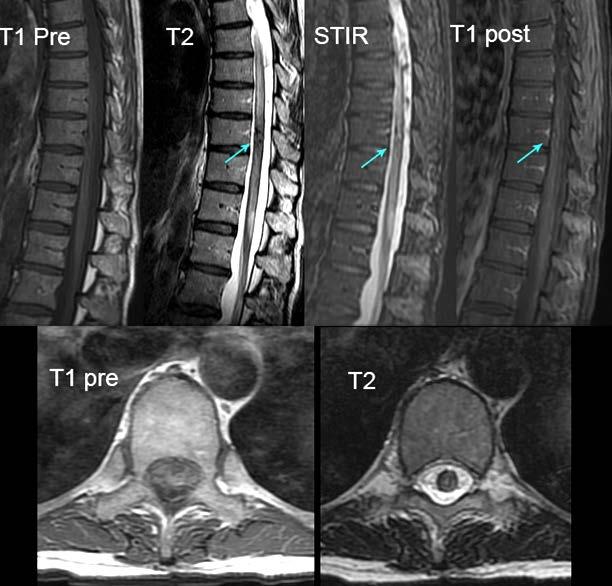
20 60 year old man with progressive sensory loss from toes up, followed by weakness. Symptoms waxed and waned

21 Different patient, same diagnosis

22 Spinal dural AVF Enlarged edematous cord Prominent flow voids on cord surface Vessels enhance Spinal angiogram is gold standard for diagnosis. Endovascular treatment common Foix Alajounine syndrome
23 69 year old, progressive RLE weakness, numbness, urinary retention



24 T1 Post T1 T2


25 T2

26 Cavernous malformation AKA: Cavernoma, cavernous angioma, cavernous hemangioma T1: Popcorn appearance T2: Heterogeneous with hypointense hemosiderin ring Contrast: minimal or absent enhancement T2
27 Inflammatory conditions

28 35 year old with ascending sensory level and LE weakness

29 Transverse myelitis Cord lesion > 2 vertebral segments long > 2/3 axial area of cord affected Cord expansion Variable enhancement Thoracic more common T2
30 Transverse myelitis: causes Idiopathic Secondary (AKA transverse myelopathy) Autoimmune disease - SLE, Sjogren, Sarcoidosis, Mixed connective tissue disease Viral - EBV, CMV, Herpes zoster, VZV, HIV, HTLV-1, enterovirus Other infection - Syphilis, Lyme, Mycoplasma, Shistosomiasis Post vaccination immune response Post irradiaton Para-neoplastic syndrome - Lung, breast, HCC - Lymphoma, leukemia, multiple myeloma

31 Transverse myelitis: DDx MS: Generally < 2 vertebral segments Neoplasm: Edema, cystic ± hemorrhage areas, slow symptom onset Cord infarct Neuromyelitis optica spectrum ADEM T2


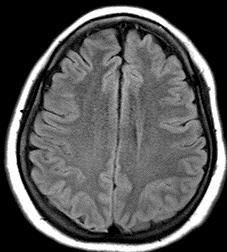
32 35 year old woman, blurred vision T2





33 Diagnosis? FLAIR T2 FLAIR T1 post Diagnostic Criteria for Multiple Sclerosis: 2010 Revisions to the McDonald Criteria." Annals of neurology 69, no. 2 (2011):

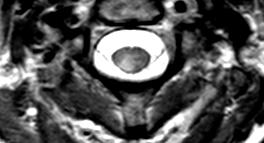
34 Multiple Sclerosis Oval, peripheral, asymmetric lesions Usually discrete Affects gray and white matter May enhance if acute/subacute Late stage: cord atrophy ** With brain lesions: MS Isolated spinal disease may occur T2




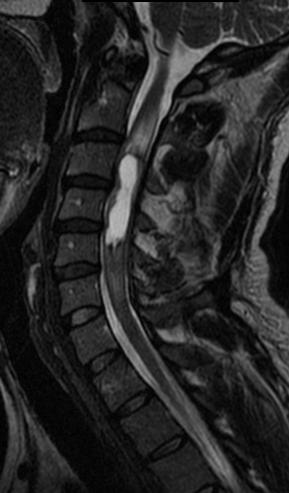
35 22 year old with upper extremity weakness and dysesthesias T2 T2 T1 post T1 post

36 Findings/differential Two long segment lesions T2 hyperintense Enhancing Mild cord expansion DDX: Demyelination - MS - ADEM - NMO Transverse myelitis Intrinsic cord tumor

37 Diagnosis? FLAIR

38 Neuromyelitis optica spectrum disorder Predominantly spine and optic nerve involvement Long lesions > 3 segments T2 involves entire cross section of cord. Brain MR classically described as normal, but brain lesions may occur


39 Cervical ependymoma T2 T1 T1 post
40 Masses/neoplasms


41 76 year old, fall with back pain +
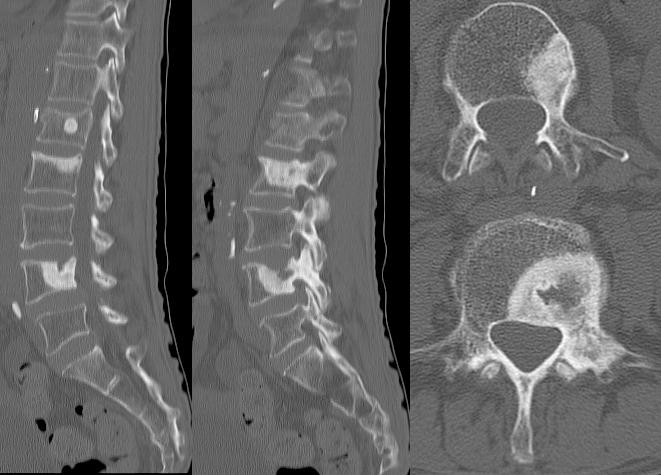
42 CT
43 Sclerotic bone mets L1 compression fracture. Always evaluate the pedicles

44 64 yo with 10 days of back pain

45 Metastatic RCC Decreased T1, increased T2/STIR and enhancement in bone Posterior vertebral body, then pedicle involvement Spares disk Draped curtain appearance epidural extension FS T1 post
46 Findings helpful in differential Metastasis Complete marrow replacement Convex bulge of posterior border Pedicle involvement Epidural mass Insufficiency Band-like low signal on T1WI Vacuum cleft May enhance acutely




47 Tumor versus infection Metastasis Osteomyelitis

48 35 year old with back pain T1 FS T1 post
49 Myxopapillary ependymoma Intensely enhancing ovoid mass at conus, filum, or cauda equina Can fill canal T1 isointense to cord (this example is hypointense) T2 hyperintense to cord Most common primary spinal cord tumor in adults FS T1 post

50 35 year old, progressive myelopathy T1 post
51 Meningioma Intradural extramedullary enhancing mass T1 isointense to cord T2 isointense or hyperintense Prominent enhancement ± dural tail T1 post


52 35 year old with radiculopathy T2 FS T1 post T1

53 Schwanomma T1 iso- or hypointense Usually T2 hyperintense T2 May be cystic or hemorrhagic Intense enhancement Dumbbell shape as exits foramen Thoracic most common FS T1 post


54 56 year old with breast cancer FS T1 post
 Germinoma Choroid plexus")
55 Leptomeningeal carcinomatosis Nodular enhancement along spinal cord and nerve roots Metastatic disease Breast cancer Lung cancer Melanoma Lymphoma Primary CNS tumors GBM Medulloblastoma PNET Ependymoma (NOT myxopapillary) Germinoma Choroid plexus carcinoma
56 Outline Acute neck and back pain Acute spine entities: Infectious Vascular Inflammatory Neoplasm
57 Thank you! Kathleen Fink
11 May Disclosure. + Outline: Acute Spine Emergencies
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet K Fink Nordic
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet K Fink Nordic
Imaging the Spinal Cord & Intradural Disease
 Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW
 Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW DISCLOSURES I have no industry relationships to disclose. I will not discuss off-label use. OBJECTIVES: TRANSVERSE MYELITIS Review
Seema Sikka, MD January 18, 2014 TRANSVERSE MYELITIS: A CLINICAL OVERVIEW DISCLOSURES I have no industry relationships to disclose. I will not discuss off-label use. OBJECTIVES: TRANSVERSE MYELITIS Review
Spinal cord tumours Luc van den Hauwe et al.
 overview spinal cord tumours L. van den Hauwe 1,2, D. Balériaux 3, J.W. Van Goethem 2, C. Venstermans 2, F. De Belder 2, P.M. Parizel 2 introduction imaging spinal tumour classification spinal cord tumours
overview spinal cord tumours L. van den Hauwe 1,2, D. Balériaux 3, J.W. Van Goethem 2, C. Venstermans 2, F. De Belder 2, P.M. Parizel 2 introduction imaging spinal tumour classification spinal cord tumours
Paraparesis. Differential Diagnosis. Ran brauner, Tel Aviv university
 Paraparesis Differential Diagnosis Ran brauner, Tel Aviv university Definition Loss of motor power to both legs Paraparesis (paraplegia) refers to partial (- paresis) or complete (-plegia) loss of voluntary
Paraparesis Differential Diagnosis Ran brauner, Tel Aviv university Definition Loss of motor power to both legs Paraparesis (paraplegia) refers to partial (- paresis) or complete (-plegia) loss of voluntary
Introduction to Neuroimaging spine. John J. McCormick MD
 Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
Spinal Vascular Lesions
 Spinal Vascular Lesions Spinal Vascular Lesions Spinal cord infarction Hemangioblastoma Cavernous malformation Vascular malformations (Type 1-4) Spinal artery aneurysm Troy Hutchins, MD Assistant Professor
Spinal Vascular Lesions Spinal Vascular Lesions Spinal cord infarction Hemangioblastoma Cavernous malformation Vascular malformations (Type 1-4) Spinal artery aneurysm Troy Hutchins, MD Assistant Professor
Pediatric Spine Tumors (and other masses)
") Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Spine. Neuroradiology. Spine. Spine Pathology. Distribution of fractures. Radiological algorithm. Role of radiology 18/11/2015
 Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Spinal Neoplasms. First Things First!! Localize the Lesion!! Ependymomas. Common Intramedullary Lesions
 Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
A Journey Down The Canal
 A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
Emergency Neurological Life Support Spinal Cord Compression
 Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Vertebral and Paravertebral Diseases
 Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Ependymoma of the spine
 Ependymoma of the spine Tenny Zhang, MS-3 Harvard Medical School 1 Case presentation: history and exam HPI: A 30-year-old man with no significant past medical history presents with one week of bilateral
Ependymoma of the spine Tenny Zhang, MS-3 Harvard Medical School 1 Case presentation: history and exam HPI: A 30-year-old man with no significant past medical history presents with one week of bilateral
NEURORADIOLOGY. Part III. Angela Csomor University of Szeged Department of Radiology
 NEURORADIOLOGY Part III Angela Csomor University of Szeged Department of Radiology DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders inflammatory processes
NEURORADIOLOGY Part III Angela Csomor University of Szeged Department of Radiology DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders inflammatory processes
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
MRI and differential diagnosis in patients suspected of having MS
 Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Andrea Falini Italy MRI and differential diagnosis in patients suspected of having MS IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Outline of presentation - Diagnostic criteria
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
MRI in Differential Diagnosis. CMSC, June 2, Jill Conway, MD, MA, MSCE
 MRI in Differential Diagnosis CMSC, June 2, 2016 Jill Conway, MD, MA, MSCE Director, Carolinas MS Center Clerkship Director, UNCSOM-Charlotte Campus Charlotte, NC Disclosures Speaking, consulting, and/or
MRI in Differential Diagnosis CMSC, June 2, 2016 Jill Conway, MD, MA, MSCE Director, Carolinas MS Center Clerkship Director, UNCSOM-Charlotte Campus Charlotte, NC Disclosures Speaking, consulting, and/or
AMERICAN ACADEMY OF NEUROLOGY SPINE FELLOWSHIP CORE CURRICULUM
 AMERICAN ACADEMY OF NEUROLOGY SPINE FELLOWSHIP CORE CURRICULUM Introduction Spine conditions affect virtually everyone at some time during their life. Surveys indicate a yearly prevalence of spine-related
AMERICAN ACADEMY OF NEUROLOGY SPINE FELLOWSHIP CORE CURRICULUM Introduction Spine conditions affect virtually everyone at some time during their life. Surveys indicate a yearly prevalence of spine-related
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
Difficult Diagnosis: Case History. 7 months prior, she happened to have undergone a C-spine MRI after a car accident
 Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Relevant Disclosures: None Difficult Diagnosis: Recent Advances in Neurology 2013 Jeffrey M. Gelfand, MD Assistant Professor UCSF Neuroinflammation and MS Center UCSF Department of Neurology Case History
Objectives. Identify and differentiate appropriate surgical cases. Good Surgical Outcomes
 ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
Contrast Guidelines for Common CT/CTA & MRI/MRA
 Contrast Guidelines for Common /A & /MRA Body Imaging Gastrointestinal CLINICAL GUIDELINES EXAM DESCRIPTION /A CPT CODES EXAM DESCRIPTION /MRA CPT CODES Abdominal mass Abdomen & Pelvis w 74177 Abdomen
Contrast Guidelines for Common /A & /MRA Body Imaging Gastrointestinal CLINICAL GUIDELINES EXAM DESCRIPTION /A CPT CODES EXAM DESCRIPTION /MRA CPT CODES Abdominal mass Abdomen & Pelvis w 74177 Abdomen
Back pain and bladder problems
 Back pain and bladder problems Search Learn the causes and symptoms of chronic back pain, as well as safe techniques that provide back pain relief better than prescriptions drugs. If back pain is reducing
Back pain and bladder problems Search Learn the causes and symptoms of chronic back pain, as well as safe techniques that provide back pain relief better than prescriptions drugs. If back pain is reducing
Chiropractic Health Plan - Diagnosis of Low Back Pain
 Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Overview. Spinal Anatomy Spaces & Meninges Spinal Cord. Anatomy of the dura. Anatomy of the arachnoid. Anatomy of the spinal meninges
 European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
Patient Chart Quotes. Spine Mythology and Evidence- Based Management of Back Pain. Patient Chart Quotes. Patient Chart Quotes
 Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES Author : RITA GONÇALVES Categories : Vets Date : April 7, 2014 RITA
Vet Times The website for the veterinary profession https://www.vettimes.co.uk SPINAL CORD DISEASE IN DOGS PART TWO: MOST LIKELY CAUSES Author : RITA GONÇALVES Categories : Vets Date : April 7, 2014 RITA
Interactive Cases: Demyelinating Diseases and Mimics. Disclosures. Case 1 25 yo F with nystagmus; look for tumor 4/14/2017
 Interactive Cases: Demyelinating Diseases and Mimics Disclosures None Brad Wright, MD 27 March 2017 Case 1 25 yo F with nystagmus; look for tumor What do you suspect? A. Demyelinating disease B. Malignancy
Interactive Cases: Demyelinating Diseases and Mimics Disclosures None Brad Wright, MD 27 March 2017 Case 1 25 yo F with nystagmus; look for tumor What do you suspect? A. Demyelinating disease B. Malignancy
Demyelinating Diseases of the Brain
 Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
Chapter 35 Back Pain. Episode overview: Wisecracks: Crack Cast Show Notes Back Pain July 2016
 Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION
 CLINICAL VIGNETTE 2017; 3:2 SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION Editor-in-Chief: Idowu, Olufemi E. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria.
CLINICAL VIGNETTE 2017; 3:2 SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION Editor-in-Chief: Idowu, Olufemi E. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria.
RADICULOPATHY AN INTRODUCTION TO
 AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
PMH: No medications; Immunizations UTD No hospitalizations or surgeries Speech Delay. Birth Hx: 24 WGA, NICU x6 months
 HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
HPI: 6 months of weakness and parathesias- originally in both feet x 2-3 months, then resolved. Now with parathesias and weakness in fingers x 1 week. Seen by podiatrist and given custom in-soles 1 month
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto
 Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
References 1. Feng S et al. Journal of Thoracic Oncology 2017; 12: Spain L et al. Annals of Oncology 2017; 28:
 Maulik Shah, MD February 15, 2019 Patient Presentation: Progressive Sensory Disturbance In early 2018, this 57 year old man was sent to the Emergency Department after complaining in the oncology clinic
Maulik Shah, MD February 15, 2019 Patient Presentation: Progressive Sensory Disturbance In early 2018, this 57 year old man was sent to the Emergency Department after complaining in the oncology clinic
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Actualização no diagnóstico e tratamento das doenças desmielinizantes na infância. Silvia Tenembaum
 Actualização no diagnóstico e tratamento das doenças desmielinizantes na infância Silvia Tenembaum Acquired CNS inflammatory/demyelinating disorders: Background information More frequent in children than
Actualização no diagnóstico e tratamento das doenças desmielinizantes na infância Silvia Tenembaum Acquired CNS inflammatory/demyelinating disorders: Background information More frequent in children than
Imaging Degeneration of the Lumbar Spine: What It All Means.
 Imaging Degeneration of the Lumbar Spine: What It All Means www.fisiokinesiterapia.biz Spine Nomenclature and Evidence for Imaging p, Talk Objectives Background Nomenclature for disc findings Who should
Imaging Degeneration of the Lumbar Spine: What It All Means www.fisiokinesiterapia.biz Spine Nomenclature and Evidence for Imaging p, Talk Objectives Background Nomenclature for disc findings Who should
Historical perspective
 SPINAL AVM Introduction Vascular malformations of spinal cord are a rare clinical entity, representing 5% of all primary spinal cord lesions, with arteriovenous malformations(avm) & cavernous malformations
SPINAL AVM Introduction Vascular malformations of spinal cord are a rare clinical entity, representing 5% of all primary spinal cord lesions, with arteriovenous malformations(avm) & cavernous malformations
Acute and subacute non-traumatic myelophaties.
 Acute and subacute non-traumatic myelophaties. Poster No.: C-0906 Congress: ECR 2016 Type: Educational Exhibit Authors: M. Jimenez De La Peña, J. Carrascoso Arranz, L. Gómez 1 3 2 3 4 Vicente, R. Garcia
Acute and subacute non-traumatic myelophaties. Poster No.: C-0906 Congress: ECR 2016 Type: Educational Exhibit Authors: M. Jimenez De La Peña, J. Carrascoso Arranz, L. Gómez 1 3 2 3 4 Vicente, R. Garcia
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Myelitis. Case 2. History. Examination. Mahtab Ghadiri
 Case 2 Myelitis Mahtab Ghadiri History A 42-year-old man presented to the emergency department with altered sensation in the lower limbs and difficulty ambulating. He first noted paresthesia in his feet
Case 2 Myelitis Mahtab Ghadiri History A 42-year-old man presented to the emergency department with altered sensation in the lower limbs and difficulty ambulating. He first noted paresthesia in his feet
Alan H Daniels, MD. Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University
 Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The Pathology of Transverse Myelitis Carlos A. Pardo, MD
 Page 8 main a member of the TMA, because we are committed to making a difference for you and we care about you! We are going to remain the TMA; it may become a vestigial name reflecting the state of medical
Page 8 main a member of the TMA, because we are committed to making a difference for you and we care about you! We are going to remain the TMA; it may become a vestigial name reflecting the state of medical
1/9/2013 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE. Introduction. Classification for Extramedullary Tumors
 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
Tony Traboulsee, MD Associate Professor (Medicine/Neurology) Head, UBC MS and NMO Programs. MRI Diagnostic Red Flags
 Head, UBC MS and NMO Programs. MRI Diagnostic Red Flags") Tony Traboulsee, MD Associate Professor (Medicine/Neurology) Head, UBC MS and NMO Programs MRI Diagnostic Red Flags UBC MS and NMO Research Programs LEARNING OBJECTIVES By the end of this presentation,
Tony Traboulsee, MD Associate Professor (Medicine/Neurology) Head, UBC MS and NMO Programs MRI Diagnostic Red Flags UBC MS and NMO Research Programs LEARNING OBJECTIVES By the end of this presentation,
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Dumbbell Shaped Thoracic Spine Cavernous Hemangioma: A Case Report and Review of the Literature
 ISPUB.COM The Internet Journal of Neurosurgery Volume 3 Number 1 Dumbbell Shaped Thoracic Spine Cavernous Hemangioma: A Case Report and Review of the Literature J Gonzalez-Cruz, A Nanda Citation J Gonzalez-Cruz,
ISPUB.COM The Internet Journal of Neurosurgery Volume 3 Number 1 Dumbbell Shaped Thoracic Spine Cavernous Hemangioma: A Case Report and Review of the Literature J Gonzalez-Cruz, A Nanda Citation J Gonzalez-Cruz,
Patologie infiammatorie encefaliche e midollari
 Patologie infiammatorie encefaliche e midollari Maria Laura Stromillo Department of Medicine, Surgery and Neuroscience Inflammatory disorders of the CNS NMOSD ADEM Multiple Sclerosis Neuro-Myelitis Optica
Patologie infiammatorie encefaliche e midollari Maria Laura Stromillo Department of Medicine, Surgery and Neuroscience Inflammatory disorders of the CNS NMOSD ADEM Multiple Sclerosis Neuro-Myelitis Optica
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Giant cystic intradural extramedullary pilocytic astrocytoma of Cauda equina
 1 di 7 13/03/2014 09.02 J Neurosci Rural Pract. 2013 Oct-Dec; 4(4): 453 456. doi: 10.4103/0976-3147.120217 PMCID: PMC3858770 Giant cystic intradural extramedullary pilocytic astrocytoma of Cauda equina
1 di 7 13/03/2014 09.02 J Neurosci Rural Pract. 2013 Oct-Dec; 4(4): 453 456. doi: 10.4103/0976-3147.120217 PMCID: PMC3858770 Giant cystic intradural extramedullary pilocytic astrocytoma of Cauda equina
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome
 A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
A pictorial review of neurological complications of systemic lupus erythematosus and antiphospholipid syndrome Poster No.: C-2780 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: E. Tavernaraki,
Vascular Malformations
 Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Radiological Appearance of Extra-axial CNS Hemangioma
 Chin J Radiol 2002; 27: 183-190 183 Radiological Appearance of Extra-axial CNS Hemangioma MING-SHIANG YANG CLAYTON CHI-CHANG CHEN WEN-HSIEN CHEN HAO-CHUN HUNG SAN-KAN LEE Department of Radiology, Taichung
Chin J Radiol 2002; 27: 183-190 183 Radiological Appearance of Extra-axial CNS Hemangioma MING-SHIANG YANG CLAYTON CHI-CHANG CHEN WEN-HSIEN CHEN HAO-CHUN HUNG SAN-KAN LEE Department of Radiology, Taichung
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
1st interactive course in MS advanced managment
 6-7 December - Toronto, Canada 1st interactive course in MS advanced managment IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Liesly Lee Sunnybrook Health Sciences Centre. Department
6-7 December - Toronto, Canada 1st interactive course in MS advanced managment IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Liesly Lee Sunnybrook Health Sciences Centre. Department
Role of MRI in the Evaluation of Compressive Myelopathy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. XIII (Apr. 2016), PP 21-26 www.iosrjournals.org Role of MRI in the Evaluation of Compressive
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. XIII (Apr. 2016), PP 21-26 www.iosrjournals.org Role of MRI in the Evaluation of Compressive
Disclosure. + Outline. Case-based approach to neurological emergencies that might present to the ED
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
4/14/2017. Unknown Case #1 Intramedullary Lesion
 4/14/2017 Intradural, Intramedullary Tumor or Mimic Intradural, Extramedullary Tumor or Mimic Extradural Tumor or Mimic Unknown Case #1 Intramedullary Lesion Unknown Case #1 -POST - MAG AXIAL Cranial Caudal
4/14/2017 Intradural, Intramedullary Tumor or Mimic Intradural, Extramedullary Tumor or Mimic Extradural Tumor or Mimic Unknown Case #1 Intramedullary Lesion Unknown Case #1 -POST - MAG AXIAL Cranial Caudal
Chapter 96 Spinal Cord
 Chapter 96 Spinal Cord Episode overview 1. Describe the arterial supply of the spinal cord 2. Label the spinal cord, and describe the major ascending and descending tracts 3. List the features of transverse
Chapter 96 Spinal Cord Episode overview 1. Describe the arterial supply of the spinal cord 2. Label the spinal cord, and describe the major ascending and descending tracts 3. List the features of transverse
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
Clinician s Guide To Ordering NeuroImaging Studies
 Clinician s Guide To Ordering NeuroImaging Studies MRI CT South Jersey Radiology Associates The purpose of this general guide is to assist you in choosing the appropriate imaging test to best help your
Clinician s Guide To Ordering NeuroImaging Studies MRI CT South Jersey Radiology Associates The purpose of this general guide is to assist you in choosing the appropriate imaging test to best help your
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
MRI of chronic spinal cord injury
 The British Journal of Radiology, 76 (2003), 347 352 DOI: 10.1259/bjr/11881183 E 2003 The British Institute of Radiology Pictorial review MRI of chronic spinal cord injury 1 K POTTER, FRCR and 1 A SAIFUDDIN,
The British Journal of Radiology, 76 (2003), 347 352 DOI: 10.1259/bjr/11881183 E 2003 The British Institute of Radiology Pictorial review MRI of chronic spinal cord injury 1 K POTTER, FRCR and 1 A SAIFUDDIN,
MYELITIS. A Mochan Neurology
 MYELITIS A Mochan Neurology ATM MS LETM NMOSD ATM LETM MS NMOSD Acute Transverse Myelitis Longitudinally Extensive Transverse Myelitis Multiple Sclerosis Neuromyelitis Optica Spectrum Disorders ATM ADEM
MYELITIS A Mochan Neurology ATM MS LETM NMOSD ATM LETM MS NMOSD Acute Transverse Myelitis Longitudinally Extensive Transverse Myelitis Multiple Sclerosis Neuromyelitis Optica Spectrum Disorders ATM ADEM
1 Normal Anatomy and Variants
 1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS
 Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS") A Pain in the Back GPCE Workshop Sydney Olympic Park May 22-24, 2015 Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS www.cnsneurosurgery.com.au VMO Neurosurgeon
A Pain in the Back GPCE Workshop Sydney Olympic Park May 22-24, 2015 Speaker: Dr Gautam (Vini) Khurana MBBS (Syd, Hons), BScMed (Syd, Medal), PhD (Mayo Clinic), FRACS www.cnsneurosurgery.com.au VMO Neurosurgeon
Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions
 Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute
 A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
Title: Recurrent myelitis after allogeneic stem cell transplantation. Report of two cases.
 Author's response to reviews Title: Recurrent myelitis after allogeneic stem cell transplantation. Report of two cases. Authors: Martin Voss (Martin.Voss@kgu.de) Felix Bischof (Felix.Bischof@uni-tuebingen.de)
Author's response to reviews Title: Recurrent myelitis after allogeneic stem cell transplantation. Report of two cases. Authors: Martin Voss (Martin.Voss@kgu.de) Felix Bischof (Felix.Bischof@uni-tuebingen.de)
NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE
 THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
Neuromyelitis optica (NMO), or Devic s disease, is a rare
, or Devic s disease, is a rare") Case Report Neuromyelitis Optica (NMO) Abstract NMO is a is a rare entity which involves the central nervous system acting as an inflammatory process by attacking the optic nerve (ON) and longitudinally
Case Report Neuromyelitis Optica (NMO) Abstract NMO is a is a rare entity which involves the central nervous system acting as an inflammatory process by attacking the optic nerve (ON) and longitudinally
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
HERNIATED DISCS AN INTRODUCTION TO
 AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO HERNIATED S This booklet provides general information on herniated discs. It is not meant to replace any personal conversations that you might wish to have with your physician or other
MRI Imaging of Neuromyelitis Optica
 July 2009 MRI Imaging of Neuromyelitis Optica Jenna Nolan, Harvard Medical School Year III Gillian Lieberman, MD Our Patient: Initial Presentation J.H. is a 29 year-old woman who presents with acute vision
July 2009 MRI Imaging of Neuromyelitis Optica Jenna Nolan, Harvard Medical School Year III Gillian Lieberman, MD Our Patient: Initial Presentation J.H. is a 29 year-old woman who presents with acute vision
Module 1: Basic Comprehensive Course
 The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
LOW BACK PAIN EPIDEMIOLOGY:
 LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽
 외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Case 7391 Intraventricular Lesion
 Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Magnetic resonance imaging of intramedullary spinal cord lesions
 Magnetic resonance imaging of intramedullary spinal cord lesions Poster No.: C-1762 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Abdelkafi, H. Derbel, H. Abid, S. Haddar, B. Souissi, N. 1 1
Magnetic resonance imaging of intramedullary spinal cord lesions Poster No.: C-1762 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Abdelkafi, H. Derbel, H. Abid, S. Haddar, B. Souissi, N. 1 1
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy