Conflict of interest disclosure
|
|
|
- Melina Pope
- 6 years ago
- Views:
Transcription
1 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have no conflict of interest to disclose. Stereotactic Body Radiation Therapy (SBRT) II: Physics and Dosimetry Considerations Stanley H. Benedict, Ph.D. University of Virginia Kamil Yenice, Ph.D. University of Chicago AAPM th Annual Meeting, Houston, Texas Therapy Continuing Education Course: SBRT: I & II Monday, July 28, 2008: 7:30 9:25AM Outline Evolution from conventional RT to SRS to SBRT Epidemiology, Rationale, Indications using SBRT for spinal metastases Radiobiology of SBRT MD Anderson clinical pathway for spinal metastases Summary of Results from Literature Case presentations Summary and conclusion IG-IMSRT Evolution Historically fractionated RT required large safety margins ~2cm around tumor for treatment uncertainties Associated with unacceptable toxicity at single dose levels needed for tumor response CT-treatment planning, and hi-precision targeting with stereotaxy has permitted safe delivery of single-dose RT to intracranial lesions (SRS) with very small to no margins 1




 Current SBRT")




2 IG-IMSRT Evolution Evolution of intracranial SRS to SBRT SRS for brain metastasis yields: 1-, 2-yr FFP 50% for Gy and >80% for 22-24Gy (Vogelbaum, J Neurosurg 104:907-12, 2006) Current SBRT technology includes IG robotic techniques, MLC, inverse planning software to generate IMRT plans conforming to tumor with steep dose gradients needed near OARs such as spinal cord Intracranial SRS Extracranial SBRT delivery systems 2

 at sometime during their illness 1 40% of skeletal metastases occur in the spine which is")

3 IJROBP 71:484-90, pts Gy x 1 Spinal cord <12-14 Gy Cauda max 15.6 Gy LC 90% F/U 15mos OS 15mos Background on Spinal Metastases Epidemiology of Spinal Metastases A common sequelae of cancer, present in 30 70% patients at post mortem examination, of which 14% will be symptomatic (pain, neurologic sx s) at sometime during their illness 1 40% of skeletal metastases occur in the spine which is the most common osseous site of tumor spread Conventional radiation therapy widely used but is inherently limited by spinal cord tolerance SBRT SBRT? 1 Perrin RG. Metastatic tumors of the axial spine. Curr Opin Oncol 1992:4: Klimo, P. et al. Oncologist2004;9:
4 RATIONALE GENERAL INDICATIONS Many pts develop recurrent or progressive pain, tumor progression or neurologic deterioration despite conventional external beam irradiation, radiopharmaceuticals, surgery, or systemic therapy Patients are very interested in noninvasive treatment options for spinal metastases which are not amenable to or are refractory to conventional irradiation LIMITED DISEASE - Newly diagnosed solitary or oligo- spinal metastases PRIMARY - Radioresistant subtypes POST-OP adjuvant or elective treatment SALVAGE - surgical or RT recurrences Spinal instability is a contraindication Radiosensitive lymphomas, germ cell tumors etc. Therapeutic Window for conventional RT 4

5 Previously irradiated spinal cord, melanomas Renal cell cancer, sarcomas etc. SBRT dosimetrically widens the therapeutic window by lowering dose to the OAR OAR Little or no therapeutic window exists for conventional irradiation Limitations in the linear-quadratic model for high doses D T is transition dose at which final portion of curve become linear Astrahan M, IJROBP 71:3:963,2008 Astrahan M, IJROBP 71:3:963,2008 5

6 Single Fraction Equivalent Dose (SFED) vs BED For high dose ablative RT Defined -as dose in a single fx that would have same biological effect as any large daily dose fractionation regimen Park C, Timmerman RD, IJROBP 71:3:963-4,2008. Park C, Timmerman RD, IJROBP 71:3:963-4,2008. Spinal Cord Radiation Exposure 50% 10% 20% 80% B 20% 90% C A 50% 80% Park C, Timmerman RD, IJROBP 71:3:963-4,2008 (a) (b) Henry Ford group proposes 10 Gy to 10% spinal cord as tolerance Ryu S et al. Cancer 109: , % 6
")
7 White Matter Necrosis of Rat spinal cord Major cause of paralysis Occurs within days after irradiation 20 Gy x 1 Pathogenesis focused on either primary glial or vascular origin Characterized by demyelination, loss of axons, focal necrosis, liquefactive necrosis after > 20 Gy x 1 Vascular edema is usually associated with development of white matter necrosis Isoeffect Dose (ED 50 ) according to irradiated length of rat cord 20mm 8mm 4mm 2mm Bijl HP et al. Van Der Kogel AJ, IJROBP 52:205-11,2002 Single Bijl HP et al. Van Der Kogel AJ, IJROBP 52:205-11,2002 High precision proton irradiation of rat spinal cord Grazing Lateral Beams (constant depth dose profile) Central Beam Bijl HP et al. Van Der Kogel AJ, IJROBP 52:205-11,2002 Bijl HP et al, IJROBP 61: ,

8 Regional Differences in Radiosensitivity in Rat Spinal Cord Dose-response Curves for Paralysis White matter necrosis in left lat column after grazing irradiation Full width And Lateral beam Central Beam Bijl HP et al, IJROBP 61: , 2005 Extensive white Matter necrosis in Dorsal column No lesions in gray Matter or lateral columns Bijl HP et al, IJROBP 61: , 2005 Bath/Shower Dose-response of Paralysis of Limbs to Unmodulated Protons in Rat Cervical Spinal Cord Clinical Pathway for Stereotactic Body Radiotherapy progra Referral from neurosurgery medical oncology radiation oncology self referral Multi-disciplinary Tumor board Patient selection Discussion of complex cases Triaging candidates Joint consultation pain, QOL assessment, Neurological exam, informed consent,video, Protocol registration SBRT simulation 1. immobilization 2. intrathecal contrast 3. CT acquisition Spinal cord tolerance of relatively small volumes (shower) strongly affected by low dose irradiation (bath) Bijl HP et al. IJROBP 64: , 2006 IMRT treatment planning Q/A dosimetry -film -ion chamber Protocol follow-up q3 months pain,qol,neuro exam, MRI Treatment setup CT acquisition image fusion, DRR, port film, delivery Spine recurrence Or new disease 8
 F/u (mos) Outcome cxs Chang 2007 63 Mets 30/5 or 27/3 9mo 85% control 0 Ryu 2007 Yamada 2008 177 93 Mets Mets 8-18 18-24 6.4 (0.")
 /4-31fxs 12mo 2 progression 0 Gerszten 2007 336 Mets 20(12-25) 21(3-53) LTC 90% 0 Yamada 2005 35 Primary and metastases 70/33 20/5 11mo M81% LC 0 Dodd 2006 19 Benign 16-30/1-5fxs 23 3worse 0 Dodd")
9 Selected stereotactic spine radiation therapy series (FRACTIONATED) Series N Pathology Dose F/U Outcome cxs Selected stereotactic spine radation series (SINGLE SESSION) Milker-zabel Mets mo 13/15 Pain relief 0 Series N Path Dose (Gy) F/u (mos) Outcome cxs Chang Mets 30/5 or 27/3 9mo 85% control 0 Ryu 2007 Yamada Mets Mets (0.5-49) 15 (2-45) 85% pain relief 90% 1 radiation injury 0 Bilsky Primary and metastases /33-38fxs 20 ( ) /4-31fxs 12mo 2 progression 0 Gerszten Mets 20(12-25) 21(3-53) LTC 90% 0 Yamada Primary and metastases 70/33 20/5 11mo M81% LC 0 Dodd Benign 16-30/1-5fxs 23 3worse 0 Dodd 2006 Gibbs 2007 Total Benign Mets /1-5fx 16-25/ mo 9mo 9-23mo 3 increased symptoms 84% Symptomatic improvement >80% 1 (3%) 3 severe mypthy 4/222 cases (1.8%) Benzil 2004 Total mets 9prim 25/ x NA 2-45mos Pain relief 32/34 tumors ~90% 2radiculit 1 rad necrosis 4/656 (0.6%) M.D. ANDERSON PHASE I AND II DATA Patient Positioning Accuracy and Safety Data Int J Radiat Oncol Biol Phys 59: ,
10 RESULTS - Patient Characteristics Dates enrolled Nov 2002 Mar 2005 Patients n 63 Male 38 (60%) Female 25 (40%) Age (yrs) Median 59 Range Histology Renal cell 25 (39.7%) Breast 9 (14.3%) Sarcoma 8 (12.7%) Lung 7 (11.1%) Melanoma 2 (3.2%) Colon 1 (1.6%) Unk Primary 2 (3.2%) Other 9 (14.3%) KPS score 60 4 (6.3%) (27%) (27%) (39.7%) RESULTS - Tumor Characteristics Tumor volume (cc) median 37.4 range Spinal Metastases (n) One 51 Two 12 Lesion Location Spinal 61 Paraspinal 13 Level cervical 5 (6.7%) thoracic 43 (57%) lumbar 26 (34.7%) sacral 1 (1.3%) RESULTS - Follow-up of Tumor and Vital Status Vital Status alive 26 (41%) dead 37 (59%) Tumor status Stable 57 (77%) Progressed 17 (23%) Follow-up Median 21.3 mos Range mos 10
, 44% (3mos), 36%")
, sleep disturbance(p<0.")
11 PAIN AND SYMPTOM CONTROL Pain incidence Pain severity 6.7% Narcotic use decreased from 60% (baseline), 44% (3mos), 36% (6mos) MDASI showed reduction in pain (p<0.001), sleep disturbance(p<0.01) with no added impairment of daily function, while fatigue severity unchanged. 11
 Fatigue (1) Non-cardiac chest pain (1) Pain, severe tongue edema, trismus (1) Grade 4 None Reported Toxicity in Literature CLINICAL CASES Fractionated")
12 Neurotoxicity evaluation Grade 1 headache (1) numbness (1)* tingling (4)* numbness and tingling (1)* (all reversible) Grade 2-4 none Grade 3-4 toxicity Grade 3 Nausea (1) Fatigue (1) Non-cardiac chest pain (1) Pain, severe tongue edema, trismus (1) Grade 4 None Reported Toxicity in Literature CLINICAL CASES Fractionated SBRT 12





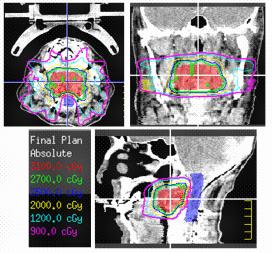


13 Case1: 46 M previously irradiated (40 Gy in 16 fxs) Lung cancer T12 metastasis progressed (biopsy proven) Case2: 52 M solitary renal cell carcinoma metastasis centered on cervical vertebrae 2 July 2004 July


14 Case3: 20 F plasmacytoma causing back pain, failed conventional RT and surgery -Extradural extension causing cord compression at T10 -Needle bx revealed plasmacytoma -45 Gy in 25 fractions to T9-11 Neuroforaminal and Epidural Disease -3 mos later, recurred below: Epidural dz T RT was not an option at the time -Laminectomy, facetectomy, resection tumor -4 mo later recurred above: Rt T7-8 neuroforamen -Received SBRT to epidural disease -Attending college and remains disease-free 4 years later Patterns of Failure 14
15 Summary and conclusions Literature and phase I/II data support the safety and effectiveness of stereotactic body radiosurgery for the spine POF data suggest routinely treating the pedicles and posterior elements using a wide bony margin posterior to the diseased vertebrae. Prospective trials are needed to determine the true spinal cord tolerance and to compare efficacy of SBRS against conventional RT All the following are indications for performing stereotactic body radiosurgery for spinal metastases EXCEPT?: 1. Solitary or oligometastatic disease 2. Failure of prior XRT or surgery 3. Spinal instability 4. Gross residual disease after surgery 10 Based on pooled published data on spinal metastases, SBRT is associated with a crude local control rate of: The following statements regarding spinal cord tolerance to single session steretoactic body radiosurgery (SBRS) are true EXCEPT: % % % 4. 80% or higher 1. Human spinal cord tolerance unknown 2. <12 Gy has been reported as safe Gy to 10% of the spinal cord volume 4. Rat spinal cord tolerance can be directly applied to humans
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Disclosure. Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed to make this presentation possible!
 were harmed to make this presentation possible!") Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
8/2/2018. Acknowlegements: TCP SPINE. Disclosures
 A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Disclosure SBRT. SBRT for Spinal Metastases 5/2/2010. No conflicts of interest. Overview
 Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
brain SPINE 2 SRS Matures into breast lung spine LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable Lung Cancer BRAIN
 NEWS AND ADVANCES IN THE MANAGEMENT AND TREATMENT OF SERIOUS DISEASE brain SPINE 2 SRS Matures into Mainstream Extracranial Technique lung spine breast LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable
NEWS AND ADVANCES IN THE MANAGEMENT AND TREATMENT OF SERIOUS DISEASE brain SPINE 2 SRS Matures into Mainstream Extracranial Technique lung spine breast LUNG Dr. Robert Timmerman Discusses SBRT for Inoperable
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Current Concepts and Trends in Spinal Radiosurgery. Edward M. Marchan
 Current Concepts and Trends in Spinal Radiosurgery Edward M. Marchan Spinal Neoplasia The spine is the most common site of skeletal metastatic disease. (70%) 40% of bony metastases involve the vertebrae
Current Concepts and Trends in Spinal Radiosurgery Edward M. Marchan Spinal Neoplasia The spine is the most common site of skeletal metastatic disease. (70%) 40% of bony metastases involve the vertebrae
Radiotherapy What are our options and what is on the horizon. Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology
 Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015
 Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
Tania Kaprealian, M.D. Assistant Professor UCLA Department of Radiation Oncology August 22, 2015 Most common brain tumor, affecting 8.5-15% of cancer patients. Treatment options: Whole brain radiation
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
a Phase II Randomised Controlled Trial Matthias Guckenberger
 Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
8/3/2017. Spine SBRT: A Clinician's Update On Techniques and Outcomes. Disclosures. Outline
 Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Vertebral Body Compression Fracture Following Spine SBRT
 RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
Can we hit the target? Can we put the dose where we want it? Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy
 Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
Quality Assurance in Stereotactic Radiosurgery and Fractionated Stereotactic Radiotherapy David Shepard, Ph.D. Swedish Cancer Institute Seattle, WA Timothy D. Solberg, Ph.D. University of Texas Southwestern
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
This LCD recognizes these two distinct treatment approaches and is specific to treatment delivery:
 National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
Overview of MLC-based Linac Radiosurgery
 SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
Stereotactic Radiosurgery. Extracranial Stereotactic Radiosurgery. Linear accelerators. Basic technique. Indications of SRS
 Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Stereotactic Radiosurgery Extracranial Stereotactic Radiosurgery Annette Quinn, MSN, RN Program Manager, University of Pittsburgh Medical Center Using stereotactic techniques, give a lethal dose of ionizing
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Chapter 5 Section 3.1
 Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
HDR Brachytherapy for Skin Cancers. Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital
 HDR Brachytherapy for Skin Cancers Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital No conflicts of interest Outline Case examples from Fairfax Hospital Understand radiation s mechanism
HDR Brachytherapy for Skin Cancers Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital No conflicts of interest Outline Case examples from Fairfax Hospital Understand radiation s mechanism
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
STEREOTACTICALLY- GUIDED SPINAL RADIOSURGERY
 1. Introduction Mark Sedrak M.D., Zachary A. Smith M.D., Ausaf Bari M.D., Michael Selch M.D., Antonio A.F. De Salles M.D. Ph.D. Hamilton et al. first described spinal SRS in 1995 using a linear accelerator.
1. Introduction Mark Sedrak M.D., Zachary A. Smith M.D., Ausaf Bari M.D., Michael Selch M.D., Antonio A.F. De Salles M.D. Ph.D. Hamilton et al. first described spinal SRS in 1995 using a linear accelerator.
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 04/01/2017
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 04/01/2017
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE. Geoffrey S. Ibbott, Ph.D. June 20, 2017
 FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Innovative RT SBRT. The variables with REQ in superscript are required.
 The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
Original Date: April 2016 Page 1 of 7 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Stereotactic Radiosurgery/Radiotherapy. What is Stereotaxis? Available Systems. Almon S. Shiu, Ph.D
 Stereotactic Radiosurgery/Radiotherapy Almon S. Shiu, Ph.D Radiation Physics Department University of Texas M. D. Anderson Cancer Center Houston, Texas What is Stereotaxis? A Method for locating points
Stereotactic Radiosurgery/Radiotherapy Almon S. Shiu, Ph.D Radiation Physics Department University of Texas M. D. Anderson Cancer Center Houston, Texas What is Stereotaxis? A Method for locating points
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Stereotactic ablative radiotherapy in early NSCLC and metastases
 Stereotactic ablative radiotherapy in early NSCLC and metastases Scheduled: 0810-0830 hrs, 10 March 2012 Professor Suresh Senan Department of Radiation Oncology SABR in stage I NSCLC A major treatment
Stereotactic ablative radiotherapy in early NSCLC and metastases Scheduled: 0810-0830 hrs, 10 March 2012 Professor Suresh Senan Department of Radiation Oncology SABR in stage I NSCLC A major treatment
Despite advances in the care of primary malignant
 J Neurosurg Spine 14:537 542, 2011 Efficacy and cost-effectiveness analysis of external beam and stereotactic body radiation therapy in the treatment of spine metastases: a matched-pair analysis Clinical
J Neurosurg Spine 14:537 542, 2011 Efficacy and cost-effectiveness analysis of external beam and stereotactic body radiation therapy in the treatment of spine metastases: a matched-pair analysis Clinical
Special Procedures Rotation I/II SBRT, SRS, TBI, and TSET
 University of Michigan Department of Radiation Oncology Division of Radiation Physics Special Procedures Rotation I/II SBRT, SRS, TBI, and TSET Resident: Rotation staff mentor/ advisor: _Scott Hadley,
University of Michigan Department of Radiation Oncology Division of Radiation Physics Special Procedures Rotation I/II SBRT, SRS, TBI, and TSET Resident: Rotation staff mentor/ advisor: _Scott Hadley,
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Radiotherapy Considerations in Extremity Sarcoma
 Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Radiotherapy Considerations in Extremity Sarcoma Peter Chung Department of Radiation Oncology Princess Margaret Hospital University of Toronto Role of RT in STS Local tumour eradication while allowing
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Treatment Planning & IGRT Credentialing for NRG SBRT Trials
 Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
11/27/2017. Modern Treatment of Meningiomas. Disclosures. Modern is Better? No disclosures relevant to this presentation
 Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
CPT code semantics 8/18/2011. SBRT Planning Case Studies. Spectrum of applications of SBRT. itreat
 Spectrum of applications of SBRT EDUCATIONAL COURSE Physics and Dosimetry of SBRT Part III: Planning Case Studies Brian D. Kavanagh, MD, MPH Department of Radiation Oncology University of Colorado School
Spectrum of applications of SBRT EDUCATIONAL COURSE Physics and Dosimetry of SBRT Part III: Planning Case Studies Brian D. Kavanagh, MD, MPH Department of Radiation Oncology University of Colorado School
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Stereotaxy. Outlines. Establishing SBRT Program: Physics & Dosimetry. SBRT - Simulation. Body Localizer. Sim. Sim. Sim. Stereotaxy?
 Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
Establishing SBRT Program: Physics & Dosimetry Lu Wang, Ph.D. Radiation Oncology Department Fox Chase Cancer Center Outlines Illustrate the difference between SBRT vs. CRT Introduce the major procedures
UCSF Uveal Melanoma Program: Outcomes with Proton Beam Radiation Therapy Kavita K. Mishra, M.D., M.P.H. UCSF Comprehensive Cancer Center
 Disclosures UCSF Uveal Melanoma Program: Outcomes with Proton Beam Radiation Therapy No disclosures Kavita K. Mishra, M.D., M.P.H. UCSF Comprehensive Cancer Center UCSF Uveal Melanoma Program: Ocular Melanoma
Disclosures UCSF Uveal Melanoma Program: Outcomes with Proton Beam Radiation Therapy No disclosures Kavita K. Mishra, M.D., M.P.H. UCSF Comprehensive Cancer Center UCSF Uveal Melanoma Program: Ocular Melanoma
Disclosures 5/13/2013. Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013
 Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
Radiotherapy and Brain Metastases. Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem
 Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Radiotherapy and Brain Metastases Dr. K Van Beek Radiation-Oncologist BSMO annual Meeting Diegem 24-02-2017 Possible strategies Watchful waiting Surgery Postop RT to resection cavity or WBRT postop SRS
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/20/2015
Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Policy Number: Original Effective Date: MM.05.008 05/12/1999 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/20/2015
Brain metastases: changing visions
 Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Brain metastases: changing visions Roberto Spiegelmann, MD Baiona, 2014 Head, Stereotactic Radiosurgery Unit Dept of Neurosurgery, Chaim Sheba Medical Center Tel Hashomer, Israel The best current estimate
Role of SBRT in the management of lung and liver metastases. Ronan TANGUY, M.D. Radiation Oncologist
 Role of SBRT in the management of lung and liver metastases Ronan TANGUY, M.D. Radiation Oncologist Oligometastatic RCC mrcc: Lung, Bone, Liver, Brain (Schlesinger-Raab, EJC2008) Targeted therapies Objective
Role of SBRT in the management of lung and liver metastases Ronan TANGUY, M.D. Radiation Oncologist Oligometastatic RCC mrcc: Lung, Bone, Liver, Brain (Schlesinger-Raab, EJC2008) Targeted therapies Objective
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors
 Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas
 Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
-Proton Beam Therapy in Paediatric Radiation Oncology -
 -Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
-Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
ARROCase Brain Metastases
 ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
ARROCase Brain Metastases Colin Hill*, Daniel M. Trifiletti*, Timothy N. Showalter*, Jason P. Sheehan Radiation Oncology* and Neurosurgery University of Virginia Charlottesville, VA Case: HPI 64 year old
20. Background. Oligometastases. Oligometastases: bone (including spine) and lymph nodes
 and lymph nodes") 125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
ASTRO econtouring for Lymphoma. Stephanie Terezakis, MD
 ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
Treating Multiple. Brain Metastases (BM)
") ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,