Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
|
|
|
- August Norton
- 5 years ago
- Views:
Transcription


1 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures None Disclosures None



2 Introduction Up to 70% of cancer patients will harbor spinal metastatic disease Cancer will become leading cause of death in western hemisphere

3 Clinical Experience has Expanded Orthopaedic Spine Surgery Principles of Musculoskeletal Oncology Neurosurgery Spine Oncology Surgery 7 The Changing Face of Spine Oncology: Key Developments and an Innovative Research Model Key Developments Surgical, Biologic, Radiation, Research Models Spine Oncology has become truly Multidisciplinary Knowledge Translation and Expansion Is it occurring in Spine Tumors? 8 SPINAL TUMOURS Primary Metastatic 9 3




4 SPINAL TUMOURS Decision Making Primary Metastatic 10 SPINAL TUMOURS Primary Metastatic 11 SPINAL TUMOURS Primary Metastatic 12 4
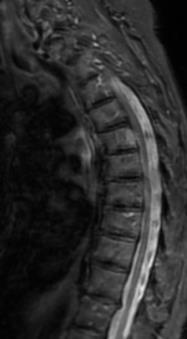
5 Patient reports symptoms suggestive of Malignant Spinal Cord Compression: Patient has history of cancer and one of the following: Severe Intractable Progressive Pain Especially Thoracic New Spinal Nerve Root Pain (Burning, Numb, Shooting) Any New Difficulty Walking Reduced Power/Altered Sensation in Limbs Bowel/Bladder disturbance Aim to start treatment within 24 hours. General Practitioner District Nurse/AHP Specialist (could also include OOH Secondary Care Macmillan Suspects Nurses & NHS 24) Suspects MSCC Nurses MSCC Suspects MSCC suspects MSCC Phones (add tel number) MSCC Coordinator 9-5 Monday Friday or to Out of Hours on-call Clinical Oncology SpR Information needed (see TVCN Referral form) Name and date of birth of patient Symptoms suggesting MSCC and onset History of cancer (type, stage) Signs on examination Coordinator ensures: Admitted to appropriate local acute service and acute service are made aware. MRI arranged/already performed. Steriods started (16mg Dexamethasone stat and 8mg b.d.) as soon as possible after assessment (unless contraindicated). Advice sought from relevant oncologist. Assessment will help inform Clinical Oncology SpR if MRI is required Patients should not be informed of possibility of MRI until referrer discusses symptoms with Clinical Oncology SpR. MSCC unlikely MSCC likely or Patient fit enough for treatment if known patient is not fit enough for treatment or fitness unknown Clinical Oncology SpR: Patients will be treated as potentially unstable spines and Advises on management of patient appropriate transport arranged to local acute medical unit by referrer or Arranges review of patient Spine unstable transport arranged by referrer or Acute local service confirms steroid commenced and updates Discusses case with appropriate specialist clinical assessment as per referral proforma. MRI -ve MRI reported to admitting team. Team informs MSCC Coordinator. MSCC Coordinator completes the referral proforma. Images tranferred to appropriate Oncology Consultant. MRI +ve Treatment decision made in consultation with Oncology Consultant. Organise urgent CT if appropriate i.e. patient suitable for surgical treatment Surgery not option Surgery option Clinical Oncology SpR proceeds with treatment planning Spinal Consultant proceeds with treatment planning 13 Pitfall - Lack of consistency Oncological Disease specific vs site specifc Heterogenous repertoire Entrenched opinion Surgical Lack of awareness Challenging surgery Lack of capacity Entrenched opinion 14 Decision Making in Spine Metastases What have we firmly established? Surgery + Radiation Is better than Radiation alone 15 5
6 Decision Making in Spine Metastases What have we firmly established? Surgery + Radiation Is better than Radiation alone Health Related Quality of Life is improved with surgery 16 Decision Making in Spine Metastases What have we firmly established? Surgery + Radiation Is better than Radiation alone Health Related Quality of Life is improved with surgery Less than $50 per day to maintain ambulation 17 Decision Making Patients feel more empowered when allowed to participate in decisions about treatment options. In other words patients want to have a say in their treatment plans. Kirsti A. Dyer : Defining Good Death 19 6





7 Decision Making Patients feel more empowered when allowed to participate in decisions about treatment options. In other words patients want to have a say in their treatment plans. Kirsti A. Dyer : Defining Good Death Approach to Spine Mets 3 factors Neurology 20 Neurology Timing <1 day OR OR
8 Pitfall - speed and adequacy Delays Awareness Capacity/infrastructure Circumferential compression 360 decompression 23 Metastatic spinal cord compression (MSCC): Radiotherapy alone 24 MSCC: Laminectomy ± Radiotherapy 25 8
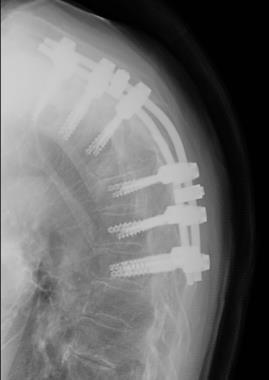
9 MSCC: Laminectomy/Decompression & Stabilisation 26 MSCC: Vertebral body resection and stabilisation 27 MSCC: Summary of treatment outcomes 28 9



10 29 30 Posterolateral Vertebrectomy 31 10

:2240-9 Wang et al.")
11 Posterolateral Vertebrectomy Reliable & safe exposure for 3 column reconstruction and neurologic decompression Acceptable complication rate Favourable patient outcome Bilsky, M.H. Et al. Spine sep 1;25(17): Wang et al. J of neurosurgery 2004 Street, fisher et al J of spinal disorders



12 35 Decision Making Patients feel more empowered when allowed to participate in decisions about treatment options. In other words patients want to have a say in their treatment plans. Kirsti A. Dyer : Defining Good Death Approach to Spine Mets 3 factors Neurology Patient 36 Decision Making Patients feel more empowered when allowed to participate in decisions about treatment options. In other words patients want to have a say in their treatment plans. Kirsti A. Dyer : Defining Good Death Approach to Spine Mets 3 factors Neurology Patient 37 12


13 Decision Making in Spine Metastases That biology is dictating decision making. PATIENT PROFILE The underestimation of life expectancy and subsequent inadequate treatment of spinal metastases may lead to dramatic alteration of the quality of life. 38 Many pre-operative scoring systems try and tell you if and how to operate, but none are particularly valid or reliable, especially in light of all the new developments in oncology. That biology is dictating decision making The only consistent factors for prognosis or life expectancy are GENERAL CONDITION and PRIMARY SITE! The importance of molecular markers! Over 4 year period found Lung and Renal Cell CA Patients living significantly longer! Influence of histopathologic parameters in the management of metastatic disease of the spine secondary to lung cancer a systematic review. Batista, N. Fisher C. et al. GS 2015 Survival of Lung Ca Patients Systemic Control Small Cell = 8 mos NSCLC - Adenocarcinoma = 11 mo - EGFR = 17.8mos - Large cell = 11 mo - Squamous = 9 mo - NOS = 5 mo Not otherwise specified (NOS) Not all spine met patients secondary to Lung Ca are bad surgical candidates. Similar variations for Renal Cell, Breast, GI. Molecular analysis is changing prognosis dramatically. Talk to named oncologist! 13
14 Breast Cancer Genome 43 Why curing cancers with drugs is difficult!! 1. Cancer genome is almost identical to normal genome (compare to bacteria) 2. Variation among cancers 44 Breast Cancer Genome Sample 45 14
15 Breast Cancer Genome Sample - 34C vs. 10C Genomes 46 Personalized Medicine aka Precision Medicine aka Genome-based Medicine 47 Pancreatic Cancer Pa34C Genome BRAF mutation 48 15

16 49 Implications of the cancer genome for non-conventional therapeutic approaches 50 Considerations for Surgery Histology Neurological condition/pain/symptoms Performance status Instability Patient s wishes Systemic Disease Status Prognosis



17 We are now able to impact survival in patients with advanced metastatic disease that have failed prior therapies Lung Cancer Spine SBRT An Alternative to CRT: Local Control 54 17
18 Radiosensitivity U = unfavourable I = intermediated F = Favorable CRT No instability Sensitive Histology Multilevel Disease Lymphoma Breast Prostate Sarcoma Melanoma GI NSCLC Renal Seminoma Myeloma F U U U U U U U F F F U U U U U F I I I U I U I F F F U U U U U F F F U U U U U F F F U U U U U F I I I U I U I 55 Radiosensitivity U = unfavourable I = intermediated F = Favorable CRT No instability Sensitive Histology Multilevel Disease SBRT Degree of Epidural Disease No instability Resistant Histology Progression after CRT Lymphoma Breast Prostate Sarcoma Melanoma GI NSCLC Renal Seminoma Myeloma F U U U U U U U F F F U U U U U F I I I U I U I F F F U U U U U F F F U U U U U F F F U U U U U F I I I U I U I 56 Radiosensitivity U = unfavourable I = intermediated F = Favorable CRT No instability Sensitive Histology Multilevel Disease SBRT Degree of Epidural Disease No instability Resistant Histology Progression after CRT Lymphoma Breast Prostate Sarcoma Melanoma GI NSCLC Renal Seminoma Myeloma F U U U U U U U F F F U U U U U F I I I U I U I F F F U U U U U F F F U U U U U F F F U U U U U F I I I U I U I 57 18




19 Bilsky Epidural Disease Grade 1a 1b 1c 2 3 Kumar,..Fisher, Sahgal, Neuro-Onc Pract Predictors of VCF Pitfall 60 19






20

 50% improvement")

21 64 65 Embolization Neurologic complications (4% + 2.5%) 50% improvement in blood loss Better outcomes with particle +/- coil 66 21
 50% improvement in blood loss Better outcomes with particle +/- coil 67 68")


22 Embolization Neurologic complications (4% + 2.5%) 50% improvement in blood loss Better outcomes with particle +/- coil Radiosensitivity U = unfavourable I = intermediated F = Favorable CRT No instability Sensitive Histology Multilevel Disease SBRT Degree of Epidural Disease No instability Resistant Histology Progression after CRT Lymphoma Breast Prostate Sarcoma Melanoma GI NSCLC Renal Seminoma Myeloma F U U U U U U U F F F U U U U U F I I I U I U I F F F U U U U U F F F U U U U U F F F U U U U U F I I I U I U I 69 22

23


24






25 76 What is en bloc? It is NOT complete macroscopic resection of lesion It is NOT total spondylectomy Resection of lesion without transgression of tumour Enbloc: marginal 78 25
26 Why consider en bloc? Solitary lesion RT insensitive Hormone secreting lesion Solitary lesion failing to respond to other therapies Why consider en bloc? Solitary lesion RT insensitive Hormone secreting lesion Solitary lesion failing to respond to other therapies Low morbidity en bloc Thoracic Posterior element Evidence.. MSCC intervention generally well supported


27 Evidence.. MSCC intervention generally well supported Evidence for en bloc..?? Evidence.. MSCC intervention generally well supported Evidence for en bloc..?? = Majority would choose this most of the time 83 Systematic Review - Search Last 10yr PubMed, Google Scholar, OVID and the Cochrane and a review of the references of the reviewed articles. Spine, metastasis and en bloc connected with the Boolean operator AND
28 Systematic Review - Inclusion articles published 1 Jan Jan 2018 articles in English/English translation adults (aged 18+) articles describing en bloc resection for isolated spinal metastasis Systematic Review - Exclusion patient recruitment prior to 2000 local tumour invasion rather than metastasis paediatric subjects articles with <5 reported en bloc resections articles not published in English Systematic Review - Results 66% for pain vs 34% for neurological compromise Tokuhashi score was 9.8 (SD 1.9) = 6-12/ % posterior only vs 9.3% anterior approach TBL mean 1596ml (SD 784ml) Operating time 6.5hrs (SD 0.8hrs) LOS (Lee) 84.2 days (SD 59 days)
 Peri-operative (30 day) death 3.")

29 Complications 35.1% Dural tear 18.5% Infection 5.3% Unplanned neurological injury 3.7% Local recurrence 8.5% Metastatic progression 54.5% at 9.7 months Death 55.7% at FU (12.1 months SD 10.7) Peri-operative (30 day) death 3.84% Complications 35.1% Dural tear 18.5% Infection 5.3% Unplanned neurological injury 3.7% Local recurrence 8.5% Metastatic progression 54.5% at 9.7 months Death 55.7% at FU (12.1 months SD 10.7) Peri-operative (30 day) death 3.84%


30



31 En Bloc? Risks remain high vs conventional surgery Therefore consider: Referral to high volume oncology centre Only highly selective use of en bloc surgery Some Renal Some Thyroid Secreting tumours Post RT Selected low risk en bloc J Bone Joint Surg Am Jan 20;98(2): doi: /JBJS.N Quality of Life and Surgical Outcomes After Soft-Tissue Reconstruction of Complex Oncologic Defects of the Spine and Sacrum Dolan RT, Butler JS, Wilson-MacDonald J, Reynolds J, Cogswell L, Critchley P, Giele H 96 31




32 97 Minimally Invasive T11 Vertebrectomy 98 Intra-operative Imaging 99 32





33 Decision Making Patients feel more empowered when allowed to participate in decisions about treatment options. In other words patients want to have a say in their treatment plans. Kirsti A. Dyer : Defining Good Death Approach to Spine Mets 3 factors Neurology Patient Stability 100 What is stable? 101 Stability = system handling of perturbation Unstable = the disturbed behavior differs significantly from the old behavior Effect of neoplastic replacement? 102 The neoplastic spine may be stable but not usually robust 33
34 Spinal Instability Neoplastic Score (SINS) Stable Potentially unstable Unstable 0-6 pts 7-12 pts >12 pts 103 Spinal Instability Neoplastic Score (SINS) Stable Potentially unstable Unstable 0-6 pts 7-12 pts >12 pts 104 Decision Making




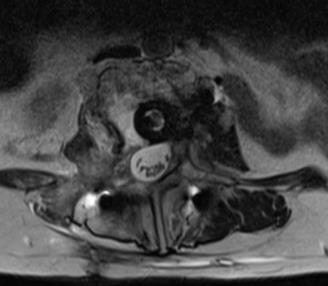
35 57yo male Progressive neuro deterioration 5 wks Male L1 ASIA C Mechanical TL pain Lymphoma pts Stable Potentially unstable Unstable 0-6 pts 7-12 pts pts yo male Progressive neuro deterioration 5 wks Male L1 ASIA C Mechanical TL pain Lymphoma

 Is VA effective")


36 55 yo female Severe LBP with mobility No neurology Lung Ca pts Stable Potentially unstable Unstable 0-6 pts 7-12 pts >12pts 110 Vertebral Augmentation (VA) Is VA effective for pain relief and improving function? Is VA safe? VA is effective and safe and should be used in the management of metastatic disease of the spine. Strong Recommendation 111 Moderate Evidence 36




37 Known primary vs CUP Staging CT Whole spine MRI Biopsy ASAP Steroids

38

39 Summary New Paradigm for Evidence Based Care Decision: Multidisciplinary Patient Factors Neurology Stability CRT SRS or IMRT Surgery Vertebral Augmentation Standardized Outcomes and Multicenter Research Palliative Care 118 Cost Effective? Expensive treatment for incurable disease?? Baseline results = $60 per additional day of ambulation 119 When survival used as measure of effect, translates to $ per life year gained Compares favorably to: vaccination programs Implantable cardioverters Screening for colorectal cancer Abdominal aortic aneurysm surgery 39
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic disease of the Spine
 Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital MSCC Metastatic Spinal
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Surgical Treatment of Spine Surgery Experience Primary Spinal Neoplasms ( ) Ziya L. Gokaslan, MD, FACS Approximately 3500 spine tumor
 Ziya L. Gokaslan, MD, FACS Approximately 3500 spine tumor") Surgical Treatment of Primary Spinal Neoplasms Ziya L. Gokaslan, MD, FACS Donlin M. Long Professor Professor of Neurosurgery, Oncology & Orthopaedic Surgery Vice Chairman Director of Spine Program Department
Surgical Treatment of Primary Spinal Neoplasms Ziya L. Gokaslan, MD, FACS Donlin M. Long Professor Professor of Neurosurgery, Oncology & Orthopaedic Surgery Vice Chairman Director of Spine Program Department
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
How a fully integrated Acute Oncology Service can benefit the busy medical unit
 How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Spinal cord compression: what it means and how it can be treated
 Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
Spinal cord compression: what it means and how it can be treated Patient Information Oncology Department Author ID: Acute Oncology Nurse Specialist Leaflet Number: CC 036 Version: 2.1 Name of Leaflet:
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO)
") North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors
 Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Suspected spinal cord compression form
 Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Suspected spinal cord compression form Enter this form into the notes at the appropriate date in the Progress / Evaluation sheets. Please copy this form to Lisa Lewis, Medical PA (ext 4551), for audit
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Modern management in vertebral metastasis
 43 B. Costachescu, C.E. Popescu Modern management in vertebral metastasis Modern management in vertebral metastasis B. Costachescu, C.E. Popescu Department of Neurosurgery, Division of Spine Surgery, University
43 B. Costachescu, C.E. Popescu Modern management in vertebral metastasis Modern management in vertebral metastasis B. Costachescu, C.E. Popescu Department of Neurosurgery, Division of Spine Surgery, University
Dr Patrick Schweder. Neurosurgeon Department of Neurosurgery Auckland Hospital Auckland
 Dr Patrick Schweder Neurosurgeon Department of Neurosurgery Auckland Hospital Auckland 8:30-9:25 WS #98: Management of Common Neurosurgical Problems in General Practice 9:35-10:30 WS #110: Management of
Dr Patrick Schweder Neurosurgeon Department of Neurosurgery Auckland Hospital Auckland 8:30-9:25 WS #98: Management of Common Neurosurgical Problems in General Practice 9:35-10:30 WS #110: Management of
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
agreed MSCC pathways and guidelines).
.") Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Managing Bone Pain in Metastatic Disease. Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018
 Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Palliative Care Emergencies
 Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Palliative Care Emergencies LAURA BARNFIELD What might constitute an emergency in Palliative Care? 1 Palliative Care Emergencies Major haemorrhage Metastatic Spinal Cord Compression (MSCC) Superior Vena
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
Red Flags for serious spinal pathology: A collaborative approach
 Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
Red Flags for serious spinal pathology: A collaborative approach Professor James Selfe DSc, PhD, MA, GD Phys (Distinction), FCSP Serious Spinal Pathology Background Collaboration Communication Solutions
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM BRAIN METASTASES CNS Site Group Brain Metastases Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRIMARY STUDIES EN BLOC VERSUS DEBULKING
 PRIMARY STUDIES EN BLOC VERSUS DEBULKING I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary outcome VI Results secondary and other outcome(s) VII Critical appraisal of
PRIMARY STUDIES EN BLOC VERSUS DEBULKING I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary outcome VI Results secondary and other outcome(s) VII Critical appraisal of
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Spinal cord compression
 Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Spinal cord compression Urology Department Patient Information Leaflet Introduction If you have been diagnosed with cancer, you need to know about spinal cord compression and the warning signs. This leaflet
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine
 Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked Response to Molecular Target Drugs
 Case Reports in Orthopedics Volume 2013, Article ID 916501, 4 pages http://dx.doi.org/10.1155/2013/916501 Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked
Case Reports in Orthopedics Volume 2013, Article ID 916501, 4 pages http://dx.doi.org/10.1155/2013/916501 Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked
Humber NHS Foundation Trust. Joint Effort
 Joint Joint is a new community based musculoskeletal service that treats patients with complex problems of the spine, upper and lower limb. Joint s experienced Consultant Orthopaedic Surgeons and Extended
Joint Joint is a new community based musculoskeletal service that treats patients with complex problems of the spine, upper and lower limb. Joint s experienced Consultant Orthopaedic Surgeons and Extended
Conflict of interest disclosure
 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Department of Orthopedic Surgery, Henan Province People s Hospital, Henan, People s Republic of China; 2
 Int J Clin Exp Med 2018;11(3):2465-2470 www.ijcem.com /ISSN:1940-5901/IJCEM0060812 Original Article Validation of a scoring system predicting survival and function outcome in patients with metastatic epidural
Int J Clin Exp Med 2018;11(3):2465-2470 www.ijcem.com /ISSN:1940-5901/IJCEM0060812 Original Article Validation of a scoring system predicting survival and function outcome in patients with metastatic epidural
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT
 Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
COSD & Source of Referral
 COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
COSD & Source of Referral A Brief guide October 2014 Michael Sharpe Data Improvement Manager National Cancer Registration Service What is COSD? Cancer and Outcomes Services Dataset Clinical dataset for
Posterior Thoracic Corpectomies with Cage Reconstruction for Metastatic Spinal Tumors: Comparing the MiniOpen Approach to the Open Approach
 Posterior Thoracic Corpectomies with Cage Reconstruction for Metastatic Spinal Tumors: Comparing the MiniOpen Approach to the Open Approach Darryl Lau, MD and Dean Chou, MD Department of Neurological Surgery
Posterior Thoracic Corpectomies with Cage Reconstruction for Metastatic Spinal Tumors: Comparing the MiniOpen Approach to the Open Approach Darryl Lau, MD and Dean Chou, MD Department of Neurological Surgery
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Imaging of bone metastases
 Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Tumours of the spinal cord Faculty of Clinical Radiology www.rcr.ac.uk Contents Primary spinal cord tumours
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Tumours of the spinal cord Faculty of Clinical Radiology www.rcr.ac.uk Contents Primary spinal cord tumours
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Workshop. Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto
 Workshop Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Workshop Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DOCTOR DISCUSSION GUIDE
 DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
En bloc spondylectomy for spinal metastases: a review of techniques
 Neurosurg Focus 15 (5):Article 6, 2003, Click here to return to Table of Contents En bloc spondylectomy for spinal metastases: a review of techniques KEVIN C. YAO, M.D., STEFANO BORIANI, M.D., ZIYA L.
Neurosurg Focus 15 (5):Article 6, 2003, Click here to return to Table of Contents En bloc spondylectomy for spinal metastases: a review of techniques KEVIN C. YAO, M.D., STEFANO BORIANI, M.D., ZIYA L.
Kim, Hyoungmin 1 ; Lee, Choon-Ki 1 ; Yeom, Jin S. 1 ; Lee, Jae Hyup 1 ; Lee, Suk- Joong 2 ; Chang, Bong-Soon 1
 The Predictive Value of the Spinal Instability Neoplastic Score (SINS) System for Adverse Events of Pathologic Fracture and Spinal Cord Compression in Patients with Single Spinal Metas tasis. Kim, Hyoungmin
The Predictive Value of the Spinal Instability Neoplastic Score (SINS) System for Adverse Events of Pathologic Fracture and Spinal Cord Compression in Patients with Single Spinal Metas tasis. Kim, Hyoungmin
Unknown Primary Service for patients at Chesterfield Royal Hospital
 Unknown Primary Service for patients at Chesterfield Royal Hospital David Brooks Macmillan Consultant in Palliative Medicine Louise Merriman GP Cancer Lead With thanks to Macmillan Cancer Support, who
Unknown Primary Service for patients at Chesterfield Royal Hospital David Brooks Macmillan Consultant in Palliative Medicine Louise Merriman GP Cancer Lead With thanks to Macmillan Cancer Support, who
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Radiation Treatment for Breast. Cancer. Melissa James Radiation Oncologist August 2015
 Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP. REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014
 SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
SOUTH THAMES CHILDREN S CANCER NETWORK GROUP REFERRAL PROTOCOLS AND DIAGNOSIS AND STAGING PROTOCOLS October 2014 Contents 1. Leukaemia Referral, Diagnostic and Staging Guidelines 2. Lymphoma Referral,
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Innovative RT SBRT. The variables with REQ in superscript are required.
 The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
The variables with REQ in superscript are required. The variables with a are single-select variables; only one answer can be selected. The variables with a are multi-select variables; multiple answers
Posterior Lumbar Spinal Fusion
 Posterior Lumbar Spinal Fusion Information to help patients prepare for a Posterior Lumbar Spinal Fusion Operation Directorates of Orthopaedic and Rheumatology, and Neurosciences Produced: February 2007
Posterior Lumbar Spinal Fusion Information to help patients prepare for a Posterior Lumbar Spinal Fusion Operation Directorates of Orthopaedic and Rheumatology, and Neurosciences Produced: February 2007
PLASTICS Referral Guidelines
 PLASTICS Referral Guidelines Austin Health PLASTICS Unit holds fortnightly multidisciplinary meetings with ENT/ Maxillary Facial and Oncology Units to discuss and plan the treatment of patients with cancerous
PLASTICS Referral Guidelines Austin Health PLASTICS Unit holds fortnightly multidisciplinary meetings with ENT/ Maxillary Facial and Oncology Units to discuss and plan the treatment of patients with cancerous
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive. Lloyd A. Mack September 19, 2015
 Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor
 Volume 2013, Article ID 254684, 6 pages http://dx.doi.org/10.1155/2013/254684 Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor Isao Shibuya, Koichi Sairyo,
Volume 2013, Article ID 254684, 6 pages http://dx.doi.org/10.1155/2013/254684 Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor Isao Shibuya, Koichi Sairyo,
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
BRIEFING PAPER THE USE OF RED FLAGS TO IDENTIFY SERIOUS SPINAL PATHOLOGY THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Jackie Turnpenney Version: Accountable Committee:
Cervical laminectomy for spinal cord compression. Information for patients Neurosurgery
 Cervical laminectomy for spinal cord compression Information for patients Neurosurgery What is a compression of the spinal cord and how has it been caused? The bones in our back are called vertebras and
Cervical laminectomy for spinal cord compression Information for patients Neurosurgery What is a compression of the spinal cord and how has it been caused? The bones in our back are called vertebras and
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre
 Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Dr Hilary Williams. Consultant in Medical Oncology at Velindre Cancer Centre Hilary.williams4@wales.nhs.uk Thinking about Acute Oncology. Why do we need acute oncology locally? What the Hub VCC provides
Metastatic spinal cord compression (MSCC) is one
 is one") SPINE Volume 41, Number 18, pp 1469 1476 ß 2016 Wolters Kluwer Health, Inc. All rights reserved SURGERY Who are the Best Candidates for Decompressive Surgery and Spine Stabilization in Patients With Metastatic
SPINE Volume 41, Number 18, pp 1469 1476 ß 2016 Wolters Kluwer Health, Inc. All rights reserved SURGERY Who are the Best Candidates for Decompressive Surgery and Spine Stabilization in Patients With Metastatic
Review Course «Musculoskeletal Oncology» October 6, 2011 UNIKLINIK BALGRIST
 «Musculoskeletal Oncology» PD Dr Elyazid MOUHSINE 06/10/11 K, 75 yo Hip pain => Standard Xrays & ct scan Kystic lesion & fracture Diagnosis? Fractured metastasis, breast cancer?! But, why not a chondrosarcoma?
«Musculoskeletal Oncology» PD Dr Elyazid MOUHSINE 06/10/11 K, 75 yo Hip pain => Standard Xrays & ct scan Kystic lesion & fracture Diagnosis? Fractured metastasis, breast cancer?! But, why not a chondrosarcoma?
Management of single brain metastasis: a practice guideline
 PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
PRACTICE GUIDELINE SERIES Management of single brain metastasis: a practice guideline A. Mintz MD,* J. Perry MD, K. Spithoff BHSc, A. Chambers MA, and N. Laperriere MD on behalf of the Neuro-oncology Disease
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory