MRI: IMPACT ON RECTAL CANCER CARE AND STANDARDISATION
|
|
|
- Amy Harrison
- 5 years ago
- Views:
Transcription
1 MRI: IMPACT ON RECTAL CANCER CARE AND STANDARDISATION Professor Gina Brown Consultant Radiologist and Professor of Gastrointestinal Cancer Imaging, The Royal Marsden Hospital and Imperial College, London, UK
2 WHICH PATIENTS ARE AT RISK OF LOCAL RECURRENCE? The following risk factors have been identified as predictors for pelvic recurrence if TME plane surgery is performed: Tumour extending to 1 mm or less of mesorectal fascia Tumours bordering 1 mm or less to the intersphincteric plane Anterior tumours <4 cm from anal verge as measured by MRI Anterior quadrant invasion below 6 cm to the anal verge Extramural venous invasion Battersby NJ, et al. Ann Surg 2016;263:
3 WHICH PATIENTS ARE AT RISK OF LOCAL RECURRENCE AFTER CHEMORADIOTHERAPY? The following risk factors have been identified as predictors for pelvic recurrence if TME plane surgery is performed: Persistent tumour extending to 1 mm or less of mesorectal fascia Persistent tumours bordering 1 mm or less to the intersphincteric plane Persistent extramural venous invasion Battersby NJ, et al. Ann Surg 2016;263:751 60; Taylor FG, et al. J Clin Oncol 2014;32:34 43; Chand M, et al. Ann Surg 2015;261:473 9.
.")
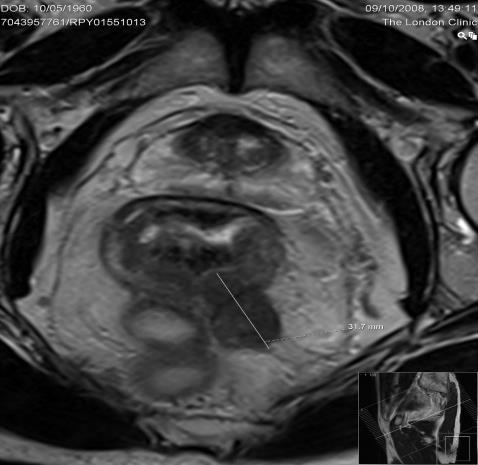
4 POST TREATMENT ASSESSMENT OF THE CRM BY MRI A. High resolution scan at baseline The baseline scans show an annular ulcerating tumour which extends to the mesorectal fascia anteriorly to the right of the midline (white arrow). There is also vascular invasion (open arrow) and a discontinuous deposit is seen in a branch of the superior rectal vein (black arrow): MRI stage is mrt3c,n1c, mremvi positive, mrcrm involved B. Post chemoradiotherapy scan The tumour is seen as dense low signal intensity signifying fibrosis rather than residual tumour at the mesorectal margin: ymrt0, N0, EMVI negative, mrcrm clear C. The pathology confirms a complete response A potentially involved CRM has been prevented by preoperative downstaging chemoradiotherapy Courtesy of The Royal Marsden Hospital
 TME plane safe 2.")
5 MR CRM PREDICTION FOR LOW RECTAL CANCERS: TME PLANE SAFETY This is a classification that does not relate to TNM but rather predicts the safety of TME plane surgery 1. MRI Low Rectal Stage 1: tumour on MRI images appears confined to bowel wall (intact muscularis propria of the internal sphincter) TME plane safe 2. MRI Low Rectal Stage 2: tumour on MRI replaces the muscle coat but does not extend into the intersphincteric plane (>1 mm muscularis is preserved). Above sphincter tumour is confined to within the mesorectum TME plane safe 3. MRI Low Rectal Stage 3: invading into the intersphincteric plane or lying within 1 mm of levator muscle above the level of the sphincter complex (verified by imaging in more than one plane) ELAPE plane is necessary 4. MRI Low Rectal Stage 4: invading the external anal sphincter and infiltrating/ extending beyond the levators +/- invading adjacent organ ELAPE or exenteration needed Shihab OC, et al. Eur Radiol 2009;19:
6 PRIMARY SURGERY FOR LOW RECTAL CANCERS Almost half (44 4%, 124/279) of study participants had a safe mrlrp and no adverse MRI features. The recommended management was to proceed straight to surgery with an intersphincteric resection, adhering to this guidance (50%) led to a clear 16 pcrm in 98% of cases When MRI low-risk patients were offered CRT or an ELAPE -this resulted in a higher pcrm involvement. Additional treatment and more radical surgery did not result in a benefit to the patient and may represent overtreatment Battersby NJ, et al. Ann Surg 2016;263:

7 MRI TOOL FOR PREDICTING RISK OF PCRM INVOLVEMENT No risk factors 2% pcrm risk MRI height <4 cm 4% 12% 9% 5% mr Unsafe plane 15% % % MRI invading edge anterior 4% mremvi 5% In patients with low rectal cancer the assessment of the safety of the intersphincteric plane and mesorectal margin are more relevant than T stage in predicting the risk of pathologic CRM involvement and consequent local recurrence risk. Battersby NJ, et al. Ann Surg 2016;263:
8 ASSESSING OTHER RISK FACTORS FOR RECURRENCE
9 HOW DOES TUMOUR SPREAD? Directly into neighbouring structures risk can be reduced by extending the TME plane to beyond TME surgery to achieve clear radial margins (1) Via the lymph nodes: removal of the total draining nodal disease by TME surgery results in low risk of distant failure if a clear CRM is achieved (2) Via the blood vessels EMVI persistence of extramural vascular invasion after preoperative therapy as detected by MRI is a risk factor for both CRM positivity and distant metastatic disease (3) 1. Bhangu AA, et al. Br J Surg 2013;100:E1 E Taylor FG, et al. Ann Surg 2011;253: Chand M, et al. Ann Surg 2015;261:473 9.
10 Relapse-free (%) PROGNOSTIC SIGNIFICANCE OF MAGNETIC RESONANCE IMAGING-DETECTED EXTRAMURAL VASCULAR INVASION IN RECTAL CANCER MRI-EMVI score= 0-2 MRI-EMVI score= p = Time since operation (years) Redrawn from Smith NJ, et al. Br J Surg 2008;95:

11 DISCONTINUOUS VASCULAR SPREAD SEEN USING MREMVI Vascular invasion is manifest on MRI as either direct spread from the primary tumour into an adjacent extramural vessel or as discontinuous seeding along the draining veins within the mesorectum as in the cases illustrated above. There is a stronger link with tumour vascular deposits and subsequent metastatic disease than that observed related to nodal spread. Vascular invasion is detected in 30-40% of preoperative MRI scans Chand M, et al. The prognostic significance of postchemoradiotherapy high-resolution MRI and histopathology detected extramural venous invasion in rectal cancer, Ann Surg 2015;261: Published with permission from Wolters Kluwer Health

12 MRI DETECTED MORE PERSISTENT EMVI POST CRT THAN PATHOLOGY Chand M, et al. Ann Surg 2015;261:
13 UNIVARIATE AND MULTIVARIATE ANALYSIS By clinical, preoperative MRI and postoperative histopathology characteristics (Cox Proportional Hazards for DFS) Variables Patient characteristics Baseline MR staging Post-CRT preoperative MR staging Final pathology staging Sex Height mrt stage mrn stage mremvi mrcrm ymrt stage ymrn stage ymremvi ymrcrm ypt ypn ypemvi ypcrm Group Female Male Upper/mid Low Good Poor Negative Positive Negative Positive Negative Positive Good Poor Negative Positive Negative Positive Clear Involved/threatened Good Poor Negative Positive Negative Positive Negative Positive Patient numbers Univariate analysis Multivariate analysis HR 95% CI P HR 95% CI P < < Comparing ymremvi and ypemvi reveals a striking difference in detection rates. Only 36.4% of ymremvi positive cases were detected on histopathology using standard methods, yet the prognostic outcomes for mremvi-positive tumours that were pathologically ypemvi negative were poor. Therefore, rather than MRI overdiagnosing EMVI at the end of treatment, these cases are hard to detect by conventional pathology. Redrawn from Chand M, et al. Ann Surg 2015;261:
14 Cumulative survival Cumulative survival Recurrences ymremvi 23/ % ymremvi+ 40/ % Recurrences ymremvi 34/ % ymremvi+ 20/ % ymremvi negative DFS 79.2% (95% CI %) ypemvi negative DFS 65.9% (95% CI %) ymremvi positive DFS 42.7% (95% CI %) ypemvi positive DFS 36.9% (95% CI %) Months Months Comparison of survival outcome of 3-year DFS between ymremvi negative and ymremvi positive patients Comparison of 3-year DFS between ypemvi negative and ypemvi positive patients Redrawn from Chand M, et al. Ann Surg 2015;261:

15 POST CRT EFFECT ON EMVI 3-YEAR DFS mrvein invasion neg mrvein converted pos to neg mrvein remains pos after Rx Chand M, et al. Ann Surg 2015;261:

16 When patients stratified patients into high- and low-risk groups on the basis of known MRI prognostic features: mremvi positive, >5 mm extramural invasion, or involved CRM. High risk group have a higher rate of synchronous metastatic disease than non-high risk confirmed % in the high-risk group vs. 4.2% Same mets PET/CT and CT 2/94 (2.1%) 94 low risk Whole group: 136 high risk 33/230 (14.3%) distant mets on PET/CT 5/94 (5.3%) distant mets on PET/CT CT mets & more mets on PET/CT 2/94 (2.1%) Mets only on PET/CT 1/94 (1.1%) Any mets on PET/CT not CT 3/94 (3.2%) 236 patients enrolled 230 patients with all imaging available Odds Ratio 4.6 (95% CI ) P=0.001 Odds ratio 4.6 (95% CI ) P=0.01 Same mets PET/CT and CT 10/136 (7.4%) 6 patients (2.5%) imaging unavailable for review 28/136 (20.6%) distant mets on PET/CT CT Mets & more mets on PET/CT 8/136 (5.9%) Mets only on PET/CT 10/136 (7.4%) Any mets on PET/CT not CT 18/136 (13.2%) Hunter CJ, et al. Ann Surg Oncol 2012;19:
17 WHAT SHOULD WE CONSIDER AS A GOOD RESPONSE? PCR? Infrequent finding for clinically staged T3 tumours Metaanalysis had shown that pcr was more likely achieved in clinical T1 and T2 tumours -? Was there a survival advantage to achieving pcr for T1 and T2 tumours? Influence of timing of surgery on pcr Is pcr realistic goal for treatment of advanced rectal cancer? Maas M, et al. Lancet Oncol 2010;11: Reprinted from Lancet Oncology, Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data Copyright 2010, with permission from Elsevier.

18 TIMING AFTER CRT? WHEN IS MAXIMUM RESPONSE REACHED? Baseline mrt4 invading Bladder and peritoneum 6 weeks ymrt3b 12 weeks ymrt2 Final Pathology: ypt2n0 Patients undergoing surgery with a delay of at least 8 weeks after completion of radiotherapy are 3 times more likely to undergo T downstaging (OR, 3.79; CI: ; P<0.03) than patients undergoing surgery at less than 8 weeks. A greater delay to surgery following the completion of pre-operative therapy is associated with an increased likelihood of achieving a pathological complete response. This is being prospectively tested in a randomised trial evaluating the timing of response assessment and surgery (the 6 vs. 12 trial) Evans J, et al. Timing of surgery following preoperative therapy in rectal cancer: the need for a prospective randomized trial? Dis Colon Rectum 2011;54: Published with permission from Wolters Kluwer Health

19 Yu SK, et al. Int J Radiat Oncol Biol Phys 2013;87:
20 RMH EXPERIENCE : SELECTIVE PREOPERATIVE CRT Analysis Good response defined as ypt0-ypt2 218 patients treated between % of patients had been enrolled into EXPERT trial 12 weeks of capecitabine and oxaliplatin neoadjuvant chemotherapy prior to CRT 118/218 showed good response 40% Criteria for preoperative CRT Tumours within 1 mm of mesorectal fascia (i.e., potential circumferential resection margin involvement) T3c (extramural spread 5-15 mm) and T3d (extramural spread >15 mm), regardless of N stage MRI T4a or T4b disease regardless of N stage Low rectal cancer with tumour bordering the intersphincteric/ distal TME plane on MRI Tumours with MRI extramural venous invasion (mremvi) Yu SK, et al. Int J Radiat Oncol Biol Phys 2013;87:
21 ypt0-2 79% ypt3-4 63% Reprinted from Int J Radiat Oncol Biol Phys, 87/3, Yu SK, Tait D, Chau I, Brown G. MRI predictive factors for tumor response in rectal cancer following neoadjuvant chemoradiation therapy - implications for induction chemotherapy?, Pages Copyright 2013, with permission from Elsevier
 PPV for node negative status")
22 POST TREATMENT YMRTN STAGE VS. PATHOLOGY TN STAGE Overall accuracy for response assessment was 72% PPV for mrt0-2 for good response on pathology was 80% (95% CI 68%-88%) PPV for node negative status on MRI was 84% (95% CI 78%-89%) Overall accuracy for path nodal assessment was 75% Yu SK, et al. Int J Radiat Oncol Biol Phys 2013;87:
23 DISEASE FREE SURVIVAL GOOD VS. POOR RESPONDERS: PATHOLOGY AND MRI ypt0-2 79% ymrt0-t2 80% ypt3-4 63% ymrt3-t4 67% Despite a lack of 100% agreement between pathology and MRI, assessment of T stage by either MRI or pathology show equal performance in the prediction of survival Yu SK, et al. Int J Radiat Oncol Biol Phys 2013;87:
24 FACTORS ASSOCIATED WITH YPT0-T2 Baseline age, sex, stage size of tumour were not independent predictors for tumour response mremvi positive tumours were significantly less likely to downstage than mremvi negative tumours with CRT (OR for EMVI 2.94, P<0.007) Height <5 cm from anal verge significantly more likely to respond (OR for <5 cm vs. >5 cm 1.96, P<0.02) mremvi status from positive to negative more likely in pathology responders (OR 3.09) strong association between induction chemotherapy and ymremvi status positive to negative change after CRT (OR 9.0, P<0.003) Yu SK, et al. Int J Radiat Oncol Biol Phys 2013;87:


25 MR TRG Assessment of tumour response using the mrtrg scale Base line scans shows an annular tumour infiltrating the mesorectal margin between the 10 and 12 o'clock position. Post treatment, the intermediate (grey) signal of tumour has been replaced by fibrotic (black) signal with fibrosis involving the rectal wall and normal fat signal at the mesorectal margins. As no intermediate signal intensity remains within the dark fibrosis this is classified as dense fibrosis only mrtrg2 with either no tumour cells or microscopic residual tumour cells of questionable long term viability Patel UB, et al. Am J Roentgenology 2012;199:W486 W95.
26 TRG AND SURVIVAL In independently validated series, mrtrg identifies prognostically distinct groups. mrtrg can distinguish between good and poor responders to CRT. This shows good interobserver agreement amongst radiologists who can undertake this scoring on high resolution T2 weighted scans Patients with mrtrg 4 & 5 have relatively little response to preoperative therapy. As expected this group has a significantly higher risk of CRM involvement, distant failure and poor OS compared with patients that have mrtrg 1-3. On the other hand, mrtrg1&2 is strongly associated with complete response p=0.001 HR 3.28 (95%CI; ) MRI TRG 4-5 Patel UB, et al. J Clin Oncol. 2011;29:
27 MRTRG IS A PROGNOSTIC (AND PREDICTIVE) BIOMARKER Shows good interobserver radiology agreement and reproducibility MERCURY trial (JCO 2011 multiple radiologists) (1) EXPERT-C trial (2) GEMCAD study (17 radiologists) (3) CORE study (interobserver agreement) (4) Identified 40% of patients with mrtrg1/2 89.8% overall survival Compared with only 8.8% patients with pathologic CR Therefore mrtrg could be justified as a more clinically relevant endpoint
28 SELECTING PATIENTS FOR DEFERRAL OF SURGERY
29 RESPONSE METHODS COMPARED Method MRI DWI DCE-MRI PET-CT mrvolume assessment mrtrg mrt and mrn stage Prospectively validated against DFS outcomes No many retrospective quantitative cut-offs and qualitative assessments none prospectively validated No many retrospective values proposed none validated No but retrospective SUV cut-offs proposed unverified prospectively Yes: >80% volume reduction Yes: TRG1-5 validated prospectively and against outcomes Validated prospectively and against outcomes

30 HOW ARE THE PATIENTS IDENTIFIED? mrtrg PET Clinically - DRE +/- biopsy



31 Courtesy of The Royal Marsden Hospital
32 ENROLMENT 4-6 weeks post CRT no viable disease (low signal intensity fibrotic scar tissue only) confirmed by 8-12 weeks 4-6 weeks post CRT a good partial response Continued incremental response on 8-12 weeks NOT INITIALLY EXCLUDED EVEN IF: DRE Thickening of rectal wall or clinically palpable tumour Endoscopically Mucosal abnormality Pathology Biopsy positive Clinical trial : Avoiding Surgery in Rectal Cancer After Pre-Operative Therapy, ClinicalTrials.gov Identifier: NCT


33 TRG 2 Good response : dense fibrosis; no obvious residual tumour, signifying microscopic residual disease only and on continued surveillance may become TRG1 no viable tumour Courtesy of The Royal Marsden Hospital
34 ROYAL MARSDEN CRITERIA MRI defined complete response: mrtrg1-2: low signal intensity fibrotic scar tissue only seen at MRI performed 4 weeks after long-course CRT, confirmed at 8-12 week MRI Biopsy positive disease not an initial exclusion criterion Thickening of rectal wall not an exclusion Abnormality on endoscopy not an exclusion Clinically palpable tumour not an exclusion PET-CT positivity not an initial exclusion Persistent DWI signal not an initial exclusion Clinical trial : Avoiding Surgery in Rectal Cancer After Pre-Operative Therapy, ClinicalTrials.gov Identifier: NCT

35 PATIENTS DEFERRING SURGERY Follow-up schedule Clinical follow-up MRI PET Sigmoidoscopy CT & colonoscopy 1M, 2M, 3Mly 1-2 yrs, 6Mly 3-4 yrs, then annually 1M, 2M, 3Mly 1 st yr, 6Mly 2 nd yr, annually 2M, 4M, 1 yr 3Mly Yr 1, 6Mly Yr 2, annually As per current NICE guidelines Clinical trial : Avoiding Surgery in Rectal Cancer After Pre-Operative Therapy, ClinicalTrials.gov Identifier: NCT

36 PATIENT ACCRUAL Proforma reporting 40 mrtrg driven FICARE 2007 Trial Protocol Clinical trial : Avoiding Surgery in Rectal Cancer After Pre-Operative Therapy, ClinicalTrials.gov Identifier: NCT

37 PROFORMA REPORTING :
38 THE ENDPOINT Local Failure Powered for unacceptable failure rate 80% power <15% local recurrence at 2 years STOPPING RULE 5 regrowth resulting in positive pathologic CRM trial ends Safe deferral 90% power 10% defer expected to be at least 25% Success 11 of 59 patients safely defer surgery at 2 years Clinical trial : Avoiding Surgery in Rectal Cancer After Pre-Operative Therapy, ClinicalTrials.gov Identifier: NCT


39 TECHNIQUE IS IMPORTANT High Resolution Low Resolution Courtesy of The Royal Marsden Hospital
40 MRTRG AS A RESPONSE BIOMARKER mrtrg 1-2 has similar DFS and OS as pcr but seen more frequently than pcr Tumours continue to show regression with 75% of patients reaching maximum response at 6months mrtrg status at the time of surgery predicts outcome which is independent of baseline tumour stage mrtrg 1-2 at end of treatment for advanced T3/T4 is associated with >80% DFS

41 THE TRIGGER TRIAL: MAGNETIC RESONANCE TUMOUR REGRESSION GRADE AS BIOMARKER FOR STRATIFIED MANAGEMENT OF RECTAL CANCER PATIENTS Clinical trial: ClinicalTrials.gov Identifier: NCT
42 MRI REASSESSMENT AFTER CRT Philosophy of avoiding APE surgery if patient has had a good response to treatment mrtrg used to identify patients suitable for deferral (many are positive on biopsy, DWI or PET-CT) Serial imaging decision for deferral is not based on a single scan Employing serial MRI monitoring = greater rate of recruitment of initially advanced cancers
43 ACKNOWLEDGEMENTS Research Fellows: U Patel, S Yu Deferral of Surgery Trial: RJ Heald, P Tekkis, D Cunningham, D Tait, A Wotherspoon, G Stamp, I Chau MERCURY trial investigators, Pelican Cancer Foundation EXPERT-C trial: A Dewdney, D. Cunningham, J Tabernero, J Capdevila, B Glimelius, A Cervantes, D Tait, A Wotherspoon, Y Chua, R Wong and I Chau CORE Trial investigators: H Rutten, E Rullier, P Quirke, N West, D Sebag-Montefiore, M Peeters, E Van Cutsem, S Ricci, C Van de Velde, R Glynne-Jones
44 WHAT DO YOU NEED? Dedicated colorectal MDT Policy of preoperative MDT review of all rectal cancers using high resolution MRI with specialist colorectal radiologist committed to MDT Patient education: importance of preoperative assessment repeat scans when necessary Team member training and support: multidisciplinary workshops effective most effective when surgeons and radiologists are together Learning curve but teachable e.g. participation and support in clinical trials
45 REPORTING MINIMUM STANDARDS Baseline assessment of Rectal cancer MRI report Primary tumour The primary tumour is demonstrated as an [ Annular Semi-annular Ulcerating Polypoidal Mucinous] mass with a [nodular / smooth] infiltrating border. The distal edge of the luminal tumour arises at a height of [ ] mm from anal verge: The distal edge of the tumour lies [ ]mm [Above,at, below] the top of the puborectalis sling The tumour extends craniocaudally over a distance of [ ] mm The proximal edge of tumour lies [above at below] the peritoneal reflection Invading edge of tumour extends from [ to ] O clock Tumour is [confined to] [extends through] the muscularis propria: Extramural spread is [ ] mm mrt stage: [T1 ] [ T2 ] [ T3a] [ T3b ] [ T3c] [ T3d ] [T4visceral ] [T4 peritoneal] Tumour is [present] [not present] the level of the puborectalis sling at this level: [Tumour is confined to the submucosal layer/part thickness of muscularis propria indicating that the intersphincteric plane/mesorectal plane is safe and intersphincteric APE or ultra low TME is possible] [Tumour extends through the full thickness of the muscularis propria : intersphincteric plane/mesorectal plane is unsafe, Extralevator APE. is indicated for radial clearance] [Tumour extends into the intersphincteric plane : intersphincteric plane/mesorectal plane is unsafe, therefore an extralevator APE. is indicated for radial clearance] [Tumour extends into the external sphincter : intersphincteric plane/mesorectal plane is unsafe.] [ Tumour extends into adjacent [prostate/vagina/bladder/sacrum] : exenterative procedure will be required Lymph node assessment Only benign reactive and no suspicious nodes shown [N0] [ ] mixed signal/irregular border nodes [N1/N2] Extramural venous invasion: [ No evidence ] [ Evidence] [ ] Small [ ]Medium [ ]Large vein invasion is present CRM The closest circumferential resection margin is at o clock The closest CRM is from [Direct spread of tumour] [Extramural venous invasion] [Tumour deposit] Minimum tumour distance to mesorectal fascia: mm [CRM clear ] [CRM involved] Peritoneal deposits: [ No evidence] [ Evidence] Pelvic side wall lymph nodes: [ None] [ Benign] [ Malignant mixed signal/irreg border] Location: [Obturator fossa R L ]. [External Iliac Nodes R L].[ Internal iliac R L ] Summary: MRI Overall stage: T N M [CRM clear], [ CRM involved ], [ EMVI positive] [EMVI negative],[psw positive ] [PSW negative] No adverse features eligible for primary surgery High risk safe margins for preoperative therapy : eligible for Serenade, Marvel Poor prognosis unsafe margins eligible for preoperative chemoradiotherapy: eligible for 6 vs 12 trial Low Rectal <6cm eligible for the Low Rectal Study. Additional comments:. :
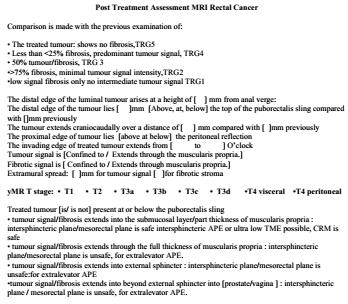
46 REPORTING TEMPLATE POST TREATMENT Post Treatment Assessment MRI Rectal Cancer Comparison is made with the previous examination of: The treated tumour: shows no fibrosis,trg5 Less than <25% fibrosis, predominant tumour signal, TRG4 50% tumour/fibrosis, TRG 3 >75% fibrosis, minimal tumour signal intensity,trg2 low signal fibrosis only no intermediate tumour signal TRG1 The distal edge of the luminal tumour arises at a height of [ ] mm from anal verge: The distal edge of the tumour lies [ ]mm [Above, at, below] the top of the puborectalis sling compared with []mm previously The tumour extends craniocaudally over a distance of [ ] mm compared with [ ]mm previously The proximal edge of tumour lies [above at below] the peritoneal reflection The invading edge of treated tumour extends from [ to ] O clock Tumour signal is [Confined to / Extends through the muscularis propria.] Fibrotic signal is [ Confined to / Extends through muscularis propria.] Extramural spread: [ ]mm for tumour signal [ ]for fibrotic stroma ymr T stage: T1 T2 T3a T3b T3c T3d T4 visceral T4 peritoneal Treated tumour [is/ is not] present at or below the puborectalis sling tumour signal/fibrosis extends into the submucosal layer/part thickness of muscularis propria : intersphincteric plane/mesorectal plane is safe intersphincteric APE or ultra low TME possible, CRM is safe tumour signal/fibrosis extends through the full thickness of muscularis propria : intersphincteric plane/mesorectal plane is unsafe, for extralevator APE. tumour signal/fibrosis extends into external sphincter : intersphincteric plane/mesorectal plane is unsafe:for extralevator APE tumour signal/fibrosis extends into beyond external sphincter into [prostate/vagina ] : intersphincteric plane / mesorectal plane is unsafe, for extralevator APE. Lymph nodes: None /Only benign reactive [N0] Present number mixed signal/irregular border [N1/N2] Extramural venous invasion: [ No evidence Evidence] [ Small Medium Large] CRM Closest circumferential resection margin: [ ]O clock Closest CRM is from [ Direct spread of tumour Extramural venous invasion Tumour deposit] Minimum tumour distance to mesorectal fascia: [ ]mm [ CRM clear CRM involved] Peritoneal deposits: [ No evidence Evidence ] Pelvic side wall lymph nodes: None Benign Malignant [Location: Obturator fossa R L. External Iliac Nodes R L. Inf Hypogastric R L ] Summary: y MRI Overall stage ymrt ymr N M, TRG Low/intermediate risk, CRM clear, TRG 1-2, EMVI negative High prognosis, CRM pos or TRG4/5 or EMVI positive TRG1-2 low tumour eligible for consideration for deferral of surgery :
47 KEY BIOIMAGING MARKERS FOR POOR OUTCOME AT BASELINE AND POST CRT CRM involvement on MRI Depth of extramural spread >5 mm Presence of MRI detected venous invasion MRI detected mucinous tumours Tumour spread into or beyond the intersphincteric plane MRI TRG status
48 THANK YOU!
49 ACKNOWLEDGEMENTS: Pelican Cancer Foundation European Mercury Study Group: Prof B Heald, B Moran, P Quirke, I Swift, P Tekkis, S Stelzner, G Branagan, M Gudgeon, J Strassburg, S Laurberg, T Holm Radiologists in MERCURY I and II: N Bees, H Blake, R Bleehan, L Blomqvist, A Chalmers, M Creagh, HL Emblemsvaag, S Evans, A Guthrie, C George, K Håkon Hole, N Hughes, S McGee, P Knuth, D Peppercorn, C Schubert, A Thrower, T Vertrus Research fellows: S Burton, N Smith, G Salerno, F Taylor, S Dighe, O Shihab, P How, U Patel, J Evans, C Hunter, P Georgiou, V Tudyka, R Siddiqui, J Bhoday, J Read, M Chand, A Wale, A Slesser, N Battersby, S Balyasnikova
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
MRI Rectal Staging Template Revision Summary
 MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
 Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Abstract With the acceleration and ever increasing costs of technologies across the imaging modalities, any
 ISMRM Syllabus Contribution Dr Gina Brown Consultant Radiologist and Reader in Gastrointestinal Cancer Imaging The Royal Marsden NHS Foundation Trust Downs Road Sutton Surrey SM2 5PT Tel +44 208 6613964
ISMRM Syllabus Contribution Dr Gina Brown Consultant Radiologist and Reader in Gastrointestinal Cancer Imaging The Royal Marsden NHS Foundation Trust Downs Road Sutton Surrey SM2 5PT Tel +44 208 6613964
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Post chemoradiation re-staging of rectal cancer using MRI
 Post chemoradiation re-staging of rectal cancer using MRI Thesis submitted in accordance with the regulations of Imperial College London for the degree of MD (Res) Uday Patel MBBS FRCR Division of Surgery,
Post chemoradiation re-staging of rectal cancer using MRI Thesis submitted in accordance with the regulations of Imperial College London for the degree of MD (Res) Uday Patel MBBS FRCR Division of Surgery,
Adjuvant chemotherapy may improve disease-free survival in patients with mremvi-positive rectal cancer following chemoradiation
 Received Date : 28-Apr-2016 Revised Date : 23-Jul-2016 Accepted Date : 05-Aug-2016 Article type : Original Article Adjuvant chemotherapy may improve disease-free survival in patients with mremvi-positive
Received Date : 28-Apr-2016 Revised Date : 23-Jul-2016 Accepted Date : 05-Aug-2016 Article type : Original Article Adjuvant chemotherapy may improve disease-free survival in patients with mremvi-positive
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
MRI in staging of rectal carcinoma
 MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Oncology Review article High-Resolution MRI in Rectal Cancer
 Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance
 Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Advances in Imaging Technology In The Management of Colorectal Cancer
 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Local staging of colon cancer: the current role of CT
 Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment.
 Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Carl Bradbury CoRIPS Research Award 130-9,963.00 The accuracy of the diagnostic pathway for staging of low-mid rectal tumours with endoscopic, MRI and Endorectal Ultrasound assessment. Lay Summary of Project
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative
 Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
MRI After Treatment of Locally Advanced Rectal Cancer: How to Report Tumor Response The MERCURY Experience
 Gastrointestinal Imaging Clinical Perspective Patel et al. MRI After Treatment of Locally Advanced Rectal Cancer Gastrointestinal Imaging Clinical Perspective Uday B. Patel 1 Lennart K. Blomqvist 2 Fiona
Gastrointestinal Imaging Clinical Perspective Patel et al. MRI After Treatment of Locally Advanced Rectal Cancer Gastrointestinal Imaging Clinical Perspective Uday B. Patel 1 Lennart K. Blomqvist 2 Fiona
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
CRC Surgery Educational Slide Deck. Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto
 CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016
 Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Timing and Deferral of Rectal Surgery Following a Continued Response to Pre-operative Chemoradiotherapy
 Timing and Deferral of Rectal Surgery Following a Continued Response to Pre-operative Chemoradiotherapy CCR Reference No.: 2759 Acronym: Deferral of surgery Consultant in Charge Investigators Dr. DM Tait,
Timing and Deferral of Rectal Surgery Following a Continued Response to Pre-operative Chemoradiotherapy CCR Reference No.: 2759 Acronym: Deferral of surgery Consultant in Charge Investigators Dr. DM Tait,
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014
 Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER
 IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER") THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Battersby et al. Trials (2017) 18:394 DOI /s
 18:394 DOI /s") Battersby et al. Trials (2017) 18:394 DOI 10.1186/s13063-017-2085-2 STUDY PROTOCOL A rectal cancer feasibility study with an embedded phase III trial design assessing magnetic resonance tumour regression
Battersby et al. Trials (2017) 18:394 DOI 10.1186/s13063-017-2085-2 STUDY PROTOCOL A rectal cancer feasibility study with an embedded phase III trial design assessing magnetic resonance tumour regression
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
FDG-PET/CT in Gynaecologic Cancers
 Friday, August 31, 2012 Session 6, 9:00-9:30 FDG-PET/CT in Gynaecologic Cancers (Uterine) cervical cancer Endometrial cancer & Uterine sarcomas Ovarian cancer Little mermaid (Edvard Eriksen 1913) honoring
Friday, August 31, 2012 Session 6, 9:00-9:30 FDG-PET/CT in Gynaecologic Cancers (Uterine) cervical cancer Endometrial cancer & Uterine sarcomas Ovarian cancer Little mermaid (Edvard Eriksen 1913) honoring
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive. Lloyd A. Mack September 19, 2015
 Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Differential lymph node retrieval in rectal cancer: associated factors and effect on survival
 Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R