Debaters For The Evening:
|
|
|
- Herbert Brooks
- 5 years ago
- Views:
Transcription

1



2 Your Debaters For The Evening:
3 Current State of Immune Checkpoint Blockade in Selected Types of Solid Tumors Jeffery Weber, MD, PhD Naiyer A. Rizvi, MD
4 Current State of ICI in Melanoma and Bladder Cancers Jeffrey S. Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center
5 Current US/EU Approval Status of ICIs US EU PD-1 PD-L1 CTLA-4 Combo Pembrolizumab Nivolumab Atezolizumab Durvalumab Avelumab Ipilimumab Nivo + ipi Line 1L+ 2L+ 1L+ 2L+ 1L+ 2L+ 2L+ 1L+ 2L+ 1L+ 1L+ mmelanoma NSCLC chl arcc mscchn muc Merkel cell MSI-H chl=classical Hodgkin lymphoma; arcc=advanced renal cell carcinoma; mscchn=metastatic head and neck squamous cell carcinoma; muc=metastatic urothelial cancer; MSI-H=microsatellite instability-high solid tumors Product Prescribing Information Current as of June 2017
6 Should Immunotherapy be the First-line Therapy in all Stage IV Patients?
7 Overall Survival (%) Immune Checkpoint Inhibitors Provide Durable Long-term Survival for Pts with Advanced Melanoma Front-line OS = >50% for Nivolumab N=210 IPI (Pooled Analysis) NIVO Monotherapy (Phase 1 CA ) NIVO Monotherapy (Phase 3 Checkmate-066) N=107 N= Years Schadendorf D, et al. J Clin Oncol. 2015; Hodi S, et al. ASCO. 2016; Atkinson V, et al. Presented at: SMR 2015; November 6-9, 2015; Boston, MA.
8 Long-term Outcomes with Single Agent Pembrolizumab in KEYNOTE mo OS rate was 50% in the pooled pembrolizumab arms (n=556) 33-mo PFS rate was 31% and ORR was 42% Median duration of response was not reached for pembro (range 1.0+ to mo) Responses were durable in pts who completed pembro; 9.7 mo after completion of pembro with estimated PFS (95% CI) 91% (80-96) in 104 pts Pembro front-line responses were durable! Robert C, et al. ASCO
9 First-line Single Agent vs. Concurrent vs. Sequential Immunotherapy?
10 Updated Survival Data in BMS-067 Trial of IPI vs. NIVO vs. IPI/NIVO Median OS, months (95% CI) HR (99.5% CI) vs. IPI HR (99.5% CI) vs. NIVO NIVO + IPI (N=314) NIVO (N=316) IPI (N=315) NR 0.55 ( )* 0.88 ( ) NR (29.1-NR) 0.63 ( )* 20 ( ) *P<.0001 Larkin J, et al. AACR Database lock: September 13, Minimum follow-up of 28 months
11 How Toxic is Combination Checkpoint Blockade? With an additional 19 months of follow-up, safety was consistent with the initial report 1 Patients Reporting Event, % Treatment-related adverse event (AE) Treatment-related AE leading to discontinuation NIVO + IPI (N=313) NIVO (N=313) IPI (N=311) Any Grade Grade 3-4 Any Grade Grade 3-4 Any Grade Grade Treatment-related death 2 (0.6) a 1 (0.3) b 1 (0.3) b a Cardiomyopathy (NIVO+IPI, N=1); Liver necrosis (NIVO+IPI, N=1). Both deaths occurred >100 days after the last treatment. b Neutropenia (NIVO, N=1); Colon perforation (IPI, N=1) 1 Most select AEs were managed and resolved within 3-4 weeks (85-100% across organ categories) ORR was 70.7% for patients who discontinued NIVO+IPI due to AEs, with median OS not reached 1 Larkin J, et al. N Engl J Med. 2015; Larkin J, et al. AACR
12 Toxicity of Immune Checkpoint Blockade Major side effects of immunotherapy are related to development of autoimmunity Immune-related adverse events, also known as immune-mediated adverse events (iraes, imaes), may occur in any organ system Certain events may be life threatening or fatal Prompt recognition of potentially severe iraes improves outcomes Early diagnosis and aggressive systemic corticosteroids are key to prevent lifethreatening consequences Combining checkpoint inhibitors with agents such as CTLA-4 inhibitors, significantly increases iraes
13 First-line Therapy for Melanoma is Immunotherapy for Most Patients Hard to beat the front-line median OS of 30+ months for nivolumab or pembrolizumab alone and 40+ estimated OS for IPI/NIVO 2 year OS for IPI/NIVO concurrent or sequential = 62% is unmatched by any targeted phase III trial Robert C, et al. ASCO. 2017; Larkin J, et al. AACR. 2017; Schadendorf D, et al. J Clin Oncol. 2015; Hodi S, et al. ASCO. 2016; Atkinson V, et al. Presented at: SMR 2015; November 6-9, 2015; Boston, MA.
14 What Should be the First Choice for Adjuvant Therapy in High-risk Melanoma?
15 Overall Survival: Ipilimumab Adjuvant Therapy Eggermont AMM, et al. N Engl J Med
16 Dosing of Ipilimumab as Adjuvant Therapy: 3 vs. 10 mg/kg in E1609 Accrual was 1,670 including 511 IPI10, 636 HDI and 523 IPI3 pts Grade 3+ AEs were seen in 57% of IPI10 and 36% IPI3 pts; discontinuation in 53.8% at IPI10 and 35.2% at IPI3 At a median follow-up of 3.1 years, unplanned RFS analysis showed 3-year RFS of 54% (95% CI: 49, 60) at IPI10 and 56% (50, 61) at IPI3 Tarhini A, et al. ASCO
17 Checkpoint Blockade for Bladder Cancer
18 Efficacy of PD-1 or PD-L1 Immune Checkpoint Inhibitors in Advanced Bladder Cancer Study Previous Platinum? Comparator Drug PD-L1 Assay PD-L1 (+) Expression Cutoff ORR Time to Response (mo) OS (mo) Atezolizumab (IMvigor 210) N=310 Yes No SP142 IC0: <1% (n=103) IC1: 1-5% (n=108) IC2/3: >5% (n=100) All: 15%, IC0: 8% IC1: 10%, IC2/3: 26% 2.1 (95% CI: 2-2.2) All: 7.9 Atezolizumab (IMvigor 210) N=119 No, firstline** No SP142 IC0: <1% (n=39) IC1: 1-5% (n=48) IC2/3: >5% (n=32) All: 19% IC1/2/3: 19% IC2/3: 22% Not Published All: 10.6 Avelumab (JAVELIN) N=241 Yes No Clone >5% (n=81) PD-L1 (-): 14.7% PD-L1 (+): 25% ~2.6 PD-L1 (-) 6 month OS: 52.7% PD-L1 (+) 6 month OS: 61.2% Durvalumab (Study 1108) N=103 Yes No SP263 >25% (n=61) PD-L1 (-): 5.1% PD-L1 (+): 31.1% All: 1.41 PD-L1 (-): 2.05 PD-L1 (+): 1.41 Not Published Nivolumab (CheckMate-275) N=265 Yes No 28-8 pharmdx >1% (n=122) >5% (n=81) All: 19.6%, PD-L1 (-): 16.1% PD-L1 >1%: 23.8% PD-L1 >5%: 28.4% 1.87 (95% CI: ) All: 8.74 PD-L1 (-): PD-L1 >1%: 11.3 Nivolumab (CheckMate-032) N=78 Yes No 28-8 pharmdx <1% (n=42) >1% (n=25) All: 24.4% PD-L1 (-): 26.2% PD-L1 (+): 24% 1.5 (95% CI: ) All: 9.7 PD-L1 (-): 9.9 PD-L1 (+): 16.2 Pembrolizumab (KEYNOTE-045) N=542 Yes Paclitaxel, docetaxel or vinflunine 22C3 pharmdx >10% (n=164)* All: 21.1 vs. 11.4% PD-L1 (+): 21.6 vs. 6.7% 2.1 All: 10.3 vs. 7.4 PD-L1 (+): 8 vs. 5.2 Pembrolizumab (KEYNOTE-052) N=100/374 No, firstline** Gill DM, et al. Immunotherapy No 22C3 pharmdx >10% (n=30) All: 24% PD-L1 (+): 37% 2 (95% CI: 0.2-5) 6 month OS: 67% *Cisplatin ineligible patients; **PD-L1 expression included percentage of tumor and infiltrating immune cells with PDL1 expression
19 % Efficacy of PD-1 or PD-L1 Inhibitors in 2 nd Line Metastatic Bladder Cancer Objective Response Rate 19.6% 20.4% 17.6% 21.1% % Historic control with chemotherapy 12% 5 0 Atezolizumab N=310 Loriot ESMO 16 Nivolumab N=265 Sharma Lancet Oncol 17 Durvalumab N=103 Powles ASCO GU 17 Avelumab N=153 Patel ASCO GU 17 Pembrolizumab N=270 Bellmunt New Engl J Med 17 Black P. Presented at AUA 2017 (Adapted from Plimack ASCO 2016).
20 % ICI Response According to PD-L1 Expression in Advanced Bladder Cancer PD-L1 Positive PD-L1 Negative Atezolizumab N=310 Loriot ESMO 16 Nivolumab N=265 Sharma Lancet Oncol 17 Durvalumab N=103 Powles ASCO GU 17 Avelumab N=153 Patel ASCO GU 17 Pembrolizumab N=270 Bellmunt New Engl J Med 17 Adapted from Black P. Presented at AUA 2017.
21 % Grade >3 Adverse Events from ICIs in Advanced Bladder Cancer 20 (2 nd line Metastatic Trials) % 18% 15% 8 7.5% 4 5.2% 0 Atezolizumab N=310 Loriot ESMO 16 Nivolumab N=265 Sharma Lancet Oncol 17 Durvalumab N=103 Powles ASCO GU 17 Avelumab N=153 Patel ASCO GU 17 Pembrolizumab N=270 Bellmunt New Engl J Med 17 Adapted from Black P. Presented at AUA 2017.
22 KEYNOTE-045 Study (NCT ) Overall Survival: Total 43.9% 30.7% Events, n HR (95% CI) P Pembro ( ) Chemo 179 Pembrolizumab Chemotherapy Median (95% CI) 10.3 mo ( ) 7.4 mo ( ) Bellmunt J, et al. N Engl J Med No. at risk
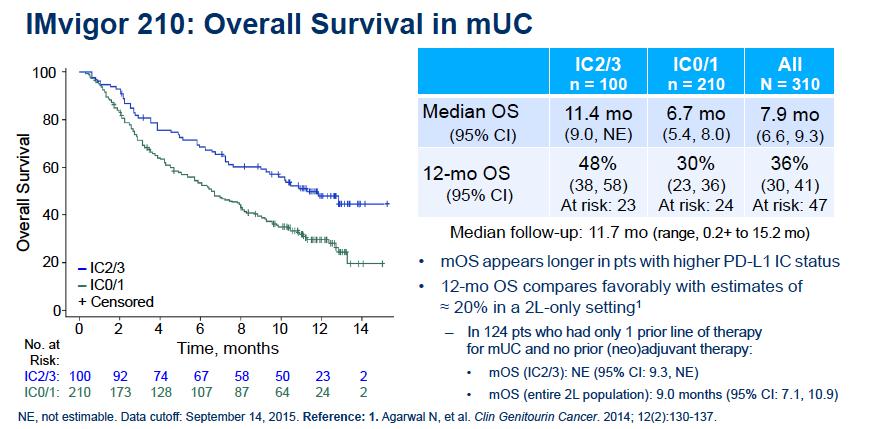
23 Long-term Survival Follow-up of the Phase I Atezolizumab Trial Median and Landmark OS by PD-L1 Status IC0/1 (N=44) IC2/3 (N=51) All Pts* (N=95) Median OS (95% CI) 7.6 mo (4.7, 13.9) 11.3 mo (7.8, NE) 10.1 mo (7.3, 17) 1-year OS rate (95% CI) 40% (25, 56) 50% (36, 64) 46% (35, 56) 2-year OS rate (95% CI) 14% (2, 26) 43% (29, 57) 30% (20, 40) NE=Not estimable; *Efficacy-evaluable population with >12 wk f/u - A trend toward longer survival in pts with higher PD-L1 status was observed. Petrylak D, et al. Presented at ASCO GU With extended follow-up, single-agent atezolizumab continues to be well-tolerated in this phase Ia study muc cohort Most AEs were grade 1-2, and no treatment-related deaths occurred. Incidence declined substantially (including grade 3-4) after the first year. Clinical benefit was observed in a heavily pre-treated muc population Confirmed, ORs were durable (40% ongoing), with a median DOR of 22 mo and DOR up to 33+ mo observed Median OS was ~10 mo, with 46% and 30% of patients alive after 1 and 2 years, respectively (median survival follow-up duration, ~29 mo) Supports a role for atezolizumab as new standard of care in previously treated muc Phase III study IMvigor211 (NCT ) is ongoing, with enrollment completed and data expected later this year.
 Urothelial Cancer Progression or recurrence of urothelial cancer following a first-line platinumcontaining regimen Randomization N=932 Estimated Completion:")

24 Atezolizumab was not Superior to Chemotherapy in Cisplatin-resistant Bladder Cancer?? IMvigor211 Study Design (NCT ) Urothelial Cancer Progression or recurrence of urothelial cancer following a first-line platinumcontaining regimen Randomization N=932 Estimated Completion: Nov 2017 Atezolizumab SOC: Docetaxel, Paclitaxel or Vinflunine Primary Endpoints OS Secondary Endpoints ORR PFS DOR Safety Primary efficacy endpoint, OS, was to be tested in a successive fashion in study populations defined by PD-L1 expression. The first population tested was people with the highest levels of PD-L1 expression (IC2/3), followed by those with any level of PD-L1 expression (IC1/2/3), and followed by the overall study population (ITT). Statistical significance needed to be achieved in the IC2/3 population in order to evaluate the IC1/2/3 population for statistical significance, and similarly achieved in the IC1/2/3 population in order to evaluate the overall study population for statistical significance.
25 Is PD-L1 Staining Associated with Clinical Outcome in Bladder Cancer? Study Agent Companion IHC Antibody Threshold for Positivity Target Cells Assay Associated w/ Response? Powles T, et al. Nature Atezolizumab Proprietary 5% TILs Yes Rosenberg JE, et al. Lancet Atezolizumab SP142 5% TILs Yes Balar AV, et al. Lancet (platinum ineligible) Atezolizumab SP142 5% TILs No Massard C, et al. J Clin Oncol Durvalumab SP263 25% TILs & TCs Yes Sharma P, et al. Lancet Oncol Nivolumab Dako % TCs No Sharma P, et al. Lancet Oncol Nivolumab Dako % TCs Yes Plimack ER, et al. Lancet Oncol Pembrolizumab 22C3 1% TILs & TCs TILs only Bellmunt J, et al. N Engl J Med (chemo vs immuno 2 nd line) Pembrolizumab 22C3 10% TILs & TCs No
26 Checkpoint Inhibitor Adverse Events (occurring in 10% of those with urothelial cancer that has progressed on platinum-containing regimen) Avelumab Atezolizumab Durvalumab Nivolumab Pembrolizumab Adverse Event, (%) All Grades Grades 3-4 All Grades Grades 3-4 All Grades Grades 3-4 All Grades Grades 3-4 All Grades Grades 3-4 Gen - Fatigue Gen - Periph edema Gen - Pyrexia GI - Constipation GI - Nausea GI - Vomiting GI Abdominal pain GI Diarrhea/colitis Resp - Cough Resp - Dyspnea Skin - Rash GU - UTI GU - Hematuria Musculoskeletal pain Reduced appetite U.S. FDA Prescribing Information
27 Conclusions: Checkpoint Blockade for Bladder Cancer Checkpoint inhibitors blocking the PD-1/PD-L1 axis including avelumab, nivolumab, pembrolizumab, durvalumab, and atezolizumab are well tolerated and active in metastatic bladder cancer Five drugs are approved in second-line bladder cancer; two of those are also approved first-line if cisplatin-ineligible PD-L1 staining is a poor biomarker for outcome, but may be associated with survival in some studies New immunotherapy combinations merit testing
28 Immunotherapy Advances in NSCLC Naiyer A. Rizvi, MD Price Family Chair, Clinical Translational Medicine Professor of Medicine Director, Thoracic Oncology Co-Director, Cancer Immunotherapy Columbia University Medical Center
29 OS (%) CA Five-Year Update: Phase I Nivolumab in Advanced NSCLC Median OS (95% CI), mo Overall (N=129) 9.9 (7.8, 12.4) y OS, 42% 2 y OS, 24% 3 y OS, 18% 5 y OS, 16% No. at Risk Years Brahmer J, et al. AACR
30 KEYNOTE-024 Study Design Key Eligibility Criteria Untreated stage IV NSCLC PD-L1 TPS 50% Pembrolizumab 200 mg IV Q3W (2 years) ECOG PS 0-1 No activating EGFR mutation or ALK translocation No untreated brain metastases No active autoimmune disease requiring systemic therapy R (1:1) N=305 Platinum-Doublet Chemotherapy (4-6 cycles) PD Pembrolizumab 200 mg Q3W for 2 years Key Endpoints Primary: PFS (RECIST v1.1 per blinded, independent central review) Secondary: OS, ORR, safety Exploratory: DOR Reck a To be eligible M, et for al. crossover, N Engl PD J Med. had to 2016; be confirmed by blinded, independent central NCT radiology review and all safety criteria had to be met.
 0 3 6 9 12 15 18 Time, months 154 104 89 44 22 3 1 151 99 70 18 9 1 0 48% 15% Pembrolizumab Chemotherapy <.001 Assessed per RECIST v1.")
31 PFS, % KEYNOTE-024: Progression Free Survival No. at risk Reck M, et al. N Engl J Med % 50% Events, n Median, mo HR (95% CI) P Pembro Chemo ( ) Time, months % 15% Pembrolizumab Chemotherapy <.001 Assessed per RECIST v1.1 by blinded, independent central review. Data cut-off: May 9, 2016.
32 O S, % No. at risk KEYNOTE-024: Overall Survival 80% 72% Time, months Reck M, et al. N Engl J Med Data cut-off: May 9, % 54% Events, n Median, mo HR (95% CI) P Pembro 44 NR 0.60 Chemo 64 NR ( ) Pembrolizumab Chemotherapy.005
33 Key Eligibility Criteria: Stage IV or recurrent NSCLC No prior systemic therapy for advanced disease No EGFR/ALK mutations sensitive to available targeted inhibitor therapy 1% PD-L1 expression CheckMate-026 Study Design Nivolumab vs. Chemotherapy in First-line NSCLC (Phase III) R 1:1 Stratification Factors at Randomization: PD-L1 Expression (<5% vs. 5%) Histology (squamous vs. non-squamous) Socinski M, et al. ESMO. 2016; Nivolumab 3 mg/kg Q2W N=271 Chemotherapy (histology dependent) Maximum of six cycles N=270 Tumor scans Q6W until week 48 then Q12W Disease Progression or Unacceptable Toxicity Disease Progression Crossover Nivolumab (optional) Primary Endpoint: PFS per BIRC ( 5% PD-L1 +) Secondary Endpoints: PFS per BIRC ( 1% PD-L1 +) OS ORR Exploratory Objective: Predictive biomarkers for outcomes with nivolumab
34 PFS (%) CheckMate-026: Primary Endpoint PFS per IRRC in (>5% PD-L1+) Median PFS, months (95% CI) Nivolumab n= (3.0, 5.6) Chemotherapy n= (5.4, 6.9) 1-year PFS rate, % HR=1.15 (95% CI: 0.91, 1.45), P= Nivolumab No. of patients at risk: Nivolumab Chemotherapy Socinski M, et al. ESMO Months Chemotherapy All randomized patients ( 1% PD-L1+): HR = 1.17 (95% CI: 0.95, 1.43)
35 PFS (%) CheckMate-026: TMB Analysis High TMB Low/Medium TMB Median PFS, months (95% CI) Nivolumab Chemotherapy n=47 n= (5.1, NR) 5.8 (4.2, 8.5) Median PFS, months (95% CI) Nivolumab Chemotherapy n=111 n= (2.8, 5.4) 6.9 (5.5, 8.6) HR = 0.62 (95% CI: 0.38, 1.00) HR = 1.82 (95% CI: 1.30, 2.55) Nivolumab Chemotherapy Chemotherapy Nivolumab No. at Risk Nivolumab Chemotherapy Adapted from Peters, et al. AACR Months Months
36 PACIFIC Study: Durvalumab Monotherapy in NSCLC Phase 3, randomized, double-blind, placebo-controlled, multicenter, global study (26 countries) Patients with locally advanced unresectable NSCLC (Stage III) in a consolidation setting (N=702) Arm 1 (n=468): Durvalumab IV 10 mg/kg Q2wks for up to 12 months Absence of progression following at least 2 cycles of platinum-based chemotherapy concomitant with radiation therapy Primary endpoints PFS, OS Secondary endpoints ORR, DoR, DSR Safety/tolerability PK, immunogenicity, QOL R 2:1 Arm 2 (n=234): Placebo IV Q2wks Est. completion: 2017 FPD: Q2 14 LPCD: Q NCT ; Creelan B, et al. Ann Oncol
37 Response Rate (%) Ipilimumab and Nivolumab: First-line NSCLC Unselected >1% PD-L1 >50% PD-L1 6 CRs CM-012 mono (1L) CM-012 combo (1L) Hellmann, et al. Lancet Oncol

38 Antonia S, et al. Lancet Oncol Durvalumab and Tremelimumab in NSCLC
39 KEYNOTE-021: Cohort G Key Eligibility Criteria Untreated stage IIIB or IV nonsquamous NSCLC No activating EGFR mutation or ALK translocation Provision of a sample for PD-L1 assessment a ECOG PS 0-1 No untreated brain metastases No ILD or pneumonitis requiring systemic steroids R (1:1) a N=123 End Points Primary: ORR (RECIST v1.1 per blinded, independent central review) Key secondary: PFS Other secondary: OS, DOR, safety Exploratory: Relationship between antitumor activity and PD-L1 TPS Pembrolizumab 200 mg Q3W for 2 years + Carboplatin AUC 5 mg/ml/min + Pemetrexed 500 mg/m 2 Q3W for 4 cycles b Carboplatin AUC 5 mg/ml/min + Pemetrexed 500 mg/m 2 Q3W for 4 cycles b PD Pembrolizumab 200 mg Q3W for 2 years Langer, et al. Lancet Oncol. 2016; NCT a Randomization was stratified by PD-L1 TPS <1% vs 1%. b Indefinite maintenance therapy with pemetrexed 500 mg/m 2 Q3W permitted.



 Pembro + chemo 23")
40 Randomized Phase II: Carbo/Pemetrexed +/- Pembrolizumab PF S, % % 63% 13.0 mo 8.9 mo Chemo Time, months No. at risk PFS Pembro + Chemo Δ26% P=.0016 Events, n HR (95% CI) Pembro + chemo ( ) Chemo alone 33 P=.0102 Langer, et al. Lancet Oncol Pembro + Chemo Chemo Alone

41 Objective Response by PD-L1 TPS Langer, et al. Lancet Oncol <1% n=21 1% n=39 1%-49% n=19 50% n=20 Pembrolizumab + Chemotherapy <1% n=23 1% n=40 1%-49% n=23 Chemotherapy Alone 50% n=17 Horizontal dotted lines represent the ORR in the total population. Assessed per RECIST v1.1 by blinded, independent central review. Data cut-off: August 8, 2016.
42 Overall Survival % 92% 75% 72% O S, % Papadimitrakopoulou, et al. ASCO (Abstract 9094) Updated HR: 0.69 No. at risk Langer, et al. Lancet Oncol Time, months
43 Phase III First-line Combination Trials in Advanced NSCLC Treatment N Arms CheckMate Nivolumab, Ipilimumab Nivolumab MYSTIC 1092 KEYNOTE Impower Durvalumab, Tremelimumab Pembrolizumab, Pemetrexed, Carboplatin Atezolizumab, Paclitaxel/Carboplatin, Bevacizumab Durvalumab Atezolizumab, Paclitaxel/ Carboplatin Platinum-doublet Chemotherapy SOC Platinum-based Chemotherapy Pemetrexed, Carboplatin Paclitaxel/Carboplatin
44

45 Current Status and Future Prospects for Development of Robust Prognostic and Predictive Biomarkers of Response in Selected Types of Solid Tumors
46 POINT: PD-L1 Staining by IHC is Generally a Useful Marker for the Benefit of PD-1 Blockade Joaquim Bellmunt, MD, PhD Associate Professor of Medicine Director, Bladder Cancer Center Dana-Farber Cancer Institute Boston, MA
47 The Rationale for PD-L1 Testing in Cancer PD-L1 Expression as a Predictive Biomarker Are tumors with high PD-L1 expression more sensitive to immune-mediated approaches compared with tumors that have low or no PD-L1 expression? The Prognostic Value of PD-L1 Expression Are tumors with high PD-L1 expression associated with better or worse prognosis compared with tumors that have low or no PD-L1 expression?
48 High PD-L1 Expression May Be Associated with Poor Prognosis Wu P, et al. PLoS ONE

49 Zhao T, et al. PLoS ONE
50 Considerations for PD-L1 Expression as a Predictive Biomarker and PD-L1 Testing Tumor Type PD-L1 Expression Level Cell Types That Express PD-L1 Variability Across PD-L1 Assays


51 PD-L1 Expression Can Vary Between Primary And Metastasis, Different Metastases, and Within One Tissue Sample Variation of PD-L1 Expression Within One Single NSCLC Tissue Sample 1 : Variation of PD-L1 Expression Between Primary Tumor Metastases 2 : Primary Melanoma Lymph Node Metastasis Brain Metastasis In 20 NSCLC samples tested with the anti PD-L IHC assay, discordant PD-L1 results were observed in 30% of the matched primary versus metastatic cases 3 1 McLaughlin J, et al. JAMA Oncol. 2016; 2 Madore J, et al. Pigment Cell Melanoma Res. 2015; 3 Phillips T, et al. Appl Immunohistochem Mol Morphol
52 PD-L1 Expression May Predict Sensitivity to Immune-Mediated Approaches Study Cancer Type Level of PD-L1 Expression ORR, % (vs. control) Fehrenbacher NSCLC TC3 or IC3* TC2 or IC2* TC1 or IC1* TC0 or IC0* 37.5 (13.0) 7.7 (15.6) 14.0 (19.1) 7.8 (9.8) Massard Bladder PD-L1 positive** PD-L1 negative** TC IC TC or IC Borghaei Non-squamous NSCLC PD-L1 10% PD-L1 5% PD-L1 1% 37 (13) 36 (13) 31 (12) Ferris SCCHN PD-L1 10% PD-L1 5% PD-L1 1% 27.9 (2.9) 22.2 (2.3) 17.0 (1.6) Rosenberg Bladder IC2/3 IC1/2/3 All IC=immune cells; IHC=immunohistochemistry; TC=tumor cells *TC3 50%, TC2 5% and <50%, TC1 1% and <5%, and TC0 <1%; IC3 10%, IC2 5% and <10%, IC1 1% and <5%, and IC0 <1% **PD-L1 positive: either TC or IC 25%, PD-L1 negative: both TC and IC <25% 1 Fehrenbacher L, et al. Lancet. 2016; 2 Massard C, et al. J Clin Oncol. 2016; 3 Borghaei H, et al. N Engl J Med. 2015; 4 Ferris RL, ASCO 2016; 5 Rosenberg JE, et al. Lancet
53 Advances in Other Treatment Settings in Advanced NSCLC: Pembrolizumab Immunotherapy (KEYNOTE 010 & 024) Pembrolizumab treatment setting: Indicated for first-line treatment for patients with metastatic NSCLC whose tumors express PD-L1 in 50% of cells and who do not have EGFR- or ALK-positive tumor mutations. Also indicated for patients with locally advanced or metastatic NSCLC progressing after 1 prior chemotherapy regimen and whose tumors express PD-L1 with 1% of cells. Patients with EGFR- or ALK-positive tumor mutations should also have received targeted therapy prior to treatment with pembrolizumab 1 Results from a randomized Phase III clinical trial: 2 Median OS TPS 50% 3,a Pembrolizumab 10 mg/kg (n=346) Pembrolizumab 2 mg/kg (n=345) Docetaxel (n=343) HR (95% CI) 0.38 (0.38, 0.77) P= (0.36, 0.7) P<.0001 Median OS a 4,a Median PFS (0.58, 0.88) P=.0008 p= (0.74, 1.05) P= (0.49, 0.75) P< (0.66, 0.94) P=.004 a Primary endpoint Time (months) 1 FDA Prescribing Information; 2 Herbst RS, et al. Lancet 2016; 3 Reck M, et al. N Engl J Med
54 Summary of FDA-Approved and Investigational PD-L1 Assays in Urothelial Carcinoma* Ab clone/ epitope Pembrolizumab 1 22C3 Atezolizumab 2,3 SP142 Nivolumab Durvalumab 5 SP263 Avelumab Cell type scored TCs and ICs ICs TCs TCs or ICs TCs Scoring method FDA status for urothelial carcinoma PD-L1 thresholds under evaluation CPS: % of PD-L1 positive TCs and ICs relative to the total number of tumor cells NA 1% 10% % of PD-L1 expressing ICs Complementary IC2/3 ( 5%), IC1 ( 1% but <5%), IC0 (<1%) % of PD-L1 expressing TCs NA 1% 5% % of PD-L1 expressing TCs or ICs NA 25% % of PD-L1 expressing TCs NA 5% * No head-to-head studies have been conducted and direct comparisons cannot be made between these studies. 1 Bellmunt J, et al. N Engl J Med. 2017; 2 Loriot Y, et al. Poster presentation at ESMO Abstract 83P; 3 Ventana. Roche receives FDA Approval for novel PD-L1 biomarker assay [press release]. May 18, 2016; 4 Sharma P, et al. Lancet Oncol. 2017; 5 Powles T, et al. Poster presentation at ASCO GU Abstract 286; 6 Patel M, et al. Poster presentation at ESMO Abstract 777PD.


55 Rosenberg JE, et al. Lancet PD-L1 Antibody Atezolimumab in Cisplatin-resistant Bladder Cancer
 2.00 (1.87 2.63) 1.87 (1.77 2.04) 3.55 (1.94 3.")
 Ongoing responders at time of response: 40/52 (77%) Safety: No new safety profile compare to prior reports a BIRC, blinded independent review committee Sharma P, et al.")
56 Phase II CheckMate 275 Study in Chemo-resistant Bladder Cancer: Nivolumab is Active All PD-L1 <1% PD-L1 1% PD-L1<5% PD-L1 5% Outcome, % N=265 n=143 n=122 n=184 n=81 Confirmed ORR by BIRC a % CI Median PFS in months (95% CI) 2.00 ( ) 1.87 ( ) 3.55 ( ) Median OS in months (95% CI) 8.74 (6.05 NR) 5.95 ( ) (8.74 NR) Responders (N=52) Time to response: 1.9 months ( ) Duration of response: NR (7.4-NR) Ongoing responders at time of response: 40/52 (77%) Safety: No new safety profile compare to prior reports a BIRC, blinded independent review committee Sharma P, et al. Lancet Oncol
57 Clinical Response to Durvalumab Monotherapy in UC Correlates with PD-L1 Expression Antitumour Activity of Durvalumab per BICR in the Primary Efficacy Population of the UC Cohort, including the Second-line or Greater ( 2L) Post-platinum Subgroup ORR, n (%) (95% CI) ORR, n (%) (95% CI) Total PD-L1 High PD-L1 Low/Neg ORR by BICR assessment Primary Efficacy Population (103pts, 13 weeks follow-up) N=103 N=61 N=39 21 (20.4) (13.1, 29.5) 19 (31.1) (19.9, 44.3) ORR by BICR assessment ( 2L) post-platinum subgroup 2 (5.1) (0.6, 17.3) N=94 N=58 N=33 19 (20.2) (12.6, 29.8) 18 (31.0) (19.5, 44.5) 1 (3.0) (0.1, 15.8) Clinical activity seen in all patient subgroups Greater efficacy occurred in patients with PD-L1 high expression Efficacy is still observed in the PD- L1 low/neg group consistent with the level seen with SoC PD-L1 SP263 assay is especially helpful in informing patients on the likelihood of response to durvalumab Powles, et al. Presented at 2017 ASCO GU.
58 KEYNOTE-052: Pembrolizumab as 1 st -Line Therapy for Cisplatin-Ineligible Bladder Cancer Objective Response (by PD-L1 Subgroups) CPS <1% N=33 CPS 1% to <10% N=33 CPS 10% N=30 N = 100 n % (95% CI) n % (95% CI) n % (95% CI) ORR (24%) 6 18% (7-36%) 5 15% (5-32%) 11 37% (20-56%) Complete response 1 3% (0.1-16%) % (4-31%) Partial response 5 15% (5-32%) 5 15% (5-32%) 7 23% (10-42%) Stable disease 3 9% (2-24%) 5 15% (5-32%) 7 23% (10-42%) Excluding those with CPS unknown *CPS=Combined positive score for PD-L1 positive cells (tumor, immune cells) Median time to response: 2.0 months (range, ) Median duration of response : Not reached (range, 1.4+ to 9.8+ months) Duration of response rate 6 months: 83% The PD-L1 high expression cut point was determined to be CPS 10% (PD-L1 positive tumor, immune cells) and enriched for response; this cut point will be validated in the remaining patients in the cohort (n=274 additional patients) Balar A, et al. Ann Oncol Data cutoff date: June 1, 2016
59 Overall Survival, (%) Adapted from 1 Bellmunt J, et al. N Engl J Med. 2017; 2 Bellmunt J, et al. Oral presentation at SITC 2016; 3 Overall Survival, (%) KEYNOTE-045: Overall Survival* No. at Risk Pembro Chemo Overall Survival: Total Time (months) Median OS, months (95% CI) Pembrolizumab 10.3 ( ) Chemotherapy 7.4 ( ) HR: 0.73; 95% CI, ; P= No. at Risk Pembro 74 Chemo 90 Overall Survival: CPS 10% 2 Median OS, months (95% CI) Pembrolizumab 8.0 ( ) Chemotherapy 5.2 ( ) HR: 0.57; 95% CI, ; P= Time (months) *Assessed per RECIST v1.1 by blinded, independent central review. Data cutoff date: Sep 7, CPS is the % of PD-L1 positive tumor cells and tumor-infiltrating immune cells relative to the total number of tumor cells.
60 PD-L1 Expression as a Predictor of Checkpoint Blockade Sensitivity in UC Powles, et al. Nature Phase I Atezolizumab Rosenberg, et al. Lancet Phase II Atezolizumab Balar, et al. Lancet Phase II Atezolizumab Massard, et al. J Clin Oncol Phase I Durvalumab Sharma, et al. Lancet Oncol Phase I/II Nivolumab Sharma, et al. Lancet Oncol Phase I/II Nivolumab Plimack, et al. Lancet Oncol Phase I Pembrolizumab Bellmunt, et al. N Engl J Med Phase III Pembrolizumab 5/8 studies reported positive association with PD-L1 staining
61 Key Diagnostic Challenges in UC In-clinic use of PD-L1 expression is likely to differ across lines of therapy Multiple diagnostic assays & algorithms used in clinical development: confusion regarding the impact of the test used
62 UC: SP263 Uses Tumor and Immune Cell Scores Durvalumab Tumour Cell (TC) Area TC area with PD-L1 expression IC area with PD-L1 expression Immune Cell (IC) area Definition Tumour Cell: Proportion of tumour cells with membrane staining for PD-L1 at any intensity above background staining Immune Cell: Proportion of tumour associated immune cells with staining for PD-L1 at any intensity above background staining OR Assay SP263 Cut-offs for PD-L1 High TC 25% or IC 25%
63 UC: SP142 Uses Tumor and Immune Cell Scores Atezolizumab Tumour Area Definition The proportion of tumour area occupied by PD- L1 expressing tumour-infiltrating immune cells of any intensity IC area with PD-L1 expression Assay Cut-offs for PD-L1 High SP142 5%

64 UC: 22C3 Uses Combined Proportion Score Pembrolizumab Tumour Cell (TC) Area TC area with PD-L1 expression Definition The percentage of PD-L1 expressing tumour and infiltrating immune cells relative to the total number of immune cells. IC area with PD-L1 expression + Assay 22C3 10% Cut-offs for PD-L1 High
65 Overall Survival (Probability) Overall Survival (Probability) CheckMate 025: OS by PD-L1 Expression in arcc Overall Survival: PD-L1 1% Median OS, months (95% CI) Nivolumab 21.8 ( ) Everolimus 18.8 ( ) Everolimus Time (months) Nivolumab No. of patients at risk Nivolumab Everolimus Overall Survival: PD-L1 <1% Median OS, months (95% CI) Nivolumab 27.4 (21.4 NE) Everolimus 21.2 ( ) HR (95% CI): 0.79 ( ) HR (95% CI): 0.77 ( ) Everolimus Time (months) Nivolumab No. of patients at risk Nivolumab Everolimus Adapted from Motzer, et al. N Engl J Med. 2015; Sharma P, et al. Oral presentation at ESMO Abstract 3LBA. Based on data cut-off of June 2015.
66 PFS PFS IMmotion 150: IRF-Assessed PFS ITT Population 1% of IC expressing PD-L1 Atezo + bev (n=101) Atezo (n=103) Sunitinib (n=101) mpfs, mos (95% CI) Stratified HR* (95% CI) 11.7 ( ) 1.00 ( ) P= ( ) 1.19 ( ) P= ( ) -- Atezo + bev (n=50) Atezo (n=54) Sunitinib (n=60) mpfs, mos (95% CI) Stratified HR* (95% CI) 14.7 ( ) 0.64 ( ) P= ( ) 1.03 ( ) P= ( ) No. at Risk Atezo + bev Atezo Sunitinib Time (months) No. at Risk Atezo + bev Atezo Sunitinib Time (months) *Compared with sunitinib. P values for descriptive purposes only and not adjusted for multiple comparisons. Adapted from McDermott D, et al. Poster presentation at ASCO GU Abstract 431.
67 Phase II Study of Atezolizumab + Bevacizumab vs. Sunitinib Phase I study: ORR 40% Phase II: PFS did not pan out but response seen in both PD-L1 high/low Overall survival a better metric Subsets of high PD-L1 cancers? McDermott D, et al. IMmotion150 biomarkers: AACR
68 PD-L1 in SCCHN Treated with Nivolumab Exploratory analysis: Patients with a tumor PD-L1 expression level of 1% or more may have a greater magnitude of effect from nivolumab therapy than those whose PD-L1 level was less than 1%. Ferris RL, et al. N Engl J Med
69 Conclusions The rationale includes potential prognostic and predictive value of PD-L1 testing PD-L1 positivity enriches for clinical benefit for selected drugs, diseases and settings IHC is unreliable for measuring PD-L1 expression Need to look beyond a single static biomarker Ergo, PD-L1 staining is not a useful helpful biomarker setting-based

70 Current Status and Future Prospects for Development of Robust Prognostic and Predictive Biomarkers of Response in Selected Types of Solid Tumors
71 COUNTERPOINT: PD-L1 Staining is Not All It s Purported to Be Jeffrey S. Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center
72 PD-L1 tumor staining makes little difference in melanoma, bladder, and RCC, but has some impact in lung cancer; with combined therapy, it is not useful
73 Nivolumab vs. DTIC-OS by PD-L1 Status in Front-line Melanoma Atkinson, et al. SMR
74 PD-L1 Staining is Associated with Superior OS and PFS with Pembrolizumab in Melanoma, but Does Not Rule Out Benefit PD-L1 positive PD-L1 positive PD-L1 negative PD-L1 negative No. at risk PD-L1 positive PD-L1 negative No. at risk PD-L1 positive PD-L1 negative Daud A, et al. J Clin Oncol
75 Larkin J, et al. AACR PD-L1 Staining Falls Out as a Factor with Combined Checkpoint Blockade in Melanoma
76 No Impact of PD-L1 Staining on Outcome in Squamous NSCLC Treated with Nivolumab Brahmer J, et al. N Engl J Med
77 No Impact of PD-L1 Staining on OS for Atezolizumab in Second-line NSCLC vs. Chemotherapy Rittmeyer A, et al. Lancet
78 Rizvi N, et al. J Clin Oncol No Impact of PD-L1 Expression on Outcome with Front-line NIVO + Chemotherapy in NSCLC
79 No Impact of PD-L1 Staining on Efficacy of Pembrolizumab in Refractory SCCHN PD-L1-positive patients PD-L1-negative patients PD-L1-positive patients PD-L1-negative patients Bauml J, et al. J Clin Oncol
80 Benefit of Nivolumab Compared to Everolimus in Renal Cell Cancer is Independent of PD-L1 Staining Kaplan-Meier Curve for Overall Survival, According to Programmed Death 1 Ligand (PD-L1) Expression Level Motzer R, et al. N Engl J Med
81 Little Impact of PD-L1 Staining on Survival in Renal Cell Cancer Patients Treated with Atezolizumab McDermott D, et al. J Clin Oncol
82 No Impact of PD-L1 Staining on OS in Refractory Bladder Cancer Patients Treated with Atezolimumab Balar A, et al. Lancet

83 Almost All Cells were PD-L1 Positive in Relapsed/Refractory Hodgkin s Lymphoma - Not Useful Chen, et al. J Clin Oncol

84 Presented By Noah Hahn at 2015 ASCO Annual Meeting PD-L1 Status Summary
85 What are the Facts? In non-squamous NSCLC, clear association of PD-L1 staining level and OS benefit from nivolumab versus chemotherapy 1 However, in all other histologies in phase II/III trials, there is unclear benefit of PD-L1 staining With combination immune checkpoint blockade, PD-L1 staining is not a useful biomarker The utility of a predictive biomarker is to inform who not to treat: by that criterion, PD-L1 staining falls short Choosing patients by PD-L1 staining will increase response rates PD-L1 staining can be difficult to quantitate, may vary from tumor to tumor, and may vary over time within a tumor, and is inducible Ergo, PD-L1 staining is not a useful biomarker 1 Borghaei, et al. N Engl J Med
86
87 Emerging Concepts of Combined Immune Checkpoint Blockade
88 POINT: The Efficacy of CTLA-4 + PD-1 is Superior to PD-1 Blockade Alone Robert L. Ferris, MD, PhD UPMC Endowed Professor and Chief Division of Head and Neck Surgery Associate Director for Translational Research Co-Leader, Cancer Immunology Program University of Pittsburgh Cancer Institute Pittsburgh, PA



89 Therapies to Drive an Immune Response Vaccines Adoptive T-cell therapies CAR-T TIL therapy Cytokines TLR agonists Agonist Abs (4-1BB, OX-40) Checkpoint blockade (Abs blocking CTLA4, PD-1, PD-L1)

90 Multiple Immuno-Inhibitory Pathways Regulate T-cell Tolerance and T-cell Exhaustion Potent ability to limit T-cell function Numerous therapeutic opportunities Many unanswered questions Freeman GJ, Sharpe AH. Nat Immunol Not Pictured: TIGIT, B7-H4, B7-H5/VISTA

91 Activating and Inhibitory Co-Receptors CD28 OX40 GITR CD137 CD27 Activating Receptors HVEM Inhibitory Receptors CTLA-4 LAG-3 PD-1 TIM-3 BTLA VISTA Ipilimumab Tremelimumab Pembrolizumab Nivolumab Durvalumab Mellman I, et al. Nature Agonistic antibodies T-cell stimulation Blocking antibodies
92 Proportion Alive Pooled OS Including EAP Data: 4846 pts Median OS (95% CI): 9.5 ( ) 3-year OS Rate (95% CI): 21% (20 22%) Ipilimumab CENSORED Months Patients at Risk Ipilimumab Schadendorf D, et al. J Clin Oncol

93 CheckMate-141 Study Design: Phase III Trial of Nivolumab in Recurrent/Metastatic SCCHN Key Eligibility Criteria R/M SCCHN of the oral cavity, oropharynx, larynx, or hypopharynx ECOG PS 0 1 Not amenable to curative therapy Progression 6 months of last dose of platinum-based therapy Documentation of p16 to determine HPV status No active CNS metastases Stratification factor Prior cetuximab treatment R 2:1 Randomized 360/360 Nivolumab 3mg/kg IV Q2W Investigator s Choice Methotrexate 40mg/m² IV weekly Docetaxel 30mg/m² IV weekly Cetuximab 400mg/m² IV once, then 250mg/m² weekly Primary endpoint OS Other endpoints PFS ORR Safety DOR Biomarkers Quality of life Ferris RL, et al. N Engl J Med
94 Overall Survival Overall Survival (% of patients) 100 Ferris RL, et al. N Engl J Med Nivolumab Investigator s Choice Median OS, mo (95% CI) Nivolumab (n=240) 7.5 ( ) Investigator s Choice (n=121) 5.1 ( ) HR (97.73% CI) 0.70 ( ) 1-y OS 1-y Rate OS Rate (95% (95% CI) CI) 36.0% 36.0% ( ) ( ) 16.6% ( ) Months No. at Risk Nivolumab Investigator s Choice
95 Overall Survival (% of patients) Overall Survival By PD-L1 Expression PD-L1 Expression 1% PD-L1 Expression <1% Treatment Arm Median OS, mo (95% CI) HR (95% CI) Treatment Arm Median OS, mo (95% CI) HR (95% CI) Nivolumab (n=88) 8.7 ( ) Investigator s Choice (n=61) 4.6 ( ) 0.55 ( ) Nivolumab (n=73) 5.7 ( ) Investigator s Choice (n=38) 5.8 ( ) 0.89 ( ) Nivolumab Investigator s Choice Months Nivolumab Investigator s Choice No. at Risk Nivolumab Investigator s Choice Ferris RL, et al. N Engl J Med Nivolumab Investigator s Choice Nivolumab Investigator s Choice Months


96 CheckMate-067: Study Design Randomized, double-blind, phase III study to compare NIVO + IPI or NIVO alone to IPI alone Previously untreated, unresectable or metastatic melanoma N=945 Randomize 1:1:1 N=314 Stratify by: PD-L1 expression* BRAF status AJCC M Stage N=315 N=316 *Verified PD-L1 assay with 5% expression level was used for the stratification of patients; validated PD-L1 assay was used for efficacy analyses. **Patients could have been treated beyond progression under protocol-defined circumstances. NIVO 1 mg/kg + IPI 3 mg/kg Q3W x 4 then NIVO 3 mg/kg Q2W NIVO 3 mg/kg Q2W + IPImatched placebo IPI 3 mg/kg Q3W x4 + NIVO-matched placebo Treat until progression** or unacceptable toxicity Wolchok JD, et al. ASCO
97 Response to Treatment NIVO + IPI (N=314) NIVO (N=316) IPI (N=315) ORR, % (95% CI) 57.6 ( ) 43.7 ( ) 19 ( ) Two-sided P value vs IPI <.001 < Best Overall Response - % Complete Response Partial Response Stable Disease Progressive Disease Unknown Duration of Response (months) Median (95% CI) NR (13.1, NR) NR (11.7, NR) NR (6.9, NR) *By RECISTv1.1; NR, not reached Wolchok JD, et al. ASCO
98 PFS by PD-L1 Expression Level (1%) *Per validated PD-L1 immunohistochemical assay based on PD-L1 staining of tumor cells in a section of at least 100 evaluable tumor cells Wolchok JD, et al. ASCO
99 Safety Summary 67.5% of patients (81/120) who discontinued the NIVO + IPI due to treatmentrelated AEs developed a response Patients Reporting Event, % Treatment-related adverse event (AE) Treatment-related AE leading to discontinuation Treatment-related death* NIVO + IPI (N=313) NIVO (N=313) IPI (N=311) Any Grade Grade 3-4 Any Grade Grade 3-4 Any Grade Grade *One reported in the NIVO group (neutropenia) and one in the IPI group (cardiac arrest). Wolchok JD, et al. ASCO
100 CTLA4 + PD-1 Targeting in Lung Cancer: CheckMate-012 NIVO 3 mg/kg Q2W + IPI 1 mg/kg Q12W (N=38) NIVO 3 mg/kg Q2W + IPI 1 mg/kg Q6W (N=39) NIVO 3 mg/kg Q2W (N=52) Confirmed ORR, % (95% CI) 47 (31-64) 39 (23-55) 23 (13-37) Median Duration of Response, months (95% CI) Median Length of Follow-up, months (range) Best Overall Response, % NR (11.3, NR) NR (8.4, NR) NR (5.7, NR) 12.9 (0.9-18) 11.8 ( ) 14.3( ) Complete Response Partial Response Stable Disease Progressive Disease Unable to Determine Median PFS, months (95% CI) 8.1 ( ) 3.9 ( ) 3.6 (2.3, 6.6) 1-year OS rate, % (95% CI) NC 69 (52-81) 73 (59-83) Antonia SJ, et al. J Thorac Oncol. 2016; Hellmann MD, et al. Lancet Oncol NC= Not calculated (when >25% of patients are censored); NR= Not reached Combination data based on a February 2016 database lock, monotherapy data based on a March 2015 database lock except for OS data, which are based on an August 2015 database lock
101 Durvalumab (Anti PD-L1) + Tremelimumab (Anti CTLA-4) Trials in SCCHN Phase II HAWK Phase II CONDOR Setting 2L SCCHN post plat in R/M setting 2L SCCHN post plat in R/M setting Regimen PD-L1 status Rationale Durvalumab Durvalumab + Tremelimumab Durvalumab Tremelimumab + N=112 N=120 N=60^ N=60^ Accelerated approval of the Monotherapy in PD-L1+ Zandberg Accelerated approval of the Combination in PD-L1 Establishes individual component contribution to combination in PD-L1 Siu Phase III EAGLE 2L SCCHN post plat 1L pts who progressed within 6 mo of multimodal tx w/pt in the locally advanced setting Durvalumab + Tremelimumab Durvalumab SOC + N=100 + N=100 + N=100 N=140 N=Adaptive 140* N=140 Confirmatory trial Combination approval in all-comers Ferris and Licitra
 or refractory (EAGLE)")
102 Potential of IO Therapies: 1L Trials with IO/IO Combinations Primary Endpoints Phase III CheckMate 651 No prior systemic therapy, platinum sensitive Nivolumab + Ipilimumab SOC (EXTREME) PFS, OS Phase II CheckMate 714 No prior therapy, platinum sensitive/refractory Nivolumab + Ipilimumab Nivolumab ORR Phase III KESTREL EAGLE No prior CT/IO, platinumsensitive (KESTREL) or refractory (EAGLE) Durvalumab + Tremelimumab Durvalumab SOC (EXTREME) PFS, OS Phase III KEYNOTE-048 1L+ R/M No prior systemic therapy, platinum sensitive Pembrolizumab + Platinum/5-FU Pembrolizumab SOC (EXTREME) PFS, OS
103 Conclusions Immune checkpoint therapy, specifically anti-pd1 or -CTLA-4 monotherapy, improves survival in patients with metastatic cancers Several questions remain: Does combining two different checkpoint inhibitors add benefit? YES Do all patients benefit from combination therapy? NO Do we need to incorporate biomarkers for patient selection? YES Do we need to consider acute and chronic AE profile, and patient PS? YES



104 Emerging Concepts of Combined Immune Checkpoint Blockade
105 COUNTERPOINT: The Efficacy of CTLA-4 + PD-1 is NOT Superior to PD-1 Blockade Alone Joaquim Bellmunt, MD, PhD Associate Professor of Medicine Director, Bladder Cancer Center Dana-Farber Cancer Institute Boston, MA
106 PD-1 Blockade Alone CTLA-4 + PD-1 Slide courtesy of A. Ribas



107 PD-1 Blockade Alone Slide courtesy of A. Ribas CTLA-4 + PD-1 Matching the images using the ipi+nivo combo approach

108 Efficacy in 611 Patients in KEYNOTE 001 ORR: 33% ORR in previously untreated: 45% Pembrolizumab provided an ORR of 25% to 52% in the initial melanoma expansion cohorts of KEYNOTE-001, irrespective of dosing schedule or prior ipilimumab status. Ribas A, et al. JAMA Central radiology review by RECIST v1.1 Data as of October 18, 2014; median follow-up: 21 months
109 Pembrolizumab Treatment-related AEs with Incidence >5% Adverse Event, % Total N=411 Any Grade Grade 3/4 Fatigue 36 2 Pruritus 24 <1 Rash 20 <1 Diarrhea 16 <1 Arthralgia 16 0 Nausea 12 <1 Vitiligo 11 0 Asthenia 9 0 Cough 9 0 Similar safety profiles in IPI-N and IPI-T patients Analysis cut-off date: October 18, Adverse Event, n (%) Total N=411 Any Grade Grade 3/4 Myalgia 9 0 Headache 8 <1 Hypothyroidism 8 <1 Decreased appetite 7 <1 Dyspnea 7 <1 Chills 6 0 Pyrexia 6 0 ALT increased 5 <1 Total Ribas A, et al. JAMA. 2016
110 CheckMate-067: Study Design Randomized, double-blind, phase III study to compare NIVO + IPI or NIVO alone to IPI alone N=314 NIVO 1 mg/kg + IPI 3 mg/kg Q3W x 4 then NIVO 3 mg/kg Q2W Previously untreated, unresectable or metastatic melanoma N=945 Randomize 1:1:1 Stratify by: BRAF status AJCC M stage Tumor PD-L1 expression <5% vs 5%* N=316 NIVO 3 mg/kg Q2W + IPImatched placebo Treat until progression** or unacceptable toxicity N=315 IPI 3 mg/kg Q3W x4 + NIVO-matched placebo *Verified PD-L1 assay with 5% expression level was used for the stratification of patients; validated PD-L1 assay was used for efficacy analyses. **Patients could have been treated beyond progression under protocol-defined circumstances. Wolchok JD, et al. ASCO The study was not powered for a comparison between NIVO and NIVO+IPI
111 Overall Survival Results From a Phase III Trial of Nivolumab Combined with Ipilimumab in Treatment-naïve Patients with Advanced Melanoma CheckMate 067 NIVO+IPI and NIVO significantly improved OS and PFS vs. IPI alone in patients with untreated advanced melanoma In descriptive analyses, NIVO+IPI resulted in numerically higher OS, PFS and ORR vs. NIVO alone For NIVO+IPI, median DOR and time to subsequent therapy are still not reached Larkin J, et al. AACR Abstract CT075.
112 Dr. Larkin s Comments about KEYNOTE-067 The trial isn t combined vs. sequential Just combo vs. single agents with crossover outside the study Study not designed or powered for comparison between nivo monotherapy vs. combination Number of events at this first OS analysis less then anticipated 112
113 Combination ICI Safety Summary With an additional 19 months of follow-up, safety was consistent with the initial report NIVO+IPI (N=313) NIVO (N=313) IPI (N=311) Patients reporting event, % Any Grade Grade 3-4 Any Grade Grade 3-4 Any Grade Grade 3-4 Treatment-related adverse event (AE) Treatment-related AE leading to discontinuation Treatment-related death, n (%) 2 (0.6) a 1 (0.3) b 1 (0.3) b Most select AEs were managed and resolved within 3-4 weeks (85 100% across organ categories) ORR was 70.7% for pts who discontinued NIVO+IPI due to AEs, with median OS not reached a Cardiomyopathy (NIVO+IPI, n=1); Liver necrosis (NIVO+IPI, n=1). Both deaths occurred >100 days after the last treatment. b Neutropenia (NIVO, n=1); colon perforation (IPI, n=1). Larkin J, et al. New Engl J Med 2015.
114 Progression-Free Survival (Intent-to-Treat) In the randomized phase III KEYNOTE-006 study, pembrolizumab had fewer toxicities and significantly improved overall survival compared with ipilimumab. Robert C, et al. N Engl J Med Wolchok JD, et al. ASCO
115 Checkmate 016: Phase 1b Trial of Nivolumab + Ipilimumab in Metastatic RCC N=175* Key Eligibility Criteria Advanced or metastatic clear cell RCC KPS 80% No active CNS metastases Available tumor tissue (archival or recent acquisition) For NIVO3 + IPI1 and NIVO1 + IPI3 expansion arms and NIVO3 + IPI3 addition arm: Treatment naïve Stopped due to toxicity Nivolumab 3 mg/kg (IV) + ipilimumab 1 mg kg (IV) Q3W x 4 Nivolumab 1 mg/kg (IV) + ipilimumab 3 mg/kg (IV) Q3W x 4 Nivolumab 3 mg/kg (IV) + ipilimumab 3 mg/kg (IV) Q3W x 4 Nivolumab 3 mg/kg (IV) Q2W Primary Outcome Measures: Safety and tolerability Secondary Outcome Measures: ORR, DOR *Estimated study enrollment including arm that terminated due to toxicity. There are 47 patients continuing in each remaining arm. One prior adjuvant or neoadjuvant therapy for localized or locally advanced RCC is allowed provided recurrence occurred 6 months after the last dose of the adjuvant or neoadjuvant therapy. Only prior cytokine-based treatment for metastatic RCC (eg, interferon-alpha [IFN-α] or interleukin 2 [IL-2]) as prior therapy is allowed. AEs, SAEs, and laboratory abnormalities. By RECIST v NCT ; Hammers HJ, et al. Poster presentation at ESMO Abstract 1062P.
116 Overall Survival (Probability) Overall Survival of Nivolumab + Ipilimumab in Advanced/Metastatic RCC (Checkmate 016) Median OS, months (95% CI) NIVO3 + IPI1 NR NIVO1 + IPI (25.99 NR) Time (months) Number of patients at risk NIVO3 + IPI NIVO1 + IPI Adapted from Hammers HJ, et al. Poster presentation at ESMO Abstract 1062P.
117 In Select Nivo-treated Pts, Median Survival Not Reached; How Much Crossover After Nivo? Motzer RJ, et al. N Engl J Med Escudier B, et al. Eur Urol
118 Phase II Study of Front Line Therapy With Nivolumab and Salvage Nivolumab + Ipilimumab in Patients With Advanced Renal Cell Carcinoma. HCRN: GU Nivolumab 240 mg IV Q2W x 6 then initial disease assessment PR or CR Part A Continue nivolumab 360 mg IV Q3W until PD, toxicity or 84 weeks PD or 12 months Part B Re-induce nivolumab 3 mg/kg and ipilimumab 1 mg/kg Q3W x 4 (must complete by week 16) Toxicity that requires discontinuation of study drug or 84 weeks of treatment completed continue being followed per protocol PD Evaluate for Part B Nivolumab 360 mg Q3W starting week PR, CR or SD Continue nivolumab until PD, toxicity or 48 weeks PD Off study NCT
119 DANUBE (Durvalumab +/- Tremelimumab) in 1 st Line UBC Randomization Stratification Factors 1. Cisplatin eligibility (eligible vs. ineligible) 2. PD-L1 status (positive vs. negative) 3. Visceral metastasis (presence or absence; i.e., bone, lung or liver) TCC of the urothelium (renal pelvis, ureters, urinary bladder and urethra) Treatment-naïve patients Unresectable/stage IV NCT Randomization N=650 Estimated Timelines Estimated Completion: September 2019 Estimated Primary Data: March 2018 Durvalumab + tremelimumab N=217 Durvalumab Monotherapy N=217 SOC N=217 Primary Endpoints PFS & OS (Combo vs. SOC) Secondary Endpoints PFS & OS (Single agents vs. SOC) PFS (PD-L1+ and PD-L1-) OS (Combo vs. SOC) ORR (Combo vs. SOC) FACT-BL Immunogenicity PK (C max and C trough )
120 Checkmate 032: Phase 1/2 Trial of Nivolumab vs Nivolumab + Ipilimumab in muc: Overall Survival and Progression-Free Survival Overall Survival (Probability) Progression-Free Survival (Probability) Median OS, months (95% CI) Median PFS, months (95% CI) NIVO 3 + IPI ( ) NIVO 3 + IPI ( ) NIVO 1 + IPI (4.5 NR) NIVO 1 + IPI ( ) No. at risk NIVO 1 + IPI 3 NIVO 3 + IPI Time (months) No. at risk NIVO 1 + IPI 3 NIVO 3 + IPI Time (months) Median follow-up times for NIVO 3 + IPI 1 arm is 16.7 months, and NIVO 1 + IPI 3 arm is 7.8 months Diamonds are censored patients. Sharma P, et al. Oral presentation at SITC Abstract 449.
121 KEYNOTE-045 Study (NCT ) Overall Survival: Total 43.9% 30.7% Events, n HR (95% CI) P Pembro ( ).0022 Chemo 179 Pembrolizumab Chemotherapy Median (95% CI) 10.3 mo ( ) 7.4 mo ( ) No. at risk Bellmunt J, et al. N Engl J Med



122 Can We Select Patients More Likely to Respond to PD-1/L1 Blockade? 1. Pre-existing T cell infiltration and adaptive PD-L1 expression 2. TCR clonality 4. Mutational load Rizvi, et al. Science Le, et al. NEJM Tumeh, et al. Nature Herbst, et al. Nature Tumeh, et al. Nature IFN signature by expression profiling Nonresponder Responder Best Overall Response, RECISTv1.1 Ribas, et al. ASCO Transcriptome Hugo, et al. Cell
123 Conclusions PD-1/PD-L1 blockade therapy should be used as single agent in patients who have a chance of responding to this therapy Combination therapies with PD-1/PD-L1 blockade should only be used in patients with a low likelihood of a tumor response to single agent therapy


124 Should PD-1 blockade be used alone or in combination?
Debaters For The Evening:
 Your Debaters For The Evening: Current State of Immune Checkpoint Blockade in Selected Types of Solid Tumors Jeffery Weber, MD, PhD Naiyer A. Rizvi, MD Current State of ICI in Melanoma and Bladder Cancers
Your Debaters For The Evening: Current State of Immune Checkpoint Blockade in Selected Types of Solid Tumors Jeffery Weber, MD, PhD Naiyer A. Rizvi, MD Current State of ICI in Melanoma and Bladder Cancers
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER
 PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Non-Small Cell Lung Cancer Webinar. Thursday, September 13, p.m. EDT
 Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Immunoterapia di 1 linea Evidenze e Prospettive Future
 Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Alessandro Inno. IRCCS Ospedale Sacro Cuore Don Calabria Negrar, Verona
 GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
Immunotherapy for the Treatment of Kidney and Bladder Cancer
 Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Biomarkers for Cancer Immunotherapy Debate
 Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018
 Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer
 Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Media Release. Basel, 21 July 2017
 Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer
 Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Recent Advances in Lung Cancer: Updates from ASCO Updates from ESMO, AACR and ASCO
 Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal. Gabriela Sousa Oncologia Médica IPO Coimbra
 O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Índice. Melanoma Cáncer de Pulmón Otros tumores
 Índice Melanoma Cáncer de Pulmón Otros tumores Carcinoma de Vejiga Carcinoma de Células Renales Carcinoma de Cabeza y Cuello Carcinomas del tubo digestivo Cáncer de Mama MELANOMA CIRUGÍA CIRUGÍA + INFa
Índice Melanoma Cáncer de Pulmón Otros tumores Carcinoma de Vejiga Carcinoma de Células Renales Carcinoma de Cabeza y Cuello Carcinomas del tubo digestivo Cáncer de Mama MELANOMA CIRUGÍA CIRUGÍA + INFa
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Integrating Immunotherapy into Urologic Oncology: The New Urothelial Cancer Paradigm
 Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
IMMUNE CHECKPOINT BLOCKADE FOR NSCLC. Marina Chiara Garassino
 IMMUNE CHECKPOINT BLOCKADE FOR NSCLC Marina Chiara Garassino Cells of the Immune System Innate immune system: Involving proteins (chemokines and cytokines) and cells, is considered to be the first line
IMMUNE CHECKPOINT BLOCKADE FOR NSCLC Marina Chiara Garassino Cells of the Immune System Innate immune system: Involving proteins (chemokines and cytokines) and cells, is considered to be the first line
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The role of immune checkpoint inhibitors in non-small cell lung cancer
 Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
Histology independent indications in Oncology
 CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens