PD-L1 EXPRESSION IS CHARACTERISTIC OF A SUBSET OF AGGRESSIVE B-CELL LYMPHOMAS AND VIRUS-ASSOCIATED MALIGNANCIES
|
|
|
- Ursula Holmes
- 5 years ago
- Views:
Transcription
1 PD-L1 EXPRESSION IS CHARACTERISTIC OF A SUBSET OF AGGRESSIVE B-CELL LYMPHOMAS AND VIRUS-ASSOCIATED MALIGNANCIES Benjamin J Chen, MD, PhD 1, Bjoern Chapuy, MD, PhD 2, Jing Ouyang, PhD 2, Heather H Sun, BA 1, Margaretha GM Roemer, MS 2, Mina L Xu, MD 3, Hongbo Yu, MD, PhD 4, Christopher DM Fletcher, MD, FRCPath 1, Gordon J. Freeman, PhD 2, Margaret A Shipp, MD 2, and Scott J Rodig, MD, PhD 1 1 Department of Pathology, Brigham and Women's Hospital, Harvard Medical School, Boston, MA; 2 Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA; 3 Yale School of Medicine, New Haven, CT; and 4 Department of Pathology, UMass Memorial Medical Center, University of Massachusetts Medical School, Worcester, MA. Brief title: PD-L1 expression in B-cell lymphomas and virus-associated malignancies Corresponding author: Scott J. Rodig Department of Pathology Brigham and Women s Hospital 75 Francis Street Boston, MA Telephone: Fax: srodig@partners.org Conflicts of interest: GJF has patents and receives patent roylaties on the PD-1 pathway. There are no other conflicts of interest from the authors to disclose.
2 STATEMENT OF TRANSLATIONAL RELEVENCE Therapies targeting the immunomodulatory PD-1/PD-L1 signaling pathway promote marked anti-tumor immunity in a subset of patients with solid tumors. However, routine methods to detect PD-L1 expression in formalin-fixed paraffin embedded (FFPE) tissue biopsy sections are lacking. Herein, we validate novel immunohistochemical assays amenable to FFPE tissue sections and analyze a broad group of aggressive B-cell and virus-associated malignancies for PD-L1 protein expression. We find that upregulation of PD-L1 is a general feature of both the malignant cells and the non-malignant tumor infiltrating macrophages of classical Hodgkin lymphoma, primary mediastinal large B- cell lymphoma, T-cell/histiocyte-rich large B-cell lymphoma, and a broad group of virusand immunodeficiency-associated malignancies, including EBV-positive diffuse large B- cell lymphoma, post-transplant lymphoproliferative disorder, plasmablastic lymphoma, primary effusion lymphoma, and extranodal NK/T-cell lymphoma. In addition, we detected PD-L1 expression on the malignant cells of nearly all EBV-associated nasopharyngeal carcinomas. These results indicate that PD-L1 positive tumor cells and tumor-infiltrating macrophages likely contribute to immune evasion in multiple lymphoid and virus-associated malignancies and suggest that these tumors may be amenable to PD- 1 blockade. 2
3 ABSTRACT Purpose: Programmed death ligand 1 (PD-L1) is an immunomodulatory molecule expressed by antigen-presenting cells and select tumors that engage receptors on T cells to inhibit T-cell immunity. Immunotherapies targeting the PD-1/PD-L1 pathway have shown durable anti-tumor effects in a subset of patients with solid tumors. PD-L1 can be expressed by Reed-Sternberg cells comprising classical Hodgkin lymphoma (CHLs) and by malignant B cells comprising EBV-positive post-transplant lymphoproliferative disorders (PTLDs). We sought to determine whether the expression of PD-L1 represents a general strategy of immune evasion among aggressive B-cell lymphomas and virus- and immunodeficiency-associated tumors. Experimental Design: Using novel antibodies and formalin-fixed, paraffin-embedded (FFPE) tissue biopsies, we examined 237 primary tumors for expression of PD-L1. Results: Robust PD-L1 protein expression was found in the majority of nodular sclerosis and mixed cellularity CHL, primary mediastinal large B-cell lymphoma, T- cell/histiocyte-rich B-cell lymphoma, EBV-positive and -negative PTLD, and EBVassociated diffuse large B-cell lymphoma (DLBCL), plasmablastic lymphoma, extranodal NK/T cell lymphoma, nasopharyngeal carcinoma, and HHV8-associated primary effusion lymphoma. Within these tumors, PD-L1 was highly expressed by malignant cells and tumor-infiltrating macrophages. In contrast, neither the malignant nor the non-malignant cells comprising nodular lymphocyte-predominant Hodgkin lymphoma, DLBCL-not otherwise specified, Burkitt lymphoma, and HHV8-associated Kaposi sarcoma expressed detectable PD-L1. 3
4 Conclusion: Certain aggressive B-cell lymphomas and virus- and immunodeficiencyassociated malignancies associated with an ineffective T-cell immune response express PD-L1 on tumor cells and infiltrating macrophages. These results identify a group of neoplasms that should be considered for PD-1/PD-L1-directed therapies, and validate methods to detect PD-L1 in FFPE tissue biopsies. 4
5 INTRODUCTION Programmed cell death ligand 1 (PD-L1, also known as B7-H1) is an immunomodulatory cell-surface glycoprotein and a member of the B7 family of costimulatory molecules primarily expressed by antigen-presenting cells and that serve to regulate the cellular immune response. 1 Binding of PD-L1 to its cognate receptor PD-1 inhibits proliferation of activated T cells in peripheral tissues leading to "T-cell exhaustion," a functional phenotype that can be reversed by PD-1 blockade. 2 In clinical trials of anti-pd-1 and anti-pd-l1 antibodies, patients with solid tumors have achieved long-lasting clinical responses and thus emphasizing the importance of the PD-1/PD-L1 axis in regulating anti-tumor immunity. 3,4 Moreover, in the limited number of cases examined, clinical responsiveness to PD-1 blockade correlated with tumor-cell specific expression of PD-L1 as detected by immunohistochemistry (IHC) using a proprietary antibody. 4 We have shown that Hodgkin lymphoma cell lines express high levels of PD-L1 transcript and protein due to multiple mechanisms including genetic amplification of CD274 (encoding PD-L1) and constitutive AP1 signaling. Hodgkin cell lines show variable copy number gain of chromosome 9p24.1, a genomic region that includes CD274 (encoding PD-L1), PDCD1LG2 (encoding PD-L2), and JAK2. 5 The copy number of 9p24.1 correlates with cell surface PD-L1 protein expression due to direct amplification of CD274, and to increased JAK2 protein expression, enhanced JAK-STAT signaling, and activation of an interferon (IFN)-stimulated regulatory element/ifnregulatory factor 1 (ISRE/IRF1) motif in the CD274 promoter. 6,7 In a series of 5
6 genetically annotated primary classical Hodgkin lymphoma (CHL) cases, we found that high copy numbers of 9p24.1 correlated with increased PD-L1 expression in Reed- Sternberg (RS) cells. 5 We have further shown that: 1) PD-L1 expression is regulated by an AP1-dependent enhancer in CD274; 2) AP1 signaling components JunB/cJun constitutively bind this enhancer in Hodgkin lines; and 3) JunB and cjun are overexpressed in primary RS cells. 5 Moreover, a subset of CHL is Epstein-Barr virus (EBV)-positive and aberrant signaling through EBV-encoded gene products provides alternative mechanisms to upregulate PD- L1. In a genetically annotated series of primary CHL we found that 9p24.1 amplification and EBV-infection were mutually exclusive. Using EBV-transformed B cells, we demonstrated that the expression of the EBV-encoded latent membrane protein (LMP)-1 promotes both AP1-signaling and JAK-STAT signaling to activate the enhancer and promoter elements of CD274, respectively. 6 Consistent with these findings, we have detected PD-L1 in the majority of examined EBV-positive post-transplant lymphoproliferative disorders (PTLD). 6 Our studies indicate that CHL and EBV-positive PTLD utilize several complementary mechanisms to upregulate PD-L1 in tumor cells. CHL is also notable for its prominent inflammatory infiltrate which includes a skewed T- cell population and abundant macrophages. In CHL, increased numbers of CD68+ tumor-associated macrophages have been associated with inferior clinical outcome. 8,9 However, the biological basis for this association remains undefined. 6
7 CHL is genetically, phenotypically, and/or histologically related to additional large cell lymphomas including primary mediastinal large B-cell lymphoma (PMLBCL), nodular lymphocyte predominant Hodgkin lymphoma (NLPHL), and T-cell rich, histiocyte-rich large B-cell lymphoma (TCRLBCL). 10,11 Similarly, EBV and the closely related virus human herpes virus-8 (HHV8, also known as Kaposi sarcoma-associated herpesvirus) are postulated or known drivers of additional malignancies that include HIV/immunodeficiency-related diffuse large B-cell lymphoma (DLBCL), EBVassociated DLBCL of the elderly, extranodal NK/T cell lymphoma (ENKTCL), nasopharyngeal carcinoma (NPC), plasmablastic lymphoma (PBL), endemic Burkitt lymphoma (BL), and the HHV8-associated primary effusion lymphoma (PEL) and Kaposi sarcoma (KS). 12,13 A comprehensive analysis of PD-L1 expression in these tumor types has not been completed. In this study, we validate two novel anti-pd-l1 antibodies for the detection of PD-L1 protein in formalin-fixed, paraffin-embedded (FFPE) tissue sections. We then evaluate PD-L1 expression in a range of aggressive lymphoid malignancies, including those related to CHL and those associated with EBV and/or HHV8 infection, as well as NPC and KS. We find that robust expression of PD-L1 is characteristic of the malignant cells and a large proportion of non-malignant cells, primarily tumor infiltrating macrophages, within the tumor microenvironment of CHL, PMLBCL, TCRLBCL, and a broad range of virus- and immunodeficiency-associated malignancies that are characterized by an ineffective immune response. Our results further provide a biological basis for the prognostic significance of tumor-infiltrating macrophages. Finally, our methods establish 7
8 a template for screening FFPE tumor biopsies for PD-L1 expression by IHC using a generally available monoclonal antibody. 8
9 MATERIALS AND METHODS Case Selection Cases were retrieved from the surgical pathology files of Brigham and Women's Hospital, Boston, MA; Yale School of Medicine, New Haven CT; UMass Memorial Medical Center, Worcester, MA; and from the consult files of one of the authors (C.D.M.F.) with institutional review boards approvals. All tumors were diagnosed and classified according to standard WHO criteria. Representative hematoxylin and eosin stained slides were reviewed to confirm the presence of adequate amounts of tumor. Cases included whole tissue sections and tissue microarrays. Cases included nodular sclerosis CHL (NSCHL, 25 cases); mixed-cellularity CHL (MCCHL, 8 cases); CHL, not otherwise specified (CHL-NOS, 5 cases); nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL, 15 cases); primary mediastinal large B-cell lymphoma (PMBCL, 21 cases); T-cell/histiocyte-rich large B-cell lymphoma (TCHRBCL, 11 cases); EBVpositive DLBCL of the elderly (9 cases); EBV-positive immunodeficiency-related DLBCL (HIV-associated and iatrogenic; excluding patients with a history of solid organ transplantation, 7 cases); EBV-positive PTLD (10 cases); EBV-negative PTLD (7 cases); DLBCL, not otherwise specified (DLBCL-NOS, 66 cases); PBL (9 cases); PEL (4 cases); ENKTCL (6 cases); EBV-positive BL (7 cases); NPC (18 cases); KS (9 cases). All cases of EBV-positive DLBCL, EBV-positive PTLD, EBV-positive BL, NPC, 4 of 6 cases of ENKTCL, and 7 of 9 cases of PBL were shown previously to be positive for EBV-encoded RNA (EBER) by in situ hybridization study. All EBV-negative PTLD and 9
10 DLBCL-NOS cases were negative for EBER. All PEL and KS cases were shown previously to be positive for HHV8 by immunohistochemistry. Cell culture and Western blot Hodgkin lymphoma cell lines (L428, SUP-HD1, and HDLM2) and DLBCL cell lines (SUDHL4 and OCI-Ly1) were cultured as previously described. 14 Preparation of cell lysates, SDS-PAGE, and Western blot were performed as previously described 14 with the following antibody conditions: PD-L1 was detected with a rabbit monoclonal antibody (#10084-R015, 1:1500, 1 ug/ml final concentration, Sino Biological, Beijing, China) in 3% non-fat dry milk (sc-2325, Santa Cruz Biotechnologies, Santa Cruz, CA). Blots were stripped and reprobed with anti-gapdh antibody (FL-335, sc-25778, 1:2000, Santa Cruz) in 3% non-fat dry milk. Immunohistochemistry IHC using a rabbit anti-pd-l1 monoclonal antibody (clone 15, #10084-R015, 6.2ug/ml final concentration, Sino Biological, Beijing, China) was performed using 4-μm-thick, FFPE tissue sections on a Benchmark XT autostainer (Ventana Medical System, Tuscon, AZ) with standard antigen retrieval methods (CC1 buffer, ph8.0, # , Ventana). UltraView Universal DAB Detection kit (# , Ventana) was used according to the manufacturer s instructions. Counterstaining was performed as part of the automated staining protocol using hematoxylin (# , Ventana). IHC using the mouse anti- PD-L1 monoclonal antibody (IgG1, generated in the laboratory of G. Freeman, clone 339.7G11, 69 ug/ml final concentration) was performed using the same protocol as 10
11 above. After staining, slides were then washed in soap water and distilled water, dehydrated in graded alcohol and xylene, mounted and coverslipped. The protocols for double IHC staining are available in Supplementary Methods. Case Evaluation All IHC stained sections were initially evaluated and scored by a hematopathologist (BJC). The same slides and the original scores were then reviewed by a second hematopathologist (SJR) for concordance of interpretation. Discrepancies in interpretation or scoring (<10% of cases) were resolved by consensus conference between the two pathologists. Twenty samples, representing both PD-L1-positive and negative staining cases, were evaluated with the rabbit and the mouse monoclonal antibodies, including EBV+ PTLD, EBV- PTLD, EBV+ DLBCL, EBV+ Burkitt lymphoma, nasopharyngeal carcinoma, and CHL. No significant differences in staining of the malignant or non-malignant cells were observed among the cases tested with both antibodies. Only tumors stained with the rabbit antibody were formally scored (for the graphical representations Figure 3, and Figure 4 D-F) because: 1) this antibody is commercially available, whereas the mouse antibody is a proprietary antibody; and 2) limited material for some cases precluded staining of the complete set of cases with the mouse antibody. For cases stained with the rabbit anti-pd-l1 antibody, the percentage of tumor cells present in tissue sections was estimated for each case. The percentage of the total cellularity staining for rabbit anti-pd-l1, including malignant and non-malignant cells, 11
12 and the percentage of the tumor cell population staining for PD-L1 were scored independently. Staining intensity was scored as follows: 0 (no staining), 1+ (weak or equivocal staining), 2+ (moderate staining), or 3+ (strong staining). Cases with membrane staining, with or without cytoplasmic staining, and cases with only cytoplasmic staining were tabulated separately. Cytoplasmic cellular staining had to unequivocally exceed background to be considered positive. Tumor staining for PD-L1 was considered positive if >5% of the tumor cell population showed 2+ or 3+ membrane staining. A case was considered to have a microenvironment positive for PD-L1 if >20% of the total tissue cellularity showed 2+ or 3+ membrane or cytoplasmic staining in malignant and/or non-malignant cells. The threshold for positive PD-L1 staining in malignant cells used here is comparable to that used in prior publications, using a distinct antibody. 4,15,16 Appropriate external positive (placenta) and negative (tonsil) controls were also included with each staining run. 12
13 RESULTS Validation of PD-L1 antibodies for IHC. After testing a variety of commercially available antibodies, we identified a rabbit monoclonal antibody that demonstrated both sensitive and specific staining for PD-L1 on a set of well-characterized cell lines and tissues (Figure 1, Materials and Methods). In addition, we validated a novel mouse monoclonal antibody (clone 339.7G11, Materials and Methods) recognizing PD-L1 that was generated by one of the co-authors on this study (GF, data not shown). By western blot analysis (Figure 1A), the rabbit anti-pd-l1 monoclonal antibody recognized a protein of ~55 kda the size of glycosylated PD- L1 in lysates derived from Hodgkin cell lines (L428, SUP-HD1, HDLM2). The relative amount of PD-L1 in the Hodgkin cell lines as detected by western blot analysis was consistent with previously reported levels of PD-L1 expression detected by flow cytometry, and also correlated with chromosome 9p24 copy number status. 5 Importantly, no band was detected in lysates derived from DLBCL cell lines (SUDHL4, OCI-Ly1), consistent with the previously reported lack of detectable PD-L1 in these lines (Figure 1A). 5 Similarly, IHC analysis of FFPE cell pellets using the rabbit monoclonal antibody revealed robust staining of the Hodgkin cell line HDLM2 in a strong membranous pattern (Figure 1B) but not in the DLBCL line SUDHL4 (Figure 1C). The staining pattern was identical using the mouse monoclonal antibody (Figures 1B and 1C insets). Additional IHC analysis of transfected cell lines showed specific staining by both rabbit and mouse PD-L1 antibodies of cell lines expressing human PD-L1 but not human PD-L2 (data not 13
14 shown). We conclude that IHC analysis using both the rabbit and mouse monoclonal antibodies is specific for PD-L1 protein. IHC analysis of human tonsil revealed little to no specific staining of the vast majority of lymphocytes within the interfollicular T cell-rich regions and in the B cell-rich secondary follicles using the rabbit monoclonal PD-L1 antibody (Figure 1D). Rare lymphoid cells within reactive germinal centers did show weak membranous staining. High-power examination of human tonsil also revealed distinct membranous staining of the tonsilar epithelium and weak, membranous staining of scattered cells morphologically consistent with macrophages (Figure 1D inset). 1,16 IHC analysis of tonsil using the mouse monoclonal PD-L1 antibody resulted in identical findings (Supplemental Figure S1). As an external positive control, syncytiotrophoblasts in human placental tissue demonstrated strong membranous expression of PD-L1, as described previously (Supplemental Figure S1). 1 We noted that with the rabbit monoclonal antibody, a mild degree of general, nonspecific background staining was observed in tissue sections. Background staining varied according to the degree of dilution necessary to achieve the final antibody concentration optimized for IHC (Supplemental Figure S1). Less background was associated with the more concentrated lots of antibody (6.2 ug/ml final concentration used; lot concentrations ranged from 0.22 to 1.55 mg/ml). Very little background was noted with the mouse monoclonal antibody (Supplemental Figure S1; S2). 14
15 Expression of PD-L1 in HL and variants. Upon validation of two novel antibodies directed against PD-L1, we next surveyed a large cohort of Hodgkin lymphomas, including NSCHL, MCCHL, CHL-NOS, and NLPHL for PD-L1 expression by IHC. Tissue sections were comprised of a varying amount of RS cells. The median estimated percent malignant cells was 5% (range 2-20%) for NSCHL, 2% (range 2-10%) for MCCHL, 50% (range 2-90%) for CHL-NOS, and 2% (range 2-5%) for NLPHL. Twenty-one of 25 (84%) cases of NSCHL, 7/8 (88%) cases of MCCHL, and 5/5 (100%) cases of CHL-NOS showed strong (2+ or 3+) membranous staining of the RS cells (Figure 2A, Table 1, Supplemental Table S1). Of the 33 cases of CHL showing positive staining in malignant cells, 32 cases (97%) had at least 50% of the RS cells positive for PD-L1 and 27 cases (82%) had at least 90% of the RS cells positive for PD-L1 (Supplemental Table S1, Figure 3A). By contrast, only two cases of NLPHL (13%) were scored as positive for PD-L1 with only 5% of the LP cells positive in each case (Figure 2B and 3C, Supplemental Table S1). Whereas the RS cells comprised a relatively small proportion of the overall tumor cellularity in CHL cases, non-malignant cells predominantly tissue macrophages contributed to the total tumor cellularity and consistently demonstrated strong membranous staining for PD-L1 (Supplemental Table S1). We found that 19/25 (76%) cases of NSCHL, 7/8 (88%) cases of MCCHL, and 5/5 (100%) cases of CHL-NOS showed strong (2+ or 3+) membranous and/or cytoplasmic staining for PD-L1 in at least 20% of the total tumor cellularity, including non-malignant cells (Figure 3B, Supplemental Table S1). Double immunostaining for PD-L1 and CD68 on a set of cases 15
16 confirmed this analysis and revealed strong membranous PD-L1 staining of CD68+ macrophages in close proximity to PD-L1 positive RS cells (Figure 2A inset). Only one case of NLPHL (7%) showed PD-L1 positive staining in 20% of the total tumor cellularity. However, malignant cells in this case were estimated to comprise 5% of the cellularity and only rare LP cells (~2%) were positive for PD-L1 (Figure 3C and 3D, Supplemental Table S1). Overall, the expression of PD-L1 on the malignant tumor cells was well correlated with the expression of PD-L1 on the tumor infiltrating CD68+ macrophages in individual tumors (Supplemental Table S3). We have previously shown that EBV-encoded LMP1 can promote PD-L1 expression in tumor cells. 6 Therefore, we looked to see if the EBV status of the Hodgkin lymphoma cases correlated with PD-L1 expression. Eleven of 12 (92%) cases of Hodgkin lymphoma that were positive for EBV showed strong (2+ or 3+) membranous PD-L1 staining in malignant RS cells. One case of EBV-positive NSCHL showed weak (1+) membranous staining in 90% of RS cells (Supplemental Table S1). Twenty of 29 (69%) Hodgkin lymphoma cases that were negative for EBV had malignant cells that scored positive for PD-L1 (Supplemental Table S1). Overall, EBV status did not predict a presence or absence of PD-L1 expression in Hodgkin lymphoma. Two entities that lie on the histologic and genetic spectrum with CHL and NLPHL are PMBCL and TCHRBCL. Strong membranous PD-L1 expression was observed in 15/21 (71%) cases of PMBCL (90% median percent malignant cells, Figure 2C) and 10/11 (91%) cases of TCHRBCL (10% median percent malignant cells, Figure 2D). Double 16
17 immunostaining for PD-L1 and PAX5 in cases of TCHRBCL demonstrated strong membranous PD-L1 staining of the scattered, PAX5-positive malignant B-cells (Figure 2D inset). PAX5-negative cells, consistent with macrophages, adjacent to the malignant B-cells also demonstrated strong PD-L1 staining. The patterns of PD-L1 expression observed using the rabbit monoclonal antibody was identical using the mouse monoclonal antibody for IHC (Supplemental Figure S2, data not shown). Expression of PD-L1 in EBV- and HHV8-positive malignancies. Previously we reported a small series of EBV-positive PTLD cases that express PD-L1. 6 Using our newly characterized PD-L1 antibodies, we extended our analysis to include additional aggressive EBV-positive and -negative B-cell lymphomas (Table 1). All EBV-positive DLBCLs, including 9/9 (100%) EBV-positive DLBCLs of the elderly and 7/7 (100%) EBV-positive immunodeficiency-related DLBCLs, demonstrated strong PD- L1 membrane staining (Figure 4A). The percentages of malignant cells staining positive for PD-L1 ranged from 5-90%, with 7 of 16 EBV-positive DLBCLs having at least 60% PD-L1-positive cells (Supplemental Table S2). Six of 10 (60%) EBV-positive PTLD cases demonstrated strong PD-L1 membrane staining on at least 80% of malignant cells, consistent with our previous study (data not shown). 6 Four of 7 (57%) EBV-negative PTLD cases also showed strong membranous PD-L1 tumor staining (Figure 4B). By contrast, only 7/66 (11%) EBV-negative DLBCL-NOS cases showed strong membranous PD-L1 tumor staining (range 10-90% of malignant cells) (Figure 4C). An additional 2 cases showed PD-L1 expression among the tumor infiltrating macrophages 17
18 (Table 1). The median tumor composition for all of the DLBCL categories ranged from 70-90%. A review of the clinical, pathological and molecular characteristics of the cases (14%) that scored as PD-L1 positive revealed that, of the 8 cases with available data, 7 cases were activated B-cell (ABC) type and 1 case was germinal center B-cell (GCB) type by the cell of origin (COO) classification scheme. In comparison to all DLBCL-NOS cases for which both the PD-L1 and COO status was known (61 cases total, 27 cases ABCtype, 23 cases GCB-type; 11 cases Type 3), the association between PD-L1 expression and the ABC-subtype was statistically significant (p=0.04, Fisher's exact test). PD-L1 expression on the variable numbers of non-malignant cells in EBV-positive DLBCL and other lymphomas consisted primarily of tumor-infiltrating macrophages (Figures 4D-F, Supplemental Table S2). Careful morphologic review and double immunostaining for CD68 or PAX5 and PD-L1 (e. g. Figure 4A and 4B insets) were used to support our histologic assessment. As for the Hodgkin lymphomas, expression of PD- L1 by malignant cells and non-malignant tumor infiltrating macrophages was correlated (Supplemental Table S3). Analysis of additional EBV- and HHV8-positive malignancies showed that 4/9 (44%) PBL, 2/4 (50%) PEL, 4/6 (67%) ENKTCL, 16/18 (89%) NPC cases showed positive PD- L1 staining in malignant cells (Figure 5, Table 1, Supplemental Table S2). The majority of cases had greater than 50% malignant cells positive for PD-L1 and all cases in this 18
19 group had at least 10% malignant cells positive for PD-L1. By contrast, no cases of EBV-positive BL or HHV8-positive KS were positive for PD-L1 (Figure 5, Table 1). For cases with available tissue, we confirmed the patterns of PD-L1 expression obtained using the rabbit monoclonal antibody with those using the mouse monoclonal antibody. We observed no differences in tumor staining between these two reagents (Figure 5D and 5E insets; Supplemental Figure S2). For the majority of tumors showing positive staining, the PD-L1 expression was distinctly membranous. However, in a few cases (2 NSCHL, 1 MCCHL, 4 PMBCL, 1 EBV-positive PTLD, 2 EBV-negative PTLD, 6 DLBCL-NOS, 1 PEL, 1 ENKTCL, and 2 KS), we observed cytoplasmic staining that unequivocally exceeded background (in at least 5% tumor cells) but with little to no distinct staining of cell membranes (Figure 4D- F, cases designated in graphs by *, Supplemental Table S2). Although this pattern was observed with both anti-pd-l1 antibodies, it is unclear whether such staining represents exclusively cytoplasmic PD-L1 expression, or both cytoplasmic and low-level membrane expression. In total, we observed robust PD-L1 expression by the malignant cells and tumor infiltrating macrophages in the majority of CHL, regardless of subtype and EBV-status, PMLBCL, TCRLBCL, EBV+ DLBCL, EBV+ and EBV- PTLD, HHV8+ PEL, and EBV+ NPC. We observed that nearly one-half of PBL and ENKTCL expressed PD-L1 19
20 as well. In contrast, only rare cases of NLPHL, DLBCL NOS, BL and no cases of KS expressed significantly detectable PD-L1 protein. 20
21 DISCUSSION EBV-associated DLBCL, PTLD, ENKTCL, PBL, NPC, and HHV8-associated PEL are rare, but often aggressive, malignancies that are largely resistant to current chemotherapeutic regimens Given their association with oncogenic viruses and with immunodeficiency, these tumors are attractive targets for immune-based therapies. Several novel immunomodulatory agents have shown great promise in clinical trials involving patients with advanced solid tumors, especially those using human antibodies directed against critical immune checkpoint molecules. Specifically, anti-pd-1 and anti- PD-L1 directed therapies have resulted in durable clinical responses in patients with nonsmall cell lung cancer, renal cell cancer and melanoma. 3,4 Furthermore, expression of PD-L1 in a subset of tumors appeared to correlate with treatment response. 4 However the efficacy of such immune targeted therapies in virus- and immunodeficiency-related malignancies has not been tested. Moreover, there remains a need for reliable methods to identify the critical immunoregulatory molecules expressed by individual tumors to improve patient selection. In this study, we validated two novel anti-pd-l1 antibodies, one of which is commercially available, and demonstrated robust PD-L1 expression in the majority of CHL/NSCHL, MCCHL, PMBCL, TCHRBCL, EBV-positive DLBCL of the immunocompromised and elderly, PTLD, NPC, and ENKTCL. A subset of PBL and PEL cases revealed unequivocal PD-L1 expression, as well. These results establish PD- L1 expression as a common feature in these malignancies, which include both viral- and 21
22 immunodeficiency-associated tumors, and provide a clinically-applicable method for screening FFPE tumor samples on a routine basis. In this analysis, we used a threshold of 5% positive staining of malignant cells to determine whether the tumors were scored as positive or negative for PD-L1. This threshold was selected to conform to the cut-point used in previous publications. 4,15,16 With this threshold, an association between cases scoring as positive for PD-L1 expression and clinical responsiveness to PD-1 immunotherapy in a small subset of cases has been reported. 4 However the antibody used to detect PD-L1 expression in that publication is distinct from those used here (and is not commercially available). The biological significance of a threshold of 5% positive staining remains poorly defined and deserves further investigation in future clinical trials. Moreover, given this uncertainty, we chose to present data showing the percentage of the malignant cells and the percentage of total cells within the tumor biopsy that are positive for PD-L1 expression for each case. We found that cases scored as PD-L1-positive generally expressed PD-L1 in far excess of 5% of the malignant tumor cells (Figures 3A, 3C; Figure 4D-F, Supplemental Table S1). PD-L1 expression is often driven by intrinsic genetic aberrations and disregulated signaling pathways within malignant cells. We have shown that RS cells of up to 40% of NSCHLs harbor amplification of 9p24.1, a genomic region that includes CD274, PDCD1LG2 (encoding PD-L2), and JAK2. 5 In cell lines, increased 9p24 copy number is associated with increased PD-L1 expression due to both direct amplification of CD274, 22
23 and through increased JAK2 and enhanced JAK-STAT signaling. 6,7 Additional, intrinsic mechanisms driving PD-L1 expression in the RS cells of CHL include EBV infection (32% of all CHL cases in this series) and constitutive AP1 activity. Similarly, approximately 70% of primary PMLBCLs also show gains in 9p24.1, 5 and thus the robust PD-L1 protein expression we observe in the majority of PMLBCLs is likely attributable, in part, to this genetic lesion. Taken together, the percentage of CHL and PMLBCL with membranous PD-L1 on the malignant cells (87% and 71%, respectively) is consistent with these prior findings. We have shown that EBV-transformed human B-cell lines (lymphoblastoid cell lines, LCLs) and EBV-positive PTLDs upregulate PD-L1. The results in the current study both confirm the PD-L1 protein expression by EBV-positive PTLDs using newly available, more robust antibodies and establish that the majority of additional EBV-associated malignancies express PD-L1, with the exception of BL. In LCLs, PD-L1 induction is dependent upon constitutive signaling through the EBVencoded protein LMP1 via its effects on both the PD-L1 enhancer and promoter. 6 In both LCLs and EBV-positive PTLDs, EBV maintains a type III latency program characterized by expression of LMP1 in addition to LMP2A, the nuclear proteins EBNA-1, -2,- 3 and - LP, and a series of non-coding RNAs (EBERs). 7,12,17 Similarly, in EBV-positive CHL, EBV maintains a type II latency program that is characterized by expression of LMP1, LMP2A, EBNA1, and EBERs. 23 In EBV-positive DLBCL, the virus maintains type II or type III latency program, 24 and suggesting that LMP1-mediated signaling is likely to 23
24 directly contribute to tumorigenesis and to the immune evasion signature for these tumors. In contrast, the virus in endemic BL resembles that of quiescent, EBV-infected memory B cells in immunocompetent hosts and is characterized by a minimal gene expression program that includes EBNA1 and EBERs, but not LMP1. 25 Consistent with a lack of signaling by EBV-encoded proteins in this tumor type, we found BL to be consistently negative for PD-L1. The EBV-encoded proteins, including LMP1, seem to be more heterogeneously expressed in ENKTCL and PBL than in EBV-positive PTLD, CHL, and DLBCL. 12,20,26 Therefore, the direct contribution of EBV-dependent and independent signaling pathways to the immune signature will require further analyses using cell culture models of these tumor types. Similarly, the contribution of viral-mediated signaling to expression of PD-L1 by NPC and PEL remains undefined. Surprisingly, we observed robust PD-L1 protein expression in EBV-negative PTLD. Very little is known about this tumor type, which comprises up to 30% of post-transplant lymphoproliferative disorders. 27,28 Because patients with these tumors can still respond to a reduction in immunosuppression, there is a likely role for immune surveillance in preventing or eradicating these tumors. In our cohort, EBV-negative PTLD was similar to EBV-positive PTLD in expressing PD-L1. Because we have shown that PD-L1 can be upregulated by mechanisms independently of viral-encoded gene products in EBVnegative CHL, we suggest that this tumor type is a good candidate for further genetic studies of the CD274 locus. 24
25 Only rare cases of DLBCL-NOS were positive for PD-L1, either in the malignant tumor cells or the tumor infiltrating macrophages. We have data as to the cell of origin for only a subset of the DLBCL-NOS cases (61 cases) and found that 7 of 8 cases positive for PD- L1 expression in either the malignant B cells or the tumor infiltrating macrophages are classified as activated B-cell (ABC) type. This enrichment is statistically significant (p=0.04, Fisher's exact test), although the total number of positive staining cases is very small. Other characteristics, including sites of disease involvement and age, were not associated with PD-L1 expression (data not shown). Given that patients with ABC-type DLBCL show inferior clinical outcome when treated with standard chemotherapy (R- CHOP), it will be of interest to determine whether PD-L1 expression, although rare in DLBCL-NOS, correlates with the cell of origin and clinical outcome using larger case series that are molecularly defined and with clinical follow-up. Given the multiple, intrinsic mechanisms malignant cells exploit to upregulate PD-L1, an important additional result of this study is the recognition that non-malignant cells, especially tissue macrophages, contribute to the PD-L1 expression in certain aggressive B-cell, immunodeficiency-related, and viral-related malignancies. In this regard, these tumors resemble a subset of T-cell lymphoproliferative disorders in which PD-L1 expression on dendritic cells can functionally inhibit T-cell proliferation. 29 We find that the intensity of PD-L1 expression in macrophages varies from absent to weak in normal tonsil and in tumors with little PD-L1 expression in malignant cells, such as NLPHL, DLBCL-NOS, and BL, to moderate and often, very strong in PD-L1-positive tumors. For several tumor types, especially CHL and other tumors with a marked inflammatory 25
26 infiltrate, a major component of the PD-L1 expression within the total tumor cellularity is derived from the tumor-infiltrating macrophages. Overall, we found a high correlation between PD-L1 expression by the malignant cells and by the non-malignant cells within an individual tumor, regardless of tumor type, and suggests coordinate regulation of PD- L1 among malignant and tumor infiltrating macrophages (Supplemental Table S3). Recently, it has been recognized that the number of tumor infiltrating macrophages in cases of CHL constitute a biomarker of inferior failure free survival and overall survival CHL. 8,9 Several studies have since confirmed this observation However, the biological basis for this association has remained undefined. PD-L1, as a major ligand for PD-1, serves to suppress T-cell immunity- including immunity directed towards virally-encoded antigens expressed in EBV-positive CHL. 6 Thus the observation that macrophages constitute a major source of PD-L1 in the tumor microenvironment of CHL suggests a critical role for the PD-1/PD-L1 signaling axis among cases of CHL with high numbers of tumor infiltrating macrophages and an inferior clinical outcome through the suppression of anti-tumor immunity. The mechanisms responsible for the recruitment of macrophages to individual tumors and the origin of PD-L1 upregulation on these cells require further definition. Cytokines, such as interferon-gamma, can upregulate PD-L1 on macrophages, potentially via the ISRE/IRF1 motif in the CD274 promoter. 5,34 Given the cytokine-rich inflammatory microenvironment of CHL, TCRLBCL, and additional viral-associated lymphomas, secreted immunomodulatory factors may be responsible for the upregulation of PD-L1 on 26
27 tumor-infiltrating macrophages in these diseases. Of note, we also observed high PD-L1 expression on the tumor-infiltrating macrophages in tumors, such as EBV-positive DLBCL and EBV-positive and -negative PTLD, in which the cytokine milieu is not well described. Further studies correlating the cytokine profiles of the tumor microenvironment and the relative expression of PD-L1 are needed. Given our development and validation of novel reagents for the detection of PD-L1 protein in FFPE tissue sections, it will be of interest to more broadly survey expression of this protein in additional hematological and non-hematological malignancies. Others have noted that PD-L1 is expressed by a subset of T-cell lymphoproliferative disorders, especially those at cutaneous sites. 29 In contrast, low grade B-cell lymphoproliferative disorders are thought to rarely express PD-L1. 35 Given our finding that PD-L1 expression can be limited to discrete and rare tumor types, it will be important to establish a comprehensive survey of hematological neoplasms based on detailed pathological classification. Moreover, it will be of interest to survey additional virusassociated malignancies. A very recent publication detailing the expression of PD-L1 in the tumor associated macrophages of human papillomavirus (HPV)-positive squamous cell carcinoma of the head and neck suggests targeting PD-1/PD-L1 signaling in HPV associated tumors. 36 Investigations of PD-L1 expression in HPV-positive cervical carcinoma, polyomavirus-positive Merkel cell carcinoma, and HCV-positive hepatocellular carcinoma are warranted. 27
28 The EBV-, HHV8-, and immunodeficiency-associated malignancies are uncommon but often aggressive, life-threatening neoplasms with limited treatment options. Our data indicate that PD-L1 expression is a common feature of these tumors. Among these tumors, EBV-positive DLBCL of the elderly is associated with a particularly dismal prognosis with a median survival of 2 years. 22 As this patient population is characterized by co-morbidities that complicate the use of standard chemotherapy, it is likely to be an ideal candidate for novel therapies that enhance anti-tumor immune responses. Although it will be important to interrogate larger tumor cohorts to confirm our findings, we suggest that clinical trials targeting PD-1 and PD-L1 may benefit patients with CHL, PMLBCL, TCHRBCL, EBV-positive DLBCL, PTLD, ENKTCL, PBL, PEL, and NPC may be appropriate candidates for clinical trials targeting the PD-1 pathway. 28
29 ACKNOWLEDGEMENTS This work was supported, in part, by R01 CA (to MAS), a Specialized Center of Research (SCOR) grant from the Leukemia and Lymphoma Society (MAS; SJR), and NIH grants AI56299, AI080192, and U54CA (to GJF). 29
30 REFERENCES 1. Keir ME, Butte MJ, Freeman GJ, Sharpe AH. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008;26: Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exp Med. 2000;192: Brahmer JR, Tykodi SS, Chow LQM, Hwu W-J, Topalian SL, Hwu P, et al. Safety and activity of anti-pd-l1 antibody in patients with advanced cancer. N Engl J Med. 2012;366: Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, et al. Safety, activity, and immune correlates of anti-pd-1 antibody in cancer. N Engl J Med. 2012;366: Green MR, Monti S, Rodig SJ, Juszczynski P, Currie T, O Donnell E, et al. Integrative analysis reveals selective 9p24.1 amplification, increased PD-1 ligand expression, and further induction via JAK2 in nodular sclerosing Hodgkin lymphoma and primary mediastinal large B-cell lymphoma. Blood. 2010;116: Green MR, Rodig S, Juszczynski P, Ouyang J, Sinha P, O Donnell E, et al. Constitutive AP-1 activity and EBV infection induce PD-L1 in Hodgkin lymphomas and posttransplant lymphoproliferative disorders: implications for targeted therapy. Clin Cancer Res. 2012;18: Marzec M, Zhang Q, Goradia A, Raghunath PN, Liu X, Paessler M, et al. Oncogenic kinase NPM/ALK induces through STAT3 expression of immunosuppressive protein CD274 (PD-L1, B7-H1). Proc Natl Acad Sci USA. 2008;105: Tan KL, Scott DW, Hong F, Kahl BS, Fisher RI, Bartlett NL, et al. Tumor-associated macrophages predict inferior outcomes in classic Hodgkin lymphoma: a correlative study from the E2496 Intergroup trial. Blood. 2012;120: Steidl C, Lee T, Shah SP, Farinha P, Han G, Nayar T, et al. Tumor-Associated Macrophages and Survival in Classic Hodgkin s Lymphoma. New England Journal of Medicine. 2010;362: Savage KJ, Monti S, Kutok JL, Cattoretti G, Neuberg D, De Leval L, et al. The molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lymphomas and shares features with classical Hodgkin lymphoma. Blood. 2003;102: Harris NL. Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: differential diagnosis and biological implications. Mod Pathol. 2013;26 Suppl 1:S
31 12. Kutok JL, Wang F. Spectrum of Epstein-Barr virus-associated diseases. Annu Rev Pathol. 2006;1: Taylor GS, Blackbourn DJ. Infectious agents in human cancers: lessons in immunity and immunomodulation from gammaherpesviruses EBV and KSHV. Cancer Lett. 2011;305: Juszczynski P, Ouyang J, Monti S, Rodig SJ, Takeyama K, Abramson J, et al. The AP1-dependent secretion of galectin-1 by Reed Sternberg cells fosters immune privilege in classical Hodgkin lymphoma. Proc Natl Acad Sci USA. 2007;104: Taube JM, Anders RA, Young GD, Xu H, Sharma R, McMiller TL, et al. Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med. 2012;4:127ra Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, et al. Tumorassociated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med. 2002;8: Knecht H, Berger C, Rothenberger S, Odermatt BF, Brousset P. The role of Epstein- Barr virus in neoplastic transformation. Oncology. 2001;60: Perri F, Bosso D, Buonerba C, Lorenzo GD, Scarpati GDV. Locally advanced nasopharyngeal carcinoma: Current and emerging treatment strategies. World J Clin Oncol. 2011;2: Nador RG, Cesarman E, Chadburn A, Dawson DB, Ansari MQ, Sald J, et al. Primary effusion lymphoma: a distinct clinicopathologic entity associated with the Kaposi s sarcoma-associated herpes virus. Blood. 1996;88: Delecluse HJ, Anagnostopoulos I, Dallenbach F, Hummel M, Marafioti T, Schneider U, et al. Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood. 1997;89: Chan JK, Sin VC, Wong KF, Ng CS, Tsang WY, Chan CH, et al. Nonnasal lymphoma expressing the natural killer cell marker CD56: a clinicopathologic study of 49 cases of an uncommon aggressive neoplasm. Blood. 1997;89: Oyama T, Yamamoto K, Asano N, Oshiro A, Suzuki R, Kagami Y, et al. Age-related EBV-associated B-cell lymphoproliferative disorders constitute a distinct clinicopathologic group: a study of 96 patients. Clin Cancer Res. 2007;13: Herbst H, Dallenbach F, Hummel M, Niedobitek G, Pileri S, Müller-Lantzsch N, et al. Epstein-Barr virus latent membrane protein expression in Hodgkin and Reed- Sternberg cells. Proc Natl Acad Sci USA. 1991;88:
32 24. Hamilton-Dutoit SJ, Rea D, Raphael M, Sandvej K, Delecluse HJ, Gisselbrecht C, et al. Epstein-Barr virus-latent gene expression and tumor cell phenotype in acquired immunodeficiency syndrome-related non-hodgkin s lymphoma. Correlation of lymphoma phenotype with three distinct patterns of viral latency. Am J Pathol. 1993;143: Vereide DT, Sugden B. Lymphomas differ in their dependence on Epstein-Barr virus. Blood. 2011;117: Elenitoba-Johnson KS, Zarate-Osorno A, Meneses A, Krenacs L, Kingma DW, Raffeld M, et al. Cytotoxic granular protein expression, Epstein-Barr virus strain type, and latent membrane protein-1 oncogene deletions in nasal T- lymphocyte/natural killer cell lymphomas from Mexico. Mod Pathol. 1998;11: Nelson BP, Nalesnik MA, Bahler DW, Locker J, Fung JJ, Swerdlow SH. Epstein- Barr virus-negative post-transplant lymphoproliferative disorders: a distinct entity? Am J Surg Pathol. 2000;24: Leblond V, Davi F, Charlotte F, Dorent R, Bitker MO, Sutton L, et al. Posttransplant lymphoproliferative disorders not associated with Epstein-Barr virus: a distinct entity? J Clin Oncol. 1998;16: Wilcox RA, Feldman AL, Wada DA, Yang Z-Z, Comfere NI, Dong H, et al. B7-H1 (PD-L1, CD274) suppresses host immunity in T-cell lymphoproliferative disorders. Blood. 2009;114: Panico L, Ronconi F, Lepore M, Tenneriello V, Cantore N, Dell angelo AC, et al. The prognostic role of tumor associated macrophages and angiogenesis in classical Hodgkin lymphoma. Leuk Lymphoma. 2013;Epub ahead of print. 31. Jones K, Vari F, Keane C, Crooks P, Nourse JP, Seymour LA, et al. Serum CD163 and TARC as disease response biomarkers in classical Hodgkin lymphoma. Clin Cancer Res. 2013;19: Kamper P, Bendix K, Hamilton-Dutoit SJ, Honoré B, Nyengaard JR, D Amore F. Tumor-infiltrating macrophages correlate with adverse prognosis and Epstein-Barr virus status in classical Hodgkin s lymphoma. Haematologica. 2011;96: Tzankov A, Matter MS, Dirnhofer S. Refined prognostic role of CD68-positive tumor macrophages in the context of the cellular micromilieu of classical Hodgkin lymphoma. Pathobiology. 2010;77: Zou W, Chen L. Inhibitory B7-family molecules in the tumour microenvironment. Nat Rev Immunol. 2008;8:
33 35. Andorsky DJ, Yamada RE, Said J, Pinkus GS, Betting DJ, Timmerman JM. Programmed death ligand 1 is expressed by non-hodgkin lymphomas and inhibits the activity of tumor-associated T cells. Clin Cancer Res. 2011;17: Lyford-Pike S, Peng S, Young GD, Taube JM, Westra WH, Akpeng B, et al. Evidence for a Role of the PD-1:PD-L1 Pathway in Immune Resistance of HPV- Associated Head and Neck Squamous Cell Carcinoma. Cancer Res. 2013;73:
34 Table 1. Cases with 5% malignant cells positive* N (%) Cases with 20% total cellularity positive** N (%) Cases Diagnosis N Classical Hodgkin lymphoma (CHL) (87) 31 (82) Nodular sclerosis CHL (84) 19 (76) Mixed cellularity CHL 8 7 (88) 7 (88) CHL-not otherwise specified (NOS) 5 5 (100) 5 (100) Nodular lymphocyte predominant Hodgkin lymphoma 15 2 (13) 1 (7) Primary mediastinal large B-cell lymphoma (71) 19 (90) T-cell/Histiocyte-rich large B-cell lymphoma (91) 11 (100) EBV+ diffuse large B-cell lymphoma (DLBCL) (100) 16 (100) EBV+ DLBCL of elderly 9 9 (100) 9 (100) EBV+ immunodeficiency associated DLBCL 7 7 (100) 7 (100) EBV+ posttransplant lymphoproliferative disorder (PTLD) 10 6 (60) 7 (70) EBV-negative PTLD 7 4 (57) 4 (57) DLBCL-NOS 66 7 (11) 9 (14) Plasmablastic lymphoma 9 4 (44) 4 (44) Primary effusion lymphoma 4 2 (50) 3 (75) Extranodal NK/T-cell lymphoma 6 4 (67) 5 (83) EBV+ Burkitt lymphoma 7 0 (0) 0 (0) EBV+ Nasopharyngeal carcinoma (89) nd HHV8+ Kaposi sarcoma 9 0 (0) nd *>2+ membranous staining; **>2+ membranous and/or cytoplasmic staining; nd - not determined. 34
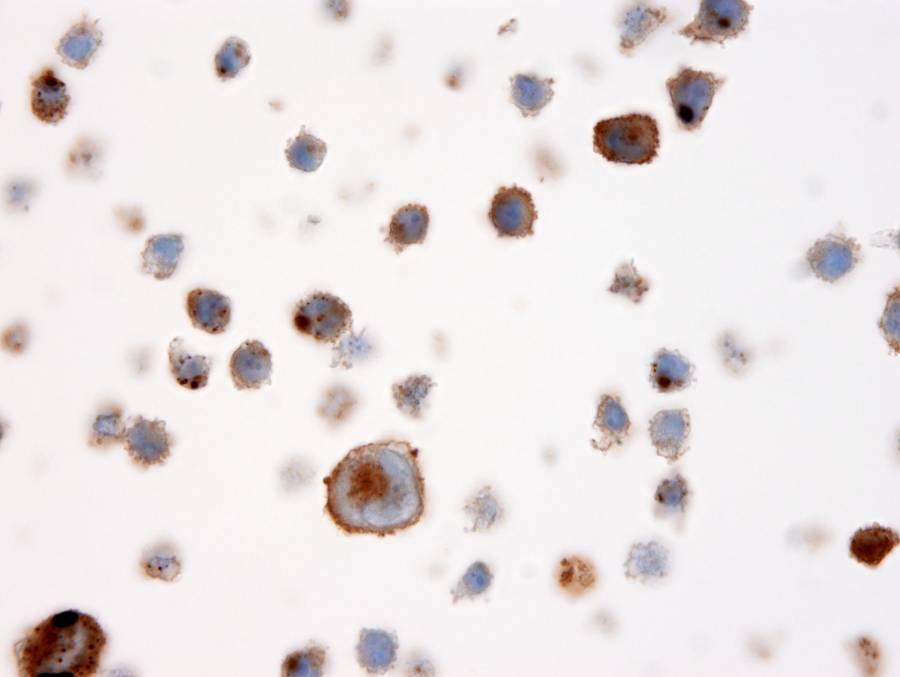
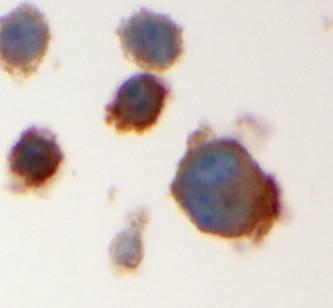
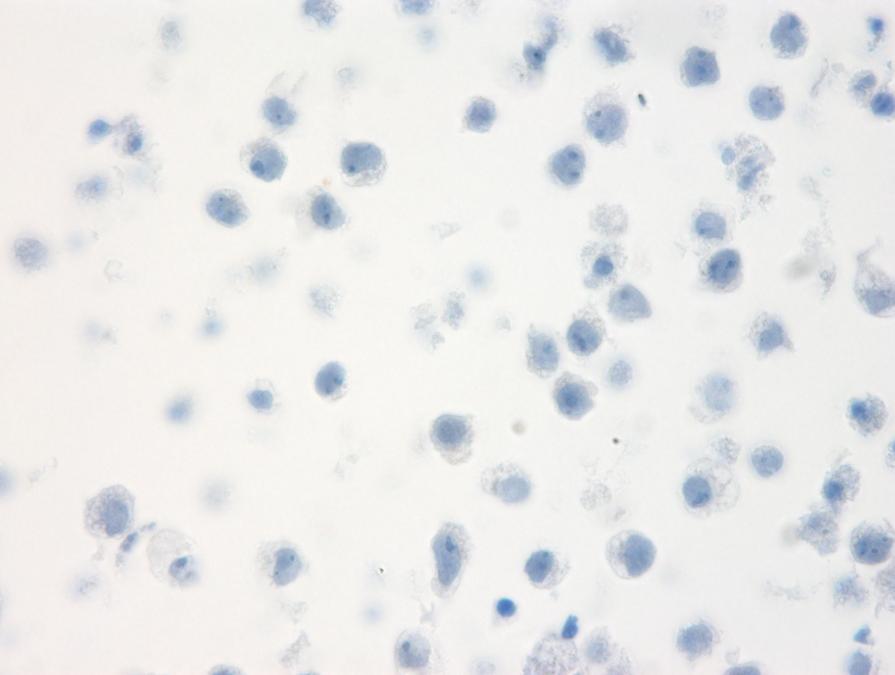
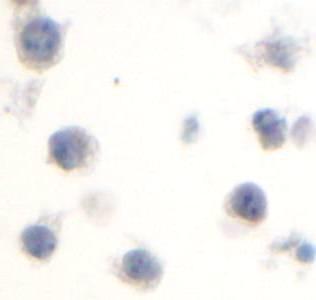
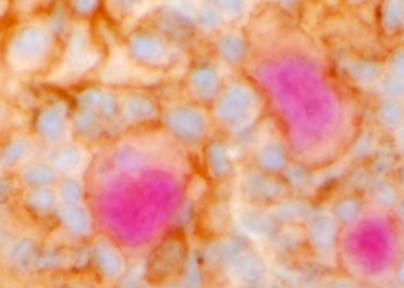
35 FIGURE LEGENDS Figure 1. PD-L1 antibody validation. (A) Western blot analysis of cell lysates derived from genetically characterized diffuse large B-cell lymphoma (DLBCL) cell lines (DHL4, Ly1) and the Hodgkin lymphoma cell lines (L428, SUP-HD1, HDLM2). Lysates were probed with a rabbit monoclonal antibody recognizing PD-L1 (top panel) showing a band at the expected size of the fully glycosylated form of PD-L1 (~55 kda). The gene copy number (CN) for the CD274 (PD-L1) locus, 9p24.1, is shown, as reported previously, for each cell line. 5 Equal loading was demonstrated by probing for GAPDH. IHC analysis of formalin-fixed, paraffin embedded (FFPE) Hodgkin cell line HDLM2 (B) and DLBCL cell line DHL4 (C) stained with the rabbit anti-pd-l1 antibody showing membranous staining of the HDLM2 cells but no staining of DHL4 cells. Insets show similar staining patterns with the mouse monoclonal anti-pd-l1 antibody. (D) FFPE human tonsil stained with rabbit anti-pd-l1 antibody showing little staining of lymphoid cells and weak membranous staining of occasional macrophages (inset, arrow). Figure 2. Immunohistochemical analysis of PD-L1 in CHL, NLPHL, PMLBCL and TCRLBCL. (A) Representative example of nodular sclerosis classical Hodgkin lymphoma (NSCHL) stained with the rabbit anti-pd-l1 antibody showing distinct membranous staining of Reed-Sternberg (RS) cells and intra-tumoral macrophages. Inset shows staining with rabbit anti-pd-l1 (brown) highlighting the cell membrane of RS cells (arrow) as well as non-malignant cells, and macrophages (arrowheads) double stained with rabbit anti-pd-l1 and the macrophage marker CD68 (red). (B) Representative case of nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) 35
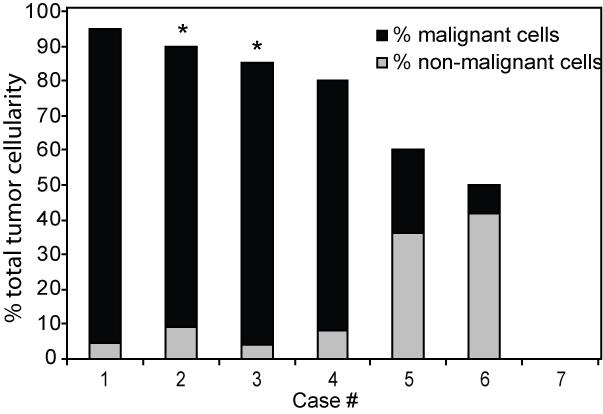
36 stained with rabbit anti-pd-l1 showing LP cells (arrows) that are negative for PD-L1. (C) Representative case of primary mediastinal large B-cell lymphoma (PMBCL) stained with rabbit anti-pd-l1 antibody showing predominantly membranous staining of lymphoma cells. (D) Representative case of T-cell/histiocyte-rich large B-cell lymphoma (TCHRBCL) stained with rabbit anti-pd-l1 antibody. Inset shows staining with mouse anti-pd-l1 (brown) highlighting macrophages adjacent to scattered malignant cells (arrow) that are double stained for PD-L1 and the B-cell lineage marker PAX5 (red). Figure 3. (A, C) Graphical representation of the percentage of the total malignant cells within the tumor sample staining positive for rabbit anti-pd-l1 and (B, C) graphical representation of the percentage of the total cells within the tumor sample staining positive with the rabbit anti-pd-l1 (with the contributions of malignant cells, black bars, and non-malignant cells, grey bars, indicated) in each case of NSCHL (A, B) and NLPHL (C, D) examined. * indicates cases exhibiting predominantly cytoplasmic staining. Figure 4. PD-L1 expression in EBV-positive DLBCLs, EBV-negative PTLD and DLBCL-NOS. (A) Representative case of an EBV-positive immunodeficiencyassociated diffuse large B-cell lymphoma (DLBCL) stained with rabbit anti-pd-l1 showing distinct membranous staining of the lymphoma cells. Inset shows a case of EBV-positive DLBCL of the elderly double stained for mouse anti-pd-l1 (brown) and PAX5 (red). (B) Representative case of an EBV-negative post-transplant 36
37 lymphoproliferative disorder (PTLD) stained with rabbit anti-pd-l1 showing distinct membranous staining of the lymphoma cells. Inset shows double staining of the same case for mouse anti-pd-l1 and PAX5. (C) Case of DLBCL-NOS stained with rabbit anti-pd-l1 showing no staining of the lymphoma cells but scattered intra-tumoral macrophages filled with apoptotic debris showing weak membrane positivity for PD-L1. (D-F) Graphical representation of the percentage of total cells within the biopsy sample staining positive with the rabbit anti-pd-l1, and showing the contributions of malignant cells (black bars) and non-malignant cells (grey bars) in each case of EBV+ DLBCL of the elderly/immunodeficiency-associated, EBV-negative PTLD, and DLBCL-NOS, respectively. * indicates cases exhibiting predominantly cytoplasmic staining. Figure 5. Immunohistochemical analysis of PD-L1 expression in viral-associated lymphomas and additional cancers. Representative cases of (A) EBV-positive plasmablastic lymphoma (PBL), (B) HHV8-positive primary effusion lymphoma (PEL), (C) EBV-positive extranodal NK/T-cell lymphoma (ENKTCL), (D) EBV-positive Burkitt lymphoma (BL), (E) EBV-positive nasopharyngeal carcinoma (NPC), and (F) HHV8-positive Kaposi sarcoma (KS) stained with rabbit anti-pd-l1 or mouse anti-pd- L1 (insets). 37



38 Figure 1 A. B. C. D.





39 Figure 2 A. B. C. D.

40 Figure 3 A. B. C. D.






41 Figure 4 A. D. B. E. C. F.








42 Figure 5 A. B. C. D. E. F.
Constitutive AP-1 Activity and EBV Infection Induce PD-L1 in Hodgkin. Lymphomas and Post-transplant Lymphoproliferative Disorders:
 Constitutive AP-1 Activity and EBV Infection Induce PD-L1 in Hodgkin Lymphomas and Post-transplant Lymphoproliferative Disorders: Implications for Targeted Therapy Running title: AP-1 Activity and EBV
Constitutive AP-1 Activity and EBV Infection Induce PD-L1 in Hodgkin Lymphomas and Post-transplant Lymphoproliferative Disorders: Implications for Targeted Therapy Running title: AP-1 Activity and EBV
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy
 Assay Guiding immunotherapy") VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
VENTANA PD-L1 (SP142) Assay
 Assay") VENTANA (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess UC patient benefit from TECENTRIQ
VENTANA (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess UC patient benefit from TECENTRIQ
EBV infection B cells and lymphomagenesis. Sridhar Chaganti
 EBV infection B cells and lymphomagenesis Sridhar Chaganti How EBV infects B-cells How viral genes influence the infected B cell Differences and similarities between in vitro and in vivo infection How
EBV infection B cells and lymphomagenesis Sridhar Chaganti How EBV infects B-cells How viral genes influence the infected B cell Differences and similarities between in vitro and in vivo infection How
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy in NSCLC
 Assay Guiding immunotherapy in NSCLC") VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Exploring the PD-L1 Pathway
 Active Within the tumor microenvironment Steps 1-3: Initiating and propagating anticancer immunity 1 may inhibit T-cell activity in the tumor microenvironment Dendritic cells capture cancer and then prime
Active Within the tumor microenvironment Steps 1-3: Initiating and propagating anticancer immunity 1 may inhibit T-cell activity in the tumor microenvironment Dendritic cells capture cancer and then prime
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16
 COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR
 Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR Pages with reference to book, From 305 To 307 Irshad N. Soomro,Samina Noorali,Syed Abdul Aziz,Suhail Muzaffar,Shahid
Gastric Carcinoma with Lymphoid Stroma: Association with Epstein Virus Genome demonstrated by PCR Pages with reference to book, From 305 To 307 Irshad N. Soomro,Samina Noorali,Syed Abdul Aziz,Suhail Muzaffar,Shahid
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Major categories of large cell lymphomas include
 ORIGINAL ARTICLE Aberrant Expression of the Dendritic Cell Marker TNFAIP2 by the Malignant Cells of Hodgkin Lymphoma and Primary Mediastinal Large B-Cell Lymphoma Distinguishes These Tumor Types From Morphologically
ORIGINAL ARTICLE Aberrant Expression of the Dendritic Cell Marker TNFAIP2 by the Malignant Cells of Hodgkin Lymphoma and Primary Mediastinal Large B-Cell Lymphoma Distinguishes These Tumor Types From Morphologically
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA. Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine
 NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
VIRUSES AND CANCER Michael Lea
 VIRUSES AND CANCER 2010 Michael Lea VIRAL ONCOLOGY - LECTURE OUTLINE 1. Historical Review 2. Viruses Associated with Cancer 3. RNA Tumor Viruses 4. DNA Tumor Viruses HISTORICAL REVIEW Historical Review
VIRUSES AND CANCER 2010 Michael Lea VIRAL ONCOLOGY - LECTURE OUTLINE 1. Historical Review 2. Viruses Associated with Cancer 3. RNA Tumor Viruses 4. DNA Tumor Viruses HISTORICAL REVIEW Historical Review
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow Up
 J Clin Exp Hematopathol Vol. 50, No. 1, May 2010 Case Study A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow
J Clin Exp Hematopathol Vol. 50, No. 1, May 2010 Case Study A Unique Case of Nasal NK/T Cell Lymphoma with Frequent Remission and Relapse Showing Different Histological Features During 12 Years of Follow
ESMO DOUBLE-HIT LYMPHOMAS
 ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
PD-1/PD-L1 Checkpoint in Lymphoprolipherative Malignancies: Focus on Critical Points for Tissue Assessment
 ARC Journal of Hematology Volume 2, Issue 2, 2017, PP 1-6 www.arcjournals.org PD-1/PD-L1 Checkpoint in Lymphoprolipherative Malignancies: Focus on Critical Points for Tissue Antonella Bianchi 1*, Ombretta
ARC Journal of Hematology Volume 2, Issue 2, 2017, PP 1-6 www.arcjournals.org PD-1/PD-L1 Checkpoint in Lymphoprolipherative Malignancies: Focus on Critical Points for Tissue Antonella Bianchi 1*, Ombretta
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas
: Aggressive B-cell Lymphomas") Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
PD-L1 and Immunotherapy of GI cancers: What do you need to know
 None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Nodular lymphocyte predominant Hodgkin lymphoma. Lymphoma Tumor Board. January 5, 2018
 Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Untangling the tumor microenvironment
 Webinar Series Untangling the tumor microenvironment Illuminating the complex interactions & functions of immune cells December 10, 2014 Instructions for Viewers To share webinar via social media: To share
Webinar Series Untangling the tumor microenvironment Illuminating the complex interactions & functions of immune cells December 10, 2014 Instructions for Viewers To share webinar via social media: To share
Circulating PD-L1 in NSCLC patients and the correlation between the level of PD-L1 expression and the clinical characteristics
 Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Circulating PD-L1 in NSCLC patients and the correlation between the level of PD-L1 expression and the clinical characteristics Jie Zhang, Jing Gao, Yanyan
Thoracic Cancer ISSN 1759-7706 ORIGINAL ARTICLE Circulating PD-L1 in NSCLC patients and the correlation between the level of PD-L1 expression and the clinical characteristics Jie Zhang, Jing Gao, Yanyan
Prevalent lymphomas in Africa
 Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
The History of Lymphoma Classification and the 2017 Revision
 The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Case Report Epstein-Barr Virus Infection in an Elderly Nonimmunocompromised Adult Successfully Treated with Rituximab
 Case Reports in Hematology, Article ID 641483, 4 pages http://dx.doi.org/10.1155/2014/641483 Case Report Epstein-Barr Virus Infection in an Elderly Nonimmunocompromised Adult Successfully Treated with
Case Reports in Hematology, Article ID 641483, 4 pages http://dx.doi.org/10.1155/2014/641483 Case Report Epstein-Barr Virus Infection in an Elderly Nonimmunocompromised Adult Successfully Treated with
Darwinian selection and Newtonian physics wrapped up in systems biology
 Darwinian selection and Newtonian physics wrapped up in systems biology Concept published in 1957* by Macfarland Burnet (1960 Nobel Laureate for the theory of induced immune tolerance, leading to solid
Darwinian selection and Newtonian physics wrapped up in systems biology Concept published in 1957* by Macfarland Burnet (1960 Nobel Laureate for the theory of induced immune tolerance, leading to solid
Anti-PD-L1 antibody [28-8] ab205921
![Anti-PD-L1 antibody [28-8] ab205921](/thumbs/84/91196262.jpg "Anti-PD-L1 antibody [28-8] ab205921") Anti-PD-L1 antibody [28-8] ab205921 2 Abreviews 16 References 15 Images Overview Product name Anti-PD-L1 antibody [28-8] Description Tested applications Species reactivity Immunogen Rabbit monoclonal [28-8]
Anti-PD-L1 antibody [28-8] ab205921 2 Abreviews 16 References 15 Images Overview Product name Anti-PD-L1 antibody [28-8] Description Tested applications Species reactivity Immunogen Rabbit monoclonal [28-8]
ENVIRONMENTAL FACTORS IN VIRUS-ASSOCIATED HUMAN CANCERS
 ENVIRONMENTAL FACTORS IN VIRUS-ASSOCIATED HUMAN CANCERS Joint Graduate Seminar Depar tment of Microbiology The Chinese University of Hong Kong PhD Candidate: Zhang Chuqing Super visor: Professor Paul Chan
ENVIRONMENTAL FACTORS IN VIRUS-ASSOCIATED HUMAN CANCERS Joint Graduate Seminar Depar tment of Microbiology The Chinese University of Hong Kong PhD Candidate: Zhang Chuqing Super visor: Professor Paul Chan
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1
, the most common aggressive form of B-cell non-hodgkin s lymphoma 1") Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1 Expression of B-cell surface antigens drives several non-hodgkin s lymphomas (NHLs)
Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1 Expression of B-cell surface antigens drives several non-hodgkin s lymphomas (NHLs)
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma
 Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.
 CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.") Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
PD-L1 Analyte Control DR
 Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma
 T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
Diffuse large B-cell lymphoma (DLBCL) is one of the
 is one of the") Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Anti-DC-SIGN/CD209 murine monoclonal antibodies
 Anti-DC-SIGN/CD209 murine monoclonal antibodies DC-SIGN (DC Specific, ICAM-3 Grabbing, Nonintegrin) / CD209 and L-SIGN (liver/lymph node-specific ICAM-3-grabbing nonintegrin CD299/ DC-SIGNR (DC-SIGN-related
Anti-DC-SIGN/CD209 murine monoclonal antibodies DC-SIGN (DC Specific, ICAM-3 Grabbing, Nonintegrin) / CD209 and L-SIGN (liver/lymph node-specific ICAM-3-grabbing nonintegrin CD299/ DC-SIGNR (DC-SIGN-related
Primary mediastinal (thymic) large B-cell lymphoma
 large B-cell lymphoma") ORIGINAL ARTICLE Expression of Programmed Cell Death 1 Ligand 2 (PD-L2) Is a Distinguishing Feature of Primary Mediastinal (Thymic) Large B-cell Lymphoma and Associated With PDCD1LG2 Copy Gain Min Shi,
ORIGINAL ARTICLE Expression of Programmed Cell Death 1 Ligand 2 (PD-L2) Is a Distinguishing Feature of Primary Mediastinal (Thymic) Large B-cell Lymphoma and Associated With PDCD1LG2 Copy Gain Min Shi,
HIV Related Malignancies: Lessons Learned. Dr. Adan Rios Division of Oncology Department of Internal Medicine
 HIV Related Malignancies: Lessons Learned Dr. Adan Rios Division of Oncology Department of Internal Medicine Cancer, HIV and HAART PI=>IL-6 % R= KS NHL J Acquir. Immune. Defic. Syndr. 2015. 68:568-577
HIV Related Malignancies: Lessons Learned Dr. Adan Rios Division of Oncology Department of Internal Medicine Cancer, HIV and HAART PI=>IL-6 % R= KS NHL J Acquir. Immune. Defic. Syndr. 2015. 68:568-577
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection. Masoud Mardani M.D,FIDSA
 Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Review of NEO Testing Platforms. Lawrence M. Weiss, MD Medical Director, Aliso Viejo
 Review of NEO Testing Platforms Lawrence M. Weiss, MD Medical Director, Aliso Viejo Lawrence Weiss, M.D. Medical Director, Aliso Viejo Dr. Weiss currently serves as NeoGenomics Medical Director, Aliso
Review of NEO Testing Platforms Lawrence M. Weiss, MD Medical Director, Aliso Viejo Lawrence Weiss, M.D. Medical Director, Aliso Viejo Dr. Weiss currently serves as NeoGenomics Medical Director, Aliso
Tumor Immunology. Tumor (latin) = swelling
 = swelling") Tumor Immunology Tumor (latin) = swelling benign tumor malignant tumor Tumor immunology : the study of the types of antigens that are expressed by tumors how the immune system recognizes and responds to
Tumor Immunology Tumor (latin) = swelling benign tumor malignant tumor Tumor immunology : the study of the types of antigens that are expressed by tumors how the immune system recognizes and responds to
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Establishing etiopathogenesis in Epstein-Barr virus associated malignancies using chromogenic in situ hybridization
 Original Article DOI: 10.18203/issn.2456-3994.IntJMolImmunoOncol20172643 Establishing etiopathogenesis in Epstein-Barr virus associated malignancies using chromogenic in situ hybridization Ashwini J. Patkar,
Original Article DOI: 10.18203/issn.2456-3994.IntJMolImmunoOncol20172643 Establishing etiopathogenesis in Epstein-Barr virus associated malignancies using chromogenic in situ hybridization Ashwini J. Patkar,
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma. PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use
 Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Interpretation Manual - Gastric or Gastroesophageal Junction Adenocarcinoma PD-L1 IHC 22C3 pharmdx is FDA-approved for in vitro diagnostic use For countries outside of the United States, see the local
Epstein-Barr virus and immunity
 Epstein-Barr virus and immunity Elena Kashuba, PhD Associate Professor Department of Microbiology, Tumor and Cell Biology (MTC) Karolinska Institutet 1 Epstein-Barr virus EBV Everybody s virus 200 nm Enveloped
Epstein-Barr virus and immunity Elena Kashuba, PhD Associate Professor Department of Microbiology, Tumor and Cell Biology (MTC) Karolinska Institutet 1 Epstein-Barr virus EBV Everybody s virus 200 nm Enveloped
VENTANA hematopathology solutions. Deliver diagnostic confidence
 VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma
 Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Hemophagocytic Lymphohistiocytosis Secondary to T cell/histiocyte-rich Large B-cell Lymphoma Katherine Devitt, M.D., Benjamin Chen, M.D., Ph.D., Hongbo Yu, M.D., Ph.D., Bruce Woda, M.D. 1 1 Department
Detection of EBV in reactive and neoplastic lymphoproliferations in adults when and how?
 J Hematopathol (2014) 7:165 170 DOI 10.1007/s12308-014-0209-0 REVIEW ARTICLE Detection of EBV in reactive and neoplastic lymphoproliferations in adults when and how? Christiane Stuhlmann-Laeisz Ilske Oschlies
J Hematopathol (2014) 7:165 170 DOI 10.1007/s12308-014-0209-0 REVIEW ARTICLE Detection of EBV in reactive and neoplastic lymphoproliferations in adults when and how? Christiane Stuhlmann-Laeisz Ilske Oschlies
Thomas Hodgkin and Hodgkin lymphoma
 J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
The author has declared no conflicts of interest.
 Epstein Barr Virus: A Biological Overview and Clinicopathological Changes of Two Epstein Barr Virus-Related Lymphoproliferative Disorders in a World Health Organization (WHO) 2017 Report Authors: *Cristiano
Epstein Barr Virus: A Biological Overview and Clinicopathological Changes of Two Epstein Barr Virus-Related Lymphoproliferative Disorders in a World Health Organization (WHO) 2017 Report Authors: *Cristiano
Bihong Zhao, M.D, Ph.D Department of Pathology
 Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Bihong Zhao, M.D, Ph.D Department of Pathology 04-28-2009 Is tumor self or non-self? How are tumor antigens generated? What are they? How does immune system respond? Introduction Tumor Antigens/Categories
Review (V1) - The Hallmarks of Cancer
 - The Hallmarks of Cancer") Review (V1) - The Hallmarks of Cancer Robert A. Weinberg 1 Review (V1) - The Hallmarks of Cancer 2 Review (V1) - Number of somatic mutations in human cancers Top: children vs. adults Numbers in parentheses
Review (V1) - The Hallmarks of Cancer Robert A. Weinberg 1 Review (V1) - The Hallmarks of Cancer 2 Review (V1) - Number of somatic mutations in human cancers Top: children vs. adults Numbers in parentheses
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping
 VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
EBV Infection and Immunity. Andrew Hislop Institute for Cancer Studies University of Birmingham
 EBV Infection and Immunity Andrew Hislop Institute for Cancer Studies University of Birmingham EBV Introduction Large ds DNA virus Spread by saliva contact Lifelong infection Predominantly B-lymphotropic
EBV Infection and Immunity Andrew Hislop Institute for Cancer Studies University of Birmingham EBV Introduction Large ds DNA virus Spread by saliva contact Lifelong infection Predominantly B-lymphotropic
Methotrexate-associated Lymphoproliferative Disorders
 Methotrexate-associated Lymphoproliferative Disorders Definition A lymphoid proliferation or lymphoma in a patient immunosuppressed with methotrexate, typically for treatment of autoimmune disease (rheumatoid
Methotrexate-associated Lymphoproliferative Disorders Definition A lymphoid proliferation or lymphoma in a patient immunosuppressed with methotrexate, typically for treatment of autoimmune disease (rheumatoid
Persistent Infections
 Persistent Infections Lecture 17 Biology 3310/4310 Virology Spring 2017 Paralyze resistance with persistence WOODY HAYES Acute vs persistent infections Acute infection - rapid and self-limiting Persistent
Persistent Infections Lecture 17 Biology 3310/4310 Virology Spring 2017 Paralyze resistance with persistence WOODY HAYES Acute vs persistent infections Acute infection - rapid and self-limiting Persistent
EBV and Infectious Mononucleosis. Infectious Disease Definitions. Infectious Diseases
 Infectious Disease Definitions Infection when a microorganism invades a host and multiplies enough to disrupt normal function by causing signs and symptoms Pathogencity ability of an organism to cause
Infectious Disease Definitions Infection when a microorganism invades a host and multiplies enough to disrupt normal function by causing signs and symptoms Pathogencity ability of an organism to cause
Hodgkin Lymphomas: An Update
 Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and Review of the Literature
 Hindawi Case Reports in Hematology Volume 2017, Article ID 7531729, 4 pages https://doi.org/10.1155/2017/7531729 Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and
Hindawi Case Reports in Hematology Volume 2017, Article ID 7531729, 4 pages https://doi.org/10.1155/2017/7531729 Case Report PAX5-Negative Classical Hodgkin Lymphoma: A Case Report of a Rare Entity and
Leukaemia Section Short Communication
 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Leukaemia Section Short Communication Classification of Hodgkin lymphoma over years Antonino Carbone, Annunziata
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL INIST-CNRS Leukaemia Section Short Communication Classification of Hodgkin lymphoma over years Antonino Carbone, Annunziata
Detection of Anaplastic Lymphoma Kinase (ALK) gene in Non-Small Cell lung Cancer (NSCLC) By CISH Technique
 gene in Non-Small Cell lung Cancer (NSCLC) By CISH Technique") Cancer and Clinical Oncology; Vol. 7, No. 1; 2018 ISSN 1927-4858 E-ISSN 1927-4866 Published by Canadian Center of Science and Education Detection of Anaplastic Lymphoma Kinase (ALK) gene in Non-Small Cell
Cancer and Clinical Oncology; Vol. 7, No. 1; 2018 ISSN 1927-4858 E-ISSN 1927-4866 Published by Canadian Center of Science and Education Detection of Anaplastic Lymphoma Kinase (ALK) gene in Non-Small Cell
Tumor Immunology. Wirsma Arif Harahap Surgical Oncology Consultant
 Tumor Immunology Wirsma Arif Harahap Surgical Oncology Consultant 1) Immune responses that develop to cancer cells 2) Escape of cancer cells 3) Therapies: clinical and experimental Cancer cells can be
Tumor Immunology Wirsma Arif Harahap Surgical Oncology Consultant 1) Immune responses that develop to cancer cells 2) Escape of cancer cells 3) Therapies: clinical and experimental Cancer cells can be
microrna Presented for: Presented by: Date:
 microrna Presented for: Presented by: Date: 2 micrornas Non protein coding, endogenous RNAs of 21-22nt length Evolutionarily conserved Regulate gene expression by binding complementary regions at 3 regions
microrna Presented for: Presented by: Date: 2 micrornas Non protein coding, endogenous RNAs of 21-22nt length Evolutionarily conserved Regulate gene expression by binding complementary regions at 3 regions
HIV and Malignancy Alaka Deshpande, Himanshu Soni
 HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
HIV and Malignancy Alaka Deshpande, Himanshu Soni Emergence of new infectious disease was documented in 1981. Within a short span of time it became a pandemic. It was Acquired Immunodeficiency Syndrome
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Accepted Manuscript. Next Steps for Immune Checkpoints in Hepatocellular Carcinoma. Patricia M. Santos, Lisa H. Butterfield
 Accepted Manuscript Next Steps for Immune Checkpoints in Hepatocellular Carcinoma Patricia M. Santos, Lisa H. Butterfield PII: S0016-5085(18)35218-1 DOI: https://doi.org/10.1053/j.gastro.2018.11.008 Reference:
Accepted Manuscript Next Steps for Immune Checkpoints in Hepatocellular Carcinoma Patricia M. Santos, Lisa H. Butterfield PII: S0016-5085(18)35218-1 DOI: https://doi.org/10.1053/j.gastro.2018.11.008 Reference:
Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?
 Histopathology 2012, 61, 1214 1218. DOI: 10.1111/j.1365-2559.2012.04351.x SHORT REPORT Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?
Histopathology 2012, 61, 1214 1218. DOI: 10.1111/j.1365-2559.2012.04351.x SHORT REPORT Does the proliferation fraction help identify mature B cell lymphomas with double- and triple-hit translocations?