Saudi Journal of Pathology and Microbiology (SJPM)
|
|
|
- Henry Fisher
- 5 years ago
- Views:
Transcription
 ISSN 2518-3370 (Online) Histopathological Study of Neoplastic Lesions in Large Intestine Dr. Prakash Roplekar 1, Dr. Akanksha Pandey 2, Dr.")
1 Saudi Journal of Pathology and Microbiology (SJPM) Scholars Middle East Publishers Dubai, United Arab Emirates Website: ISSN (Print) ISSN (Online) Histopathological Study of Neoplastic Lesions in Large Intestine Dr. Prakash Roplekar 1, Dr. Akanksha Pandey 2, Dr. Prasmit Shah 3 1 Prof & Head of Department, Dr. D. Y. Patil University School of Medicine, 11, Ayyappa Rd, Dr D Y Patil Vidyanagar, Sector 7, Nerul, Navi Mumbai, Maharashtra, India 2 Resident, Dr. D. Y. Patil University School of Medicine, 11, Ayyappa Rd, Dr D Y Patil Vidyanagar, Sector 7, Nerul, Navi Mumbai, Maharashtra, India 3 Department of Pathology, Dr. D. Y. Patil University School of Medicine, 11, Ayyappa Rd, Dr D Y Patil Vidyanagar, Sector 7, Nerul, Navi Mumbai, Maharashtra, India Original Research Article *Corresponding author Mohammed Tbouda Article History Received: Accepted: Published: DOI: /sjpm Abstract: The Large Intestine neoplasms are one of the most common neoplasms encountered now a days. It consists of both colon and rectum malignancies. At present it ranks second to bronchogenic carcinoma in most prevalent cancers. Globally 8,00,000 Colo-Rectal Cancer cases are believed to occur and mortality of this is expected to be near 4,50,000. Overall incidence is 10% of all cancers. The present study was undertaken to study neoplastic lesions in the large intestine for the period of twenty-two months. The study consisted of total 65 cases out of which, 46 were surgically resected specimen and 19 were biopsies. Majority of the cases were Adenocarcinomas (61.5%), followed by Mucinous adenocarcinoma (24.6%). Most common location of Colo-Rectal Cancer was rectum (47.7%) followed by sigmoid colon (15.4%). Rare cases like Signet ring cell carcinoma, squamous cell carcinoma, Gastrointestinal stromal tumor and lymphoma were also found in the study. Histopathological evaluation is the only confirmatory investigation for diagnosis of such tumors. Present study emphasizes the need for early histopathological diagnosis for appropriate treatment. Keywords: Large Intestine, Neoplastic Lesions, Adenocarcinoma INTRODUCTION The colon including rectum is one of the most common host of primary neoplasm in the body [1]. It is reported as the 2nd most prevalent malignancy in USA & Europe [2]. National Cancer Registry Programme (NCRP), a part of Indian Council of Medical Research (ICMR) reported incidence of Colo-Rectal Cancer (CRC) as 2.3% in females for colon cancers and 3.3% in males for Rectal cancers. Above study was based on population of Mumbai and Barshi respectively [3]. The incidence is on rise for CRC. It ranks fourth most common cancer in female and third most common cancer in males [4]. But it ranks second most common in the mortality aspect, first being Bronchogenic Carcinoma [5]. Globally 8,00,000 CRC cases are believed to occur and mortality of this is expected to be near 4,50,000. Overall incidence is 10% of all cancers. Majority of the neoplastic lesions of large intestine are of epithelial origin and virtually 95% of them are Adenocarcinoma. They typically arise in Polyps and produce symptoms relatively early and hence it is always a challenge in the medical profession to diagnose as early as possible. These lesions are curable with resection [6]. The malignant form has unpredictable behavior and hence it has led many clinicians to search for the factors that helps in preparing the prognostic index. Thus, staging and Grading has been evolved to show the Prognostic significance [7]. Hence this study was conducted to find the varying histological patterns and their stage at presentation which will be helpful in the prognosis of the patient. MATERIALS AND METHODS This is a prospective study of large intestinal neoplastic lesions conducted in a tertiary care hospital over a period of 22 months. It is composed of 65 cases. During this period the surgically resected specimens and biopsies in whom the neoplastic lesion was suspected were included in the study. Inclusion Criteria All confirmed cases as well as suspected cases of large intestinal neoplasms sent for histopathological examination in department of Pathology are included in this study. Available online: scholarsmepub.com 471
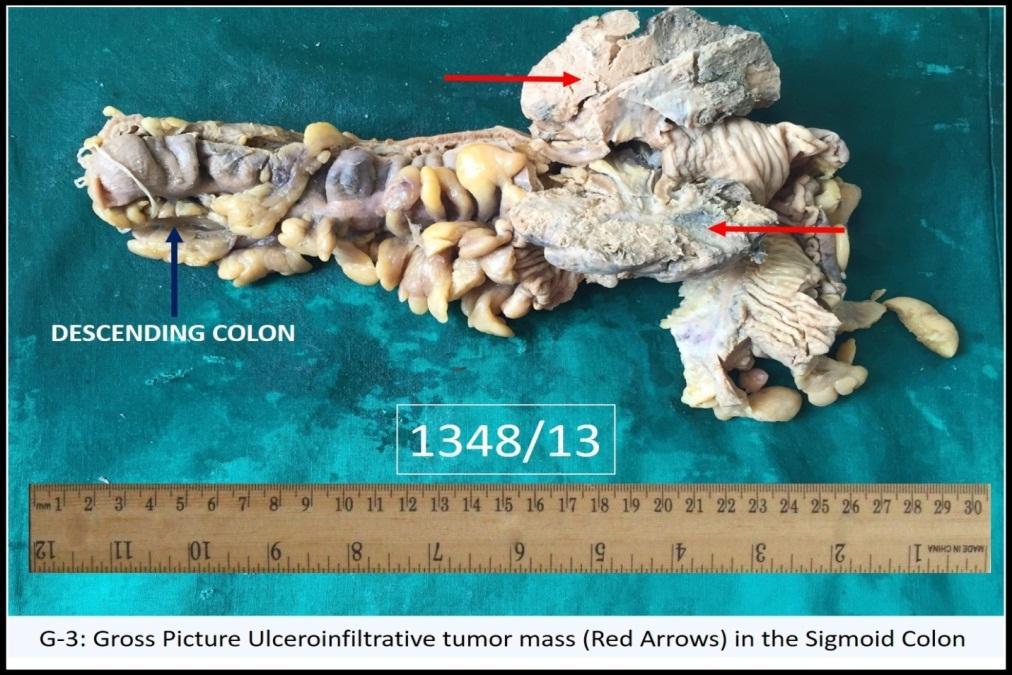
2 Exclusion Criteria Already diagnosed or those patients whose histopathological examination is not carried out in our hospital. Received specimen and biopsies were kept in 10% formalin. Gross and microscopic findings of the benign and malignant lesions were noted. The study consisted of 46 surgically resected specimen and 19 biopsies. Out of 19 biopsies three cases which proved malignant were inoperable. Out of total 46 surgically resected cases, 30 of them have had diagnostic endoscopic biopsy. Apart from biopsy other modalities of investigations are also being done like Ultrasonography, Barium studies, Colonoscopy, Proctosigmoidoscopy and CT-Scan (Both plain and contrast). All these investigations thoroughly supported the clinicians as well as pathologists for final diagnosis. Out of total 65 cases, 27 patients were Anemic with the hemoglobin of less than 8 g/dl and one patient was HIV seropositive. Ten patients were suggested to do the tumor marker Carcinoembryonic antigen (CEA) in which all of them were above the normal levels. Adequate number of tissue blocks were made so as to look for different findings as mentioned above. Tissue processing was done as per standard methods and tissue was embedded in paraffin. Five microns thick sections were taken using a rotatory microtome and stained with Hematoxylene and Eosin stain. Thereafter the sections were studied under the light microscope and findings were noted. Special stains like Periodic acid Schiff (PAS), Mucicarmine were done wherever required. Final diagnosis was then framed. The statistical analysis of the data was done using SPSS version 11.0 for windows. Chi-square and Student s t-test were used for checking the significance Table-1: Number of Colorectal Neoplastic Lesions NATURE OF SPECIMEN NUMBER PERCENTAGE BIOPSY RESECTED SPECIMEN TOTAL of the data. A p-value of 0.05 and lesser was defined to be statistical significant. RESULTS Table-1 shows the number of colorectal neoplastic lesions. The majority of cases came to us after surgical resection of colon. Out of nineteen biopsies two cases were inoperable while remaining were referred to some other hospital. Table-2 shows the distribution of colo-rectal carcinomas sex wise. The incidence of Colo-rectal neoplastic lesions was more in males (57%) as compared to females (43%). Table-3 shows the distribution of colorectal neoplastic lesions. The majority of cases were adenocarcinoma (61.5%), followed by Mucinous adenocarcinoma (24.6%). Table- 4 shows the distribution of colorectal neoplastic lesions age wise. The maximum incidence of adenocarcinoma was found in the sixth decade. Youngest case was 20 years and oldest case was 83 years old. Mucinous adenocarcinomas were common in the fifth decade. Juvenile polyps were common among the tumor like lesions in the first decade. Table 5 shows the distribution of colo-rectal neoplastic lesions site wise. Most common location of Colo-rectal neoplastic lesions is Rectum (47.7%) followed by sigmoid colon (15.4%) while the least common location is Descending colon (4.6%) (Fig-1). Table-6 shows the distribution of macroscopic type of growth in colo-rectal carcinomas. The Ulceroproliferative type of growth is the most common type (44.4%) of all macroscopic type of growths, followed by Ulceroinfiltrative type (37.8%) (Fig-2). Table-7 shows the distribution of symptomatology in patients. The most common symptom to the patients in colo-rectal neoplastic lesions is pain in abdomen (70.8%) followed by intestinal obstruction (69.2%) and rectal bleeding (67.7%). Table-2: Distribution of Colo-Rectal Carcinomas Sex Wise TITLE MALE FEMALE TOTAL CASES PERCENTAGE Available online: 472
3 Table-3: Distribution of Colorectal Neoplastic Lesions TUMOURS AND RELATED CONDITIONS NO. OF CASES PERCENTAGE A.BENIGN EPITHELIAL LESIONS: Tubular Adenoma Villous Adenoma 0 0 Tubulo-Villous Adenoma 0 0 B.MALIGNANT EPITHELIAL LESIONS: Adenocarcinoma Mucinous Adenocarcinoma Signet-Ring Cell Carcinoma Squamous Cell Carcinoma Undifferentiated Carcinoma 0 0 C.CARCINOID TUMOUR: 0 0 D.NON-EPITHELIAL TUMOURS: 0 0 Leiomyoma 0 0 Leiomyosarcoma 0 0 Gastrointestinal Stromal Tumor E.LYMPHOMA: F.SECONDARY TUMOURS: 0 0 G.TUMOUR LIKE LESIONS: Peutz-Jegher s Polyp 0 0 Juvenile Polyp Hyperplastic Polyp Inflammatory Polyp 0 0 H.RECURRENCE IN ADENOCARCINOMA 0 0 Table-4: Distribution of Colorectal Neoplastic Lesions Age Wise TUMOURS AND RELATED CONDITIONS >80 A.BENIGN EPITHELIAL LESIONS: Tubular Adenoma Villous Adenoma Tubulo-Villous Adenoma B.MALIGNANT EPITHELIAL LESIONS: Adenocarcinoma Mucinous Adenocarcinoma Signet-Ring Cell Carcinoma Squamous Cell Carcinoma C.CARCINOID TUMOUR: D.NON-EPITHELIAL TUMOURS: Leiomyoma Leiomyosarcoma Gastrointestinal Stromal Tumor E.LYMPHOMA: F.SECONDARY TUMOURS: G.TUMOUR LIKE LESIONS: Peutz-Jegher s Polyp Juvenile Polyp Hyperplastic Polyp Inflammatory Polyp H.RECURRENCE IN ADENOCARCINOMA Table-5: Distribution of Colo-Rectal Neoplastic Lesions Site Wise SITE OF LESION NO. OF CASES PERCENTAGE (%) Caecum Ascending Colon Transverse Colon Descending Colon Sigmoid Colon Rectum TOTAL Available online: 473
4 Fig 1: Table-6: Distribution of Macroscopic Type of Growth in Colo-Rectal Carcinomas TYPE TOTAL PERCENTAGE Polypoid Ulceroinfiltrative Ulceroproliferative Fungating TOTAL Fig-2: Table-7: Distribution of Symptomatology In Patients SYMPTOMS NUMBER PERCENTAGE Rectal Bleeding Lump in Abdomen Pain in Abdomen Weight Loss Loss of Appetite Anaemia S/O Intestinal Obstruction Available online: 474

5 Fig-3: Fig-4: Fig-5: Available online: 475

. Maximum number of cases belonged to 50-59 years of age group.")
6 Fig-6: Hyperplastic Polyp - Rectum Fig-7: Well Differentiated Adenocarcinoma - Caecum DISCUSSION The colon including the rectum are the most common host of primary neoplasm in the body. Majority of these lesions are adenocarcinoma. The present study was undertaken to study neoplastic lesions in the large intestine for the period of twenty two months. Sixty five cases were included in the study and they were evaluated to study the incidence in the relation of age, sex, site and various histological patterns. Majority of cases were Colorectal Adenocarcinoma. In our study 40 cases were adenocarcinomas with an incidence of (61.5%). Maximum number of cases belonged to years of age group. Youngest case was 20 year old and oldest case was 83 year old. Goligher suggested that the commonest age group of years [8]. Mohsin-ul- Rassol et al., [9] reported the age group of years and these findings are consistent with our study. Incidence of CRC was more common on males (57%) than in the females (43%). Considering adenocarcinoma incidence was higher in males (62.1%) than in females (60.7%) with the ratio of 1.03:1. The findings are consistent with Silverberg [14] who reported the rough incidence of 1:1. Mohsin-ul-Rassol et al., [9] reported the incidence of 1.3:1. Most common presenting symptom was pain in abdomen (70.8%) followed by intestinal obstruction (69.2%) and rectal bleeding (67.7%). These symptoms are in the agreement with other studies. Two cases of benign epithelial lesions were noted and both of them were in females and in the age group of years. Most common location of CRC was found to be in the rectum (47.7%) followed by sigmoid colon (15.4%) [9]. Similar findings was reported by Fenn et al., Goligher and Bouchier and Mohsin-ul-Rassol et al., who found that more than half of the cases were found in the rectum [9-11]. Considering colon and rectal cancers separately incidence of rectal cancers were more common in females. Regarding the macroscopic type of growth Ulceroproliferative type of growth is the most common Available online: 476
7 (44.4%) followed by ulceroinfiltrative type (37.8%). Also, the Ulceroproliferative type of growth dominates the right colon while the Ulceroinfiltrative type of growth dominates the left colon. Similar findings were reported by Fenn et al., Goligher and Bouchier [9-11]. Most of the CRC are moderately differentiated (53.0%). This fining was not in the favour of Duke and Qizilbash [12, 13]. They reported the most common differentiation as Well differentiated. Lymphatic invasion is the commonest followed by vascular and neural invasion. The primary tumor had equal distribution of the cases among T2 and T3 (42.5%) while the least common primary tumor stage is T4b (5%). In majority of the cases the lymph node status was N0 (65%), which means that majority if the cases were without lymph node involvement. When lymph nodes are involved, the most common status is N2a (10%). Most common TNM stage in this study is Stage- I (40%) followed by Stage-II (30%), while stage IIC and IVB was not found in any of the case. Most common DUKE stage in this study is Stage-A (41%) followed by Stage-B (33.3%) [11, 12]. Most common MAC stage in this study is Stage-B2 (33.3%) followed by Stage-B1 (30.8%). Among other malignant epithelial lesions mucinous adenocarcinomas predominated (24.6%). One case of each Signet ring cell carcinoma, Squamous cell carcinoma, Gastrointestinal stromal tumor and Non-Hodgkin s lymphoma were found. But as these cases are very few, no specific conclusion could be withdrawn. Three cases of tumor like lesions were found namely juvenile polyp and hyperplastic polyp. Again, the cases were very few and hence no specific conclusion was formed. CONCLUSION From the present study it can be concluded that the malignant lesions are more common than the benign lesions. The age and sex prevalence, as well as histopathological characteristics, are similar to that reported in the rest of India and world. Colonic carcinoma is seen with increasing frequency in young adults, so any person with vague abdominal pain, bowel symptoms, iron deficiency anemia should undergo proper evaluation as early as possible. REFERENCES 1. Robbins, S. L., Cotran, R. S., & Turner, J. R. (2012). The Gastrointestinal tract. Pathologic basis of disease, 8th ed. Haryana: Elsevier, Van der Schouw, Y. T., Verbeek, A. L. M., Wobbes, T., Segers, M. F. G., & Thomas, C. M. G. (1992). Comparison of four serum tumour markers in the diagnosis of colorectal carcinoma. British journal of cancer, 66(1), National cancer registry program : An overview Indian council of medical research. 4. Park, K. (2012). Textbook of Preventive and social medicine, 19th ed. Bhanot, Mohsin, U. R., Basharat, M., Riyaz, U. S., Sajad, H., Zubaida, R., & Parveen, S. (2014). Histopathological study of neoplastic lesions of large intestine in Kashmir valley-india. International journal of Research in medical sciences, 3: Jusaawala, D. J., & Gangadharan, P. (1973). Epidemiology of cancer in indian subcontinent. Ind Journal of Cancer; Nacopoulou, L., Azaris, P., Papacharalampous, N., & Davaris, P. (1981). Prognostic significance of histologic host response in cancer of the large bowel. Cancer, 47(5), Goligher, J. C., Duthie, H. L., & Nixon, H. H. (1984). Surgery of the anus, rectum and colon, 5th ed. (p. 246). London: Bailliere Tindall. 9. Rasool, M. U., Mubeen, B., Hamid, S., Rasool, Z., Shah, P., & Shah, O. J. (2017). Histopathological study of neoplastic lesions of large intestine in Kashmir Valley, India. International Journal of Research in Medical Sciences, 2(3), Fenn, L., & Nora, H. (1968). Carcinoma of the large bowel-advances in proctology. 11. Bouchier, I. A. (Ed.). (1984). Textbook of gastroenterology. Baillière Tindall. 12. Dukes, C. E. (1932). The classification of cancer of the rectum. The Journal of Pathology and Bacteriology, 35(3), Qizilbash, A. H. (1982). Pathologic studies in colorectal cancer. A guide to the surgical pathology examination of colorectal specimens and review of features of prognostic significance. Pathology annual, 17, Silverberg, E. (1981). Cancer statistics, CA: a cancer journal for clinicians, 31(1), 13. Available online: 477
Histopathological Study of Neoplastic lesions of large Intestine in Kashmir Valley, India
 International Research Journal of Medical Sciences ISSN 2320 7353 Histopathological Study of Neoplastic lesions of large Intestine in Kashmir Valley, India Mohsin-ul-Rasool 1, Basharat Mubeen 1, Riyaz-u-Saif
International Research Journal of Medical Sciences ISSN 2320 7353 Histopathological Study of Neoplastic lesions of large Intestine in Kashmir Valley, India Mohsin-ul-Rasool 1, Basharat Mubeen 1, Riyaz-u-Saif
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Clinico-Pathological Study of Endoscopic Gastric Biopsies
 Original Article Clinico-Pathological Study of Endoscopic Gastric Biopsies SumalathaKasturi, Raju Mulaka 2 Associate Professor Department of Pathology Chalmeda Anand Rao Institute of Medical Sciences Karimnagar,
Original Article Clinico-Pathological Study of Endoscopic Gastric Biopsies SumalathaKasturi, Raju Mulaka 2 Associate Professor Department of Pathology Chalmeda Anand Rao Institute of Medical Sciences Karimnagar,
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
ISPUB.COM. A Clinical Study Of Right Iliac Fossa Mass. S K Shetty, M Shankar INTRODUCTION AIMS AND OBJECTIVES
 ISPUB.COM The Internet Journal of Surgery Volume 30 Number 4 S K Shetty, M Shankar Citation S K Shetty, M Shankar.. The Internet Journal of Surgery. 2013 Volume 30 Number 4. Abstract Background and Objectives
ISPUB.COM The Internet Journal of Surgery Volume 30 Number 4 S K Shetty, M Shankar Citation S K Shetty, M Shankar.. The Internet Journal of Surgery. 2013 Volume 30 Number 4. Abstract Background and Objectives
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema
 Bahrain Medical Bulletin, Vol.24, No.3, September 2002 Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema Najeeb S Jamsheer, MD, FRCR* Neelam. Malik, MD, MNAMS** Objective: To
Bahrain Medical Bulletin, Vol.24, No.3, September 2002 Frequency of Diagnosis of Colorectal Cancer with Double Contrast Barium Enema Najeeb S Jamsheer, MD, FRCR* Neelam. Malik, MD, MNAMS** Objective: To
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Shore Medical Center Site-Specific Study: Colorectal Cancer 2013
 Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
In-situ and invasive carcinoma of the colon in patients with ulcerative colitis
 Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Prognosis after Treatment of Villous Adenomas
 Prognosis after Treatment of Villous Adenomas of the Colon and Rectum JOHN CHRISTIANSEN, M.D., PREBEN KIRKEGAARD, M.D., JYTTE IBSEN, M.D. With the existing evidence of neoplastic polyps of the colon and
Prognosis after Treatment of Villous Adenomas of the Colon and Rectum JOHN CHRISTIANSEN, M.D., PREBEN KIRKEGAARD, M.D., JYTTE IBSEN, M.D. With the existing evidence of neoplastic polyps of the colon and
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Value of sigmoidoscopy and biopsy in detection of
 Gut, 1979, 20, 575-580 Value of sigmoidoscopy and biopsy in detection of carcinoma and premalignant change in ulcerative colitis R. H. RIDDELL' AND B. C. MORSON From the Department ofpathology, St. Marks
Gut, 1979, 20, 575-580 Value of sigmoidoscopy and biopsy in detection of carcinoma and premalignant change in ulcerative colitis R. H. RIDDELL' AND B. C. MORSON From the Department ofpathology, St. Marks
COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION.
 The West London Medical Journal 2009 Vol No 1 pp 23-31 COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION. Competing interests: None declared ABSTRACT Sarah
The West London Medical Journal 2009 Vol No 1 pp 23-31 COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION. Competing interests: None declared ABSTRACT Sarah
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
A Study of Various Histopathological Types of Colorectal Carcinomas
 ISSN (Online): 2393-915X; (Print): 2454-7379 IJCMR 1330 ORIGINAL RESEARCH A Study of Various Histopathological Types of Colorectal Carcinomas Shashi Kiran K 1, V. Hari Shanker 2, Triveni Bhopal 3, Kandukuri
ISSN (Online): 2393-915X; (Print): 2454-7379 IJCMR 1330 ORIGINAL RESEARCH A Study of Various Histopathological Types of Colorectal Carcinomas Shashi Kiran K 1, V. Hari Shanker 2, Triveni Bhopal 3, Kandukuri
Scholars Journal of Applied Medical Sciences (SJAMS)
") Scholars Journal of Applied Medical Sciences (SJAMS) Abbreviated Key Title: Sch. J. App. Med. Sci. Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India www.saspublisher.com
Scholars Journal of Applied Medical Sciences (SJAMS) Abbreviated Key Title: Sch. J. App. Med. Sci. Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India www.saspublisher.com
Histopathological Study of Lacrimal Gland Tumors
 ORIGINAL ARTICLE Pratikkumar B. Desai 1, Ami Shah 2 1 4 th Year Resident, Pathology Department, B.J.Medical College, Civil Hospital, Ahmedabad 2 Associate Professor, M. J. Institute of Ophthalmology, Civil
ORIGINAL ARTICLE Pratikkumar B. Desai 1, Ami Shah 2 1 4 th Year Resident, Pathology Department, B.J.Medical College, Civil Hospital, Ahmedabad 2 Associate Professor, M. J. Institute of Ophthalmology, Civil
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colon Cancer , The Patient Education Institute, Inc. oc Last reviewed: 05/17/2017 1
 Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
HISTOMORPHOLOGICAL SPECTRUM OF BREAST LESIONS
 HISTOMORPHOLOGICAL SPECTRUM OF BREAST LESIONS Kiran H. S, Jayaprakash Shetty, Chandrika Rao Assistant Professor, Department of Pathology, Yenepoya Medical College, Mangalore. Professor, Department of Pathology,
HISTOMORPHOLOGICAL SPECTRUM OF BREAST LESIONS Kiran H. S, Jayaprakash Shetty, Chandrika Rao Assistant Professor, Department of Pathology, Yenepoya Medical College, Mangalore. Professor, Department of Pathology,
Clinicopathological Characteristics of Superficial Type
 Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Endoscopic Detection and Removal of Recto-sigmoid Myomatous (Leiomyoma) Tumour
 Tumour") Article ID: ISSN 2046-1690 Endoscopic Detection and Removal of Recto-sigmoid Myomatous (Leiomyoma) Tumour Author(s):Mr. Sridhar Dharamavaram, Dr. Ritu Kamra, Dr. Anu Priya, Mr. Rajiva Ranjan Das Corresponding
Article ID: ISSN 2046-1690 Endoscopic Detection and Removal of Recto-sigmoid Myomatous (Leiomyoma) Tumour Author(s):Mr. Sridhar Dharamavaram, Dr. Ritu Kamra, Dr. Anu Priya, Mr. Rajiva Ranjan Das Corresponding
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
BOWEL CANCER. Causes of bowel cancer
 A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Purpose. Encourage standard exchange of data between two key public health partners
 Reporting Pathology Protocols for Colorectal Cancer 2005 NAACCR Conference: June 9, 2005 Ken Gerlach: CDC-NPCR Bette Smith: Ohio Cancer Registry Kathleen Davidson-Allen: PHI/California Cancer Registry
Reporting Pathology Protocols for Colorectal Cancer 2005 NAACCR Conference: June 9, 2005 Ken Gerlach: CDC-NPCR Bette Smith: Ohio Cancer Registry Kathleen Davidson-Allen: PHI/California Cancer Registry
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Outcome High Priority
 MEASURE TYPE: Outcome High Priority") Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Colorectal Cancer Care
 Colorectal Cancer Care A Cancer Care Map for Patients Understanding the process of care that a patient goes through in the diagnosis and treatment of colorectal cancer in BC. ROUND2.3_CRCa_20pages_5.5x8.5_FINAL.indd
Colorectal Cancer Care A Cancer Care Map for Patients Understanding the process of care that a patient goes through in the diagnosis and treatment of colorectal cancer in BC. ROUND2.3_CRCa_20pages_5.5x8.5_FINAL.indd
Incidence and Multiplicities of Adenomatous Polyps in TNM Stage I Colorectal Cancer in Korea
 Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
BOWEL CANCER. Cancer information.
 BOWEL CANCER Cancer information www.cancervic.org.au What is bowel cancer? Bowel cancer is the second most common cancer in both men and women in Australia1 and is more common in people over the age of
BOWEL CANCER Cancer information www.cancervic.org.au What is bowel cancer? Bowel cancer is the second most common cancer in both men and women in Australia1 and is more common in people over the age of
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
AMSER Rad Path Case of the Month: December 2018
 AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
Colonic adenomas-a colonoscopy survey
 Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Malignant colorectal polyps: venous invasion and
 774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
GATTEX (Teduglutide) for Injection REMS Program: Prescriber Education
 for Injection REMS Program: Prescriber Education") GATTEX (Teduglutide) for Injection REMS Program: Prescriber Education Shire-NPS Pharmaceuticals, Inc. 300 Shire Way, Lexington, MA 02421 A REMS (Risk Evaluation and Mitigation Strategy) is a program required
GATTEX (Teduglutide) for Injection REMS Program: Prescriber Education Shire-NPS Pharmaceuticals, Inc. 300 Shire Way, Lexington, MA 02421 A REMS (Risk Evaluation and Mitigation Strategy) is a program required
Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
 Case Reports in Medicine Volume 2012, Article ID 340947, 4 pages doi:10.1155/2012/340947 Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
Case Reports in Medicine Volume 2012, Article ID 340947, 4 pages doi:10.1155/2012/340947 Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test
 test") 753 Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test Dr. Abhishek A Mangaonkar *, Dr. A G Valand 1 Intern, Grant Medical College and Sir J.J. Group of Hospitals, Mumbai, India 2 Professor,
753 Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test Dr. Abhishek A Mangaonkar *, Dr. A G Valand 1 Intern, Grant Medical College and Sir J.J. Group of Hospitals, Mumbai, India 2 Professor,
The Incidence and Significance of Villous Change in Adenomatous Polyps
 The Incidence and Significance Villous Change in Adenomatous Polyps CHRISTOPHER H. K. FUNC, M.D., AND HARVEY GOLDMAN, M.D. Department Pathology, Harvard Medical School and Beth Israel Hospital, Boston,
The Incidence and Significance Villous Change in Adenomatous Polyps CHRISTOPHER H. K. FUNC, M.D., AND HARVEY GOLDMAN, M.D. Department Pathology, Harvard Medical School and Beth Israel Hospital, Boston,
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NPQR Quality Payment Program (QPP) Measures 21_18247_LS.
 Measures 21_18247_LS.") NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Gastrointestinal stromal tumours - clinicopathological study
 Original research article Gastrointestinal stromal tumours - clinicopathological study *Dr. Putrevu Venkata Gurunadha Raju, ** Dr. Kanwaljit Kaur *Professor, **Assistant Professor Department of Pathology,
Original research article Gastrointestinal stromal tumours - clinicopathological study *Dr. Putrevu Venkata Gurunadha Raju, ** Dr. Kanwaljit Kaur *Professor, **Assistant Professor Department of Pathology,
2007 Multiple Primary and
 2007 Multiple Primary and Histology Coding Rules Beyond the Basics Florida Cancer Data System Annual Conference Tampa, FL July 26,2007 Steven Peace, CTR Westat Carol Johnson, CTR NCI SEER Peggy Adamo,
2007 Multiple Primary and Histology Coding Rules Beyond the Basics Florida Cancer Data System Annual Conference Tampa, FL July 26,2007 Steven Peace, CTR Westat Carol Johnson, CTR NCI SEER Peggy Adamo,
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Romanian Journal of Morphology and Embryology 2006, 47(3):
:") Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases
 Original article: The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases Dr Dimple Mehta*,Dr Alpesh Chavda**, Dr Hetal Patel*** *Assistant Professor, **Tutor, ***3
Original article: The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases Dr Dimple Mehta*,Dr Alpesh Chavda**, Dr Hetal Patel*** *Assistant Professor, **Tutor, ***3
Changing Trends of Presentation in Colorectal Carcinoma
 ORIGINAL ARTICLE Changing Trends of Presentation in Colorectal Carcinoma ASHFAQ AHMAD, AMEER AFZAL, HAFIZ MUHAMMAD ASIF, ABHISHEK CHAUDARY, KHALID MASOOD ALAM, ALI AZIM KHAWAJA, MUHAMMAD AZIM KHAWAJA ABSTRACT
ORIGINAL ARTICLE Changing Trends of Presentation in Colorectal Carcinoma ASHFAQ AHMAD, AMEER AFZAL, HAFIZ MUHAMMAD ASIF, ABHISHEK CHAUDARY, KHALID MASOOD ALAM, ALI AZIM KHAWAJA, MUHAMMAD AZIM KHAWAJA ABSTRACT
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Saudi Journal of Pathology and Microbiology (SJPM)
") Saudi Journal of and Microbiology (SJPM) Scholars Middle East Publishers Dubai, United Arab Emirates Website: http://scholarsmepub.com/ ISSN 2518-3362 (Print) ISSN 2518-3370 (Online) Bone Marrow Aspiration
Saudi Journal of and Microbiology (SJPM) Scholars Middle East Publishers Dubai, United Arab Emirates Website: http://scholarsmepub.com/ ISSN 2518-3362 (Print) ISSN 2518-3370 (Online) Bone Marrow Aspiration
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Carcinoembryonic Antigen
 Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Other Names/Abbreviations CEA 190.26 - Carcinoembryonic Antigen Carcinoembryonic antigen (CEA) is a protein polysaccharide found in some carcinomas. It is effective as a biochemical marker for monitoring
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
JMSCR Vol 04 Issue 07 Page July 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i7.47 Lymph Node Aspirations: A Study of Pattern
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i7.47 Lymph Node Aspirations: A Study of Pattern
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4