acute pulmonary coccidioidomycosis Katsunori; Ohkusu, Kiyofumi; Kohno,
|
|
|
- Tobias Norton
- 5 years ago
- Views:
Transcription

1 NAOSITE: Nagasaki University's Ac Title Author(s) Multiple lung abscesses caused by A acute pulmonary coccidioidomycosis Nagaoka, Kentaro; Izumikawa, Koichi Katsunori; Ohkusu, Kiyofumi; Kohno, Citation Journal of Clinical Microbiology, 5 Issue Date URL Right 2012, American Society for Microb This document is downloaded
2 A case of multiple lung abscesses caused by Actinomyces graevenitzii mimicking acute pulmonary coccidioidomycosis Kentaro Nagaoka a,b,1, Koichi Izumikawa a,1, Yoshihiro Yamamoto a, Katsunori Yanagihara a,b, Kiyofumi Ohkusu c, Shigeru Kohno a a Department of Molecular Microbiology and Immunology, b Department of Laboratory Medicine, Nagasaki University Graduate School of Biomedical Sciences, Nagasaki, Japan c Department of Microbiology, Gifu University Graduate School of Medicine, Gifu, Japan 1 These authors contributed equally to this work. Corresponding author: Koichi Izumikawa Department of Molecular Microbiology and Immunology, Nagasaki University Graduate School of Biomedical Sciences, Sakamoto, Nagasaki , Japan.
3 Tel: ; Fax: Running title: Multiple lung abscesses by Actinomyces. graevenitzii Keywords: Actinomyces graevenitzii, lung abscess, pulmonary actinomycosis
4 Abstract Actinomyces graevenitzii is a newly recognized Actinomyces species, that is seldom isolated from clinical specimens. A case of multiple pulmonary abscesses mimicking acute pulmonary coccidioidomycosis is described in this study, and the findings indicate that this organism as an opportunistic human pathogen. (41 words) Case Report: A 38-year-old apparently healthy woman complained of fever and dry cough after visiting Los Angeles, California. Her medical history did not reveal any specific illness, including acquired-immune deficiency syndrome. She did not smoke or consume alcohol. During her 3-day stay, she visited the beach in California. On her way to the beach, she encountered a dust storm and inhaled a large amount of dust. Seven days after she returned to Japan (9 days after encountering the dust storm), she was admitted to a local hospital in Nagasaki owing to a progressive dry cough (clinical day 8). On admission, the vital signs of the patient were as follows: body temperature, 37.5 ; blood
5 pressure, 99/64 mm Hg; pulse, 72 beats/min with a regular rhythm; SpO2, 96% in a room air condition; and respiratory rate, 16 breaths/min. Cyanosis, cardiac murmur, and breath sounds were absent. Moreover, her liver, spleen and lymph nodes were not palpable. Her white blood cell count was /ml, with a shift to the left (71% neutrophils), and her C-reactive protein value was 5 mg/dl (normal range, mg/dl). The chest computed tomography (CT) images revealed multiple round lesions located on both lobes, with diameters of cm (Figures 1 and 2). The radiological findings strongly suggested metastatic tumors; hence, digestive tract endoscopy and positron emission tomography (PET) of the entire body were performed. No other lesions, except the lesions in the lungs, were found to contribute to the findings. Two weeks later (clinical day 21), the multiple pulmonary lesions had grown in size by 3-fold, with partial cavity formation (Figures 1 and 2). Owing to the extreme rapid progression of the lesions, the patient was transferred to our hospital for further examination and treatment. An oral antibiotic, faropenem (FRPM), at 600 mg/day was given from clinical day 21 to 24. On admission (clinical day 25), we suspected acute pulmonary coccidioidomycosis because of her travel history to the US West Coast and
6 the similarities of her CT images with those of typical pulmonary Coccidioides infection, (3 and we administered liposomal amphotericin B (L-AMB) at 150 mg/day intravenously on clinical day 26. We also initiated tazobactam/piperacillin (TAZ/PIPC) therapy at 18 g/day concurrently because the presence of other bacterial infections was not completely excluded. Before the initiation of antibiotic therapy, a transbronchial biopsy (TBB) using endobronchial ultrasonography with a guide sheath was performed 48 h after the cessation of FRPM treatment. The presence of antibodies against Coccidioides was also examined before the initiation of antifungal treatment (clinical day 26). After 9 days of treatment (clinical day 35), her fever subsided, but the pulmonary lesions that were observed on radiological examination had not improved. Primary culturing of bronchoalveolar lavage fluid (BALF) was performed with blood and chocolate agar plates. BALF (inoculum volume, 5 μl) was streaked onto the plate quantitatively and incubated at 37 C in 5% CO2. Only molar tooth-like colonies were observed in 3 days. Hemolysis around the colonies was not observed, and the quantitative culture yielded CFU/mL. The organism was a coryneform gram-positive rod that did not
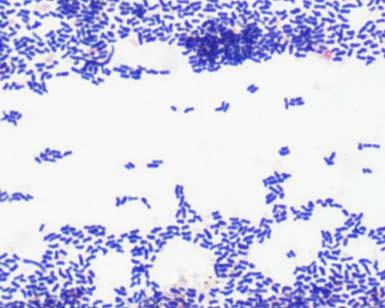
7 produce catalase. On commercial biochemical testing (ID panel; Phoenix Automated Microbiology System, Becton Dickinson Co., Ltd., Japan), the organism was initially identified as Erysipelothrix rhusiopathiae, contrary to its colony characteristics. Upon repeated biochemical testing, the isolate was reidentified as Arcanobacterium haemolyticum. The microphotographs and colony characteristics of the organism isolated from the BALF are shown in Figure 3. The MIC values of the tested antibiotics, including penicillin G, ampicillin, piperacillin, cefotiam, cefotaxime, ceftizoxime, ceftazidime, ceftriaxone, cefepime, imipenem, meropenem, erythromycin, and clarithromycin were found to be less than 0.05 μg/ml. Only minocycline had an MIC value of 4 μg/ml. Results of the acid-fast staining and PCR testing of the patient s BALF for Mycobacterium tuberculosis, M. avium, and M. intracellulare were negative. Although a gram-positive rod bacterium was isolated from the BALF cultures, the histological findings of the TBB specimen could only reveal nonspecific inflammation. Thus, there was a possibility of coinfection with other etiologic pathogens. The Coccidioides antibody was not detected on clinical day 32. However, owing to her unique travel history and radiological
8 findings, we could not completely exclude the possibility of acute pulmonary coccidioidomycosis. Therefore, we performed an additional histological assessment and repetitive examinations for detection of Coccidioides antibody to confirm the diagnosis. On clinical day 36, video-assisted thoracoscopic surgery (VATS) was performed to acquire lung tissue. During VATS, the nodule (30 mm) in the right lower lobe was resected and examined. On histological examination, lymphocyte infiltration, fibrous change, and several Masson bodies were found within the resected nodule, but no pathogen, including Coccidioides, was identified by pathological or microbiological examination. On clinical day 53, after confirming the result of VATS and obtaining negative results for the repetitive tests for serum antibody against Coccidioides, we replaced TAZ/PIPC and L-AMB with amoxicillin (AMPC) therapy at 2 g/day. After 2 months of administration, the pulmonary abscesses were no longer detected on radiological examination. Because of the rarity of her clinical course, we performed molecular identification by PCR amplification and sequencing analysis of the 16S rrna gene using DNA extracted from the isolates. The universal primers 8UA (5 -AGAGTTTGATCMTGGCTCAG-3 ) and 1485B
9 (5 -ACGGGCGGTGTGTRC-3 ) were used, as described previously. (9 We performed a sequencing analysis using a GenBank BLAST search and BiBi ( phylogenetic tools. The sequence of the 16S rrna gene showed 99.7% identity (1403 base pairs [bp] over the entire 1407-bp fragment) with that of the type strain Actinomyces graevenitzii (CCUG27294, Genbank accession no. AJ ). On the basis of this result, we identified the isolate as A. graevenitzii. Discussion: Actinomyces spp. are the most common commensal anaerobic bacterium in the human oral cavity, and 6 species of this genus are considered pathogenic in humans: A. israeli, A. naeslundii, A. odontolyticus, A. viscosus, A. meyeri and A. gerencseriae. (8,13 Pulmonary actinomycosis is well known as a cause of chronic infection, and it constitutes 15% of the total burden of actinomycosis in humans. (8 The clinical features usually include low-grade inflammation with indolent advancement, which is similar to the presentation of fungal infection or lung neoplasms. (8 Several reports (7,8,15 found that 25% 49% of cases of pulmonary actinomycosis were suspected to be lung malignancy upon hospital admission, and the mean duration of illness before a definitive
10 diagnosis was 2 6 months. A diagnosis of pulmonary actinomycosis is often confirmed by histological findings, which reflect chronic inflammation consisting of granulomatous change with sulfur granules. (6 Bacterial confirmation of a clinicopathological diagnosis is usually obtained in <50% of cases owing to inadequate culturing techniques, previous antibiotic therapy, and bacterial overgrowth. (1 Song et al. (15 found that positive culture results were obtained in only 3 of 40 cases of pulmonary actinomycosis. Thus, the diagnosis of conventional pulmonary actinomycosis requires a combination of several factors, including respiratory specimen culture, correlation with clinical and radiological features, histological findings, and response to antibiotic treatment. In addition to these traditional actinomycotic forms, some coryneform anaerobic bacteria have also recently been assigned to the genus Actinomyces by the US Centers for Disease Control. (4,5 A. graevenitzii is a newly recognized Actinomyces sp. that was first isolated from 4 clinical human specimens in 1997 by Ramos et al. (11 It is a filamentous gram-positive rod with no catalase production and is facultatively anaerobic with a distinct biochemical profile. (11 Sarkonen et al. isolated A. graevenitzii from failed
11 dental implant surfaces for their study on the distribution of Actinomyces spp. in 33 dental implant fixtures. (12 Similar to other Actinomyces spp., A. graevenitzi is possibly a component of the oropharyngeal flora. Very little is known about the clinical features and pathogenesis of A. graevenitzii, (14 and only 1 case report has described the disseminated infection of A. graevenitzii, which showed coinfection with Mycobacterium tuberculosis. (16 Our case presented different clinical features of conventional pulmonary actinomycosis, such as the rapid progression of lung lesions and the lack of specific histological features, including granulomatous change or presence of sulfur granules. Acute pulmonary coccidioidomycosis was first suspected because of the patient s travel history to an endemic area of coccidioidomycosis, and the radiological features of multiple round shadows predominantly located in the lower lobes. A histological examination of lung specimens by VATS was necessary for definite differentiation. Although the pathogen could not be identified by histological examination, the quantitative culture of BALF yielding CFU/mL organisms supports the diagnosis of infection by A. graevenitzii as the etiological pathogen present in the patient s lesions. Quantitative culturing of BALF is one of
12 the most reliable methods for differentiating respiratory tract pathogens from colonization related to pneumonia, particular for organisms that can colonize the respiratory tract. (2,10 Because the progression of the lung lesions in our case was more rapid than that of conventional pulmonary actinomycosis, the histological findings revealed acute inflammatory change, which is different from the features of typical pulmonary actinomycosis. As our patient was a 32-year-old previously healthy woman with no known predisposing conditions, the rapid growth of pulmonary actinomycosis in our case was assumed to be due to pathogenic factors rather than host factors. Interestingly, the strain of A. graevenitzii isolated in our case formed molar tooth-like colonies within h of incubation. Its growth rate is faster than that of other Actinomyces spp. that can be cultured anaerobically for up to 3 weeks. (17 We presume that the rapid growth of A. graevenitzi in aerobic conditions may contribute to rapidly progressive pneumonia. However, the reason for the rapid growth of the pulmonary lesion in this patient is unknown. To our knowledge, this is the first report describing multiple lung abscesses caused by A. graevenitzii, which was diagnosed using a quantitative culture
13 of BALF. In our patient, a PET examination before treatment revealed that the lesions were located only in the lungs. Combined with the onset of clinical manifestation after inhalation of dust on a US beach, it could be considered that the pulmonary multiple abscesses were caused by the entry of the pathogens to the lungs via the respiratory tract as opposed to hematogenous infection. As the habitat of A. graevenitzii is unknown, further caution is necessary for this organism, in particular when differentiation of such cases is required from those of acute pulmonary abscesses developing after the inhalation of soil, such as in cases of acute pulmonary coccidioidomycosis. In conclusion, we report a unique case of lung abscesses caused by A. graevenitzii that resembled pulmonary coccidioidomycosis in its clinical features and CT findings. Because of its rarity, the documentation of more cases is required to define the pathogenesis of A. graevenitzii. Acknowledgement The identification of A. graevenitzii using the molecular method described in this study was partially funded by a grant from the Global Centers of
14 Excellence Program, Nagasaki University. References 1) Bennhoff, D. F Actinomycosis: diagnostic and therapeutic consideration and a review of 32 cases. Laryngoscope. 94: ) Canadian Critical Care Trials Group A randomized trial of diagnostic techniques for ventilator-associated pneumonia. N. Engl. J. Med. 355: ) Capone, D., et al Acute pulmonary coccidiodomycosis: CT findings from 15 patients. Br. J. Radiol. 81: ) Finegold, S. M., H. Jousimies-Somer Recently described clinically important bacteria: medical aspects. Clin. Infect. Dis. 25(Suppl. 2): S88-S93. 5) Funke, G., A. von Graevenitz Infections due to Actinomyces neuii (former CDC coryneform group 1 bacteria). Infection. 23: ) Kim, T. S., et al Thoracic actinomycosis: CT features with histopathologic correlation. Am. J. Roentgenol. 186: ) Kolditz, M., et al Medical management of pulmonary actinomycosis: data from 49 consecutive cases. J. Antimicrob. Chemother. 63:
15 8) Mabeza, G. F., J. Macfarlane Pulmonary actinomycosis. Eur. Respir. J. 21: ) Masaki, T., et al Mycobacterium kumamotonense sp. nov. recovered from clinical specimen and the first isolation report of Mycobacterium arupense in Japan: Novel slowly growing, nonchromogenic clinical isolates related to Mycobacterium terrae complex. Microbiol. Immunol. 50: ) Niederman, M The argument against using quantitative cultures in clinical trials and for the management of ventilator-associated pneumonia. Clin. Infect. Dis. 51(Suppl 1): ) Ramos, C. P., et al Actinomyces graevenitzii sp. Nov., Isolated from human clinical specimens. Int. J. Syst. Bacteriol. 47: ) Sarkonen, N., et al Characterization of Actinomyces species isolated from failed dental implant fixtures. Anaerobe. 11: ) Smego, R. A., G. Foglia Actinomycosis. Clin. Infect. Dis. 26: ) Smith, A. J., V. Hall, B. Thakker, C. G. Gemmell Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J Antimicrob. Chemother. 56:
16 15) Song, J. U., et al Treatment of thoracic actinomycosis: A retrospective analysis of 40 patients. Ann. Thorac. Med. 5: ) Tietz, A., K. E. Aldridge, J. E. Figueroa Disseminated coinfection with Actinomyces graevenitzii and mycobacterium tuberculosis: Case report and review of the literature. J. Clin. Microbiol. 43: ) Wong VK, Turmezei TD, Weston VC Actinomycosis. BMJ. 343:d6099. Figure Legends: Figure 1. Chest radiography film images: (A) 2 weeks before admission (clinical day 8), showing several nodules in the bilateral lower lung field; (B) on admission (clinical day 25), showing enlargement of the lung nodules, as the bilateral lower lung field is almost entirely covered by the lesions. Figure 2. Chest CT image of the thorax (A) 2 weeks before admission (clinical day 8), showing multiple round lesions located in both lobes with diameters of 1 2 cm; (B) on admission (clinical day 25), showing increases in the number and size (diameters of 2 4 cm) of the lung nodules.
17 Figure 3. Microphotographs and colony morphological features of the organism isolated from the bronchoalveolar lavage. Panel A shows numerous coryneform gram-positive rods (Gram stain). Panel B shows the molar tooth-like appearance of the colonies on blood agar (72 h after incubation).

18 Figure 1 A B


19 Figure 2 A B

20 Figure 3 A B
Actinomycosis of Thoracic Spine A Rare Case
 Actinomycosis of Thoracic Spine A Rare Case Nanda Patil 1, Avinash Mane 2, Rashmi L. Sonawane 3, Suchi Gadhiya 4 Abstract: Introduction: Actinomycosis is a chronic suppurative infection caused by Actinomyces
Actinomycosis of Thoracic Spine A Rare Case Nanda Patil 1, Avinash Mane 2, Rashmi L. Sonawane 3, Suchi Gadhiya 4 Abstract: Introduction: Actinomycosis is a chronic suppurative infection caused by Actinomyces
Authors: B.S. Leenstra, C.C.M. Schaap, M. Bessems, N.H.M. Renders, K. Bosscha
 Accepted Manuscript Title: Primary Actinomycosis in the breast caused by Actinomyces neuii. A report of 2 cases Authors: B.S. Leenstra, C.C.M. Schaap, M. Bessems, N.H.M. Renders, K. Bosscha PII: S2214-2509(17)30044-6
Accepted Manuscript Title: Primary Actinomycosis in the breast caused by Actinomyces neuii. A report of 2 cases Authors: B.S. Leenstra, C.C.M. Schaap, M. Bessems, N.H.M. Renders, K. Bosscha PII: S2214-2509(17)30044-6
ESCMID Online Lecture Library. by author
 Actinomyces species: Clinical aspects and diagnostic possibilities Willem Manson Prof. dr. John Degener, dr. Willem Manson University Medical Center Groningen UMCG AIM OF THIS PRESENTATION, to gain knowledge
Actinomyces species: Clinical aspects and diagnostic possibilities Willem Manson Prof. dr. John Degener, dr. Willem Manson University Medical Center Groningen UMCG AIM OF THIS PRESENTATION, to gain knowledge
Upper Respiratory Infections. Mehreen Arshad, MD Assistant Professor Pediatric Infectious Diseases Duke University
 Upper Respiratory Infections Mehreen Arshad, MD Assistant Professor Pediatric Infectious Diseases Duke University Disclosures None Objectives Know the common age- and season-specific causes of pharyngitis
Upper Respiratory Infections Mehreen Arshad, MD Assistant Professor Pediatric Infectious Diseases Duke University Disclosures None Objectives Know the common age- and season-specific causes of pharyngitis
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Actinomycosis A Common Incidental Diagnosis at Different Sites
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 2 Ver. V (February. 2017), PP 61-65 www.iosrjournals.org Actinomycosis A Common Incidental
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 2 Ver. V (February. 2017), PP 61-65 www.iosrjournals.org Actinomycosis A Common Incidental
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
RHODOCOCCUS EQUI. Post-mortem Environmental Persistence Specific Control Measures Release of Animals from Isolation
 RHODOCOCCUS EQUI Definition Clinical Signs Transmission Diagnostic Sampling, Testing and Handling Post-mortem Environmental Persistence Specific Control Measures Release of Animals from Isolation Biosecurity
RHODOCOCCUS EQUI Definition Clinical Signs Transmission Diagnostic Sampling, Testing and Handling Post-mortem Environmental Persistence Specific Control Measures Release of Animals from Isolation Biosecurity
Actinomyces neuii, An Uncommon Bacterial Isolate From A Neck Abscess Lei Li 1, Amitabh Gautam 2 and Nancy S. Miller 1 *
 Actinomyces neuii, An Uncommon Bacterial Isolate From A Neck Abscess Lei Li 1, Amitabh Gautam 2 and Nancy S. Miller 1 * Authors details: 1 Department of Pathology and Laboratory Medicine, 670 Albany Street,
Actinomyces neuii, An Uncommon Bacterial Isolate From A Neck Abscess Lei Li 1, Amitabh Gautam 2 and Nancy S. Miller 1 * Authors details: 1 Department of Pathology and Laboratory Medicine, 670 Albany Street,
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review
 Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
Showa Univ J Med Sci 28 4, 373 377, December 2016 Case Report Clarithromycin-resistant Mycobacterium Shinjukuense Lung Disease: Case Report and Literature Review Makoto HAYASHI 1, Satoshi MATSUKURA 1,
Fungal Diseases of the Respiratory System
 Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
CERVICOFACIAL ACTINOMYCOSIS: REPORT OF TWO CASES
 Nagoya J. Med. Sci. 55. 83-88, 1993 CERVICOFACIAL ACTINOMYCOSIS: REPORT OF TWO CASES MICHIO KAWAI, HIDEKI MIZUTANI, MINORU VEDA, TAKESHI HOSHINO l and TOSHIO KANEDA Department of Oral Surgery and JDepartment
Nagoya J. Med. Sci. 55. 83-88, 1993 CERVICOFACIAL ACTINOMYCOSIS: REPORT OF TWO CASES MICHIO KAWAI, HIDEKI MIZUTANI, MINORU VEDA, TAKESHI HOSHINO l and TOSHIO KANEDA Department of Oral Surgery and JDepartment
Disseminated Coinfection with Actinomyces graevenitzii and Mycobacterium tuberculosis: Case Report and Review of the Literature
 JOURNAL OF CLINICAL MICROBIOLOGY, June 2005, p. 3017 3022 Vol. 43, No. 6 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.6.3017 3022.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
JOURNAL OF CLINICAL MICROBIOLOGY, June 2005, p. 3017 3022 Vol. 43, No. 6 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.6.3017 3022.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
Actinomycosis and aspergillosis in the nose of a diabetic: A case report
 Volume 2 Issue 3 2012 ISSN 2250-0359 Actinomycosis and aspergillosis in the nose of a diabetic: A case report 1 Meenu Khurana Cherian 1*, Rajarajeswari 2 1 Department of ENT, Gulf Medical College Hospital
Volume 2 Issue 3 2012 ISSN 2250-0359 Actinomycosis and aspergillosis in the nose of a diabetic: A case report 1 Meenu Khurana Cherian 1*, Rajarajeswari 2 1 Department of ENT, Gulf Medical College Hospital
Subcutaneous Fungi 10/13/2009. General Characteristics. Pathogenesis. Epidemiology. Laboratory Diagnosis. Specimens. Growth rate: 1-4 weeks
 General Characteristics Growth rate: 1-4 weeks Subcutaneous Fungi Clinical Laboratory Science Program Carol Larson MSEd, MT(ASCP) Dematiaceous septate hyphae Hyaline septate hyphae Branching GPR Epidemiology
General Characteristics Growth rate: 1-4 weeks Subcutaneous Fungi Clinical Laboratory Science Program Carol Larson MSEd, MT(ASCP) Dematiaceous septate hyphae Hyaline septate hyphae Branching GPR Epidemiology
Labquality External Quality Assessment Programmes General Bacteriology 1 3/2014
 Labquality External Quality Assessment Programmes General Bacteriology 1 3/2014 Photos and text: Markku Koskela, M.D., Ph.D. Clinical microbiology specialist Nordlab Oulu, Finland Specimen 31/2014 Abscess
Labquality External Quality Assessment Programmes General Bacteriology 1 3/2014 Photos and text: Markku Koskela, M.D., Ph.D. Clinical microbiology specialist Nordlab Oulu, Finland Specimen 31/2014 Abscess
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Yersinia pestis. Yersinia and plague. Dr. Hala Al Daghistani
 Yersinia pestis Dr. Hala Al Daghistani Yersinia species Short, pleomorphic gram-negative rods that can exhibit bipolar staining. Catalase positive, and microaerophilic or facultatively anaerobic. Animals
Yersinia pestis Dr. Hala Al Daghistani Yersinia species Short, pleomorphic gram-negative rods that can exhibit bipolar staining. Catalase positive, and microaerophilic or facultatively anaerobic. Animals
Available from December &volume=3&issue=6&page= &id=456
 JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH How to cite this article: GOLSHA R,NAJAFI L,REZAEI-SHIRAZI R,VAKILINEJHAD M,MORTAZAVI B, ROSHANDEL G.ACTINOMYCOSIS MAY BE PRESENTED IN UNUSUAL ORGANS: A REPORT
JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH How to cite this article: GOLSHA R,NAJAFI L,REZAEI-SHIRAZI R,VAKILINEJHAD M,MORTAZAVI B, ROSHANDEL G.ACTINOMYCOSIS MAY BE PRESENTED IN UNUSUAL ORGANS: A REPORT
Laryngologica is available online a. ume=126&issue=9&spage=1001.
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation A case of actinomycosis causing uni Takasaki, Kenji; Kitaoka, Kyoko; Ka Abe, Kuniko; Takahashi, Haruo Acta oto-laryngologica. 126(9), pp. Issue
NAOSITE: Nagasaki University's Ac Title Author(s) Citation A case of actinomycosis causing uni Takasaki, Kenji; Kitaoka, Kyoko; Ka Abe, Kuniko; Takahashi, Haruo Acta oto-laryngologica. 126(9), pp. Issue
Nontuberculous Mycobacterial Lung Disease
 Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Persistent Spontaneous Pneumothorax for Four Years: A Case Report
 303) Persistent Spontaneous Pneumothorax for Four Years: A Case Report Mizuno Y., Iwata H., Shirahashi K., Matsui M., Takemura H. Department of General and Cardiothoracic Surgery, Graduate School of Medicine,
303) Persistent Spontaneous Pneumothorax for Four Years: A Case Report Mizuno Y., Iwata H., Shirahashi K., Matsui M., Takemura H. Department of General and Cardiothoracic Surgery, Graduate School of Medicine,
Pseudo-Outbreak of Actinomyces graevenitzii Associated with Bronchoscopy
 JCM Accepts, published online ahead of print on 29 October 2014 J. Clin. Microbiol. doi:10.1128/jcm.02302-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 1 Pseudo-Outbreak
JCM Accepts, published online ahead of print on 29 October 2014 J. Clin. Microbiol. doi:10.1128/jcm.02302-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 1 Pseudo-Outbreak
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Ventriculoperitoneal Shunt Infection Caused by ACCEPTED. Division of Infectious Diseases, Akron General Medical Center, Akron OH, 1
 JCM Accepts, published online ahead of print on 26 March 2008 J. Clin. Microbiol. doi:10.1128/jcm.02141-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 26 March 2008 J. Clin. Microbiol. doi:10.1128/jcm.02141-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
A Vietnamese woman with a 2-week history of cough
 Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
Delphine Natali 1, Hai Tran Pham 1, Hung Nguyen The 2 delphinenatali@gmail.com Case report A Vietnamese woman with a 2-week history of cough A 52-year-old nonsmoker Vietnamese woman without any past medical
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Common things are common, but not always the answer
 Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Kevin Conroy, Joe Mackenzie, Stephen Cowie kevin.conroy@nhs.net Respiratory Dept, Darlington Memorial Hospital, Darlington, UK. Common things are common, but not always the answer Case report Cite as:
Pulmonary Nocardiosis Caused by Nocardia concava with a Literature Review
 CASE REPORT Pulmonary Nocardiosis Caused by Nocardia concava with a Literature Review Tatsuro Hirayama 1, Takahiro Takazono 1,2, Yoshiro Horai 3, asato Tashiro 2,4, Tomomi Saijo 1,2, Kosuke Kosai 5, Yoshitomo
CASE REPORT Pulmonary Nocardiosis Caused by Nocardia concava with a Literature Review Tatsuro Hirayama 1, Takahiro Takazono 1,2, Yoshiro Horai 3, asato Tashiro 2,4, Tomomi Saijo 1,2, Kosuke Kosai 5, Yoshitomo
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
A case of pulmonary cryptococcosis followed by pleuritis in an apparently. immunocompetent patient during fluconazole treatment
 A case of pulmonary cryptococcosis followed by pleuritis in an apparently immunocompetent patient during fluconazole treatment KOICHI IZUMIKAWA 1, YONG ZHAO 1, KOHEI MOTOSHIMA 1, TAKAHIRO TAKAZONO 1, TOMOMI
A case of pulmonary cryptococcosis followed by pleuritis in an apparently immunocompetent patient during fluconazole treatment KOICHI IZUMIKAWA 1, YONG ZHAO 1, KOHEI MOTOSHIMA 1, TAKAHIRO TAKAZONO 1, TOMOMI
Multi-clonal origin of macrolide-resistant Mycoplasma pneumoniae isolates. determined by multiple-locus variable-number tandem-repeat analysis
 JCM Accepts, published online ahead of print on 30 May 2012 J. Clin. Microbiol. doi:10.1128/jcm.00678-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Multi-clonal origin
JCM Accepts, published online ahead of print on 30 May 2012 J. Clin. Microbiol. doi:10.1128/jcm.00678-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Multi-clonal origin
MYCOBACTERIA. Pulmonary T.B. (infect bird)
") MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Lung Abscess due to Clostridium barati in a Patient with Invasive Pulmonary Aspergillosis ACCEPTED
 JCM Accepts, published online ahead of print on 3 January 2008 J. Clin. Microbiol. doi:10.1128/jcm.02446-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 3 January 2008 J. Clin. Microbiol. doi:10.1128/jcm.02446-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
Actinomycosis with pericardio-pleural effusion and ascites. A Rare presentation
 Actinomycosis with pericardio-pleural effusion and ascites. A Rare presentation Article by Naresh Sen 1, Sonal Tanwar 2 1 Anand Multispeciality Hospital, Beawar, Rajasthan (India) Email id- drnaresh.sen@gmail.com
Actinomycosis with pericardio-pleural effusion and ascites. A Rare presentation Article by Naresh Sen 1, Sonal Tanwar 2 1 Anand Multispeciality Hospital, Beawar, Rajasthan (India) Email id- drnaresh.sen@gmail.com
Terumitsu; Nagayasu, Takeshi
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
Emergence of Klebsiella pneumoniae ST258 with KPC-2 in Hong Kong. Title. Ho, PL; Tse, CWS; Lai, EL; Lo, WU; Chow, KH
 Title Emergence of Klebsiella pneumoniae ST258 with KPC-2 in Hong Kong Author(s) Ho, PL; Tse, CWS; Lai, EL; Lo, WU; Chow, KH Citation International Journal Of Antimicrobial Agents, 2011, v. 37 n. 4, p.
Title Emergence of Klebsiella pneumoniae ST258 with KPC-2 in Hong Kong Author(s) Ho, PL; Tse, CWS; Lai, EL; Lo, WU; Chow, KH Citation International Journal Of Antimicrobial Agents, 2011, v. 37 n. 4, p.
Work up of Respiratory & Wound Cultures:
 Work up of Respiratory & Wound Cultures: Culture work up 2 Systematic approaches 1 Work up of Respiratory & Wound Cultures Resident flora Colonizing organisms Pathogens 2 Work up of Respiratory & Wound
Work up of Respiratory & Wound Cultures: Culture work up 2 Systematic approaches 1 Work up of Respiratory & Wound Cultures Resident flora Colonizing organisms Pathogens 2 Work up of Respiratory & Wound
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
International Journal of Pharma and Bio Sciences ACTINOMYCOSIS OF TONSILS INCIDENTAL OR PATHOLOGICAL? A CASE REPORT ABSTRACT
 Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ACTINOMYCOSIS OF TONSILS INCIDENTAL OR PATHOLOGICAL? A CASE REPORT Dr.S.ANU PRIYADHARSHINI* 1, Dr.A.R.SUBHASHREE 2
Case Report Pathology International Journal of Pharma and Bio Sciences ISSN 0975-6299 ACTINOMYCOSIS OF TONSILS INCIDENTAL OR PATHOLOGICAL? A CASE REPORT Dr.S.ANU PRIYADHARSHINI* 1, Dr.A.R.SUBHASHREE 2
A Case of Empyema Thoracis Caused by Actinomycosis
 Med. J. Malaysia Vo!. 47 NoA December 1992 A Case of Empyema Thoracis Caused by Actinomycosis L.N. Hooi, MRCP its. Na, IVfflBS Chest Unit, Penang General Hospital K.S. Sin, BSc Department of Pathology,
Med. J. Malaysia Vo!. 47 NoA December 1992 A Case of Empyema Thoracis Caused by Actinomycosis L.N. Hooi, MRCP its. Na, IVfflBS Chest Unit, Penang General Hospital K.S. Sin, BSc Department of Pathology,
PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Discussion points CLSI M100 S19 Update. #1 format of tables has changed. #2 non susceptible category
 Discussion points 2009 CLSI M100 S19 Update Nebraska Public Health Laboratory Changes most important to routine antimicrobial susceptibility testing. Documents available Janet Hindler discussion slide
Discussion points 2009 CLSI M100 S19 Update Nebraska Public Health Laboratory Changes most important to routine antimicrobial susceptibility testing. Documents available Janet Hindler discussion slide
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Treatment of serious Pseudomonas infections with azlocillin
 Journal of Antimicrobial Chemotherapy (983), Suppl. B, 53-58 Treatment of serious Pseudomonas infections with azlocillin S. Olive, W. J. Mogabgab, B. Holmes, B. Pollock, B. Pauling and R. Beville Tulane
Journal of Antimicrobial Chemotherapy (983), Suppl. B, 53-58 Treatment of serious Pseudomonas infections with azlocillin S. Olive, W. J. Mogabgab, B. Holmes, B. Pollock, B. Pauling and R. Beville Tulane
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Aspergillus species. The clinical spectrum of pulmonary aspergillosis
 Pentalfa 3 maart 2016 The clinical spectrum of pulmonary aspergillosis Pascal Van Bleyenbergh, Pneumologie UZ Leuven Aspergillus species First described in 1729 * >250 species * ubiquitous Inhalation of
Pentalfa 3 maart 2016 The clinical spectrum of pulmonary aspergillosis Pascal Van Bleyenbergh, Pneumologie UZ Leuven Aspergillus species First described in 1729 * >250 species * ubiquitous Inhalation of
Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms
 Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Murine Pulmonary Aspergillosis
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation Efficacy of SPK-843, a Novel Polyen Amphotericin B, Liposomal Amphoteri Murine Pulmonary Aspergillosis Kakeya, Hiroshi; Miyazaki, Yoshitsu Tsutomu;
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Efficacy of SPK-843, a Novel Polyen Amphotericin B, Liposomal Amphoteri Murine Pulmonary Aspergillosis Kakeya, Hiroshi; Miyazaki, Yoshitsu Tsutomu;
Unit II Problem 2 Microbiology Lab: Pneumonia
 Unit II Problem 2 Microbiology Lab: Pneumonia - What are the steps needed to obtain a proper sputum specimen? You need the following: A wide-mouth labeled container. Gloves. Water. Mouth wash + tissues.
Unit II Problem 2 Microbiology Lab: Pneumonia - What are the steps needed to obtain a proper sputum specimen? You need the following: A wide-mouth labeled container. Gloves. Water. Mouth wash + tissues.
Pneumocystis. Pneumocystis BIOL Summer Introduction. Mycology. Introduction (cont.) Introduction (cont.)
 Introduction (cont.)") Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Lumbar Actinomycosis: A Case Report 1
 Lumbar Actinomycosis: A Case Report 1 Min Hee Lee, M.D., Jang Gyu Cha, M.D., Eun Ju Choo, M.D. 2, Kyeong Cheon Jung, M.D. 3, Jai Soung Park, M.D., Sung-Il Park, M.D., Sang Hyun Paik, M.D., Hae Kyung Lee,
Lumbar Actinomycosis: A Case Report 1 Min Hee Lee, M.D., Jang Gyu Cha, M.D., Eun Ju Choo, M.D. 2, Kyeong Cheon Jung, M.D. 3, Jai Soung Park, M.D., Sung-Il Park, M.D., Sang Hyun Paik, M.D., Hae Kyung Lee,
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Dr Marie Bruyneel and Deborah Konopnicki. BVIKM/SBMIC November 8th, 2012
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Actinomycosis is a chronic suppurative infectious
 Case Report 66 Recurrent Life Threatening Massive Hemoptysis as a Presentation of Pulmonary Actinomycosis Kuo-Chin Kao, MD; Yao-Kuang Wu, MD; Chung-Chi Huang, MD; Meng-Jer Hsieh, MD; Ying-Huang Tsai, MD
Case Report 66 Recurrent Life Threatening Massive Hemoptysis as a Presentation of Pulmonary Actinomycosis Kuo-Chin Kao, MD; Yao-Kuang Wu, MD; Chung-Chi Huang, MD; Meng-Jer Hsieh, MD; Ying-Huang Tsai, MD
Medical Bacteriology Lecture 15
 Medical Bacteriology Lecture 15 Gram Negative Coccobacilli Haemophilus Bordetella pertussis Haemophilus "loves heme" small gram-negative coccobacilli, non-spore forming, non-motile, require enriched media
Medical Bacteriology Lecture 15 Gram Negative Coccobacilli Haemophilus Bordetella pertussis Haemophilus "loves heme" small gram-negative coccobacilli, non-spore forming, non-motile, require enriched media
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013
 Stephen Munday, MD MPH Imperial County Public Health May 21, 2013") Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013 Objectives Assess the epidemiology of Coccidioidomycosis (aka Valley Fever) Describe the
Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013 Objectives Assess the epidemiology of Coccidioidomycosis (aka Valley Fever) Describe the
Case Study 2016 Wisconsin Mycobacteriology Laboratory Network Annual Conference November 17, 2016
 Case Study 2016 Wisconsin Mycobacteriology Laboratory Network Annual Conference November 17, 2016 Raymond P. Podzorski, Ph.D, D(ABMM) St. Mary s Hospital Laboratory and Wisconsin Region SSMHealth 608-258-6393
Case Study 2016 Wisconsin Mycobacteriology Laboratory Network Annual Conference November 17, 2016 Raymond P. Podzorski, Ph.D, D(ABMM) St. Mary s Hospital Laboratory and Wisconsin Region SSMHealth 608-258-6393
Making the Right Call With. Pneumonia. Community-acquired pneumonia (CAP) is a. Community-Acquired. What exactly is CAP?
 is a. Community-Acquired. What exactly is CAP?") Making the Right Call With Community-Acquired Pneumonia In this article: By Thomas J. Marrie, MD The case of Allyson Allyson, 32, presented to the emergency department with a 48-hour history of anorexia,
Making the Right Call With Community-Acquired Pneumonia In this article: By Thomas J. Marrie, MD The case of Allyson Allyson, 32, presented to the emergency department with a 48-hour history of anorexia,
A Case of Pediatric Plasma Cell Granuloma
 August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
Diagnostic Approach to Pleural Effusion
 Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
Original Article GCSMC J Med Sci Vol (IV) No (I) January-June 2015 Diagnostic Approach to Pleural Effusion Rushi Patel*, Viral Shah*, Deepali Kamdar** Abstract : Aim : Normally the pleural cavities contain
THIS IS AN OFFICIAL NH DHHS HEALTH ALERT
 THIS IS AN OFFICIAL NH DHHS HEALTH ALERT Distributed by the NH Health Alert Network Health.Alert@nh.gov August 25, 2018 0800 EDT NH-HAN 20180825 Cluster of Legionella pneumophila Pneumonia (Legionnaire
THIS IS AN OFFICIAL NH DHHS HEALTH ALERT Distributed by the NH Health Alert Network Health.Alert@nh.gov August 25, 2018 0800 EDT NH-HAN 20180825 Cluster of Legionella pneumophila Pneumonia (Legionnaire
- Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including
: important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including") KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic
 Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic Hepatocellular Carcinoma Chih-Hao Shen, MD 3, Jung-Chung Lin, MD, PhD 2, Hsuan-Hwai Lin, MD 1, You-Chen Chao, MD 1, and Tsai-Yuan
Early Klebsiella pneumoniae Liver Abscesses associated with Pylephlebitis Mimic Hepatocellular Carcinoma Chih-Hao Shen, MD 3, Jung-Chung Lin, MD, PhD 2, Hsuan-Hwai Lin, MD 1, You-Chen Chao, MD 1, and Tsai-Yuan
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Management of Pleural Effusion
 Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
Management of Pleural Effusion Development of Pleural Effusion pulmonary capillary pressure (CHF) capillary permeability (Pneumonia) intrapleural pressure (atelectasis) plasma oncotic pressure (hypoalbuminemia)
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case Series
 Hindawi Publishing Corporation Case Reports in Pulmonology Volume 2015, Article ID 314831, 6 pages http://dx.doi.org/10.1155/2015/314831 Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case
Hindawi Publishing Corporation Case Reports in Pulmonology Volume 2015, Article ID 314831, 6 pages http://dx.doi.org/10.1155/2015/314831 Case Report Pulmonary Nocardiosis in the Immunocompetent Host: Case
Medical Bacteriology- Lecture 13 Gram Negative Coccobacilli Haemophilus Bordetella
 Medical Bacteriology- Lecture 13 Gram Negative Coccobacilli Haemophilus Bordetella 1 Haemophilus "loves heme" Small gram-negative coccobacilli Non-spore forming Non-motile Growth is enhanced in CO2 Present
Medical Bacteriology- Lecture 13 Gram Negative Coccobacilli Haemophilus Bordetella 1 Haemophilus "loves heme" Small gram-negative coccobacilli Non-spore forming Non-motile Growth is enhanced in CO2 Present
Guiding principles* for treating Mycoplasma pneumoniae pneumonia
 1 Guiding principles* for treating Mycoplasma pneumoniae pneumonia The Committee of Japanese Society of Mycoplasmology Shigeru Kohno (Chair, Nagasaki University) Tadashi Ishida (Kurashiki Central Hospital)
1 Guiding principles* for treating Mycoplasma pneumoniae pneumonia The Committee of Japanese Society of Mycoplasmology Shigeru Kohno (Chair, Nagasaki University) Tadashi Ishida (Kurashiki Central Hospital)
Dose-dependent effects of tobramycin in an animal model of Pseudomonas sinusitis Am J Rhino Jul-Aug; 21(4):423-7
:423-7") AMINOGLYCOSIDES Dose-dependent effects of tobramycin in an animal model of Pseudomonas sinusitis Am J Rhino. 2007 Jul-Aug; 21(4):423-7 http://www.ncbi.nlm.nih.gov/pubmed/17882910 Evaluation of the in-vivo
AMINOGLYCOSIDES Dose-dependent effects of tobramycin in an animal model of Pseudomonas sinusitis Am J Rhino. 2007 Jul-Aug; 21(4):423-7 http://www.ncbi.nlm.nih.gov/pubmed/17882910 Evaluation of the in-vivo
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference. Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2
 June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
PRESENTER: DENNIS NYACHAE MOSE KENYATTA UNIVERSITY
 18/8/2016 SOURCES OF MICROBIAL CONTAMINANTS IN BIOSAFETY LABORATORIES IN KENYA PRESENTER: DENNIS NYACHAE MOSE KENYATTA UNIVERSITY 1 INTRODUCTION Contamination occurs through avoidable procedural errors
18/8/2016 SOURCES OF MICROBIAL CONTAMINANTS IN BIOSAFETY LABORATORIES IN KENYA PRESENTER: DENNIS NYACHAE MOSE KENYATTA UNIVERSITY 1 INTRODUCTION Contamination occurs through avoidable procedural errors
The Surgical Treatment of Tracheobronchial Tuberculosis. The Thoracic Department of Beijing Chest Hospital, Capital Medical University
 The Surgical Treatment of Tracheobronchial Tuberculosis ) The Thoracic Department of Beijing Chest Hospital, Capital Medical University Named also: endobronchial tuberculosis,ebtb defined as tuberculous
The Surgical Treatment of Tracheobronchial Tuberculosis ) The Thoracic Department of Beijing Chest Hospital, Capital Medical University Named also: endobronchial tuberculosis,ebtb defined as tuberculous
Relationships and Emerging Pathogens: Microbiology, Infection Prevention and Public Health Working Together
 Relationships and Emerging Pathogens: Microbiology, Infection Prevention and Public Health Working Together Objectives Using the M. chimaera outbreak as the discussion scenario, explore communication roles
Relationships and Emerging Pathogens: Microbiology, Infection Prevention and Public Health Working Together Objectives Using the M. chimaera outbreak as the discussion scenario, explore communication roles
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Materials and Methods: Literature review and Authors opinion.
 Haffajee AD, Bogren A, Hasturk H et al. Subgingival microbiota of chronic periodontitis subjects from different geographic locations. J Clin Periodontol 2004; 31:996-1002. Purpose: To compare the subgingival
Haffajee AD, Bogren A, Hasturk H et al. Subgingival microbiota of chronic periodontitis subjects from different geographic locations. J Clin Periodontol 2004; 31:996-1002. Purpose: To compare the subgingival
A Rare Case of Pulmonary Actinomycosis Presented as a Pseudotumor Diagnosed after Pneumonectomy: A Case Report and Literature Review
 A Rare Case of Pulmonary Actinomycosis Presented as a Pseudotumor Diagnosed after Pneumonectomy: A Case Report and Literature Review Pichaya Petborom, M.D.*, Prasit Upapan, M.D.** *Division of Pulmonary
A Rare Case of Pulmonary Actinomycosis Presented as a Pseudotumor Diagnosed after Pneumonectomy: A Case Report and Literature Review Pichaya Petborom, M.D.*, Prasit Upapan, M.D.** *Division of Pulmonary
In vitro and Intracellular Activities of Peptide Deformylase. Inhibitor GSK against Legionella pneumophila Isolates
 AAC Accepts, published online ahead of print on 27 October 2014 Antimicrob. Agents Chemother. doi:10.1128/aac.04006-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 2 In vitro
AAC Accepts, published online ahead of print on 27 October 2014 Antimicrob. Agents Chemother. doi:10.1128/aac.04006-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 2 In vitro
Introduction. Study of fungi called mycology.
 Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Clinical Comparative Study of Sulbactam/Ampicillin and Imipenem/Cilastatin in Elderly Patients with Community-Acquired Pneumonia
 ORIGINAL ARTICLE Clinical Comparative Study of Sulbactam/Ampicillin and Imipenem/Cilastatin in Elderly Patients with Community-Acquired Pneumonia Katsunori Yanagihara 1,2, Yuichi Fukuda 1, Masafumi Seki
ORIGINAL ARTICLE Clinical Comparative Study of Sulbactam/Ampicillin and Imipenem/Cilastatin in Elderly Patients with Community-Acquired Pneumonia Katsunori Yanagihara 1,2, Yuichi Fukuda 1, Masafumi Seki
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting
 Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Discrepancies in the recovery of bacteria from multiple sinuses in acute and chronic sinusitis
 Journal of Medical Microbiology (2004), 53, 879 885 DOI 10.1099/jmm.0.45655-0 Short Communication Correspondence Itzhak Brook ib6@georgetown.edu Received 1 March 2004 Accepted 18 May 2004 Discrepancies
Journal of Medical Microbiology (2004), 53, 879 885 DOI 10.1099/jmm.0.45655-0 Short Communication Correspondence Itzhak Brook ib6@georgetown.edu Received 1 March 2004 Accepted 18 May 2004 Discrepancies
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Phenotypic Identification of Actinomyces and Related Species Isolated from Human Sources
 JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2001, p. 3955 3961 Vol. 39, No. 11 0095-1137/01/$04.00 0 DOI: 10.1128/JCM.39.11.3955 3961.2001 Copyright 2001, American Society for Microbiology. All Rights Reserved.
JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2001, p. 3955 3961 Vol. 39, No. 11 0095-1137/01/$04.00 0 DOI: 10.1128/JCM.39.11.3955 3961.2001 Copyright 2001, American Society for Microbiology. All Rights Reserved.