CT Contrast Protocols for Different Organ Imaging
|
|
|
- Zoe Holt
- 6 years ago
- Views:
Transcription
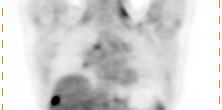
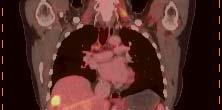
1 CT Contrast Protocols for Different Organ Imaging g Paul Shreve, M.D. Advanced Radiology Services, P.C. & Spectrum Health Grand Rapids, MI, USA Correlative Imaging Council Society of Nuclear Medicine 56 th Annual Meeting Toronto, Canada June 13, 2009
2 PET-CT: CT Contrast Protocols Why use Intravenous Contrast (IV) with PET-CT? To get the best of both worlds PET-CT is PET + CT






3 PET PET/ct PET-CT Emerging understanding Diagnostic AC PET with PET + diagnostic CT for AC PET CT anatomic merged diagnosis exam localization
4 PET-CT Scanners What was PET-CT originally intended to be? It is to be emphasized that the documented objectives of this development was to offer clinical CT and clinical PET scans from a single device; the intended purpose of the CT was to provide clinical patient information and not just attenuation correction and localization alone. David Townsend, Co-Inventor of PET/CT Townsend D. Combined Positron Emission Tomography-Computed Tomography : The Historical Perspective. Seminars in Ultrasound, CT and MR 2008; 29:
5 PET-CT: CT Contrast Protocols Intravenous Contrast (IV) IV contrast do not make a CT diagnostic including in the setting of body oncology imaging. IV contrast is an enhancement making interpretation of the morphologic findings of the CT scan easier and more accurate Use of oral and IV contrast in the setting of PET/CT never really was a problem and was used in the late 1990s at the University of Pittsburgh on the first PET-CT prototype and used by many in 2001 as the first commercial scanners became available.






6 Fully optimized whole torso breath hold CT with oral and IV contrast performed as part of PET/CT exam using one of the first commercial PET/CT scanners in 2001 Antoch, et. al. AJR 2002; 179:
7 PET-CT: CT Contrast Protocols Intravenous Contrast Positively depicts vascular space Enhances soft tissue delineation Depicts internal anatomy of viscera Tumor neo-vascularity can be seen


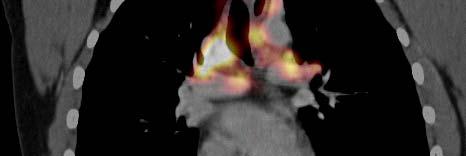
8 Mediastinal lymph nodes, enlarged and non-enlarged, in patient with right hilar mass positive for NSCLC
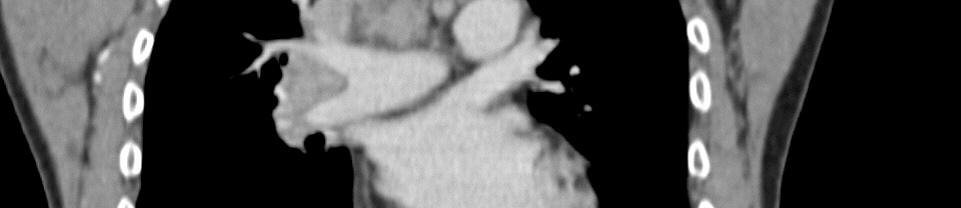
9 Vascular structures and landmarks and soft tissue features depicted by use of intravenous contrast
10 Margins of squamous cell carcinoma depicted on CT by contrast enhancement of tumor neovascularity



11 FDG PET delineates primary lung cancer from post obstructive atelectasis grossly, CT contrast enhancement to within mm
12 PET-CT: CT Contrast Protocols Intravenous Contrast Determining extent of tumor (T staging) is largely dependent on CT findings.
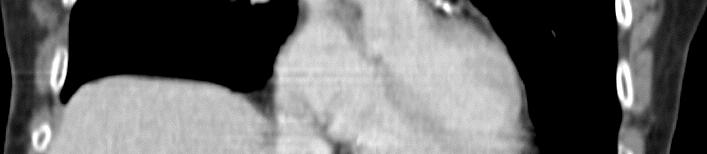
13 Primary lung carcinoma directly invading diaphragm Slides are not into to be reproduced liver without








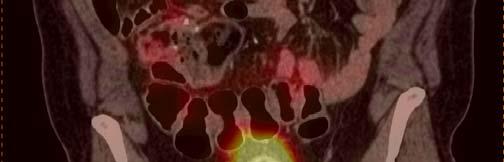
14 Quiet breathing 240 ma with oral and IV contrast and IV fluids and Lasix for urinary tracer washout
15 PET-CT: CT Contrast Protocols Intravenous Contrast Not all cancer is FDG avid, CT requires IV contrast to depict many of these cancer manifestations Non-FDG avid cancers (cystic and mucinous neoplasms, renal cell carcinoma, hepatocellular carcinoma, carcinoid, low grade and small cell type lymphoma, protate cancer) Highly necrotic tumors








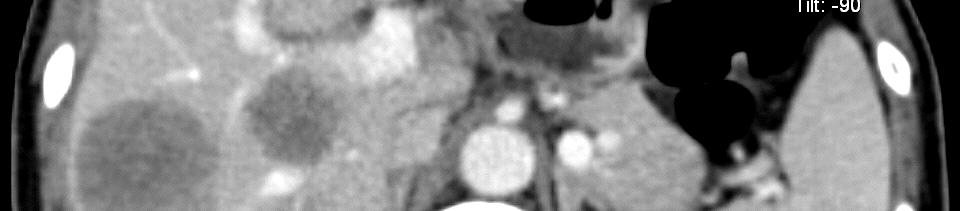
16 Recurrent hepatocellular carcinoma seen in liver on portal venous phase contrast enhanced CT



17 Negative non-contrast CT, negative FDG PET






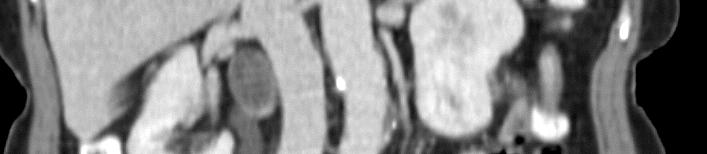
18 Non-FDG avid renal cell carcinoma with no contour abnormality clearly seen on contrast enhanced CT







19 Brain metastasis of breast cancer
20 PET-CT: CT Contrast Protocols Intravenous Contrast Certain clinically important non-cancer incidental findings seen in cancer patients on CT only require IV contrast DVT, thrombus associated with central venous lines, pulmonary embolism
21 Deep venous thrombus
22 Pulmonary embolism
23 PET-CT: CT Contrast Protocols Intravenous Contrast Negative oral contrast depends on bowel wall enhancement by intravenous contrast for optimal depiction on mucosal and serosal abnormalities






24 Negative Oral Contrast with IV Contrast
25 Serosal implant metastases of ovarian cancer depicted on negative oral contrast exam with intravenous contrast. Courtesy of Joseph Busch, MD.
26
27 PET-CT: CT Contrast Protocols PET-CT and IV Contrast Undiluted contrast laden venous blood in the subclavian vein and superior vena cava will cause beam hardening artifacts on CT with resultant hot spot artifacts on the attenuation corrected PET images at common infusion rates (2-3.5 ml/sec) 13% of subjects in study of 30 patients Antoch et. al. J Nucl Med 2002; 43:








28 Subclavian vein contrast artifact can occur when CT scanning gprotocol is not properly p optimized for whole body scanning Contrast CT Attenuation corrected OSEM using contrast CT attenuation Non-attenuation corrected FBP
29 PET-CT: CT Contrast Protocols Intravenous Contrast and SUVs No statistically or clinically significant spuriously elevated SUV that might interfere with diagnosis due to use of IV contrast enhanced CT for attenuation correction of the PET images (< 10% for tissues) No artifacts on images when CT properly performed Application of Intravenous Contrast in PET/CT. Does It Really Introduce Significant Attenuation Correction Error? Yau YY, et. al. J Nucl Med : PET/CT With Intravenous Contrast can be used for PET Attenuation Correction in Cancer Patients Berthelsen AK, et. al. Euro J Nucl Med : Quantifying the Effect of IV Contrast Media on Integrated PET/CT: Clinical Evaluation. Mawlawi O, et. al. AJR :
30 PET-CT: CT Contrast Protocols PET/CT Mythology: You have to perform two complete CT acquisitions if you want a diagnostic CT as part of the PET/CT, a localization CT scan and a separate diagnostic CT scan to avoid contrast artifacts No, if the fully optimized contrast enhanced CT scan is performed properly there are no clinically significant artifacts on images or with SUV values Contrast related artifacts are more a problem on the CT than the attenuation corrected PET images
31 PET-CT Scans PET-CT protocols mas CT PET Emission mas CT with contrast Whole torso PET-CT with diagnostic CT and CT attenuation scan
32 PET-CT Scans PET-CT protocols mas CT with contrast PET Emission Whole torso PET-CT with diagnostic CT
33 PET-CT: CT Contrast Protocols Intravenous Contrast Chemical composition is iodinated aromatics with solublizing functionality Opacification capacity given by mg Iodine per ml (ie 270, 300, 320, 350, 370 mg/ml) Three general classes: improved patient tolerance, fewer overall reactions -Ionic (hypertonic - no longer widely used) -Non-ionic (low osmolarity - commonly used -Isotonic non-ionic (iso osmolar - newest class) Frequently asked questions: Iodinated d Contrast t Agents Bettmann MA Radiographics 2004; 24:S3-S10
34 PET-CT: CT Contrast Protocols Intravenous Contrast - Relative Contraindications Renal failure Renal insufficiency History of contrast reaction, allergy Diabetes on oral therapy (metformin)
35 PET-CT: CT Contrast Protocols Intravenous Contrast - Contrast Reactions Reviewed 29,508 patients that underwent CT with IV contrast (iopromide) % mild adverse reaction % moderate adverse reaction % severe adverse reaction % 003% death Kortele et al AJR 2005; 184: 31-34
36 PET-CT: CT Contrast Protocols Intravenous Contrast - Contrast Reactions Of 29,508 patients t that t underwent CT with IV contrast (iopromide), 211 had reactions Of those that had reaction, 14% had history of prior contrast reaction and 44% had history of allergy - 76% urticaria - 6.2% facial/laryngeal edema - 4.7% nausea and vomiting - 3.8% bronchospasm - 9% other Kortele et al AJR 2005; 184: Slides are not to be reproduced without
37 PET-CT: CT Contrast Protocols Intravenous Contrast Putting it in Power injector has become standard Twin power injectors have advantage of gradients and saline chase A 20 gauge angiocatheter in a peripheral vein is preferred, a 22 gauge is acceptable for slower (2 ml/sec injection rates) PICC lines suitable for power injector IV contrast administration are now coming into common use (purple PICC line)
38
39
40
41 PET-CT: CT Contrast Protocols Intravenous Contrast t Timing i For most body CT protocols used in cancer imaging, intravenous contrast is injected as a continuous bolus at 2-3 ml/sec initiated at a specified time after scan acquisition commences As with comedy, sex and real estate investment, timing is everything CT scan acquisition must occur when the contrast material is in the desired vessels and had passed into the soft tissues at the time of maximum enhancement
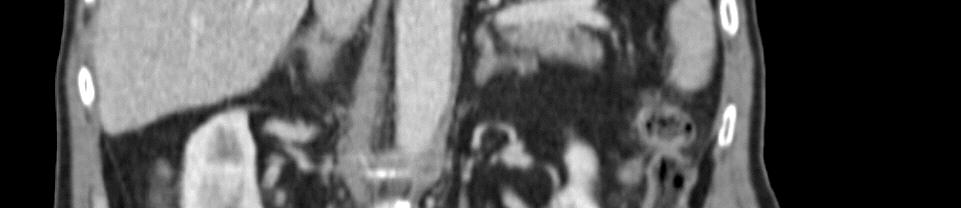
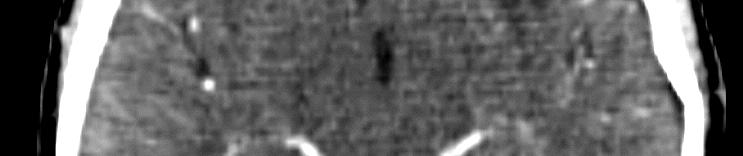
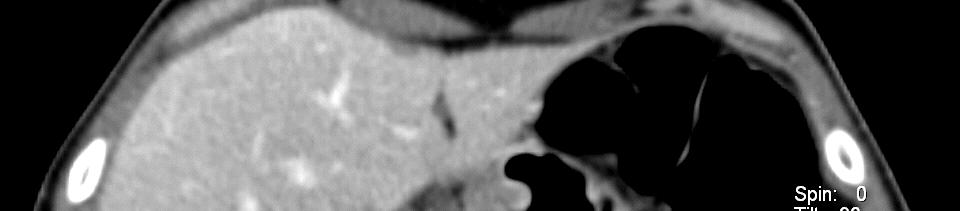
42 Portal venous phase contrast enhancement of the liver
43 Hepatocellular carcinoma Irregular FDG uptake corresponds to areas of abnormal abnormal contrast enhancement on arterial contrast phase of CT (arrows).
44 PET-CT: CT Contrast Protocols Intravenous Contrast t Timing i For most body CT protocols CT scanning commences seconds after initiation of contrast bolus For dedicated neck protocols seconds For an arterial phase seconds Bolus timing will depend on distant contrast has to travel and patient s vascular flow dynamics (blood-and contast gets there faster in younger patients heart failure, aneurysms, ect. slow things down requiring longer bolus delay)
45 PET-CT: CT Contrast Protocols IV contrast - General Principals For general body oncology CT scans, goal is relative equal arterial and venous opacification throughout the scan matching table feed to progress of contrast t bolus Contrast bolus can be extended by increasing total contrast infused or slowing infusion rate Contrast opacification (both vessels and tissue) can be increased by high rate of contrast infusion and/or greater density (mg I/ml) Artifacts from undiluted contrast in subclavian and SVC can be eliminated by saline chase or biphasic i infusion i rate and caudad-cranial d scan (Beyer et. al. JNM 2005; 46: )
46 Intravenous contrast opacity for 3 ml/min for 100ml Scan cranial-caudal arterial (upper chest) venous (lower pelvis) arterial (lower pelvis) venous (lower pelvis) sec Time post start of intravenous contrast injection
47 Intravenous contrast (3 ml/sec) with saline chase: note equal opacification of iliac arteries and veins
48 PET-CT: CT Contrast Protocols IV contrast - Technique with MDCT Moderate infusion rates (2-3 ml/sec) Saline chase using dual injector Body 3.0 ml/sec for ml with 50 ml saline chase, second delay, scan cranial-caudad over roughly 8-30 seconds Neck ml/sec for 65 ml with 50 ml chase, second delay Key is to bring injection route venous blood to similar contrast concentration as distal outflow vessels and not out run bolus at pelvis, and image liver in portal-venous phase
49 Intravenous contrast (3 ml/sec) with saline chase: note equal opacification of subclavian arteries and veins and absent intravenous contrast related beam hardening artifact





50 Metatstatic colon cancer to liver depicted on portal venous phase contrast enhanced CT Pre-therapy Post chemotherapy
51 PET-CT: CT Contrast Protocols Intravenous Contrast t Thorax Generally desire uniform enhancement of arteries, pulmonary arteries and veins, and central veins in chest second bolus delay works well with craniocaudad scanning starting at skull base Pulmonary arterial phase scanning can be added to better depict relationship of a mass with vessels for surgical planning


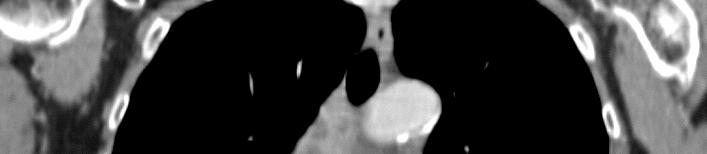







52 65 second bolus delay
53 PET-CT: CT Contrast Protocols Multi-phase contrast enhanced CT of thorax table reposition 25s 35s 65s 85s breath hold CT arterial phase quiet breathing whole torso CT at equil phase PET emission acquisitions Whole torso PET-CT with limited arterial phase acquisition followed by whole torso enhanced scan








54 Dual phase protocol for lung cancer provides intense vascular enhancement with reduced contrast load Arterial phase 25 second bolus delay Equilibrium phase 65 second bolus delay
55 Imaging Sequences for Head and Neck PET-CT a PET emission bed position 2-4 min PET emission bed position 4-10 minutes b Contrast CT whole torso technique, including neck, with arms down at side Reposition patient with arms up Contrast CT whole torso technique with arms raised c Contrast CT skull base to upper mediastinum, neck technique, arms down Reposition patient with arms up
56 PET-CT: CT Contrast Protocols Intravenous Contrast Head & Neck Primary Head & Neck cancers should be evaluated using dedicated CT and PET acquisitions from above the skull base to the thoracic inlet with arms down PET acquisition generally performed with a fine matrix and longer emission acquisition (5-10 minutes) CT acquisition using thin section reconstruction (< 2 mm) and contrast in arteriovenous phase 45 second bolus delay generally works well
57 Dedicated CT and PET acquisitions with arteriovenous Slides are not phase to be reproduced CTwithout
58 Necrotic metastatic lymph node: contrast helps define margins of node to assess for extracapsular spread
59 PET-CT: CT Contrast Protocols Intravenous Contrast Abdomen & Pelvis Generally portal venous phase is optimal IV contrast timing for scanning through the abdomen in cancer patients second bolus delay when CT scanning initiated from the skull base will result in timing such that the portal venous phase is present when the scan acquisition reaches the abdomen Faster CT scanners or faster bolus (> 3 ml/sec) require more careful timing such that there is venous opacification at the pelvis (don t out-run the bolus)





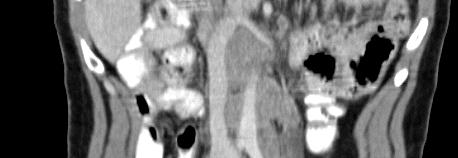
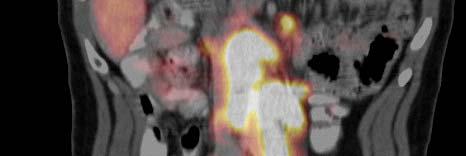



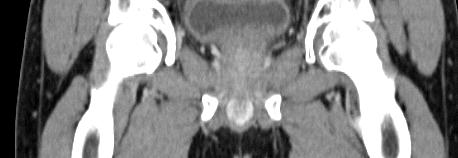
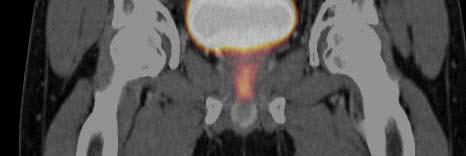
60 Intravenous contrast (3 ml/sec) with saline chase: note equal opacification of iliac arteries and veins
61 PET-CT: CT Contrast Protocols Multi-phase scanning Abdomen & Pelvis Certain diagnostic requirements may require anarterial phase (vascular depiction, hypervascular tumors) in addition to portal venous phase Evaluation of kidneys and certain liver masses may require a 3-5 minute delay phase scan in addition to the portal venous phase scanning
62 PET-CT Scans Multi-phase contrast enhanced CT table reposition 20s 30s 65s 85s breath hold CT arterial phase quiet breathing whole torso CT at equil phase PET emission acquisitions Whole torso PET-CT with limited arterial phase acquisition of the abdomen followed by whole torso scan








63 Adenocarcinoma of the pancreas with encasement of celiac axis



64 Liver Metastases of Hypervascular Neoplasm Late Arterial Phase Portal Venous Phase FDG PET



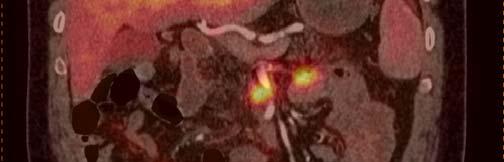
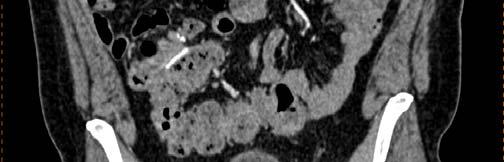
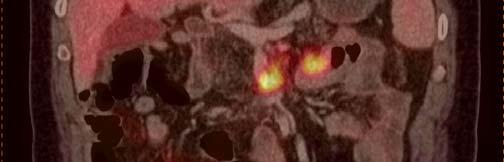
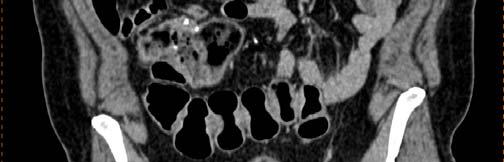
65 Pancreatic Tail Adenocarcinoma and Liver Metastases Late Arterial Phase Portal Venous Phase FDG PET




66 Recurrent metatstatic colon cancer in upper abdomen Arterial phase PET-CT of superior mesenteric artery



67 Recurrent metatstatic colon cancer in upper abdomen Portal-venous phase PET-CT of superior mesenteric vein




68 Recurrent metatstatic colon cancer in upper abdomen Portal-venous phase PET-CT of superior mesenteric vein






69 Involvement of superior mesenteric vein by mesenteric colon cancer metastasis
70 PET-CT: CT Contrast Protocols Conclusions Intravenous contrast use with PET-CT is not a new concept and is not difficult Fully optimized i CT with intravenous contrast t is part of the best of both worlds
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Breast Cancer PET/CT Imaging Protocol
 Breast Cancer PET/CT Imaging Protocol Scanning Protocol: Patients are scanned from the top of the neck through the pelvis. Arms-up position is used to avoid beam-hardening artifact in the chest and abdomen.
Breast Cancer PET/CT Imaging Protocol Scanning Protocol: Patients are scanned from the top of the neck through the pelvis. Arms-up position is used to avoid beam-hardening artifact in the chest and abdomen.
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Sectional Anatomy Quiz - III
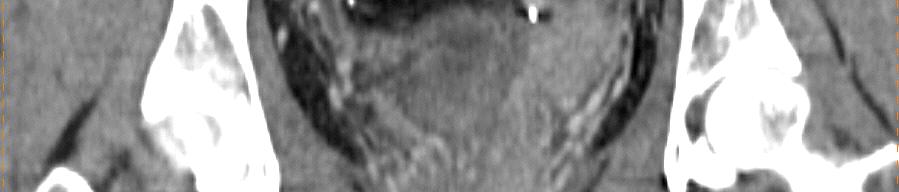
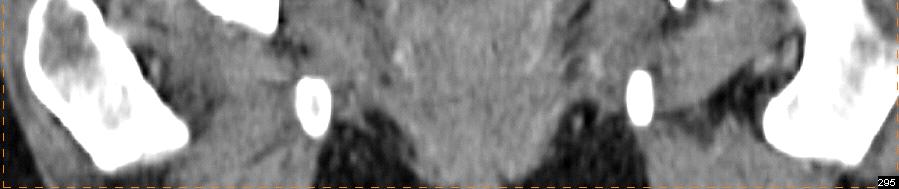
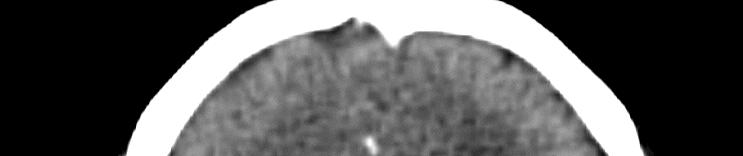
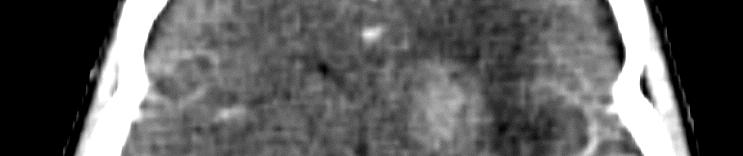
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Renal and adrenal tumours Faculty of Clinical Radiology www.rcr.ac.uk Contents Renal cell carcinoma 3 Clinical
CT angiography techniques. Boot camp
 CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
CT angiography techniques Boot camp Overview Basic concepts Contrast administration arterial opacification Time scan acquisition during the arterial phase Protocol examples Helical non-gated CTA Pulmonary
Liver imaging takes a step forward with Ingenia
 Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
Publication for the Philips MRI Community ISSUE 49 2013 / 2 Liver imaging takes a step forward with Ingenia Lyon South Hospital strives to move from several studies first CT, then MR or PET to using just
Ryan Niederkohr, M.D. Slides are not to be reproduced without permission of author
 Ryan Niederkohr, M.D. CMS: PET/CT CPT CODES 78814 Limited Area (e.g., head/neck only; chest only) 78815 78816 Regional (skull base to mid-thighs) True Whole Body (skull vertex to feet) SELECTING FIELD
Ryan Niederkohr, M.D. CMS: PET/CT CPT CODES 78814 Limited Area (e.g., head/neck only; chest only) 78815 78816 Regional (skull base to mid-thighs) True Whole Body (skull vertex to feet) SELECTING FIELD
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Customizing Contrast Injection for Body MDCT: Algorithmic Approach
 Customizing Contrast Injection for Body MDCT: Algorithmic Approach Lincoln L. Berland, M.D., F.A.C.R. University of Alabama at Birmingham Before Contrast Prep and Hydration Hydration single most important
Customizing Contrast Injection for Body MDCT: Algorithmic Approach Lincoln L. Berland, M.D., F.A.C.R. University of Alabama at Birmingham Before Contrast Prep and Hydration Hydration single most important
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
The Role of PET / CT in Lung Cancer Staging
 July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
July 2004 The Role of PET / CT in Lung Cancer Staging Vlad Vinarsky, Harvard Medical School Year IV Patient AM HPI: 81 yo F p/w hemoptysis x 1 month LLL lesion on CXR, not responsive to Abx 35 pack-year
Handzettel 1. CT Contrast Media. Agenda. Contrast Media Definition. Agenda. Why we need contrast media? Agenda
 Agenda CT Contrast Media Weena Swatdiswanee Factorinvolvein contrast enchancement Senior Application Specialist, CT Regional Headquarter Asia Australia weena.swat@siemens.com Page 1 Page 2 Agenda Contrast
Agenda CT Contrast Media Weena Swatdiswanee Factorinvolvein contrast enchancement Senior Application Specialist, CT Regional Headquarter Asia Australia weena.swat@siemens.com Page 1 Page 2 Agenda Contrast
International Journal of Current Medical Sciences- Vol. 6, Issue,, pp , June, 2016 A B S T R A C T
 ISSN: 2320-8147 International Journal of Current Medical Sciences- Vol. 6, Issue,, pp. 122-126, June, 2016 COMPUTED TOMOGRAPHY IN HEPATIC METASTASES Ananthakumar P and Adaikkappan M., Available online
ISSN: 2320-8147 International Journal of Current Medical Sciences- Vol. 6, Issue,, pp. 122-126, June, 2016 COMPUTED TOMOGRAPHY IN HEPATIC METASTASES Ananthakumar P and Adaikkappan M., Available online
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital
 Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital jeffrey.weinreb@yale.edu 1991 1997 Whole body MRI: multistation approach x z Isocenter: Table Move: Multiple Steps Whole body
Jeffrey C. Weinreb, MD, FACR Yale School of Medicine Yale-New Haven Hospital jeffrey.weinreb@yale.edu 1991 1997 Whole body MRI: multistation approach x z Isocenter: Table Move: Multiple Steps Whole body
FDG-PET/CT for cancer management
 195 REVIEW FDG-PET/CT for cancer management Hideki Otsuka, Naomi Morita, Kyo Yamashita, and Hiromu Nishitani Department of Radiology, Institute of Health Biosciences, The University of Tokushima, Graduate
195 REVIEW FDG-PET/CT for cancer management Hideki Otsuka, Naomi Morita, Kyo Yamashita, and Hiromu Nishitani Department of Radiology, Institute of Health Biosciences, The University of Tokushima, Graduate
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
An Introduction to PET Imaging in Oncology
 January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
8/3/2016. Consultant for / research support from: Astellas Bayer Bracco GE Healthcare Guerbet Medrad Siemens Healthcare. Single Energy.
 U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
U. Joseph Schoepf, MD Prof. (h.c.), FAHA, FSCBT-MR, FNASCI, FSCCT Professor of Radiology, Medicine, and Pediatrics Director, Division of Cardiovascular Imaging Consultant for / research support from: Astellas
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Optimized. clinical pathway. propels high utilization of PET/MR at Pitié-Salpêtrière Hospital
 Optimized propels high utilization of PET/MR at Pitié-Salpêtrière Hospital clinical pathway As one of Europe s largest teaching hospitals, Pitié-Salpêtrière Hospital is renowned for its innovative research
Optimized propels high utilization of PET/MR at Pitié-Salpêtrière Hospital clinical pathway As one of Europe s largest teaching hospitals, Pitié-Salpêtrière Hospital is renowned for its innovative research
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V
 CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CT Pancreas 3 Phase CT Abdomen WO W - NC.A.V Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest
 CTA Thoracic Aorta = CTA Chest") (Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
(Non-EKG Gated) CTA Thoracic Aorta = CTA Chest Reviewed By: Dan Verdini, MD, Rachael Edwards, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA principle, TRA
Liver 4 Phase CT Abdomen WO W - NC.A.V.D
 Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
Liver 4 Phase CT Abdomen WO W - NC.A.V.D Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the ALARA
Role of imaging in RCC. Ultrasonography. Solid lesion. Cystic RCC. Solid RCC 31/08/60. From Diagnosis to Treatment: the Radiologist Perspective
 Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Pancreatic Cancer. What is pancreatic cancer?
 Scan for mobile link. Pancreatic Cancer Pancreatic cancer is a tumor of the pancreas, an organ that is located behind the stomach in the abdomen. Pancreatic cancer does not always cause symptoms until
Scan for mobile link. Pancreatic Cancer Pancreatic cancer is a tumor of the pancreas, an organ that is located behind the stomach in the abdomen. Pancreatic cancer does not always cause symptoms until
Sectional Anatomy Quiz II
 Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
HEALTHFIRST 2011 RADIOLOGY PROGRAM CODE LIST
 HEALTHFIRST 2011 RADIOLOGY PROGRAM CODE LIST Outpatient Radiology utilization call Carecore at 1-877-773-6964 Modality CPT CODE Description CT SCANS 70450 CT HEAD/BRAIN W/O CONTRAST CT SCANS 70460 CT HEAD/BRAIN
HEALTHFIRST 2011 RADIOLOGY PROGRAM CODE LIST Outpatient Radiology utilization call Carecore at 1-877-773-6964 Modality CPT CODE Description CT SCANS 70450 CT HEAD/BRAIN W/O CONTRAST CT SCANS 70460 CT HEAD/BRAIN
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous)
 & CT Abdomen + Pelvis W (venous)") CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
CTA Chest Pulmonary Embolism & Routine CT Abdomen + Pelvis W CTA Chest W (arterial) & CT Abdomen + Pelvis W (venous) Reviewed By: Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: August 2018 Contact:
Radiation Exposure in Pregnancy. John R. Mayo UNIVERSITY OF BRITISH COLUMBIA
 Radiation Exposure in Pregnancy John R. Mayo UNIVERSITY OF BRITISH COLUMBIA Illustrative Clinical Scenario 32 year old female 34 weeks pregnant with recent onset shortness of breath and central chest pain
Radiation Exposure in Pregnancy John R. Mayo UNIVERSITY OF BRITISH COLUMBIA Illustrative Clinical Scenario 32 year old female 34 weeks pregnant with recent onset shortness of breath and central chest pain
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
CT evaluation of small bowel carcinoid tumors
 CT evaluation of small bowel carcinoid tumors Poster No.: C-0060 Congress: ECR 2015 Type: Educational Exhibit Authors: N. V. V. P. Costa, L. Nascimento, T. Bilhim ; Estoril/PT, PT, 1 2 3 1 2 3 Lisbon/PT
CT evaluation of small bowel carcinoid tumors Poster No.: C-0060 Congress: ECR 2015 Type: Educational Exhibit Authors: N. V. V. P. Costa, L. Nascimento, T. Bilhim ; Estoril/PT, PT, 1 2 3 1 2 3 Lisbon/PT
POSITRON EMISSION TOMOGRAPHY (PET)
") Status Active Medical and Behavioral Health Policy Section: Radiology Policy Number: V-27 Effective Date: 08/27/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Radiology Policy Number: V-27 Effective Date: 08/27/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
FieldStrength. Leuven research is finetuning. whole body staging
 FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
FieldStrength Publication for the Philips MRI Community Issue 40 May 2010 Leuven research is finetuning 3.0T DWIBS for whole body staging The University Hospital of Leuven is researching 3.0T whole body
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
LYMPHATIC DRAINAGE IN THE HEAD & NECK
 LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
LYMPHATIC DRAINAGE IN THE HEAD & NECK Like other parts of the body, the head and neck contains lymph nodes (commonly called glands). Which form part of the overall Lymphatic Drainage system of the body.
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Cancer Cases Treated and Results
 Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Cardiac Imaging Tests
 Cardiac Imaging Tests http://www.medpagetoday.com/upload/2010/11/15/23347.jpg Standard imaging tests include echocardiography, chest x-ray, CT, MRI, and various radionuclide techniques. Standard CT and
Cardiac Imaging Tests http://www.medpagetoday.com/upload/2010/11/15/23347.jpg Standard imaging tests include echocardiography, chest x-ray, CT, MRI, and various radionuclide techniques. Standard CT and
Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate)
") Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate) Overview Ga-68 dotatate binds to somatostatin receptors, with highest affinity for subtype 2 receptors (sstr2). It binds to cells that express
Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate) Overview Ga-68 dotatate binds to somatostatin receptors, with highest affinity for subtype 2 receptors (sstr2). It binds to cells that express
Molecular Imaging and Cancer
 Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
YOU MUST BRING GLOVES FOR THIS ACTIVITY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 5e. All text references are for this textbook. 2) Observe and sketch histology slide
VESSELS: GROSS ANATOMY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Typical PET Image. Elevated uptake of FDG (related to metabolism) Lung cancer example: But where exactly is it located?
 Lung cancer example: But where exactly is it located?") Typical PET Image Elevated uptake of FDG (related to metabolism) Lung cancer example: But where exactly is it located? PET/CT Oncology Imaging Anatometabolic fusion images are useful in the management
Typical PET Image Elevated uptake of FDG (related to metabolism) Lung cancer example: But where exactly is it located? PET/CT Oncology Imaging Anatometabolic fusion images are useful in the management
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Positron emission tomography computed tomography
 Interpretation and Reporting of Positron Emission Tomography Computed Tomographic Scans Harry Agress, Jr, MD,* Terence Z. Wong, MD, PhD, and Paul Shreve, MD Body oncology positron emission tomography computed
Interpretation and Reporting of Positron Emission Tomography Computed Tomographic Scans Harry Agress, Jr, MD,* Terence Z. Wong, MD, PhD, and Paul Shreve, MD Body oncology positron emission tomography computed
Lines and tubes. 1 Nasogastric tubes Endotracheal tubes Central lines Permanent pacemakers Chest drains...
 Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
Lines and tubes 1 Nasogastric tubes... 15 2 Endotracheal tubes.... 19 3 Central lines... 21 4 Permanent pacemakers.... 25 5 Chest drains... 30 This page intentionally left blank 1 Nasogastric tubes Background
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Question 1 History. Likely Diagnosis Differential. Further Investigation or Management. Requires Paediatric Surgical referral for laparotomy
 Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Question 1 Male newborn spilling green tinged vomit day 1 of life Imaging Abdominal X-Rays performed on 03/05/2012 Upper and lower gastrointestinal contrast studies performed on 03/05/2012 Abdominal X-Rays
Liver Perfusion Analysis New Frontiers in Dynamic Volume Imaging. Case Study Brochure Chang Gung Memorial Hospital.
 New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
New Frontiers in Dynamic Volume Imaging dynamic volume CT Case Study Brochure Chang Gung Memorial Hospital http://www.toshibamedicalsystems.com Toshiba Medical Systems Corporation 2010-2011. All rights
Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF)
") Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF) Overview Indication Sodium Fluoride F18 injection is a radioactive diagnostic agent for positron emission
Austin Radiological Association Nuclear Medicine Procedure PET SODIUM FLUORIDE BONE SCAN (F-18 NaF) Overview Indication Sodium Fluoride F18 injection is a radioactive diagnostic agent for positron emission
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Clinical PET/CT imaging. PET/CT - Optimization of torso imaging. CT-based attenuation correction. PET/CT torso imaging
 / - Optimization of torso imaging Clinical / imaging Torso FDG, 1976 Torso FDG-/, 2007 Thomas Beyer thomas.beyer@cmi-experts.com CE 30, SNM Annual Meeting, Toronto, June 2009 Software Hardware Neck Thorax
/ - Optimization of torso imaging Clinical / imaging Torso FDG, 1976 Torso FDG-/, 2007 Thomas Beyer thomas.beyer@cmi-experts.com CE 30, SNM Annual Meeting, Toronto, June 2009 Software Hardware Neck Thorax
CTA Pulmonary Embolism CTA Chest W (arterial)
") CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
CTA Pulmonary Embolism CTA Chest W (arterial) Reviewed By: Rachael Edwards, MD; Anna Ellermeier, MD; Brett Mollard, MD Last Reviewed: January 2019 Contact: (866) 761-4200, Option 1 In accordance with the
Anaplastic Thyroid Carcinoma in a Young Boy
 18 F-FDG PET/CT in the Diagnosis of Tumor Thrombus from Anaplastic Thyroid Carcinoma in a Young Boy Maria M. D Souza, Abhinav Jaimini, Rajnish Sharma, Madhavi Tripathi, Dinesh Singh, Santosh Pandey, Anupam
18 F-FDG PET/CT in the Diagnosis of Tumor Thrombus from Anaplastic Thyroid Carcinoma in a Young Boy Maria M. D Souza, Abhinav Jaimini, Rajnish Sharma, Madhavi Tripathi, Dinesh Singh, Santosh Pandey, Anupam
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review
 Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Review Article Common and unusual CT and MRI manifestations of pancreatic adenocarcinoma: a pictorial review Min-Jie Yang, Su Li, Yong-Guang Liu, Na Jiao, Jing-Shan Gong Department of Radiology, Shenzhen
Lugano classification: Role of PET-CT in lymphoma follow-up
 CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
CAR Educational Exhibit: ID 084 Lugano classification: Role of PET-CT in lymphoma follow-up Charles Nhan 4 Kevin Lian MD Charlotte J. Yong-Hing MD FRCPC Pete Tonseth 3 MD FRCPC Department of Diagnostic
Abdomen Sonography Examination Content Outline
 Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Staging recurrent ovarian cancer with 18 FDG PET/CT
 ONCOLOGY LETTERS 5: 593-597, 2013 Staging recurrent ovarian cancer with FDG PET/CT SANJA DRAGOSAVAC 1, SOPHIE DERCHAIN 2, NELSON M.G. CASERTA 3 and GUSTAVO DE SOUZA 2 1 DIMEN Medicina Nuclear and PET/CT
ONCOLOGY LETTERS 5: 593-597, 2013 Staging recurrent ovarian cancer with FDG PET/CT SANJA DRAGOSAVAC 1, SOPHIE DERCHAIN 2, NELSON M.G. CASERTA 3 and GUSTAVO DE SOUZA 2 1 DIMEN Medicina Nuclear and PET/CT
IAEA RTC. PET/CT and Planning of Radiation Therapy 20/08/2014. Sarajevo (Bosnia & Hercegovina) Tuesday, June :40-12:20 a.
 Tuesday, June :40-12:20 a.") IAEA RTC PET/CT and Planning of Radiation Therapy Sarajevo (Bosnia & Hercegovina) Tuesday, June 17 2014 11:40-12:20 a.m María José García Velloso Servicio de Medicina Nuclear Clínica Universidad de Navarra
IAEA RTC PET/CT and Planning of Radiation Therapy Sarajevo (Bosnia & Hercegovina) Tuesday, June 17 2014 11:40-12:20 a.m María José García Velloso Servicio de Medicina Nuclear Clínica Universidad de Navarra
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
Cigna - Prior Authorization Procedure List: Radiology & Cardiology
 Cigna - Prior Authorization Procedure List: Radiology & Cardiology Category CPT Code CPT Code Description 93451 Right heart catheterization 93452 Left heart catheterization 93453 Combined right and left
Cigna - Prior Authorization Procedure List: Radiology & Cardiology Category CPT Code CPT Code Description 93451 Right heart catheterization 93452 Left heart catheterization 93453 Combined right and left
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
CT Chest. Verification of an opacity seen on the straight chest X ray
 CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
CT Chest Indications: To assess equivocal plain x-ray findings Staging of lung neoplasm Merastatic workup of extra thoraces malignancies Diagnosis of diffuse lung diseases with HRCT Assessment of bronchietasis
Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors
 Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors Lars Stegger, Benjamin Noto Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to
Bone PET/MRI : Diagnostic yield in bone metastases and malignant primitive bone tumors Lars Stegger, Benjamin Noto Department of Nuclear Medicine University Hospital Münster, Germany Content From PET to
Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound
 Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound Mollie Rashid, MD Corinne Deurdulian, MD Hisham Tchelepi, MD Keck School of Medicine, University of Southern
Fusion Ultrasound: Characterization of Abdominal Masses with MR, CT, PET, and Contrast Ultrasound Mollie Rashid, MD Corinne Deurdulian, MD Hisham Tchelepi, MD Keck School of Medicine, University of Southern
General Nuclear Medicine
 General Nuclear Medicine What is General Nuclear Medicine? What are some common uses of the procedure? How should I prepare? What does the equipment look like? How does the procedure work? How is the procedure
General Nuclear Medicine What is General Nuclear Medicine? What are some common uses of the procedure? How should I prepare? What does the equipment look like? How does the procedure work? How is the procedure
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Screening tests. When you need them and when you don t
 Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review
 How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review Mannudeep K. Kalra, MD, DNB Massachusetts General Hospital Harvard Medical School Financial Disclosure This presentation
How do the Parameters affect Image Quality and Dose for Abdominal CT? Image Review Mannudeep K. Kalra, MD, DNB Massachusetts General Hospital Harvard Medical School Financial Disclosure This presentation
STAGING AND FOLLOW-UP STRATEGIES
 ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR