Prostate cancer: Update from the BCCA
|
|
|
- Elwin Cameron
- 6 years ago
- Views:
Transcription
1 Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing ADT duration 3. Brachytherapy results 4. Adjuvant & Salvage RT RADICALS 1
2 2 Provincial incidence EBRT Provincial incidence Brachy Incidence RRP
3 Provincial incidence Curative treatments as % of incidence 40% 35% EBRT EBRT 30% 25% 20% 15% 10% RRP RRP Brachy Brachy 5% 0% Incidence projections Number of People 3
4 Prevalence projections 14,000 12,000 Postate Cancer Prevalence 10,000 8,000 6,000 4,000 2, Age Distribution 2015 Age Distribution 2025 Age Distribution 2035 Age Distribution - 2. New developments with External RT 4
5 EBRT is getting better! Why EBRT is getting better 1980 s Conventional simulation 1990 s CT planning (2d) CT planning (2½d) CT planning (3d conformal RT) 2000 s IMRT (Intensity Modulated RT) Now IGRT (Image Guided RT) VMAT (Volumetric Modulated RT) 5

 Mid-prostate CT used to")

6 Conventional simulation (80 s) Plain X-Ray with urethrogram Based on bony landmarks No prostate position verification Max dose 66Gy CT planned treatment (early 90 s) Mid-prostate CT used to determine patient shape Prostate identified on all slices But Radiation planning was not true 3-Dimensions Max dose 70Gy 6


7 EBRT: Conformal RT Increased dose effects Increased cure Increased toxicity Grade Rectal 10% v 1% - Urinary 4% v 2% ALAN POLLACK, et al Int. J. Radiation Oncology Biol. Phys., Vol. 53, No. 5, pp ,



8 CT planned treatment (late 90 s) True 3-D planning Radiation dose calculated using all CT information to correct for tissue inhomogeneities Max dose ~76Gy Did this lead to better outcomes? Probably! 3D group Late GU toxicity 2D 3D Grade 1 28% 10% Grade 2 20% 11% Grade 3 8% 6% Grade proportion not failing D group Planning group 2 Planning group 3 Agranovich et al. Radiotherapy & Oncology; p. S time (months) 8

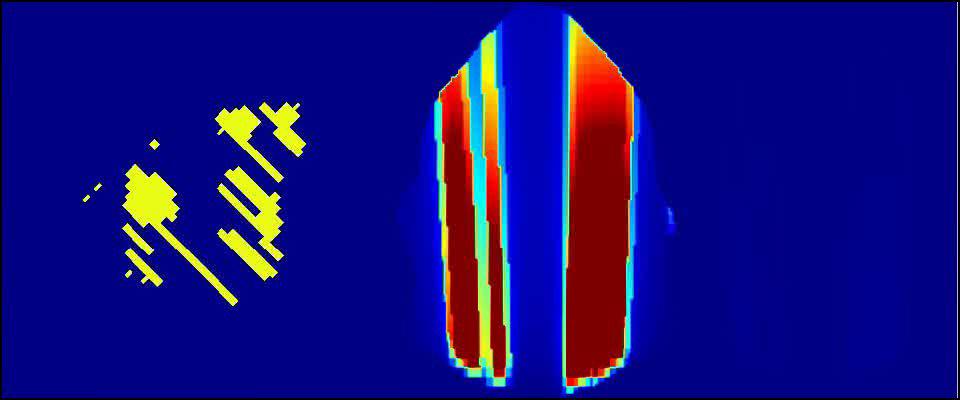
9 IMRT Many beams of radiation Each can be modulated by the MLC leaves in complex patterns High dose region very tight Allows rectal sparing Simple RT technique 9
10 IMRT technique Volumetric Modulated Arc Inventor: Karl Otto Single 360º source rotation Variable collimation Variable dose 10


11 Volumetric Modulated Arc Inventor: Karl Otto Single 360º source rotation Variable collimation Variable dose 11
12 12
13 VMAT Volume Modulated Arc Therapy 3-D Conformal - limits dose to ~76Gy IMRT - limits dose to ~80Gy VMAT -?86Gy 13
14 Prostate movement Usually <5mm Exceptionally <10mm Worse in the obese Worse with distended rectums Int. J. Radiation Oncology Biol. Phys., Vol. xx, No. x, pp. xxx,
15 Potential downsides Treatment complexity Errors Diverts resources Impact on waiting lists Cost Brachytherapy $10,400 EBRT $6,600 IMRT?$13,000 RRP (open) $7,700 Markov model estimates intermediate risk $22,000 per QALY 3-D $48,000 per QALY IMRT Second malignancy Konski et al USING DECISION ANALYSIS TO DETERMINE THE COST-EFFECTIVENESS OF IMRT Int. J. Radiation Oncology Biol. Phys., 2006 Induced cancers Overall men with prostate cancer have Reduced risk of other cancers Life expectancy greater than general popl n Some cancers are increased with prostate cancer Bladder SIR 1.3 Testis SIR 2.8 Some cancers are increased with RT Colorectal SIR 1.2 Sarcoma SIR 1.7 1/220 overall. 1/70 after 10 years follow-up Pickles et al. Radiotherapy and Oncology 65 (2002)
16 b. Androgen Deprivation Therapy with radiation therapy Optimizing ADT High risk bned outcomes, BCCA % % % ADT use 93% 87% 12% 16
17 ADT with radiation: survival benefits Bolla I: 0 v 3 years RTOG 8531: 0 v 5+ years D Amico: 0 v 6 months Bolla II: 0.5 v 3 years RTOG 8610: 0 v 4mo Something special is going on 9% absolute survival improvement 1.4 years median survival benefit From 4 months ADT a decade earlier! Roach. JCO VOLUME 26 NUMBER 4 FEBRUARY
18 Why does ADT work with RT? 1. Reduces tumour volume 2. Decreases tumour hypoxia Post-treatment versus pretreatment marginal mean prostate cancer po2 levels in 22 patients. Dark points, significant (P V 0.001) changes in oxygenation with androgen withdrawal; bars, SEs. The line of unity is also shown. Milosevic et al., Cancer Res 2007; 67: (13). July 1, 2007 Why does ADT work with RT? 1. Shinogi Tumour Model RT & castration before RT & castration after RTalone % Local Control Radiation Dose (Gy) Zietman 18
19 Why does ADT work with RT? 1. Reduces tumour volume 2. Decreases tumour hypoxia 3. Increases apoptosis 4. Affects dendritic cells increasing immunologic recognition of prostate cancer Timing of ADT neoadjuvant or adjuvant? 893 men with ADT/EBRT median ADT dur n 33% pure neoadjuvant 5mo 16% neoadjuvant-concurrent 8mo 50% NA-C-Adjuvant 17mo In multivariate analysis No effect of timing Reanalyzed 2008 BCCA Prostate Cohort Outcomes Initiative (unpublished) Pickles T, Prostate Cohort Outcomes Initiative. Duration, Not Timing Is Important When Androgen Ablation Is Combined With External Beam RT. CUA Annual Meeting; 2004; Whistler, BC: Canadian Journal of Urology; p
20 Timing of ADT study 4 month NA v 4mo Adjuvant Lawton 9413 update. Int. J. Radiation Oncology Biol. Phys., Vol. -, No. -, pp. 1 10, 2007 Timing: Before or after? Most survival benefit was shown in studies using adjuvant bned benefits from neoadjuvant Overall duration most important 20
:362-7 Brachytherapy - unpublished But ADT has potential toxicity Nuisance Weight gain Hot flashes ED Memory change Osteopenia/porosis Arthritis Muscle weakness Serious Metabolic syndrome")
21 & it s not permanent castration Testosterone recovery following ADT 1.0 Proportion recovering TTT to 5nmol/l Years post cessation of AA EBRT - Cancer. 2002;94(2):362-7 Brachytherapy - unpublished But ADT has potential toxicity Nuisance Weight gain Hot flashes ED Memory change Osteopenia/porosis Arthritis Muscle weakness Serious Metabolic syndrome Weight gain Diabetes risk HR MI risk HR Death rate MI inc ~x2fold 2 1: Keating et al, J Clin Oncol 24: : Tsai et al., J Natl Cancer Inst 2007;99:
22 So how much adjuvant ADT do men really need? Life long? 3 years? 2 years? 6 months? None? So how much adjuvant ADT do men really need? 3941 cases with intermediate or high risk cancer 4 centres proportional hazards model of bned outcome bootstrap resampling to derive non-parametric confidence intervals (CI) Work in progress Scott Williams, Tom Pickles, Larry Kestin, Mark Buyyounouski, Gill Duchesne 22
23 Hazard Ratio So how much adjuvant ADT do men really need? Work in progress Months Scott Williams, of Androgen Tom Pickles, Deprivation Larry Kestin, Mark Buyyounouski, Gill Duchesne So how much adjuvant ADT do men really need? No ADT 0% of the benefit c/w 3 yrs 6 mo 54% 1yr 83% Hazard Ratio yr 96% Months of Androgen Deprivation Work in progress Scott Williams, Tom Pickles, Larry Kestin, Mark Buyyounouski, Gill Duchesne 23
24 Do all risk groups benefit? - Effect of ADT on bned by risk group 110% 100% 100% 100% 90% 90% 80% 70% 60% 50% ADT No ADT 80% 70% 60% 50% ADT 80% 60% ADT 40% 40% 40% bned (Phoenix) 30% 20% 10% 0% bned (Phoenix) 30% 20% 10% 0% No ADT bned (Phoenix) 20% 0% No ADT Years post - radiation Low risk n.s. Months post - radiation Intermediate p=0.01 Years post - radiation High p< BCCA GURO data Beasley M, Williams SG, Pickles T. In Press BMC Radiation Oncology Dec 2007 Effect of ADT on bned intermediate risk 100% 90% 80% 70% ADT 60% 50% 40% bned (Phoenix) 30% 20% 10% 0% No ADT Months post - radiation Beasley M, Williams SG, Pickles T. In Press BMC Radiation Oncology Dec
25 Effect of ADT on bned intermediate risk 100% 90% 80% 70% ADT 60% 50% 40% bned (Phoenix) 30% 20% 10% 0% No ADT % Months post - radiation 100% PSA <10, Gleason 7 PSA 15-20, Gleason 6 80% 80% ADT bned (Houston) 60% 40% PSA Gleason 6 bned (Houston) 60% 40% 20% No ADT 20% 0% % Years Years Low-intermediate p= n.s. High-intermediate P=0.003 HR 1.7 Contemporary BCCA radiation results by risk group Low Intermediate High Unpublished PCOI data. Patients treated
26 Optimizing ADT High risk bned outcomes By number of risk factors BCCA: EBRT & ADT (99%) Median ADT dur n 17 months Median f/up 4.1 yrs VGH: RRP & ADT (83%) Median ADT dur n 18 months Median f/up 3.3 yrs BCCA PCOI outcomes & Rod Studd 2007 Urology Rounds 3. Brachytherapy 26
27 Why might brachytherapy give better outcomes? Very high radiation doses Equivalent to ~90Gy EBRT (maybe) Very focal Low toxicity except for urinary Margin ~5mm Enough for extracapsular spread Low radiation dose rate Radiobiological advantages (?) How does brachy shape up? No randomized data available Institutional data very suggestive that results with brachy are superior to EBRT 1. Meta comparison (adjusted) 2. BCCA results & comparison 27
28 Meta comparison bned rates low risk 1 % Progression Free Years wd Brachy Surg EBRT Cryo HIFU *Hypofractionated ** HDR *** D 90 > 130 Gy wd= well Diff Courtesy Peter Grimm Meta comparison bned rates low risk 1 % Progression Free Years wd Brachy Surg adjusted EBRT Cryo HIFU *Hypofractionated ** HDR *** D 90 > 130 Gy wd= well Diff Courtesy Peter Grimm 28
29 Meta comparison bned rates low risk *** % Progression Free Years wd Brachy Surg adjusted EBRT Cryo HIFU *Hypofractionated ** HDR *** D 90 > 130 Gy wd= well Diff Courtesy Peter Grimm Meta comparison bned rates intermediate risk % Progression Free Years 26 Brachy Surg EBRT Cryo EBRT & Seeds Courtesy Peter Grimm 29
30 Meta comparison bned rates intermediate risk 1 % Progression Free Years Brachy Surg adj EBRT Cryo EBRT & Seeds Courtesy Peter Grimm Meta comparison bned rates intermediate risk % Progression Free Years Brachy Surg adj EBRT Cryo EBRT & Seeds Courtesy Peter Grimm 30
31 BCCA results Brachy program is 10 years old this summer >2200 implants Prospective data collection Real time data entry and analysis 1006 consecutive patients from #1 7/ /2003 Data cut off Oct 2007 = minimum 4 yrs f/up No exclusions Patient selection Low risk PSA 10 Gleason 6 ADT for TRUS volumes > 50cc Intermediate (low tier) PSA 10 and Gleason 7 or PSA Gleason 6 ADT for 3 months before & 3 months after 31
32 Outcomes 1. bned (Phoenix = Nadir +2) Low: bned 95.4 % Int: bned 96.3% Outcomes Metastases n=5 (99.1% KM) Deaths 54 non-prostate 1 prostate 1 complication (renal failure/urosepsis) 32
33 Toxicity GU Prevalence RTOG grades 60% 50% 40% 30% 20% 10% Grade 1 Grade 2 Grade 3 Minor nuisance Medication Minor surgical (excl catheterization) 0% Years Brachytherapy outcomes database 2008 unpublished BCCA Toxicity publications Bucci, J, W J Morris, M Keyes, et al.: Predictive factors of urinary retention following prostate brachytherapy. Int J Radiat Oncol Biol Phys, 53,(1): 91-8, [2002]. Macdonald, A G, M Keyes, A Kruk, et al.: Predictive factors for erectile dysfunction in men with prostate cancer after brachytherapy: is dose to the penile bulb important? Int J Radiat Oncol Biol Phys, 63,(1): , [2005]. Keyes et al. Urinary toxicity 845 patients. In preparation AUR rates Peak time of AUR in first few weeks ~0.6% long term Learning curve related to Procedure dexterity Needle loading Patient selection 33
34 Toxicity GI Prevalence RTOG grades 60% 50% 40% 30% Grade 1 Minor nuisance Grade 2 Medication Grade 3 Minor surgical 20% 10% 0% Years Brachytherapy outcomes database 2008 unpublished Potency by age group 1, 2, and 3 years after implant Macdonald, A G, M Keyes, et al Int J Radiat Oncol Biol Phys, 63,(1): , [2005]. 34
35 How does Brachy compare with EBRT? 1:1 matched pair analysis with EBRT Same dates (7/98-2/01) Same PSA (within 1ng/ml) Same use ADT (within 2 months) Same Gleason total (exact) Same % positive cores (<>50%) Same T stage (major T category) How does brachy compare with EBRT? Baseline prognostic features Brachy EBRT Patient numbers Median follow-up 68mo 66mo NCCN risk group Low 77.7% 77.7% Intermed 22.3% 22.3% p=ns ipsa median p=ns Stage(1997) 1a-c 38.8% 41.7% 2a 54% 50.4% 2b 7.2% 7.9% p=ns %PC <=50% 87.8% p=ns Gleason % 87.8% % 12.2% p=ns ADT use Yes 31.7% 30.2% p=ns Duration 6mo 5.8mo p=ns 35
 6mo 24mo How does brachy compare with surgery?")
36 How does brachy compare with EBRT? 7 yr rates: 95% 75% p= Brachy EBRT Last PSA (in non-relapsers) PSAdt (relapsers) 6mo 24mo How does brachy compare with surgery? Canadian trial 3 v 8 months Neoadjuvant ADT Courtesy Martin Gleave 36
37 4. Post-op adjuvant radiation Treatment of the positive margin 24% from 3 month arm of 3 v 8 mo study Margin ve or Margin +ve & RT +ve margin No adjuvant RT Van der Kwast. JCO VOLUME 25 NUMBER 27 SEPTEMBER
38 Treatment of the positive margin 3 randomized trials EORTC men, 5 yr follow-up Relapse HR 0.52 No survival advantage (yet) NCIC-SWOG. 473 men, 10 yr follow-up Relapse HR 0.51 Mets HR 0.8 (ns) No survival advantage (HR 0.76, ns) ARRO. 293 men, 3 yr follow-up Relapse HR 0.4 No survival advantage How about waiting for the PSA to rise? Salvage RT.7 BF Estimate Adjuvant RT Months Allan Pollack personal communication 38


39 Or using ADT instead? EPC trial of bicalutamide Increased non-cancer death rate with survival detriment RTOG 9601 trial results soon Also used bicalutamide though Retrospective data conflicting RADICALS Radiotherapy and Androgen Deprivation In Combination After Local Surgery 39
40 RADICALS randomised comparisons: Flow diagram Radical prostatectomy All Groups Assess need for RT Time RADICALS randomised comparisons: Flow diagram Radical prostatectomy Uncertain Group Assess need for RT Uncertain group RANDOMISE Immediately after surgery Time 40
41 RADICALS randomised comparisons: Flow diagram Radical prostatectomy Uncertain Group Assess need for RT Uncertain group Immediately after surgery RANDOMISE Immediate RT RANDOMISE Immediately after surgery Monitor on trial RT + no AD RT + short AD RT + long AD Time RADICALS randomised comparisons: Flow diagram Radical prostatectomy Uncertain Group Assess need for RT Uncertain group Immediately after surgery RANDOMISE Immediate RT RANDOMISE Immediately after surgery Monitor on trial RT + no AD RT + short AD RT + long AD Trial follow-up Deferred RT RANDOMISE At rising PSA RT + no AD RT + short AD RT + long AD Time 41
42 RADICALS randomised comparisons: Flow diagram Radical prostatectomy Immediate Group Assess need for RT Immediate RT group Immediate RT Immediately after surgery RANDOMISE RT + no AD RT + short AD RT + long AD Trial follow-up Time Outcome measures RADICALS randomised comparisons: Flow diagram Radical prostatectomy Deferred Group Assess need for RT Deferred RT group Monitor, not on trial Time 42
43 RADICALS randomised comparisons: Flow diagram Radical prostatectomy Deferred Group Assess need for RT Deferred RT At rising PSA RANDOMISE Deferred RT group (Monitored off trial, now PSA rising) RT + no AD RT + short AD RT + long AD Trial follow-up Time Outcome measures RADICALS randomised comparisons: Flow diagram Radical prostatectomy All Groups Assess need for RT Immediate RT group Uncertain group Immediately after surgery RANDOMISE Immediate RT RANDOMISE Immediately after surgery Monitor on trial RT + no AD RT + short AD RT + long AD Trial follow-up Note: Patients can be randomised between three AD arms or any two AD arms Deferred RT At rising PSA RANDOMISE Deferred RT group (Monitored off trial, now PSA rising) RT + no AD RT + short AD RT + long AD Trial follow-up Time Outcome measures 43
44 RADICALS randomised comparisons: Flow diagram Radical prostatectomy All Groups Assess need for RT Immediate RT group Uncertain group Immediately after surgery RANDOMISE Immediate RT RANDOMISE Immediately after surgery Monitor on trial RT + no AD RT + short AD RT + long AD Trial follow-up Deferred RT At rising PSA RANDOMISE Deferred RT group (Monitored off trial, now PSA rising) RT + no AD RT + short AD RT + long AD Trial follow-up Time Outcome measures Outcome measures Primary: Disease-specific survival (death after PCa progression) Secondary: Freedom from treatment failure Clinical progression-free survival Overall survival Duration of androgen deprivation Quality of life 44
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet
 S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
The Phoenix Definition of Biochemical Failure Predicts for Overall Survival in Patients With Prostate Cancer
 55 The Phoenix Definition of Biochemical Failure Predicts for Overall Survival in Patients With Prostate Cancer Matthew C. Abramowitz, MD 1 Tiaynu Li, MA 2 Mark K. Buyyounouski, MD 1 Eric Ross, PhD 2 Robert
55 The Phoenix Definition of Biochemical Failure Predicts for Overall Survival in Patients With Prostate Cancer Matthew C. Abramowitz, MD 1 Tiaynu Li, MA 2 Mark K. Buyyounouski, MD 1 Eric Ross, PhD 2 Robert
Jure Murgic 1, Matthew H Stenmark 1, Schuyler Halverson 1, Kevin Blas 1, Felix Y Feng 1,2 and Daniel A Hamstra 1,3*
 Murgic et al. Radiation Oncology 2012, 7:127 RESEARCH Open Access The role of the maximum involvement of biopsy core in predicting outcome for patients treated with dose-escalated radiation therapy for
Murgic et al. Radiation Oncology 2012, 7:127 RESEARCH Open Access The role of the maximum involvement of biopsy core in predicting outcome for patients treated with dose-escalated radiation therapy for
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes
 ORIGINAL RESEARCH Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes Michael J. Metcalfe, MD ; Patricia Troncoso, MD 2 ; Charles C. Guo,
ORIGINAL RESEARCH Salvage prostatectomy for post-radiation adenocarcinoma with treatment effect: Pathological and oncological outcomes Michael J. Metcalfe, MD ; Patricia Troncoso, MD 2 ; Charles C. Guo,
Clinical and biochemical outcomes of men undergoing radical prostatectomy or radiation therapy for localized prostate cancer
 Original Article Radiat Oncol J 205;33():2-28 http://dx.doi.org/0.3857/roj.205.33..2 pissn 2234-900 eissn 2234-356 Clinical and biochemical outcomes of men undergoing radical prostatectomy or radiation
Original Article Radiat Oncol J 205;33():2-28 http://dx.doi.org/0.3857/roj.205.33..2 pissn 2234-900 eissn 2234-356 Clinical and biochemical outcomes of men undergoing radical prostatectomy or radiation
2018 ASTRO Refresher Course: Prostate Cancer. Timur Mitin, MD PhD Oregon Health and Science University
 2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
Section: Therapy Effective Date: October 15, 2016 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD
 after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD") Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Heterogeneity in high-risk prostate cancer treated with high-dose radiation therapy and androgen deprivation therapy
 Cagney et al. BMC Urology (2017) 17:60 DOI 10.1186/s12894-017-0250-2 RESEARCH ARTICLE Heterogeneity in high-risk prostate cancer treated with high-dose radiation therapy and androgen deprivation therapy
Cagney et al. BMC Urology (2017) 17:60 DOI 10.1186/s12894-017-0250-2 RESEARCH ARTICLE Heterogeneity in high-risk prostate cancer treated with high-dose radiation therapy and androgen deprivation therapy
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
Salvage External Beam Radiotherapy for Prostate Cancer After
 Radical Prostatectomy July 22, 2010 Prostate Cancer [1], Genitourinary Cancers [2], Oncology Journal [3]By Daniel A. Hamstra, MD, PhD [4], Sung Kim, MD [5], and James B. Yu, MD [6] This article defines
Radical Prostatectomy July 22, 2010 Prostate Cancer [1], Genitourinary Cancers [2], Oncology Journal [3]By Daniel A. Hamstra, MD, PhD [4], Sung Kim, MD [5], and James B. Yu, MD [6] This article defines
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer
 Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
in 32%, T2c in 16% and T3 in 2% of patients.
 BJUI Gleason 7 prostate cancer treated with lowdose-rate brachytherapy: lack of impact of primary Gleason pattern on biochemical failure Richard G. Stock, Joshua Berkowitz, Seth R. Blacksburg and Nelson
BJUI Gleason 7 prostate cancer treated with lowdose-rate brachytherapy: lack of impact of primary Gleason pattern on biochemical failure Richard G. Stock, Joshua Berkowitz, Seth R. Blacksburg and Nelson
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Outcomes Following Negative Prostate Biopsy for Patients with Persistent Disease after Radiotherapy for Prostate Cancer
 Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update
 BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
Intensity Modulated Radiotherapy (IMRT) of the Prostate
 of the Prostate") Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
Tanaka et al. BMC Cancer (2017) 17:573 DOI /s
 17:573 DOI /s") Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
GRANDANGOLO: CA PROSTATA
 GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Androgen Deprivation Therapy A Question of Timing
 Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November D. Maruzzi - L. Ruggera
 High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
PSA bouncing after brachytherapy HDR and external beam radiation therapy: a study of 121 patients with minimum 5-years follow-up
 Original article Original articles PSA bouncing after brachytherapy HDR and external beam radiation therapy: a study of 121 patients with minimum 5-years follow-up Roman Makarewicz, MD, PhD, Prof., Andrzej
Original article Original articles PSA bouncing after brachytherapy HDR and external beam radiation therapy: a study of 121 patients with minimum 5-years follow-up Roman Makarewicz, MD, PhD, Prof., Andrzej
Stereotactic Ablative Radiotherapy for Prostate Cancer
 Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
PACE Study. Hypofractionation 17/12/2014. Traditional Model of Fractionation 200 Response. What s the fraction sensitivity of prostate cancer?
 0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer
 Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation
 Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
Active surveillance for low-risk Prostate Cancer Compared with Immediate Treatment: A Canadian cost evaluation Alice Dragomir, PhD Fabio Cury, MD Armen Aprikian, MD Introduction Clinical and economic burden
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer
 Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
HALF. Who gets radiotherapy? Who gets radiotherapy? Half of all cancer patients get radiotherapy. By 1899 X rays were being used for cancer therapy
 The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Updated Results of High-Dose Rate Brachytherapy and External Beam Radiotherapy for Locally and Locally Advanced
 Clinical Urology High-Dose Rate Brachytherapy for Prostate Cancer International Braz J Urol Vol. 34 (3): 293-301, May - June, 2008 Updated Results of High-Dose Rate Brachytherapy and External Beam Radiotherapy
Clinical Urology High-Dose Rate Brachytherapy for Prostate Cancer International Braz J Urol Vol. 34 (3): 293-301, May - June, 2008 Updated Results of High-Dose Rate Brachytherapy and External Beam Radiotherapy
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Radiotherapy Advances
 Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings
 Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Description. Section: Therapy Effective Date: October 15, 2015 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2015 Page: 1 of 14 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2015 Page: 1 of 14 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate