Fever in Infants: Pediatric Dilemmas in Antibiotherapy
|
|
|
- Shannon Ryan
- 6 years ago
- Views:
Transcription
1 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S
2 Objectives S Review definition of fever without a source(fws) and serious bacterial infection(sbi) S Review epidemiology of FWS S Discuss clinical decision rules and their validity S Discuss Viral illness and SBI S Discuss variation in FWS management and outcomes S Review ACEP Guidelines
3 Fever Without a Source S
, documented in the clinical setting or at home within the past 24 hours* *Ann Emerg Med. 2016;67:625-639 http://kjworks.pbworks.")
4 Fever without a Source S Acute onset, duration of less than 1 week, and absence of localizing signs* S rectal temperature of greater than or equal to 38.0C (100.4F), documented in the clinical setting or at home within the past 24 hours* *Ann Emerg Med. 2016;67:
5 Fever without a Source S Most common chief complaint among infants and children presenting to an emergency department (ED) S 15% of all ED visits* S Majority of febrile children will have a benign, self-limited viral infection *CDC Hospital Rates 2011
6 Fever Without a Source S A small number (<3 months) will have a serious infection S The dilemma is to differentiate the well-appearing febrile infant or child with a SBI
7 Serious Bacterial Infection S
8 Serious Bacterial Infection SBI S The definitions vary greatly S Studies may includes bacteremia, bacterial meningitis, UTI, pneumonia, septic arthritis, osteomyelitis, cellulitis, and enteritis S Most studies define SBI as a positive culture result from a sample of blood, urine, cerebrospinal fluid, or stool

9 Epidemiology S
 http://dhhs.ne.gov/publichealth/immunization/pages/home.")
10 Prevention Strategies S Dramatic reduction in vaccine preventable infections following the widespread use of immunizations S Active prevention strategies have also decreased not vaccine preventable diseases (GBS)
11 Invasive Pneumococcal Disease (IPD) S Overall IPD incidence declined from 100 cases per 100,000 in 1998 to 9 cases per 100,000 in 2015* S IPD caused by PCV13 serotypes declined from 91 cases per 100,000 in 1998 to 2 cases per 100,000 in 2015* *
12 Invasive Pneumococcal Disease (IPD) Changes in the incidence of invasive pneumococcal disease (IPD) among children <5 years old from 1998 through 2015 in the United States. CDC Active Bacterial Core Surveillance
13 H. influenza S Since the implementation of conjugate vaccines for infants (1990) and children (1987), rates of Hib disease among children younger than five years old have declined by 99% in the United States * S Nontypeable disease now causes the majority of invasive H. influenzae disease among all age groups in the United States* *
14 Group B Streptococcus (GBS) S GBS emerged in the 1970s as the most common cause of sepsis in newborns S Early-onset disease (younger than 1 week old) has declined by 80% since increased use of intrapartum prophylaxis has occurred * *

15 Changes in Pathogens


16 Epidemiology of Bacteremia in Febrile Infants in the United States. Eric Biondi et al. Pediatrics 2013;132;990 S Retrospective Review S Positive blood culture results in febrile infants < 90 days admitted to ward S Data from ED and ward of 6 hospital systems through US,
17 Ø Non-low risk bacteremic infants were significantly more likely than low risk bacteremic infants to have E. coli (P =.001) or GBS (P =.01) Ø Infants who had S. pneumoniae bacteremia were significantly more likely to be older than infants who had other causes of bacteremia (P =.01).
18 Epidemiology of Bacteremia in Febrile Infants in the United States. Eric Biondi et al. Pediatrics 2013;132;990 S Most common pathogens were Escherichia coli (42%), group B Streptococcus (23%), and Streptococcus pneumoniae (6%) S No Listeria monocytogenes was identified S Emergence of S. aureus as a leading pathogen in bacteremia in young infants S Concurrent UTI or meningitis more common with E.coli(92%) and GBS(27%) respectively

19 Younger Infants and Clinical Decision Rules S
20 Clinical Decision Rules S Before 1985 S all febrile infants <60 days of age S hospitalized and treated with parenteral antibiotic therapy after a full sepsis evaluation S unnecessary hospitalizations, nosocomial infections, injudicious use of antibiotics, emergence of resistant bacteria, and adverse effects of antibiotics S After 1980 s S development of low risk criteria: clinical decision rules
21 Clinical Decision Rules
22 Clinical Decision Rules
23 Performance of Low-Risk Criteria S
24 Performance of Low-Risk Criteria in the Evaluation of Young Infants With Fever: Review of the Literature Anna R. Huppler, MD,a Jens C. Eickhoff, PhD,b,c and Ellen R. Wald, Mda. PEDIATRICS 2010 S Data published after 1985 from 21 studies, total of 8540 infants between 0-90 days S Objective: Determine the performance of low-risk criteria for SBIs in febrile infants S Compare prospective studies where empiric antibiotic treatment was withheld vs. studies (prospective and retrospective) in which empiric antibiotic treatment was administered S SBI: bacteremia, meningitis, bacterial diarrhea, pneumonia, and UTI
25 Performance of Low-Risk Criteria in the Evaluation of Young Infants With Fever: Review of the Literature Anna R. Huppler, MD,a Jens C. Eickhoff, PhD,b,c and Ellen R. Wald, Mda. PEDIATRICS 2010 S Prospective studies without empiric antibiotic treatment S Six patients low-risk category had SBIs S all recovered uneventfully S 2 bacteremia and 4 with UTIs S Rate of SBIs in these low-risk patients was 0.67% S Relative risk (RR) of SBIs in high-risk versus low-risk patients in these studies was (95% confidence interval: )
26 Performance of Low-Risk Criteria in the Evaluation of Young Infants With Fever: Review of the Literature Anna R. Huppler, MD,a Jens C. Eickhoff, PhD,b,c and Ellen R. Wald, Mda. PEDIATRICS 2010 S Studies with empiric antibiotic treatment of low risk patients S 89 low risk infants (2.71%) were diagnosed as having SBI s S 2 cases of meningitis (1 with UTI and 1 with bacteremia), 22 cases of bacteremia (1 with gastroenteritis and 1 with osteomyelitis), 39 cases of UTI, and 14 cases of gastroenteritis S 12 cases of SBI did not have a source identified

27 Performance of Low-Risk Criteria in the Evaluation of Young Infants With Fever: Review of the Literature Anna R. Huppler, MD,a Jens C. Eickhoff, PhD,b,c and Ellen R. Wald, Mda. PEDIATRICS 2010
28 Performance of Low-Risk Criteria in the Evaluation of Young Infants With Fever: Review of the Literature Anna R. Huppler, MD,a Jens C. Eickhoff, PhD,b,c and Ellen R. Wald, Mda. PEDIATRICS 2010 S Rate of SBIs in low-risk patients in studies without empiric antibiotic treatment was different from the rate in all other studies (0.67% vs 2.71%; P 0.01) S The total number of SBIs was 931(10.9%) consistent with rates reported in the literature S Rate of SBIs in low-risk patients in all studies was 2.23% S With the use of low-risk criteria, ~ 30% of febrile infants can be identified as being at low risk for SBIs and can be treated with observation alone
29 New Low Risk Criteria? S
30 Validation of the ''Step-by-Step'' Approach in the Management of Young Febrile Infants Borja Gomez et al. Pediatrics 2016 S Prospective study including infants 90 days with fever without source S Followed the retrospective study done on 2014 by same group with 7 European Peds ED S 11 European pediatric emergency departments between September 2012 and August 2014 S Objective: Compare the accuracy of the Step-by-Step approach, the Rochester criteria, and the Lab-score in identifying patients at low risk of IBI (invasive bacterial infection)
31 Validation of the ''Step-by- Step'' Approach in the Management of Young Febrile Infants Borja Gomez et al. Pediatrics 2016 Ø Different definitions Ø IBI(+ culture blood or CSF) Ø Non IBI(UTI or bacterial gastroenteritis) Ø Different cut off age Ø 21 days vs. 28 days
32 Validation of the ''Step-by-Step'' Approach in the Management of Young Febrile Infants Borja Gomez et al. Pediatrics 2016 S Eighty-seven(4.0%) of 2185 infants were diagnosed with an IBI S IBI higher in infants classified as high risk or intermediate risk according to the Step by Step than in low risk patients S Sensitivity and negative predictive value for ruling out an IBI S Step by Step: 92.0% and 99.3% S Rochester Criteria: 81.6% and 98.3% S Lab Score: 59.8% and 98.1% S Infants with an IBI misclassified S Step by Step: 7, Rochester criteria: 16, Lab-score: 35
33 Validation of the ''Step-by-Step'' Approach in the Management of Young Febrile Infants Borja Gomez et al. Pediatrics 2016 S The study validated the Step by Step as a valuable tool for the management of infants with fever without source in the emergency department S Confirmed its superior accuracy in identifying patients at low risk of IBI, compared with the Rochester criteria and the Lab-score


34 What about viral illness and SBI? S
35 Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis a systematic review Ralston S, Hill V, Waters A. Arch Pediatr Adolesc Med. 2011;165: S Systematic review of the literature and meta-analysis S Objective: summarize the risk of occult SBI in the youngest febrile infants presenting with clinical bronchiolitis or RSV infection S SBI: meningitis, bacteremia, and UTI S Only applies to fever evaluated at the time of presentation to an acute care setting
36 Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis a systematic review Ralston S, Hill V, Waters A. Arch Pediatr Adolesc Med. 2011;165:
37 Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis a systematic review Ralston S, Hill V, Waters A. Arch Pediatr Adolesc Med. 2011;165:
38 Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis a systematic review Ralston S, Hill V, Waters A. Arch Pediatr Adolesc Med. 2011;165: S Rate of UTI in the 11 studies analyzed was 3.3% (95% CI, 1.9%-5.7%) S No case of bacteremia was reported in 8 of 11 studies S No case of meningitis was reported in any of the studies S Clinical bronchiolitis performs better than RSV positivity in characterizing an infant as low risk for UTI
39 Occult serious bacterial infection in infants younger than 60 to 90 days with bronchiolitis a systematic review Ralston S, Hill V, Waters A. Arch Pediatr Adolesc Med. 2011;165: S Screening with cultures for SBI in febrile infants presenting with bronchiolitis or RSV infection is very low yield and a more selective approach may be rational S UTI is the only SBI reported with significant frequency S universal screening is relatively low risk S significant association with bacteremia in the youngest infants S data do not strongly support any modification to this approach S though asymptomatic bacteriuria may confound these results
40 So UTI if is the most common SBI when do we screen and treat? S
41 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Objective: Revise the American Academy of Pediatrics practice parameter regarding the diagnosis and management of initial urinary tract infections (UTIs) in febrile infants and young children

42 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics FIGURE 1 AAP evidence strengths.
43 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S For ill patients requiring antibiotics S Urine specimen is obtained for both culture and urinalysis before an antimicrobial agent is administered S specimen needs to be obtained through catheterization or supra pubic aspiration, because the diagnosis of UTI cannot be established reliably through culture of urine collected in a bag (evidence quality: A; strong recommendation)
44 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Febrile infant with no apparent source for the fever as not being so ill as to require immediate antimicrobial therapy, then the clinician should assess the likelihood of UTI (see below for how to assess likelihood) (evidence quality: A; strong recommendation).

45 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics
46 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S If the clinician determines the febrile infant to have a low likelihood of UTI then clinical follow-up monitoring without testing is sufficient (evidence quality: A; strong recommendation).
47 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Febrile infant is not in a low-risk group (see below), then there are 2 choices (evidence quality: A; strong recommendation). S obtain a urine specimen through catheterization or SPA for culture and urinalysis S obtain a urine specimen through the most convenient means and to perform a urinalysis
48 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S If the urinalysis suggest a UTI (positive leukocyte esterase test results or nitrite test or microscopic analysis results positive for leukocytes or bacteria) S urine specimen should be obtained through catheterization or SPA and cultured S If urinalysis of fresh (<1 hour since void) urine yield negative leukocyte esterase and nitrite test results S it is reasonable to monitor the clinical course without initiating antimicrobial therapy, recognizing that negative urinalysis results do not rule out a UTI with certainty
49 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics
50 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Diagnosis of UTI S both urinalysis results that suggest infection (pyuria and/or bacteriuria) and the presence of at least 50,000 colonyforming units (CFUs) per ml of a uropathogen cultured from a urine specimen obtained through catheterization or SPA (evidence quality: C; recommendation).
51 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Initiating treatment orally or parenterally is equally efficacious S Based the choice of agent on local antimicrobial sensitivity patterns (if available) and should adjust the choice according to sensitivity testing of the isolated uropathogen (evidence quality: A; strong recommendation). S choose 7 to 14 days as the duration of antimicrobial therapy (evidence quality: B; recommendation).
52 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics
53 CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children 2 to 24 Months American Academy of Pediatrics S Febrile infants with UTIs should undergo renal and bladder ultrasonography (RBUS) (evidence quality: C; recommendation). S VCUG should not be performed routinely after the first febrile UTI S indicated if RBUS reveals hydronephrosis, scarring, or other findings that would suggest either high-grade VUR or obstructive uropathy, as well as in other atypical or complex clinical circumstances (evidence quality B; recommendation). S Further evaluation should be conducted if there is a recurrence of febrile UTI (evidence quality: X;recommendation).

54 With all this evidence what s going on? S
55 Variation in Care S
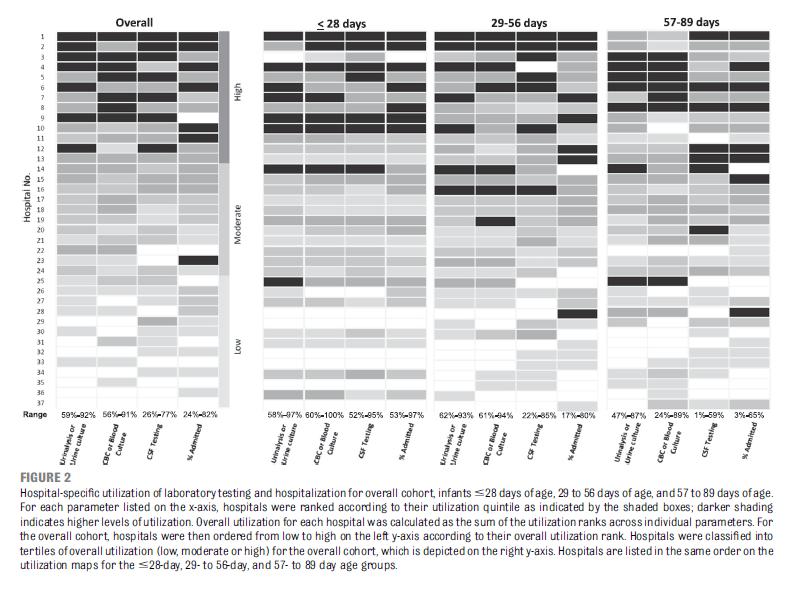
56 Variation in Care of the Febrile Young Infant <90 Days in US Pediatric Emergency Departments Paul L. Aronson, MD, et al. Pediatrics 2015 S Retrospective cohort study of infants < 90 days of age with a diagnosis code of fever S 37 pediatric Eds between July 1, June 30, 2013 S Objective: S Assessed patient and hospital level variation in testing, treatment, and disposition for patients in 3 distinct age groups: < 28, 29 to 56, and 57 to 89 days S Compare interhospital variation for 3-day revisits and revisits resulting in hospitalization
57 S
58 S
59
60 Variation in Care of the Febrile Young Infant <90 Days in US Pediatric Emergency Departments Paul L. Aronson, MD, et al. Pediatrics 2015 S Proportion of patients who underwent comprehensive evaluation decreased with increasing patient age S Significant interhospital variation in testing, treatment, and hospitalization rates overall and across all 3 age groups S but little variation in outcomes S Hospitalization rate in the overall cohort did not correlate with 3- day revisits or revisits resulting in hospitalization S Opportunities for hospitals to improve resource use for management of the febrile young infant?
61 Revisits? Sicker patients? S
62 Repeated Emergency Department Visits Among Children Admitted With Meningitis or Septicemia: A Population-Based Study Samuel Vaillancourt, MDCM, MPH et al. Annals of Emergency Medicine 2014 S Retrospective cohort study S all children aged 30 days - 5 years hospitalized with a final diagnosis of meningitis or septicemia between 2005 and 2010 S Objective: Describe the frequency of repeated emergency department visits among children admitted with meningitis or septicemia in Ontario, Canada
, critical care use (21.1% versus 16.7%, P=0.28), and mortality (P= 0.")
63 Admitted on initial visit and with repeated visits had similar median lengths of stay (13 versus 12 days, P=0.37), critical care use (21.1% versus 16.7%, P=0.28), and mortality (P= 0.86) S
64
65 Repeated Emergency Department Visits Among Children Admitted With Meningitis or Septicemia: A Population-Based Study Samuel Vaillancourt, MDCM, MPH et al. Annals of Emergency Medicine 2014 S Of 521 children,114 (21.9%) had repeated ED visits before admission S One in 3 children repeating visits returned to a different hospital S Revisit associated with older age, less acute triage score, and initial visit to a community hospital without available pediatric consultation
66 Sick Kids Look Sick?
67 Sick Kids Look Sick Steven M. Green, MD*; Lise E. Nigrovic, MD, MPH; Baruch S. Krauss, MD, EdM S Commentary S Vaillancourt et al. S children identified on a second ED visit will have a similar clinical outcome S sepsis and meningitis are not occult conditions and that, accordingly, sick kids look sick (outside of the neonatal period) S after ED discharge, a more serious infection may in rare cases develop S child will then look sick and be clinically identifiable
68 Sick Kids Look Sick Steven M. Green, MD*; Lise E. Nigrovic, MD, MPH; Baruch S. Krauss, MD, EdM S Progression of illness to sepsis or meningitis is unpredictable in normal healthy children S The addition of screening interventions is unwarranted S Sepsis and meningitis are rare S Revisits often involve different EDs S Careful evaluation remains the best approach S The status quo is working
69 What ACEP says? S
70 Clinical Policy for Well-Appearing Infants and Children Younger Than 2 Years of Age Presenting to the Emergency Department With Fever Approved by the ACEP Board of Directors, January 27, 2016 Endorsed by the Emergency Nurses Association, February 29, 2016 S
71 ACEP Policy S Systematic review of the literature for EBM recommendations S Evidence was graded and recommendations were made based on the strength of the available data
72 Guidance: Recommendations Levels S A: Generally accepted principles for patient care that reflect a high degree of clinical certainty (eg, based on evidence from 1 or more Class of Evidence I or multiple Class of Evidence II studies). S B: Patient care that may identify a particular strategy or range of strategies that reflect moderate clinical certainty (eg, based on evidence from 1 or more Class of Evidence II studies or strong consensus of Class of Evidence III studies). S C: Patient care that are based on evidence from Class of Evidence III studies or, in the absence of any adequate published literature, based on expert consensus.
73 For well appearing immunocompetent full-term infants aged 1 month to 3 months (29 days to 90 days) presenting with fever (38.0C [100.4F]) Ø are there predictors that identify patients at risk for meningitis from whom cerebrospinal fluid should be obtained? S
74 Level C recommendations S (1) Although there are no predictors that adequately identify full-term well-appearing febrile infants aged 29 to 90 days from whom CSF should be obtained the performance of a lumbar puncture may still be considered
75 Level C recommendations S (2) In the full-term well-appearing febrile infant aged 29 to 90 days diagnosed with a viral illness, deferment of lumbar puncture is a reasonable option, given the lower risk for meningitis S When LP is deferred antibiotics should be withheld unless another bacterial source is identified S Admission, close follow-up with the primary care provider, or a return visit for a recheck in the ED is needed
76 For well-appearing immunocompetent infants and children aged 2 months to 2 years presenting with fever (38.0C [100.4F]) Ø are there clinical predictors that identify patients at risk for urinary tract infection? S
77 Level C recommendations S Infants and children at increased risk for UTI include: S Females < than 12 months, uncircumcised males, nonblack race, fever duration > than 24 hours, higher fever (39C), negative test result for respiratory pathogens, and no obvious source of infection. S Although the presence of a viral infection decreases the risk, no clinical feature has been shown to effectively exclude urinary tract infection.
78 Level C recommendations S Physicians should consider urinalysis and urine culture testing to identify urinary tract infection in well-appearing infants and children aged 2 months to 2 years with a fever 38C (100.4F), especially among those at higher risk for urinary tract infection.
79 For well-appearing febrile infants and children aged 2 months to 2 years undergoing urine testing, Ø which laboratory testing method(s) should be used to diagnose a urinary tract infection? S
80 Level B recommendations S Physicians can use a positive test result for any one of the following to make a preliminary diagnosis of urinary tract infection in febrile patients aged 2 months to 2 years S urine leukocyte esterase, nitrites, leukocyte count, or Gram s stain.
81 Level C recommendations. S (1) Physicians should obtain a urine culture when starting antibiotics for the preliminary diagnosis of urinary tract infection in febrile patients aged 2 months to 2 years. S (2) In febrile infants and children aged 2 months to 2 years with a negative dipstick urinalysis result in whom urinary tract infection is still suspected, obtain a urine culture.
82 For well-appearing immunocompetent infants and children aged 2 months to 2 years presenting with fever (38.0C [100.4F]), Ø are there clinical predictor that identify patients at risk for pneumonia for whom a chest radiograph should be obtained? S
83 Level B recommendations S In well-appearing immunocompetent infants and children aged 2 months to 2 years presenting with fever (38C [100.4F]) and no obvious source of infection, physicians should consider obtaining a chest radiograph for those with cough, hypoxia, rales, high fever (39C), fever duration greater than 48 hours, or tachycardia and tachypnea out of proportion to fever.
84 Level C recommendations S In well-appearing immunocompetent infants and children aged 2 months to 2 years presenting with fever (38C [100.4F]) and wheezing or a high likelihood of bronchiolitis, physicians should not order a chest radiograph.

85 The question is what are you going to do now?
86 To Consider History Time and degree of fever Associated symptoms Follow up Past medical conditions High risk? Physical Exam Appearance Well appearing vs. ill Other source of infection
87 To Consider S Level of comfort S Risk tolerance S Experience S Parents/Family S Group practice patterns

88 Questions? S
UTI Update: Have We Been Led Astray? Disclosure. Objectives
 UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Nicolette Janzen, MD Texas Children's Hospital
 Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Advanced Pediatric Emergency Medicine Assembly
 (+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
(+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
Surveillance report Published: 7 July 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
Pediatric Urinary Tract Infections
 Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
Does This Child Have a Urinary Tract Infection?
 EVIDENCE-BASED EMERGENCY MEDICINE/RATIONAL CLINICAL EXAMINATION ABSTRACT Does This Child Have a Urinary Tract Infection? EBEM Commentator Contact Rupinder Singh Sahsi, BSc, MD Christopher R. Carpenter,
EVIDENCE-BASED EMERGENCY MEDICINE/RATIONAL CLINICAL EXAMINATION ABSTRACT Does This Child Have a Urinary Tract Infection? EBEM Commentator Contact Rupinder Singh Sahsi, BSc, MD Christopher R. Carpenter,
Group B Streptococcus
 Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Pediatric urinary tract infection. Dr. Nariman Fahmi Pediatrics/2013
 Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 66/ Aug 17, 2015 Page 11432
 BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
CLINICAL PRACTICE GUIDELINE FROM THE AMERICAN ACADEMY OF PEDIATRICS
 FROM THE AMERICAN ACADEMY OF PEDIATRICS CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children
FROM THE AMERICAN ACADEMY OF PEDIATRICS CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children
Key Definitions. Downloaded from
 Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured
 9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist
 Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Haemophilus influenzae
 Haemophilus influenzae type b Severe bacterial infection, particularly among infants During late 19th century believed to cause influenza Immunology and microbiology clarified in 1930s Haemophilus influenzae
Haemophilus influenzae type b Severe bacterial infection, particularly among infants During late 19th century believed to cause influenza Immunology and microbiology clarified in 1930s Haemophilus influenzae
Should blood cultures be obtained in all infants 3 to 36 months presenting with significant fever? abstract CLINICAL QUESTION REVIEW
 CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
more than 90% of the bacterial isolates identified as Streptococcus pneumoniae
 Research Highlights Highlights from the latest papers in pediatric emergency medicine NEWS & VIEWS Wendy L Woolley & John H Burton Author for correspondence Department of Emergency Medicine Albany Medical
Research Highlights Highlights from the latest papers in pediatric emergency medicine NEWS & VIEWS Wendy L Woolley & John H Burton Author for correspondence Department of Emergency Medicine Albany Medical
Urinary tract infections, renal malformations and scarring
 Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Children s Services Medical Guideline
 See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra
 UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
Of 142 cases where sex was known, 56 percent were male; of 127cases where race was known, 90 percent were white, 4 percent were
 Group B Streptococcus Surveillance Report 2014 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: November 2015 Background The Active Bacterial Core surveillance
Group B Streptococcus Surveillance Report 2014 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: November 2015 Background The Active Bacterial Core surveillance
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Giovanni Montini has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 Giovanni Montini has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Imaging in Pediatric UTI Giovanni Montini Milano, Italy giovanni.montini@unimi.it
Giovanni Montini has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Imaging in Pediatric UTI Giovanni Montini Milano, Italy giovanni.montini@unimi.it
Haemophilus influenzae Surveillance Report 2012 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: July 2014
 Center for Public Health Practice Updated: July 2014") Haemophilus influenzae Surveillance Report 2012 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: July 2014 Background The Active Bacterial Core surveillance (ABCs)
Haemophilus influenzae Surveillance Report 2012 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: July 2014 Background The Active Bacterial Core surveillance (ABCs)
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase
 By Dr. Lindokuhle Mahlase") UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
CHAPTER 167 Pediatric Fever
 CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Paediatrica Indonesiana. Urine dipstick test for diagnosing urinary tract infection
 Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age
 Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Urinary Tract Infections in Children: What We Know and What We Don t
 Urinary Tract Infections in Children: What We Know and What We Don t Daniel Hirselj, MD Northwest Urology, LLC North Pacific Pediatric Society Conference April 29, 2017 Urinary Tract Infections in Children:
Urinary Tract Infections in Children: What We Know and What We Don t Daniel Hirselj, MD Northwest Urology, LLC North Pacific Pediatric Society Conference April 29, 2017 Urinary Tract Infections in Children:
Diagnosis and Management of UTI s in Care Home Settings. To Dip or Not to Dip?
 Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist
 UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
Management of Pediatric Urinary Tract Infections in Kuwait: Current Practices and Practicality of New Guidelines
 June 215 KUWAIT MEDICAL JOURNAL 139 Original Article Management of Pediatric Urinary Tract Infections in Kuwait: Current Practices and Practicality of New Guidelines Entesar H Husain 1,2, Talal Al-Saleem
June 215 KUWAIT MEDICAL JOURNAL 139 Original Article Management of Pediatric Urinary Tract Infections in Kuwait: Current Practices and Practicality of New Guidelines Entesar H Husain 1,2, Talal Al-Saleem
Pneumococcal Disease and Pneumococcal Vaccines
 Pneumococcal Disease and Epidemiology and Prevention of - Preventable Diseases Note to presenters: Images of vaccine-preventable diseases are available from the Immunization Action Coalition website at
Pneumococcal Disease and Epidemiology and Prevention of - Preventable Diseases Note to presenters: Images of vaccine-preventable diseases are available from the Immunization Action Coalition website at
Guidelines for the management of urinary tract infections in children 0-17 years
 Guidelines for the management of urinary tract infections in children 0-17 years Guideline to be used where appropriate in conjunction with the Ashford and St Peter s sepsis guideline (Dr Ruth Mew 2016)
Guidelines for the management of urinary tract infections in children 0-17 years Guideline to be used where appropriate in conjunction with the Ashford and St Peter s sepsis guideline (Dr Ruth Mew 2016)
Urinary Tract Infections in Children
 Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Incidence per 100,000
 Streptococcus pneumoniae Surveillance Report 2005 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services Updated: March 2007 Background
Streptococcus pneumoniae Surveillance Report 2005 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services Updated: March 2007 Background
Haemophilus influenzae, Invasive Disease rev Jan 2018
 Haemophilus influenzae, Invasive Disease rev Jan 2018 BASIC EPIDEMIOLOGY Infectious Agent Haemophilus influenzae (H. influenzae) is a small, Gram-negative bacillus, a bacterium capable of causing a range
Haemophilus influenzae, Invasive Disease rev Jan 2018 BASIC EPIDEMIOLOGY Infectious Agent Haemophilus influenzae (H. influenzae) is a small, Gram-negative bacillus, a bacterium capable of causing a range
Urinary tract infection and hyperbilirubinemia
 The Turkish Journal of Pediatrics 2006; 48: 51-55 Original Urinary tract infection and hyperbilirubinemia Hülya Bilgen 1, Eren Özek 1, Tamer Ünver 1, Neşe Bıyıklı 2 Harika Alpay 2, Dilşat Cebeci 3 Divisions
The Turkish Journal of Pediatrics 2006; 48: 51-55 Original Urinary tract infection and hyperbilirubinemia Hülya Bilgen 1, Eren Özek 1, Tamer Ünver 1, Neşe Bıyıklı 2 Harika Alpay 2, Dilşat Cebeci 3 Divisions
Appendix A: Disease-Specific Chapters
 Ministry of Health and Long-Term Care Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Haemophilus influenzae disease, all types, invasive Effective: May 2018 Haemophilus influenzae,
Ministry of Health and Long-Term Care Infectious Diseases Protocol Appendix A: Disease-Specific Chapters Chapter: Haemophilus influenzae disease, all types, invasive Effective: May 2018 Haemophilus influenzae,
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P.
 Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
PDFlib PLOP: PDF Linearization, Optimization, Protection. Page inserted by evaluation version
 PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com ACAD EMERG MED d December 2004, Vol. 11, No. 12 d www.aemj.org 1297 A Low Peripheral
PDFlib PLOP: PDF Linearization, Optimization, Protection Page inserted by evaluation version www.pdflib.com sales@pdflib.com ACAD EMERG MED d December 2004, Vol. 11, No. 12 d www.aemj.org 1297 A Low Peripheral
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Medline Abstracts for References 15,30-37
 Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Medline Abstracts for References 15,30-37 of 'Fever without a source in children 3 to 36 months of age' 15 Check for full text
Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Medline Abstracts for References 15,30-37 of 'Fever without a source in children 3 to 36 months of age' 15 Check for full text
Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach. No disclosures. Importance of Topic 5/14/11. Biases
 Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach Thomas B. Newman, MD, MPH Professor of Epidemiology & Biostatistics and Pediatrics University of California, San Francisco May
Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach Thomas B. Newman, MD, MPH Professor of Epidemiology & Biostatistics and Pediatrics University of California, San Francisco May
REVIEW ARTICLE. Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With Bronchiolitis
 REVIEW ARTICLE Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With A Systematic Review Shawn Ralston, MD; Vanessa Hill, MD; Ami Waters, MD Objective: To summarize the risk of
REVIEW ARTICLE Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With A Systematic Review Shawn Ralston, MD; Vanessa Hill, MD; Ami Waters, MD Objective: To summarize the risk of
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
CRACKCast E167 Pediatric Fever. Key Concepts. CrackCast Show Notes Pediatric Fever April 2018
 CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Preventing & Controlling the Spread of Infection
 Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Fever is one of the most frequent reasons for consultation in
 ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
ArchCare ASB:Proposed Guidelines-DS-8/17/12 Pg 1 of 5 ArchCare Proposed Clinical Guidelines: Asymptomatic Bacteriuria
 Pg 1 of 5 ArchCare Proposed Clinical Guidelines: Asymptomatic Bacteriuria Asymptomatic Bacteriuria (ASB) is defined as a positive urine culture obtained from a person without signs or symptoms referable
Pg 1 of 5 ArchCare Proposed Clinical Guidelines: Asymptomatic Bacteriuria Asymptomatic Bacteriuria (ASB) is defined as a positive urine culture obtained from a person without signs or symptoms referable
Recurrent Pediatric UTI Revisited 2013
 Recurrent Pediatric UTI Revisited 2013 PIDSP 21.2.2013 Shai Ashkenazi, MD, MSc Medicine changes constantly Some aspects of the standard practice of ~40 years are probably not valid and need to be changed
Recurrent Pediatric UTI Revisited 2013 PIDSP 21.2.2013 Shai Ashkenazi, MD, MSc Medicine changes constantly Some aspects of the standard practice of ~40 years are probably not valid and need to be changed
Pneumococcal Vaccine in Children: current situation
 Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
UTI and VUR practical points and management
 UTI and VUR practical points and management Søren Rittig, Prof., DMSc Child and Adolescent Medicine, Aarhus University Hospital Aarhus, Denmark Outline Definition and diagnosis of UTI Treatment of UTI
UTI and VUR practical points and management Søren Rittig, Prof., DMSc Child and Adolescent Medicine, Aarhus University Hospital Aarhus, Denmark Outline Definition and diagnosis of UTI Treatment of UTI
Ancillary Testing in Children with Rotavirus Gastroenteritis
 ORIGINAL RESEARCH Ancillary Testing in Children with Rotavirus Gastroenteritis Peter A. Rowinsky, MD 1,2 Andrew P. Steenhoff, MBBCh, DCH (UK), FCP (SA) Paed 3,4,5,6,7 Shiang-Ju Kung, MBBCh, DCH (SA) 8
ORIGINAL RESEARCH Ancillary Testing in Children with Rotavirus Gastroenteritis Peter A. Rowinsky, MD 1,2 Andrew P. Steenhoff, MBBCh, DCH (UK), FCP (SA) Paed 3,4,5,6,7 Shiang-Ju Kung, MBBCh, DCH (SA) 8
'Diagnostic Stewardship for Urinary Tract Infections. Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC
 'Diagnostic Stewardship for Urinary Tract Infections Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC Objectives Describe the difference between asymptomatic
'Diagnostic Stewardship for Urinary Tract Infections Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC Objectives Describe the difference between asymptomatic
Diagnosis of Pneumococcal Disease
 Diagnosis of Pneumococcal Disease Limitations of Surveillance for Invasive Disease David Murdoch University of Otago, Christchurch New Zealand Key Points We are still reliant on culture-based methods for
Diagnosis of Pneumococcal Disease Limitations of Surveillance for Invasive Disease David Murdoch University of Otago, Christchurch New Zealand Key Points We are still reliant on culture-based methods for
PYELONEPHRITIS. Wendy Glaberson 11/8/13
 PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
Antibiotic Stewardship and the Misdiagnosis of UTI
 Antibiotic Stewardship and the Misdiagnosis of UTI Daniel J. Pallin, MD, MPH Director of Research, Department of Emergency Medicine Chairman, Clinical Investigation Committee Brigham and Women s Hospital
Antibiotic Stewardship and the Misdiagnosis of UTI Daniel J. Pallin, MD, MPH Director of Research, Department of Emergency Medicine Chairman, Clinical Investigation Committee Brigham and Women s Hospital
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
10/11/2017 TOPICS FOR TODAY THE FEBRILE CHILD IS THERE TRUTH IN GOOGLE? EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT?
 EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT? Richard M. Cantor, MD FAAP/FACEP Professor of Emergency Medicine and Pediatrics Director of Pediatric Emergency Services Director, Pediatric
EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT? Richard M. Cantor, MD FAAP/FACEP Professor of Emergency Medicine and Pediatrics Director of Pediatric Emergency Services Director, Pediatric
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Acute fever without an apparent Source in Young Children: Experience of the pediatric medical emergency department of Rabat
 Acute fever without an apparent Source in Young Children: Experience of the pediatric medical emergency department of Rabat Hanane EL OUARDI, Brahim ELGAJOUI, Lamya KARBOUBI, Badr Sououd Benjelloun Dakhama
Acute fever without an apparent Source in Young Children: Experience of the pediatric medical emergency department of Rabat Hanane EL OUARDI, Brahim ELGAJOUI, Lamya KARBOUBI, Badr Sououd Benjelloun Dakhama
Evelyn A. Kluka, MD FAAP November 30, 2011
 Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which
Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which