Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
|
|
|
- Elvin Stevenson
- 5 years ago
- Views:
Transcription
1 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
2 Disclosures I have nothing to disclose
3 Learning Objectives At the end of the talk, participants should be able to 1. Recognize different models for evaluating febrile babies 2. Develop a plan for addressing fever in infants and children

4
5

6 Occult bacteremia in outpatients
7 McGowan etc June 21, 1973 N Engl J Med 1973; 288:
8 Untreated, unsuspected bacteremia with: N % meningitis % focal infection S. pneumoniae % 10.5% H. influenzae 15 20% 60% N. meningitidis 11 36% 63.6% Woods AJDC 1983;137:544 Dashefsky J Peds 1983 Sullivan PEDS 1987
9


10



11

12
13
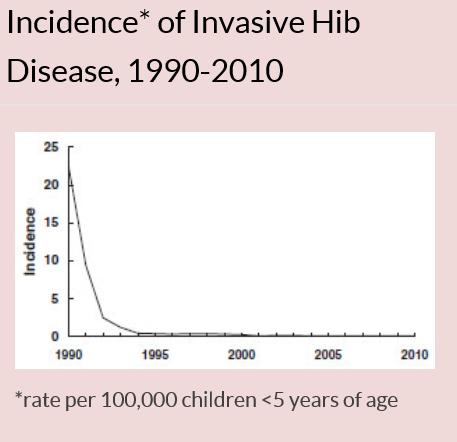
14 Rates of pneumococcal disease in children < 5 years

15 Occult bacteremia in outpatients
16 Strategies to treat suspected cases of bacteremia High risk groups Low risk Groups (Rochester criteria, etc)
17 Fever as Predictor of Bacteremia Temp (F) McGowan Teele Waskerwitz < 102 2/212 (0.9) 0/ /122 (4.1) 19/459 (4.1) /150 (8.7) *** 17/292 (5.8) /112 (8.0) *** > 105 1/16 (6.2)
18 High Fever and Bacteremia T (Celsius) N % / / >41 15/58 26 McCarthy. Pediatrics 1977;59:663
19 WBC as Predictor of Bacteremia Baraff,Pediatr Annals Aug 1993 Study Ages Temp ( o C) N WBC < 15k WBC >15k Teele 1-24 > Murray 3-24 > Schwartz 2-36 > Carrol 6-24 > Jaffe 3-36 > Bass Bass 3-36 > TOTAL
20 low risk vs non-toxic Probability of bacterial infection in infants < 90 days of age Low risk Nontoxic Toxic SBI 1.4% 8.6% 17.3% Bacteremia 1.1% 2.0% 10.7% Meningitis 0.5% 1.0% 3.9% Baraff LJ. Pediatr Infect Dis J 1992;11:
21 Social Smile and Bacteremia Present n=250 Absent n=262 p value Gender 49% female 44% female 0.26 Age (mo) WBC (x 1000) Temp Fever duration Bacteremia 26 of of Bass, Wittler, Weisse. Pediatr Infect Dis J 1996
22
23


24 Management of Infants and Young Children with Fever without Source Baraff, Larry J, MD. Pediatric Annals; Vol. 37, Iss. 10, (Oct 2008):


25 Febrile Infant CPG at 21 Children s Hospitals Association of clinical practice guidelines with emergency department management of febrile infants 56 days of age. Aronson Pl, et al J Hosp Med Jun;10(6):


26 Traffic light system for identifying risk of serious illness National Institute for Health & Care Excellence 2013 National Guidelines, London
27 Sick vs Not Sick Focus vs No Focus Well vs Unwell
28 15 m/o boy 3 days of fever Previously well- normal development 3 day history of fussiness, fever UTD on vaccines - Prevnar x 3 No focus on exam
29 What work-up would you do? A. UA & UC B. CBC, UA & UC C. CBC, BC, UA & UC D. Reassurance, watchful waiting
30 Same patient, but also RSV (+) A. UA & UC B. CBC, UA & UC C. CBC, BC, UA & UC D. Reassurance, watchful waiting
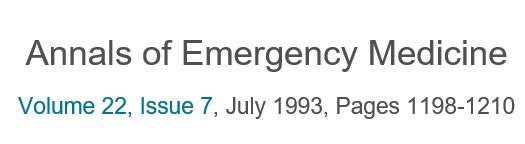
31 CBC H/H 9.5/28.9 WBC 7.5 (31p45b21l) BC: S. pneumoniae type 6A CSF WBC: 3625 Glucose: 32 Protein: 284


32 Bilateral frontal infarcts T2 DWI
33 10 m/o boy 1 day of fever Previously well- normal development Seen in ER with 1 day of fever, 12 hour so vomiting, loose stool UTD on vaccines - Prevnar x 3 No focus on exam
34 What work-up would you do? A. UA & UC B. CBC, UA & UC C. CBC, BC, UA & UC D. Reassurance, watchful waiting
35 CBC H/H 10.1/30.5 WBC 28.3 (71p2b21l) BMP 137/ / 17 16/ Fluid Bolus x 2 139/ / 16 14/.03
36 Admitted to Pediatric ward around 7 a.m. On rounds at 10:30, parents and baby were sleeping, so they were not interrupted Intern mentions that since WBC was elevated, maybe we should get a BC and give a dose of Ceftriaxone. Attending and SR remark that the guidelines state that CBC was not even recommended, and WBC is no longer a discriminator.

37 What would you do? A. Continue to watch clinically B. Send a blood culture, do not give antibiotics C. Give antibiotics, no BC is needed D. Send a blood culture and give ceftriaxone
38 At 1:30 p.m. parents called nurse to room Child was having extensor posturing A code was called Intubated, BC drawn, Vanc/Ceftazidime started CT scan showed herniation Blood culture grew S. pneumo (non-vaccine strain)

39

40
41

42 Hospital Pediatrics Vol 2, Issue 2, 2012
43 The emerged themes were fear of complications by 18 (75%), perception that LP was unnecessary by 5 (21%), and distrust of the motives behind the request for consent. Fear of paralysis and conviction that LP is unnecessary encompassed 80% of the causes for refusal. Eleven families (46%) stated that nothing would have made them consent, and 10 (42%) would agree only if the child looked unwell or deteriorated.
44
45 Let s divide the risk people are worried about into two components. The technical side of the risk focuses on the magnitude and probability of undesirable outcomes: paralysis, other complication, poorly performed procedure, discomfort of their child. Call all this hazard. The non-technical side of the risk focuses on everything negative about the situation itself (as opposed to those outcomes). Is it voluntary or coerced, familiar or exotic, dreaded or not dreaded? Are you trustworthy or untrustworthy, responsive or unresponsive? Call all of this outrage.
46 My recommendations 0-30 days- Temp 38 Complete work-up for all babies Blood, Urine CSF HSV PCR and Acyclovir for babies with seizures, skin lesions, CSF lymphocytosis, elevated ALT/AST days- Temp of 38.3 Toxic- Full evaluation Unwell- Urine and WBC Well- Urine
47 My recommendations 3-6 month- Temp of 39 Toxic- Full evaluation Unwell- CBC, BC, Urine Well- Urine > 6 months, fully immunized- Temp of 39.5 Non-Toxic- CBC, Urine Well- Urine or nothing >6 months, under-immunized- Temp of 39.5 CBC, BC, Urine
48 What if there is a focus on exam? Is a Recognizable Viral Syndrome a focus? NB: Vomiting is not a focus, it is a RED FLAG
49 < 3 mo
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Should blood cultures be obtained in all infants 3 to 36 months presenting with significant fever? abstract CLINICAL QUESTION REVIEW
 CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P.
 Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Managing meningitis not just antibiotics. Helena White December 2013
 Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Managing meningitis not just antibiotics Helena White December 2013 Case history 43 year old British-born Asian lady Legal advisor Married with a three year old child (on Amoxicillin for recent ear infection)
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Fever without Localizing Signs
 PART II Clinical Syndromes and Cardinal Features of Infectious Diseases: Approach to Diagnosis and Initial Management SECTION B Cardinal Symptom Complexes 14 Fever without Localizing Signs Eugene D. Shapiro
PART II Clinical Syndromes and Cardinal Features of Infectious Diseases: Approach to Diagnosis and Initial Management SECTION B Cardinal Symptom Complexes 14 Fever without Localizing Signs Eugene D. Shapiro
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases") Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
Fever without a source. Management of Febrile Infants (0 3 months) or Please, can t I just send them home? Saturday Night Fever
 or Please, can t I just send them home? Saturday Night Fever") Saturday Night Fever Management of Febrile Infants (0 3 months) or Please, can t I just send them home? K. Alexander, M.D. Section of Pediatric Infectious Diseases Fever without a source! Normal infants
Saturday Night Fever Management of Febrile Infants (0 3 months) or Please, can t I just send them home? K. Alexander, M.D. Section of Pediatric Infectious Diseases Fever without a source! Normal infants
REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3
 REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3 HOW TO CITE THIS ARTICLE: Amita Jane D Souza, Anil Shetty, Divya Krishnan
REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3 HOW TO CITE THIS ARTICLE: Amita Jane D Souza, Anil Shetty, Divya Krishnan
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster
 Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Hot Stuff: The Febrile Child
 Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Advanced Pediatric Emergency Medicine Assembly
 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
(+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Fever in children aged less than 5 years
 Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Welcome to Big Sky Country. Pediatrics Infectious disease update. Todd TwogoodMD
 Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Fever in the Pediatric Patient (part one)
") Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
My kid is always sick!!
 Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Status Epilepticus in Children
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Fever is one of the most frequent reasons for consultation in
 ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
ORIGINAL STUDIES Impact of Rapid Viral Testing for Influenza A and B Viruses on Management of Febrile Infants Without Signs of Focal Infection Javier Benito-Fernández, MD, Miguel A. Vázquez-Ronco, MD,
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Case Report. Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage
 1 Case Report Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage Authors: Shila, MD, *Jessica Erfan, MPAS, PA-C, Ray Bogitch, MD, Jefferson T. Miley, MD Department of Neurology, Dell
1 Case Report Herpes simplex virus encephalitis presenting as frontal lobe hemorrhage Authors: Shila, MD, *Jessica Erfan, MPAS, PA-C, Ray Bogitch, MD, Jefferson T. Miley, MD Department of Neurology, Dell
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Journal of Pediatric Sciences
 Journal of Pediatric Sciences Buccal Cellulitis in 3 Infants Martin W Stallings Journal of Pediatric Sciences 2016;8:e252 http://dx.doi.org/10.17334/jps.78460 How to cite this article: Stallings MW. Buccal
Journal of Pediatric Sciences Buccal Cellulitis in 3 Infants Martin W Stallings Journal of Pediatric Sciences 2016;8:e252 http://dx.doi.org/10.17334/jps.78460 How to cite this article: Stallings MW. Buccal
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements
![Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements](/thumbs/77/74744886.jpg "Case Study 6C. [TQ, 7-months-old infant girl] Dengue Clinical Management. Acknowledgements") Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
Case Study 6C [TQ, 7-months-old infant girl] Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from the University of Malaya Medical Centre. Materials
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases
 Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Online Video Library Pediatric Emergency Room Puzzlers
 Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
Fever Paul L. McCarthy. DOI: /pir
 Paul L. McCarthy Pediatr. Rev. 1998;19;401 DOI: 10.1542/pir.19-12-401 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://pedsinreview.aappublications.org/cgi/content/full/19/12/401
Paul L. McCarthy Pediatr. Rev. 1998;19;401 DOI: 10.1542/pir.19-12-401 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://pedsinreview.aappublications.org/cgi/content/full/19/12/401
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Urinary tract infection (UTI) in children. Children s Hospital. Information for Parents and Carers DRAFT. University Hospitals of Leicester.
 in children. Children s Hospital. Information for Parents and Carers DRAFT. University Hospitals of Leicester.") Urinary tract infection (UTI) in children Children s Hospital Information for Parents and Carers University Hospitals of Leicester NHS Trust Acute Open Access to Children s Hospital Your child (Insert
Urinary tract infection (UTI) in children Children s Hospital Information for Parents and Carers University Hospitals of Leicester NHS Trust Acute Open Access to Children s Hospital Your child (Insert
Evaluating Fever in Infants. Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist
 Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California. a complete physical examination,
 Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
Bacterial meningitis
 Bacterial meningitis Children s Ward Parent/Carer Information Leaflet What is meningitis? Meningitis is an infection that causes inflammation (swelling) of the meninges. The meninges are protective membranes
Bacterial meningitis Children s Ward Parent/Carer Information Leaflet What is meningitis? Meningitis is an infection that causes inflammation (swelling) of the meninges. The meninges are protective membranes
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
The evaluation of well-appearing febrile children
 CLINICAL PRACTICE Prevalence of Occult Bacteremia in Children Aged 3 to 36 Months Presenting to the Emergency Department with Fever in the Postpneumococcal Conjugate Vaccine Era Matthew Wilkinson, MD,
CLINICAL PRACTICE Prevalence of Occult Bacteremia in Children Aged 3 to 36 Months Presenting to the Emergency Department with Fever in the Postpneumococcal Conjugate Vaccine Era Matthew Wilkinson, MD,
Practice Guideline for the Management of Infants and Children 0 to 36 Months of Age With Fever Without Source
 CONCEPTS.fever, pediatric Practice Guideline for the Management of Infants and Children 0 to 36 Months of Age With Fever Without Source From the UCLA Emergency Medicine Center, Los Angeles, California;*
CONCEPTS.fever, pediatric Practice Guideline for the Management of Infants and Children 0 to 36 Months of Age With Fever Without Source From the UCLA Emergency Medicine Center, Los Angeles, California;*
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
GUIDELINE FOR THE MANAGEMENT OF
 GUIDELINE FOR THE MANAGEMENT OF Reference: Febrile Convulsions Version No: 1 Applicable to All children admitted with Febrile Convulsion to the Children s Hospital for Wales Classification of document:
GUIDELINE FOR THE MANAGEMENT OF Reference: Febrile Convulsions Version No: 1 Applicable to All children admitted with Febrile Convulsion to the Children s Hospital for Wales Classification of document:
Blue Babies, Twitchy Toddlers, and Kool Kids. By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN
 Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Vaccine Information Statement: PEDIATRIC VACCINES (Multiple)
") Vaccine Information Statement: PEDIATRIC VACCINES (Multiple) 1. Your Baby s First Vaccines: What You Need to Know Babies get six vaccines between birth and 6 months of age. These vaccines protect your
Vaccine Information Statement: PEDIATRIC VACCINES (Multiple) 1. Your Baby s First Vaccines: What You Need to Know Babies get six vaccines between birth and 6 months of age. These vaccines protect your
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Factors predicting bacterial meningitis in children aged 6-18 months presenting with first febrile seizure
 International Journal of Contemporary Pediatrics Khosroshahi N et al. Int J Contemp Pediatr. 2016 May;3(2):537-541 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Research Article DOI: http://dx.doi.org/10.18203/2349-3291.ijcp20161033
International Journal of Contemporary Pediatrics Khosroshahi N et al. Int J Contemp Pediatr. 2016 May;3(2):537-541 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Research Article DOI: http://dx.doi.org/10.18203/2349-3291.ijcp20161033
2/27/19 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019
 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019 1 OBJECTIVES v Understand the ddx and management of abdominal masses in kids v Understand strategies for dealing
TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019 1 OBJECTIVES v Understand the ddx and management of abdominal masses in kids v Understand strategies for dealing
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
Meningococcal. Disease. Know the. symptoms. Don t wait talk to your doctor or nurse
 Meningococcal Disease Know the symptoms Don t wait talk to your doctor or nurse Meningococcal disease Meningococcal disease is an infection caused by a bacteria, and can lead to two very serious illnesses:
Meningococcal Disease Know the symptoms Don t wait talk to your doctor or nurse Meningococcal disease Meningococcal disease is an infection caused by a bacteria, and can lead to two very serious illnesses:
CRACKCast E167 Pediatric Fever. Key Concepts. CrackCast Show Notes Pediatric Fever April 2018
 CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
Diagnosing and managing sepsis in children
 Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
Continuing malaria education modules. Module 1 Severe malaria triage, diagnosis, and treatment
 The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
more than 90% of the bacterial isolates identified as Streptococcus pneumoniae
 Research Highlights Highlights from the latest papers in pediatric emergency medicine NEWS & VIEWS Wendy L Woolley & John H Burton Author for correspondence Department of Emergency Medicine Albany Medical
Research Highlights Highlights from the latest papers in pediatric emergency medicine NEWS & VIEWS Wendy L Woolley & John H Burton Author for correspondence Department of Emergency Medicine Albany Medical
Diagnosis of Pneumococcal Disease
 Diagnosis of Pneumococcal Disease Limitations of Surveillance for Invasive Disease David Murdoch University of Otago, Christchurch New Zealand Key Points We are still reliant on culture-based methods for
Diagnosis of Pneumococcal Disease Limitations of Surveillance for Invasive Disease David Murdoch University of Otago, Christchurch New Zealand Key Points We are still reliant on culture-based methods for
Risk Management in an Office Setting: Who are we sending home?
 Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Which Diseases Should My Child Be Protected Against?
 What is Immunization? Immunization is a process that helps your body fight off diseases caused by certain viruses and bacteria. One way for you to be immunized is to receive a vaccine. What is a Vaccine?
What is Immunization? Immunization is a process that helps your body fight off diseases caused by certain viruses and bacteria. One way for you to be immunized is to receive a vaccine. What is a Vaccine?
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN
 MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
MANAGEMENT OF SUSPECTED VIRAL ENCEPHALITIS IN CHILDREN OVERVIEW 1980s: dramatically improved by aciclovir HSV encephalitis in adults Delays treatment(> 48h after hospital admission): associated with a
Guillain-Barré Syndrome in a Patient with Pneumococcal Meningitis
 Guillain-Barré Syndrome in a Patient with Pneumococcal Meningitis An Uncommon Complication of a Common Infection ACP Wisconsin, September 2017 Jesse Maupin, MD (PGY-2) University of Wisconsin Hospital
Guillain-Barré Syndrome in a Patient with Pneumococcal Meningitis An Uncommon Complication of a Common Infection ACP Wisconsin, September 2017 Jesse Maupin, MD (PGY-2) University of Wisconsin Hospital
Fever in the Pediatric Office Practice
 Fever in the Pediatric Office Practice Jane Murahovschi J Pediatr (Rio J) 2003; 79 Suppl 1:S55-S64 Lester A. Deniega, M.D. Abstract Objective: 1. To determine how to select a child who requires in depth
Fever in the Pediatric Office Practice Jane Murahovschi J Pediatr (Rio J) 2003; 79 Suppl 1:S55-S64 Lester A. Deniega, M.D. Abstract Objective: 1. To determine how to select a child who requires in depth
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy