Case Presentation. Alireza Sadeghi MD Lutheran Medical Center University Hospital of Brooklyn Downstate Medical Center March 10 th 2006
|
|
|
- Shona Walton
- 6 years ago
- Views:
Transcription
1 Case Presentation Alireza Sadeghi MD Lutheran Medical Center University Hospital of Brooklyn Downstate Medical Center March 10 th 2006
2 Case Presentation xx years old Caucasian Male History of Stage III Colon Cancer in xxxx year S/P Resection and Chemotherapy Presented to Thoracic Service at LMC for elective VATS & Pulmonary Resection for a 3.1 cm lesion in the Right Lower Lobe on date. Denied SOB, Weight Loss, Cough, Hemoptysis No other complaints
3 Case Presentation Past Medical History: DM, BPH, HTN Past Surgical History: Colon Cancer (date): S/P resection and chemotherapy Pulmonary Metastasectomy (date) for metastatic colon CA: Left upper lobectomy Bladder Cancer (date): TURBT Allergies: PCN Medications: Proscar Glipizide Cozaar Multivitamins Social History: 51 Pk yr Tobacco EtOH
4 Case Presentation Vital Signs Temp: 98.1 F BP: 108/61 HR: 70 RR: 18 O 2 Sat: 100 % RA Physical Exam No cervical adenopathy No head/neck/arm edema Chest: CTA B/L RRR, S 1 & S 2, no murmurs Abd: S/ND/NT/+BS Exterm: 2+ distal pulses Neuro: Intact
5 Preoperative Labs: Case Presentation WBC: 7.5 Hgb/HCT: 15.3/46.3 Plts: 170 Chem: 144/5.0/108/28/21/1.1/115 INR: 0.9 CEA level: ng/ml since initial surgery in (date) ABG: 7.45/37/85/25.6/+1.8/99%
6 Case Presentation Cardiac Catheterization: LV Function: Normal EF 55% Non obstructive CAD Minimal MR
7 Case Presentation Pulmonary Function Tests: Parameters Predicted Actual % Predicted FVC 4.87 L 3.63 L 75 FEV L 2.78 L 72 FEV1/FVC 78 % 77% NA FEF 25-75% 3.79 L/sec 1.81 L/sec 48 MVV 142 L/min 98 L/min 69 TLC 7.27 L 6.22 L 86 DLCO (ml/min/mmhg)
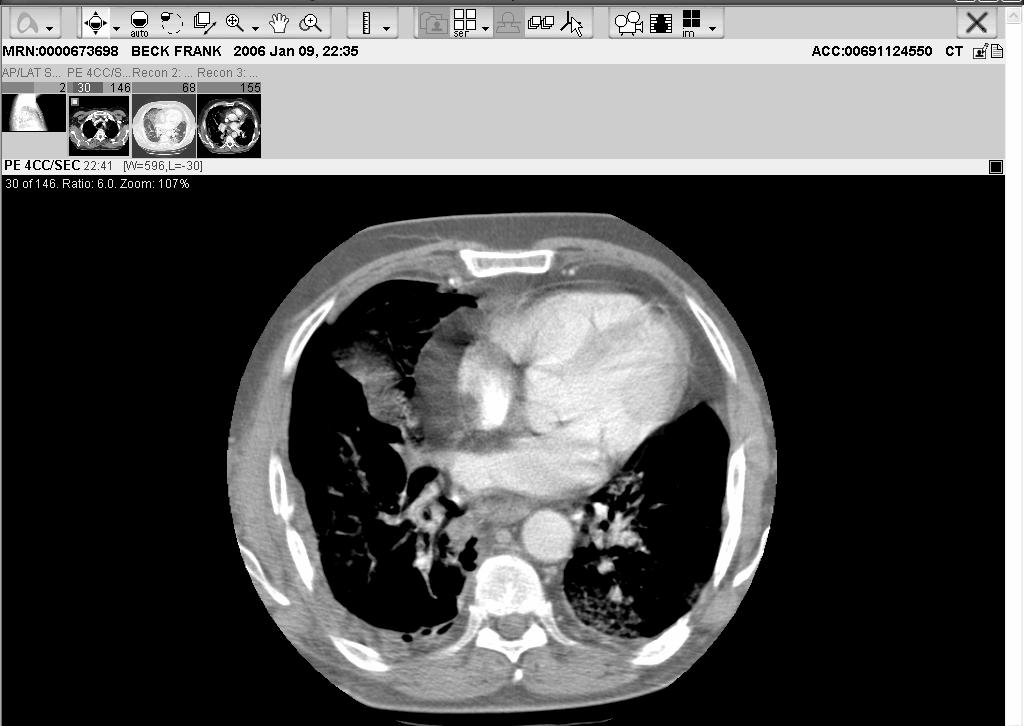
8 Case Presentation Imaging: Surveillance CT Scan (date) Lobulated mass in the RLL; posteriomedial location 3.1 x 2.5 x 2.8 cm No Axillary LN involvement Previous Surveillance CT Scans did not reveal any lesions 10/28/ /12/ /03/2003 PET Scan (date) Single Hyper metabolic focus in the Right Lower Lobe

9 Case Presentation Operative Course: Bronchoscopy: No intraluminal lesions Double lumen ET intubation SCD Boots Patient positioned in R Thoracotomy position Right VATS performed Patient tolerates LLL ventilation: O 2 Sat 97-99% Unable to safely remove the lesion due to its location Procedure abandoned Right Muscle Sparing Thoracotomy performed

10 Case Presentation Operative Course: Exploratory Right Thoracotomy: Lesion not amenable to wedge resection due to central location Decision made to perform a complete right lower lobectomy EBL: 900 cc 2 chest tubes inserted and the chest was closed. Patient tolerated procedure well.
11 Case Presentation Pathology Report: Right Lower Lobe Metastatic Moderately Differentiated Adenocarcinoma 3.1 cm x 2.9 cm x 2.8 cm Solitary Lesion Histologically compatible with Colonic Origin
12 Case Presentation Postoperative Course: POD #1: SICU Supportive Management: 2U PRBC & Pressor Support HCT Extubated successfully SCD boots No evidence postoperative MI Chest Tubes: 1200 cc/24 hr Post Extubation ABG on 3 L NC: 7.42/34.9/153/22/-1.9/99%

13
14 Case Presentation Postoperative Course: POD #2: SICU Supportive Care/SCD Boots & HSC Chest tubes: 300 cc/24 hrs Apical CT removed Diet Advanced POD #3: Floor OOB/Incentive Spirometry/SCD Boots & HSC Chest tube: 130 cc/24 hrs CXR: mild atelectasis
15 Case Presentation Postoperative Course: POD #4: Floor Acute SOB with desaturation to 90% Afebrile/VSS/No evidence of MI ABG: 7.46/36/225/25/+1.9/100% on NRB mask A-a Gradient: 371 CTA Chest: Large hypo dense filling defect within R Middle Lobe PA B/L Pneumonitis Lower Extremity Duplex: No evidence of DVT Heparin Anticoagulation Started/Broad Spectrum Abx Transferred to ICU
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40 Case Presentation Postoperative Course: POD #5: ICU Brief initial improvement IV Anticoagulation therapeutic/warfarin started Respiratory Distress continues Medical Oncology team assumes care of patient Oxygen Saturation 90-93% on NRB Mask Patient maintained on BIPAP ventilation INR therapeutic 2.9 Transferred to MICU
41 Case Presentation Postoperative Course: POD #5: MICU Continued Respiratory Failure Patient deteriorates BIPAP ABG: 7.45/41/63/28/+3.3/93% POD #6: MICU Fulminant Respiratory Failure BIPAP ABG: 7.47/38/28 Cardiac Arrest/Unsuccessful ACLS Pt Expired.
42 Preoperative Evaluation for Lung Resection Surgery Alireza Sadeghi MD University Hospital of Brooklyn Downstate Medical Center March 10 th 2006
43 Spirometry Recording of the volume of air inhaled & exhaled, plotted against time, during a series of Ventilatory maneuvers. Results depict a Normal vs. Abnormal pattern of Ventilatory reserve Obstructive Restrictive Mixed Disorders Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
44 Mazzone PJ et al. Interpreting pulmonary function tests. Cleveland Clinic Journal Medicine 2003; 70(10):

45 Terminology Mazzone PJ et al. Interpreting pulmonary function tests. Cleveland Clinic Journal Medicine 2003; 70(10):
46 Terminology Forced vital capacity (FVC): Total volume of air that can be exhaled forcefully from TLC The majority of FVC can be exhaled in <3 seconds under normal circumstances Measured in liters (L)
47 Terminology Forced expiratory volume in 1 second: (FEV 1 ) Volume of air forcefully expired from full inflation (TLC) in the first second Measured in liters (L) Normally more than 75-80% of FVC is exhaled in the first second
48 Terminology Forced expiratory flow 25-75% (FEF ) Mean forced expiratory flow during middle half of FVC Measured in L/sec May reflect effort independent expiration and the status of the small airways Highly variable
49 FVC Interpretation of % predicted: % Normal 70-79% Mild reduction 50%-69% Moderate reduction <50% Severe reduction FEV 1 Interpretation of % predicted: >75% Normal 60%-75% Mild obstruction 50-59% Moderate obstruction <49% Severe obstruction
50 FEF Interpretation of % predicted: >60% Normal 40-60% Mild obstruction 20-40% Moderate obstruction <10% Severe obstruction
51 Introduction Statistics from Center for Disease Control & Prevention About 30,000 lung resections are performed annually in the United States Commonly performed surgeries for lung cancer include Pneumonectomy Lobectomy Wedge Resection Segmentectomy Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
52 Introduction Indications for Pulmonary Resection: Neoplastic Disease Primary Metastatic Bullous Lung Disease: LVRS Diagnosis & Management of inflammatory conditions Granulomas Pulmonary infiltrates Resection of segments destroyed by bronchiectasis Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
53 Introduction Recent Studies: Mortality Rates Pneumonectomy: 6.8% 1 & 5.7% 2 Bilobectomy: 4.4 % 2 Lobectomy: 3.9% 1 Lesser Resection: 1.4% 2 Risk of morbidity & mortality mandatory to assess as accurately as possible which patients with anatomically resectable disease are suitable candidates for resectional surgery 1. Kadri MA et al Survival and prognosis following resection of primary non-small cell bronchogenic carcinoma. Eur J Cardiovasc Surg 1991; 5: Damhuis et al. Resection rates and postoperative mortality in 7899 patients with lung cancer. Eur Respir J 1996; 9:7 10.
54 Purpose The Purpose of Preoperative Physiologic Assessment: Using the least invasive test possible Identify the High Risk Patient Complications Long term Disability Adequately Counsel the patient on treatment options and risks to make an informed decision Identify possible steps to reduce risks of peri-operative complications & long-term pulmonary disability Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S
55 Complications Postoperative Cardiopulmonary Complications Acute Hypercapnia Mechanical Ventilation > 48hrs Arrhythmias Pneumonia Pulmonary Emboli Myocardial Infarction Lobar Atelectasis requiring Bronchoscopy
56 Preoperative Evaluation Who should be evaluated? The general answer History All patients undergoing lung resection surgery, irrespective of age or extent of the lesion. Smoking & COPD Preoperative Medical Optimization Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
57 Pulmonary-Specific Evaluation The aims of pulmonary-specific evaluation Assessment of the patient s physiologic pulmonary function Determining the patient candidacy for surgery and the extent of resection that can be tolerated. There is no single measure that is a gold standard in accurately predicting complications. However, certain criteria, when applied have been shown to be predictive of outcome. Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
58 The Algorithm Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
59 Risk Factors for Postoperative Cardiopulmonary Complications Non Pulmonary Factors Site of Surgery Duration of Surgery Laparoscopic approach Nutrition Age Obesity Pulmonary Factors COPD Smoking Obesity Productive Cough Wheezing FEV 1 /FVC ratio PaCO 2 ASA Classification Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
60 Pulmonary-Specific Evaluation Pulmonary Functions Tests Used to evaluate risk for postoperative complications since 1950s 1955 first published case of preoperative PFTs Patients undergoing lung resection for pulmonary TB MVV <50% & FVC <70% 40% Mortality following Thoracotomy Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
61 Pulmonary-Specific Evaluation Pulmonary Function Tests Include: Spirometry Lung Volumes Diffusion Capacity Oximetry Arterial Blood Gas Analysis Radionuclide Lung Scanning Cardiopulmonary Exercise Testing Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
62 Stages of Pulmonary-Specific Evaluation Stage I Assessment (Preop lung function) Spirometry Arterial Blood Gas Analysis DLCO Stage II Assessment (Postop lung function) Quantitative Ventilation-Perfusion Scan Quantitative CT Scan Stage III Assessment Exercise Testing: Oxygen Uptake (VO 2 Max) Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
63 Stage I Spirometry: Simple, inexpensive, standardized & readily available FVC volume FEV1 airflow Factor regarded as being the best for predicting complications of lung resection in the initial assessment FEF 25 75% airflow Maximal voluntary ventilation (MVV) Muscle Strength Maximal inhalation & exhalation over 12 sec: Air Flow & MS Dependent on patient effort Predicted values of pulmonary function depend on age, height, gender and race Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
64 Stage I Forced Expiratory Volume One Second: FEV 1 Correlates well with the degree of respiratory impairment in patients with COPD Indirect measure of pulmonary reserve In studies evaluating preoperative spirometric values a reduced FEV 1 (<60% of predicted) Strongest predictor of postoperative complications ACCP & BTS Guidelines: FEV 1 > 2 L tolerate pneumonectomy FEV 1 > L tolerate lobectomy Mazzone PJ et al. Lung Cancer: Preoperative pulmonary evaluation of the lung resection candidate. Am J Med 2005; 118:
65 Stage I Retrospective Studies in 1970s British Thoracic Society (BTS) Guidelines compiled on data from >2000 patients in 3 large series FEV 1 studied at the main factor Mortality Rate < 5% FEV 1 > 1.5 L for Lobectomy FEV 1 > 2 L or FEV 1 > 80% predicted for Pneumonectomy Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S
66 Stage I Diffusing capacity of the lung for carbon monoxide (DLCO) Reflects alveolar membrane integrity & pulmonary capillary blood flow in the patient s lungs. In the past (Ferguson et al) 237 patients Was the most important predictor of mortality & was the sole predictor of postoperative pulmonary complications. In recent studies Equally significant predictor of postoperative complications as FEV 1 Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123: Ferguson MK et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg 1988; 96:894

67 Stage I Factors That Enhance CO Diffusion: Increase in Lung Capillary Blood Volume Recruitment & distention of Pulmonary Capillaries Supine Position Factors That Decrease CO Diffusion: Age Standing Position Decrease in Lung Capillary Blood Volume Alveolar disease Loss of Lung Disease Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S
68 Stage I DLCO as a useful marker of operative risk Ferguson et al in 237 patients Relation between preoperative DLCO and M&M Preoperative DLCO as percentage predicted had higher correlation with postoperative mortality than FEV 1 DLCO < 60% predicted associated with mortality. DLCO & FEV 1 should be viewed as complementary physiologic tests Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S

69 Stage I Arterial Blood Gas Analysis (ABG) Not extensively studied as predictor of postoperative complication (PCO 2 >50 mmhg & PO 2 <60 mmhg) Hypercapnia (PCO 2 >50 mm Hg) in arterial blood has been a traditional contraindication to lung resection as it indicates chronic respiratory failure. In recent studies Patients with a PCO 2 of 45 mm Hg did well postoperatively Was not predictive of postoperative complications Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
70 Stage I Arterial Blood Gas Analysis (ABG) Evidence: Kearney et al (1994) No difference in postoperative complications Preoperative PCO 2 < 45 mmhg vs. PCO 2 > 45 mmhg 17% vs. 13% Hypercapnia is now NOT a contraindication to surgery Low PPO FEV 1 Poor exercise tolerance Hypoxemia (SaO 2 < 90%) was associated with risk of postoperative complications
71 Original Studies Study complications in 500 patients undergoing lung resection and correlated them with preoperative spirometric indexes & type of surgery performed. Recommendation for Pneumonectomy MVV 55%; FEV 1 2 L; FEF 25 75% 1.6 L/min. Recommendation for Lobectomy MVV 40%; FEV 1 1 L; FEF 25 75% 0.6 L/s. Recommendation for Segmentectomy or Wedge Resection MVV 40%; FEV L; FEF 25 75% 0.6 L/s Miller JI, Grossman GD, Hatcher CR. Pulmonary function test criteria for operability and pulmonary resection. Surg Gynecol Obstet 1981; 153:
72 Recent Studies Summary: following criteria are predictive of increased postoperative complications and mortality: Pneumonectomy: FEV 1 <2L or 60% of predicted & MVV 55% of predicted DLCO <50% of predicted & FEF 25 75% 1.6L/s. Lobectomy: FEV 1 <1 L & MVV <40% of predicted FEF 25 75% 0.6 L/s, DLCO <50% of predicted. Wedge resection/segmentectomy: FEV 1 <0.6 L & DLCO <50% of predicted. Stephan F, Boucheseiche S, Hollande J, et al. Pulmonary complication following lung resection: a comprehensive analysis of incidence and possible risk factors. Chest 2000; 118:
73 Stage II Quantitative Ventilation-Perfusion Scan: Measures predicted Postoperative lung function Quantitative measurement of the contribution of each lung to pulmonary ventilation & perfusion Readily available with negligible risk to the patient Highly accurate in the prediction of postoperative pulmonary function following resection Spirometry & Lung Scan Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
 Right Lung (3/2/5): 55 % & Left Lung(3/2/4): 45% Calculation: Predicted Postoperative FEV 1 of the remaining lung Debapriya D et al.")
74 Stage II Inhaled 133 Xe or IV 99 Tc-Labeled Macroaggregates of Albumin % of radioactivity contributed by each lung correlates with the contribution of the function of that lung Normally: 19 Segments (10 R & 9 L) Right Lung (3/2/5): 55 % & Left Lung(3/2/4): 45% Calculation: Predicted Postoperative FEV 1 of the remaining lung Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:

75 Stage II Using 133 Xe Inhalation: Predicted Postoperative (PPO) FEV 1 of < 1 L is indicative of physiologic inoperability. Kristersson S et al. Prediction of pulmonary function loss due to pneumonectomy using 133 Xe radioisometry. Chest 1972; 62: Using 99 Tc Macroaggregate of Albumin Perfusion: Predicted Postoperative (PPO) FEV 1 of < 0.8 L is indicative of surgical inoperability. Olsen GN, Block AJ, Tobias JA. Prediction of postpneumonectomy pulmonary function using quantitative macroaggregate lung scanning. Chest 1974; 66:13 16
76 Stage II Predictors of Morbidity & Mortality after lung resection Evidence: PPO FEV 1 < 40% of predicted 50% Mortality PPO FEV 1 > 40% of predicted 50% Mortality PPO DLCO < 40% of predicted Mortality Best predictor of postoperative respiratory failure Recommendation: If PPO FEV 1 & DLCO > 40% (or PPO FEV 1 > 1 L) may undergo lung resection including pneumonectomy. Otherwise Exercise Testing Markos J et al. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis 1989; 139:
77 Stage II Other Tests: Bronchospirometry, Lateral position testing & Total Unilateral pulmonary artery occlusion Invasive tests & Require specialized equipment with a high level of technical expertise These test are no longer performed in the preoperative evaluation of patients awaiting lung resection Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
 Incremental exercise challenge Work rate is sequentially increased to a desired end point Submaximal vs.")
78 Stage III Cardio-Pulmonary Exercise Testing (CPET) Stresses the entire cardiopulmonary & oxygen delivery system Provides a good estimate of cardiopulmonary reserve Pulmonary/cardiac function & peripheral oxygen utilization Used before the advent of PFTs & sophisticated exercise testing Two major types of tests Fixed exercise challenge Sustained level of work (i.e. walking a fixed distance or a flight of stairs) Incremental exercise challenge Work rate is sequentially increased to a desired end point Submaximal vs. Maximal oxygen consumption (VO 2 Max) Debapriya D et al. Preoperative Evaluation of Patients Undergoing Lung Resection Surgery. CHEST 2003; 123:
79 Stage III Maximal Oxygen Consumption: With increasing muscular work VO 2 rises to a point where there is a plateau of the VO 2 work rate slope. VO 2 max is a measure of aerobic capacity of the peripheral tissue i.e. Oxygen Consumption Mazzone PJ et al. Lung Cancer: Preoperative pulmonary evaluation of the lung resection candidate. Am J Med 2005; 118:
80 Stage III Fixed Challenge Exercise Testing Van Nostrand 1968 Test of endurance in the preoperative evaluation 50% postoperative mortality rate in patients who failed to climb one flight of stairs with minimal dyspnea 11% postoperative mortality rate in patients who successfully climbed two flight of stairs with minimal dyspnea Van Nostrand D, Kjelsberg MD, Humphrey EW. Pre-resectional evaluation of risk from pneumonectomy. Surg Gynecol Obstet 1968; 127:
81 Stage III Fixed Challenge Exercise Testing Olsen et al 1991 Patients who were able to climb 3 flights of stairs (i.e. 75 steps) had number of postoperative complications Holden et al 1992 Prospective study of 16 patients 6-min walk distance > 1000 feet & Stair climb of > 44 steps» Successful surgical outcome Girsch et al % complication rate in patients unable to walk up one flight of stairs. Olsen GN, Bolton JWR, Weiman DS, et al. Stair climbing as an exercise test to predict the post-operative complications of lung resection. Chest 1991; 99: Holden DA, Rice TW, Stelmach K. Exercise testing, 6-minute walk and stair climbing in the evaluation of patients at high risk for pulmonary resection. Chest 1992; 102: Girish M, Trayner E, Dammann O, et al. Symptom-limited stair climbing as a predictor of postoperative cardiopulmonary complications after high-risk surgery. Chest 2001; 120:
82 Stage III Incremental Exercise Testing Exercise to maximal exertion Measurement VO 2 max in patients for lung resection VO 2 Max > 1 L/min No mortality VO 2 Max < 1 L/min 100% mortality Incidence of Postoperative complications VO 2 Max < 15 ml/kg/min 100% complication rate VO 2 Max ml/kg/min 66% complication rate VO 2 Max > 20 ml/kg/min 10% complication rate Eugene J, Brown SE, Light RW, et al. Maximum oxygen consumption: a physiologic guide to pulmonary resection. Surg Forum 1982; 33: Smith TP, Kinasewitz GT, Tucker WY, et al. Exercise capacity as a predictor of post-thoracotomy morbidity. Am Rev Respir Dis 1984; 129:
83 Changes in Lung Volume Decline in Lung Function Varies with the extent of resection Pneumonectomy: FEV 1 reduced by 34-36% FVC reduced by 36-40% VO 2 max reduced by 20-28% Lobectomy: FEV 1 reduced by 9-17% FVC reduced by 7-11% VO 2 max reduced by 0-13% Mazzone PJ et al. Lung Cancer: Preoperative pulmonary evaluation of the lung resection candidate. Am J Med 2005; 118:

84 Lung Volume Reduction Surgery Selected patients with severe emphysema Surgery may lead to improvement in lung function Lung Nodules: In individuals who do not meet standard criteria Mazzone PJ et al. Lung Cancer: Preoperative pulmonary evaluation of the lung resection candidate. Am J Med 2005; 118:

85 Summary Reasons for Resection of Lung Cancer Poor prognosis without resection Low Operative Mortality Rate Improve Surgical Technique Improved Anesthesia & Postoperative Care Modest decline in lung function Mazzone PJ et al. Lung Cancer: Preoperative pulmonary evaluation of the lung resection candidate. Am J Med 2005; 118:
86 Summary Guidelines for Preoperative Evaluation: British Thoracic Society & Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party in British Thoracic Society and Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001; 56: American College of Chest Physicians in Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S
87 Guidelines British Thoracic Society and Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001; 56: Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S

88 Guidelines British Thoracic Society and Society of Cardiothoracic Surgeons of Great Britain and Ireland Working Party. Guidelines on the selection of patients with lung cancer for surgery. Thorax 2001; 56: Beckles MA et al. Lung Cancer Guidelines: The physiologic evaluation of patients with lung cancer being considered for resectional surgery. CHEST 2003; 123:105S-114S
89 The Algorithm Jeng-Shing Wang. Pulmonary function tests in preoperative pulmonary evaluation. Resp Med 2004; 98:
90 The End
Preoperative Workup for Pulmonary Resection. Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016
 Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital
 Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
Preoperative Evaluation of Patients Undergoing Lung Resection Surgery* Debapriya Datta, MD; and Bimalin Lahiri, MD, FCCP
 reviews Preoperative Evaluation of Patients Undergoing Lung Resection Surgery* Debapriya Datta, MD; and Bimalin Lahiri, MD, FCCP Lung cancer continues to be the leading case of cancer deaths in the United
reviews Preoperative Evaluation of Patients Undergoing Lung Resection Surgery* Debapriya Datta, MD; and Bimalin Lahiri, MD, FCCP Lung cancer continues to be the leading case of cancer deaths in the United
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Preoperative assessment for lung resection. RA Dyer
 Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Surgical resection is the treatment of choice for nonsmall
 Preoperative Risk Assessment for Marginal Patients Requiring Pulmonary Resection J. Ryan Burke, MD, Ignacio G. Duarte, MD, Vinod H. Thourani, MD, and Joseph I. Miller, Jr, MD Department of Surgery, Section
Preoperative Risk Assessment for Marginal Patients Requiring Pulmonary Resection J. Ryan Burke, MD, Ignacio G. Duarte, MD, Vinod H. Thourani, MD, and Joseph I. Miller, Jr, MD Department of Surgery, Section
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Chapter 3. Pulmonary Function Study Assessments. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Does preoperative predictive lung functions correlates with post surgical lung functions in lobectomy?
 Preoperative and post surgical lung functions in lobectomy Original Research Article ISSN: 2394-0026 (P) Does preoperative predictive lung functions correlates with post surgical lung functions in lobectomy?
Preoperative and post surgical lung functions in lobectomy Original Research Article ISSN: 2394-0026 (P) Does preoperative predictive lung functions correlates with post surgical lung functions in lobectomy?
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard
 Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
SURGERY FOR GIANT BULLOUS EMPHYSEMA
 SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
DLCO and postpneumonectomy complications RELATIONSHIP OF CARBON MONOXIDE PULMONARY DIFFUSING CAPACITY TO POSTOPERATIVE CARDIOPULMONARY COMPLICATIONS I
 RELATIONSHIP OF CARBON MONOXIDE PULMONARY DIFFUSING CAPACITY TO POSTOPERATIVE CARDIOPULMONARY COMPLICATIONS IN PATIENTS UNDERGOING PNEUMONECTOMY Jeng-Shing Wang Respiratory Medicine Section, Vancouver
RELATIONSHIP OF CARBON MONOXIDE PULMONARY DIFFUSING CAPACITY TO POSTOPERATIVE CARDIOPULMONARY COMPLICATIONS IN PATIENTS UNDERGOING PNEUMONECTOMY Jeng-Shing Wang Respiratory Medicine Section, Vancouver
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Objective: Prepare NBRC candidate for CRT and WRT Content Outline
 STRESS TEST AND HEMODYNAMICS Lois Rowland, MS, RRT-NPS, RPFT, FAARC Objective: Prepare NBRC candidate for CRT and WRT Content Outline Perform, evaluate patient response to, interpret results from: Stress
STRESS TEST AND HEMODYNAMICS Lois Rowland, MS, RRT-NPS, RPFT, FAARC Objective: Prepare NBRC candidate for CRT and WRT Content Outline Perform, evaluate patient response to, interpret results from: Stress
Reducing lung volume in emphysema Surgical Aspects
 Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
ASSESSMENT FOR LUNG. Dr. Devendra S. Dadhwal SR Pulmonary & Critical Care Medicine PGIMER
 PREOPERATIVE PULMONARY ASSESSMENT FOR LUNG RESECTION SURGERY Dr. Devendra S. Dadhwal SR Pulmonary & Critical Care Medicine PGIMER Introduction Lung Resection CA lung One of the main indication Prognosis
PREOPERATIVE PULMONARY ASSESSMENT FOR LUNG RESECTION SURGERY Dr. Devendra S. Dadhwal SR Pulmonary & Critical Care Medicine PGIMER Introduction Lung Resection CA lung One of the main indication Prognosis
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Lung Volume Reduction Surgery. February 2013
 Lung Volume Reduction Surgery February 2013 Presentation Outline Lung Volume Reduction Surgery (LVRS) Rationale & Historical Perspective NETT Results Current LVRS Process (from referral to surgery) Diagnostic
Lung Volume Reduction Surgery February 2013 Presentation Outline Lung Volume Reduction Surgery (LVRS) Rationale & Historical Perspective NETT Results Current LVRS Process (from referral to surgery) Diagnostic
Cardiopulmonary Exercise Testing Cases
 Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Basics of Cardiopulmonary Exercise Test Interpretation. Robert Kempainen, MD Hennepin County Medical Center
 Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Exercise Stress Testing: Cardiovascular or Respiratory Limitation?
 Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Preoperative Assessment of the High-Risk Patient for Lung Resection
 Preoperative Assessment of the High-Risk Patient for Lung Resection Preston Pate, MD, Michael F. Tenholder, MD, John P. Griffin, MD, Charles E. Eastridge, MD, and Darryl S. Weiman, MD Division of Pulmonary
Preoperative Assessment of the High-Risk Patient for Lung Resection Preston Pate, MD, Michael F. Tenholder, MD, John P. Griffin, MD, Charles E. Eastridge, MD, and Darryl S. Weiman, MD Division of Pulmonary
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Usefulness of Lung Perfusion Scintigraphy Before Lung Cancer Resection in Patients with Ventilatory Obstruction
 Usefulness of Lung Perfusion Scintigraphy Before Lung Cancer Resection in Patients with Ventilatory Obstruction Tommaso C. Mineo, MD, Orazio Schillaci, MD, Eugenio Pompeo, MD, Davide Mineo, MD, and Giovanni
Usefulness of Lung Perfusion Scintigraphy Before Lung Cancer Resection in Patients with Ventilatory Obstruction Tommaso C. Mineo, MD, Orazio Schillaci, MD, Eugenio Pompeo, MD, Davide Mineo, MD, and Giovanni
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
The cardiopulmonary exercise test (CPET) has been
 has been") Minute Ventilation-to-Carbon Dioxide Output (V E/V CO2 ) Slope Is the Strongest Predictor of Respiratory Complications and Death After Pulmonary Resection Alessandro Brunelli, MD, Romualdo Belardinelli,
Minute Ventilation-to-Carbon Dioxide Output (V E/V CO2 ) Slope Is the Strongest Predictor of Respiratory Complications and Death After Pulmonary Resection Alessandro Brunelli, MD, Romualdo Belardinelli,
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
LOBECTOMY COMBINED WITH VOLUME REDUCTION FOR PATIENTS WITH LUNG CANCER AND ADVANCED EMPHYSEMA
 LOBECTOMY COMBINED WITH VOLUME REDUCTION FOR PATIENTS WITH LUNG CANCER AND ADVANCED EMPHYSEMA Steven R. DeMeester, MD* G. Alexander Patterson, MD R. Sudhir Sundaresan, MD Joel D. Cooper, MD Objective:
LOBECTOMY COMBINED WITH VOLUME REDUCTION FOR PATIENTS WITH LUNG CANCER AND ADVANCED EMPHYSEMA Steven R. DeMeester, MD* G. Alexander Patterson, MD R. Sudhir Sundaresan, MD Joel D. Cooper, MD Objective:
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Different Diffusing Capacity of the Lung for Carbon Monoxide as Predictors of Respiratory Morbidity
 Different Diffusing Capacity of the Lung for Carbon Monoxide as Predictors of Respiratory Morbidity Robert J. Cerfolio, MD, and Ayesha S. Bryant, MSPH, MD Department of Surgery, Division of Cardiothoracic
Different Diffusing Capacity of the Lung for Carbon Monoxide as Predictors of Respiratory Morbidity Robert J. Cerfolio, MD, and Ayesha S. Bryant, MSPH, MD Department of Surgery, Division of Cardiothoracic
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Pulmonary function and exercise capacity after lung resection
 Eur Respir J, 1996, 9, 415 421 DOI: 1.1183/931936.96.93415 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 Pulmonary function and exercise
Eur Respir J, 1996, 9, 415 421 DOI: 1.1183/931936.96.93415 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 Pulmonary function and exercise
Ontario s Referral and Listing Criteria for Adult Lung Transplantation
 Ontario s Referral and Listing Criteria for Adult Lung Transplantation Version 3.0 Trillium Gift of Life Network Adult Lung Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The patient
Ontario s Referral and Listing Criteria for Adult Lung Transplantation Version 3.0 Trillium Gift of Life Network Adult Lung Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The patient
Predicting Postoperative Pulmonary Function in Patients Undergoing Lung Resection*
 Predicting Postoperative Pulmonary Function in Patients Undergoing Lung Resection* Bernhardt G. Zeiher, MD; Thomas ]. Gross, MD; Jeffery A. Kern, MD, FCCP; Louis A. Lanza, MD, FCCP; and Michael W. Peterson,
Predicting Postoperative Pulmonary Function in Patients Undergoing Lung Resection* Bernhardt G. Zeiher, MD; Thomas ]. Gross, MD; Jeffery A. Kern, MD, FCCP; Louis A. Lanza, MD, FCCP; and Michael W. Peterson,
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Testing Clinical Implications
 Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Respiratory Pathophysiology Cases Linda Costanzo Ph.D.
 Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Triennial Pulmonary Workshop 2015
 Triennial Pulmonary Workshop 2015 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2015 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Indications for sublobar resection for localized NSCLC
 Indications for sublobar resection for localized NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke University School of Medicine
Indications for sublobar resection for localized NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke University School of Medicine
Physiologic Evaluation of the Patient. With Lung Cancer Being Considered for Resectional Surgery
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES With Lung Cancer Being Considered for Resectional Surgery Diagnosis and Management of Lung Cancer, 3rd ed: American College
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES With Lung Cancer Being Considered for Resectional Surgery Diagnosis and Management of Lung Cancer, 3rd ed: American College
Evaluation of operability before lung resection Chris Thomas Bolliger, MD, PhD
 Evaluation of operability before lung resection Chris Thomas Bolliger, MD, PhD Lung resection remains the treatment of choice in the curative approach to nonsmall cell lung cancer. Because most lung cancer
Evaluation of operability before lung resection Chris Thomas Bolliger, MD, PhD Lung resection remains the treatment of choice in the curative approach to nonsmall cell lung cancer. Because most lung cancer
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
ESTABLISHING NORMATIVE VALUES FOR THE STAIR CLIMB TEST
 ESTABLISHING NORMATIVE VALUES FOR THE STAIR CLIMB TEST Introduction Gait speed is a useful tool in: Predicting morbidity and mortality Assessing fall risks and functional mobility Typically, gait speed
ESTABLISHING NORMATIVE VALUES FOR THE STAIR CLIMB TEST Introduction Gait speed is a useful tool in: Predicting morbidity and mortality Assessing fall risks and functional mobility Typically, gait speed
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Akihiro Hayashi, MD, Shinzo Takamori, MD, Masahiro Mitsuoka, MD, Keisuke Miwa, MD, Mari Fukunaga, MD, Keiko Matono, MD, and Kazuo Shirouzu, MD
 Case Report The UPAO Test in Preoperative Evaluation for Major Pulmonary Resection: An Operative Case with Markedly Improved Ventilatory Function after Radical Pulmonary Resection for Lung Cancer Associated
Case Report The UPAO Test in Preoperative Evaluation for Major Pulmonary Resection: An Operative Case with Markedly Improved Ventilatory Function after Radical Pulmonary Resection for Lung Cancer Associated
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Outcome of the Surgical Treatment of Bullous Lung Disease: A Prospective Study
 Original Article 2012 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Outcome of the Surgical Treatment of Bullous Lung Disease: A Prospective Study
Original Article 2012 NRITLD, National Research Institute of Tuberculosis and Lung Disease, Iran ISSN: 1735-0344 TANAFFOS Outcome of the Surgical Treatment of Bullous Lung Disease: A Prospective Study
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Preoperative pulmonary evaluation in patients scheduled for lung operations
 Journal of BUON 12: 163-171, 2007 2007 Zerbinis Medical Publications. Printed in Greece REVIEW ARTICLE Preoperative pulmonary evaluation in patients scheduled for lung operations P. Myrianthefs 1, C. Batistaki
Journal of BUON 12: 163-171, 2007 2007 Zerbinis Medical Publications. Printed in Greece REVIEW ARTICLE Preoperative pulmonary evaluation in patients scheduled for lung operations P. Myrianthefs 1, C. Batistaki
ORIGINAL ARTICLE. Thoracoscopic minimally invasive surgery for non-small cell lung cancer in patients with chronic obstructive pulmonary disease
 ORIGINAL ARTICLE Thoracoscopic minimally invasive surgery for non-small cell lung cancer in patients with chronic obstructive pulmonary disease Fei Cui 1,2*, Jun Liu 1,2*, Wenlong Shao 1,2, Jianxing He
ORIGINAL ARTICLE Thoracoscopic minimally invasive surgery for non-small cell lung cancer in patients with chronic obstructive pulmonary disease Fei Cui 1,2*, Jun Liu 1,2*, Wenlong Shao 1,2, Jianxing He
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Comparative efficacy of different modules on pulmonary functions after lung resection
 International Surgery Journal Gandhi S et al. Int Surg J. 2017 Aug;4(8):2770-2776 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173416
International Surgery Journal Gandhi S et al. Int Surg J. 2017 Aug;4(8):2770-2776 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173416
PULMONARY FUNCTION TEST(PFT)
") PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Lung-Volume Reduction Surgery ARCHIVED
 Lung-Volume Reduction Surgery ARCHIVED Policy Number: Original Effective Date: MM.06.008 04/15/2005 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST 03/22/2013 Section: Surgery Place(s) of
Lung-Volume Reduction Surgery ARCHIVED Policy Number: Original Effective Date: MM.06.008 04/15/2005 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST 03/22/2013 Section: Surgery Place(s) of
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Parenchymal air leak is a frequent complication after. Pleural Tent After Upper Lobectomy: A Randomized Study of Efficacy and Duration of Effect
 Pleural After Upper Lobectomy: A Randomized Study of Efficacy and Duration of Effect Alessandro Brunelli, MD, Majed Al Refai, MD, Marco Monteverde, MD, Alessandro Borri, MD, Michele Salati, MD, Armando
Pleural After Upper Lobectomy: A Randomized Study of Efficacy and Duration of Effect Alessandro Brunelli, MD, Majed Al Refai, MD, Marco Monteverde, MD, Alessandro Borri, MD, Michele Salati, MD, Armando
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Approach to CPET. CPET Cases. Case 1 4/4/2018. Impaired? Cardiac factors? Ventilatory factors?
 Approach to CPET CPET Cases Neil MacIntyre MD Duke University Medical Center Durham NC Impaired? Work,, /kg Cardiac factors?, /, BP, Rhythm Ventilatory factors? Ve/MVV (incl EIB, trapping), PaCO2 Gas exchange
Approach to CPET CPET Cases Neil MacIntyre MD Duke University Medical Center Durham NC Impaired? Work,, /kg Cardiac factors?, /, BP, Rhythm Ventilatory factors? Ve/MVV (incl EIB, trapping), PaCO2 Gas exchange
Cardiopulmonary Exercise Testing: its principles, interpretation & application. DM Seminar Harshith
 Cardiopulmonary Exercise Testing: its principles, interpretation & application DM Seminar Harshith Outline Physiology of exercise Introduction Equipment and working Principles Interpretation and variables
Cardiopulmonary Exercise Testing: its principles, interpretation & application DM Seminar Harshith Outline Physiology of exercise Introduction Equipment and working Principles Interpretation and variables
Five Consecutive Cases of Non-Pharmacologic Therapy for COPD
 Five Consecutive Cases of Non-Pharmacologic Therapy for COPD Michael Jantz, MD Director of Interventional Pulmonology University of Florida Michael.Jantz@medicine.ufl.edu Emphysema: Background Loss of
Five Consecutive Cases of Non-Pharmacologic Therapy for COPD Michael Jantz, MD Director of Interventional Pulmonology University of Florida Michael.Jantz@medicine.ufl.edu Emphysema: Background Loss of
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
2. OBJECTIVE. Vesna Cukic Clinic for pulmonary diseases and TB Podhrastovi, Clinical center of Sarajevo University, Bosnia and Herzegovina
 Preoperative Prediction of ung Function in Pneumonectomy by Spirometry and ung Perfusion Scintigraphy 221 ACTA INFORM MED. 2012 Dec; 20(4): 221-225 doi: 10.5455/aim.2012.20.221-225 Received: 15 August
Preoperative Prediction of ung Function in Pneumonectomy by Spirometry and ung Perfusion Scintigraphy 221 ACTA INFORM MED. 2012 Dec; 20(4): 221-225 doi: 10.5455/aim.2012.20.221-225 Received: 15 August
Protocol. Lung Volume Reduction Surgery for Severe Emphysema
 Protocol Lung Volume Reduction Surgery for Severe Emphysema (70171) Medical Benefit Effective Date: 01/01/12 Next Review Date: 09/14 Preauthorization Yes Review Dates: 02/07, 01/08, 11/08, 09/09, 09/10,
Protocol Lung Volume Reduction Surgery for Severe Emphysema (70171) Medical Benefit Effective Date: 01/01/12 Next Review Date: 09/14 Preauthorization Yes Review Dates: 02/07, 01/08, 11/08, 09/09, 09/10,
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
Preanesthetic Assessment for Thoracic Surgery
 2 Preanesthetic Assessment for Thoracic Surgery Peter Slinger and Gail Darling Introduction... 11 Assessment of Respiratory Function... 13 Pulmonary Parenchymal Function... 15 Cardiopulmonary Interaction...
2 Preanesthetic Assessment for Thoracic Surgery Peter Slinger and Gail Darling Introduction... 11 Assessment of Respiratory Function... 13 Pulmonary Parenchymal Function... 15 Cardiopulmonary Interaction...
Perioperative Pulmonary Management. Objectives
 Citywide Resident Perioperative Medical Consult Conference Perioperative Pulmonary Management Frank Jacono, MD May 5, 2017 Objectives Definition of post-operative pulmonary complications (PPC) Risk factors
Citywide Resident Perioperative Medical Consult Conference Perioperative Pulmonary Management Frank Jacono, MD May 5, 2017 Objectives Definition of post-operative pulmonary complications (PPC) Risk factors
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
i. Zone 1 = dead space ii. Zone 2 = ventilation = perfusion (ideal situation) iii. Zone 3 = shunt
 iii. Zone 3 = shunt") Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic