What I Learned from 3 Cases and 3 Antibodies
|
|
|
- Silas Oliver
- 6 years ago
- Views:
Transcription




1 What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner have, or have had, within the past 12 months, which relates to the content of this educational activity and creates a conflict of interest. Dr. Melinda Sanders declares he/she has no conflict(s) of interest to disclose. Case #1 History Left Breast Biopsy 61 yo female with stage 4 appendiceal adenocarcinoma 2.1 cm left breast mass and an enlarged axillary lymph node found during staging work up Core needle biopsy performed Left Breast Biopsy Left breast biopsy 1












2 Appendiceal adenocarcinoma Breast biopsy GATA3 Biopsy #1 Immunohistochemistry CDX 2 SOX10 Repeat Needle Core Biopsy of Breast Negative expression GATA3, ER, PR, CK7, CK20, CDX 2 Diagnosis: Poorly differentiated malignant neoplasm and skeletal muscle, cytologically different from abdominal mutinous adenocarcinoma (CDX 2 + ) Note: Does not exclude a breast primary 2




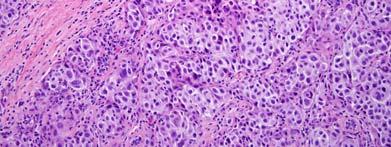
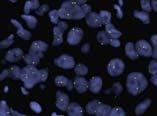
3 CK AE1/3 S100 Biopsy #2 Immunohistochemistry GATA3 CK 7 CK 8/18 SOX10 MITF MelanA HMB 45 Diagnosis Malignant Melanoma Wire localized partial mastectomy 17 mm Malignant Melanoma SNL 1/1 lymph node 2.5 mm metastasis LN dissection 0/19 lymph nodes Case #1 Melanoma AE 1/3 + patchy weak mod CK7 Breast ER GATA3 CK 8/18 S100 + SOX10 + Melanoma MITF + MelanA + HMB45 + GI CDX2 HER2 ND Melanoma is most common non hematopoietic malig to met to breast, may rare occur as primary Think about melanoma when ER /PR tumor, nested morphology, especially if TILs Aberrant CK expression = major pitfall, especially in melanoma metastases. If GATA3 negative, perform panel of MM markers Keratin Expression in Melanoma Keratin expression typically helps support a diagnosis of carcinoma and rules out sarcoma, lymphoma, and melanoma Expression not infrequent most common AE 1/3, CK8, CK18, MNF 116 Aberrant keratin expression more common in metastatic than primary 4 10% primary melanomas 40 70% metastatic melanoma Implies a correlation between keratin expression and a more aggressive tumor phenotype. Safadi et al.,oral and Maxillofacial Pathol 2016;121: Plaza et al., App Immunohistochem Mol Morphol 2007;15: Percentage of Primary vs. Metastatic Melanoma Cases with Keratin Expression MNF 116 CK18 CK7 CK18 MNF 116 CK8 CK7 S 100 is Highly Sensitive but not Specific for MM Normally found in cells derived for neural crest including melanocytes and myoepithelial cells Most sensitive melanoma marker (>95%), not very specific Approximately 50% of BC may express S100 DDx for cytokeratin + /S100 + tumor inc. melanoma and BC Additional markers mandatory to distinguish Primary Melanoma Metastatic Melanoma Safadi et al., Oral and Maxillofacial Pathol 2016;121: Dwarakanath Hum Pathol 1987;18: Stroup Hum Pathol 1988;19:





4 Case #2 History 31 yo female h/o left shoulder melanoma ; Negative left axillary sentinel nodes Presented 7 mo later with left axillary mass Core needle biopsy performed Left Axillary Lymph Node Biopsy Left Axillary Mass Immunohistochemistry CK 7 CAM5.2 GATA3 CK AE 1/3 Diagnosis Melan A SOX10 S100 HMB45 Metastastic carcinoma, most consistent with breast cancer AR, likely ruling out adnexal carcinoma 4





5 Melanoma Left Shoulder Immunohistochemistry Left Shoulder Mass CK7 AE 1/3 GATA3 AR HMB 45 S100 MelanA SOX10 Case #2, Diagnosis #2 Left Shoulder Malignant melanoma with intratumoral focus of carcinoma consistent with metastasis from breast cancer BC vs Melanoma Immunohistochemistry Case #1 Case #2 Melanoma BC Melanoma AE 1/3 + patchy weak mod + diffuse weak CK7 + diffuse strong Breast ER ND GATA3 + diffuse strong CK 8/18 ND ND S SOX Melanoma MITF + ND ND MelanA + + HMB GI CDX2 ND ND HER2 ND ND 5

6 Primary Clinical Use Breast carcinoma (92% primary, 96% met) Urothelial carcinoma (91% primary) GATA3 Expression Other Carcinomas SCC variety of sites 80% Adnexal carcinomas 70% Salivary gland carcinomas >99% Choriocarcinoma and trophoblastic tumors >99% Mesothelioma 58% Chromophobe carcinoma 51% Pancreatic ductal carcinoma 10 37% Other adenocarcinomas < 10% lung stomach endometrium ovary thyroid Metastatic melanoma 0/74 GATA3 in the Breast Transcription factor with role in differentiation of mammary luminal epithelial cells In BC cell lines and mouse models 1) reduces tumor initiating capacity of luminal progenitor cells & 2) impedes EMT by interaction with BRCA1 In ER+ cell lines, required for estradiol stimulation of cell cycle prog In ER-/BRCA1 mutant cell lines, BRCA1 unable to associate with GATA3 leading to a drug-resistant and mesenchymal phenotype GATA3 somatic mutations identified most commonly in ER+ but also ER- Asch Kendrick Hum Path 2016;48:37 47 Miettinen Am J Surg Pathol 2014;38:13 22 Yang Mod Pathol 2010;23: Asch Kendrick Hum Path 2016;48:37 47 Kouros Mehr Curr Open Cell Bio 2008;20:164 Tkocz Oncogene 2012;31: GATA3 Expression in Breast Cancer Primary BC ER % NST (ductal) % Lobular % ER+/HER2+ 100% ER-/HER % TNBC 2.6%-83%(70-80%) Apocrine 83-91% Metaplastic 17-56% MBC All 73-95% ER+ >99% HER2+ >99% TNBC 56% (44-70%) Useful internal positive controls B9 luminal cells and lymphocytes Recommendations for GATA3 use Breast Primary Highly sensitive for ER+, routinely unnecessary Greatest utility, ER HG tumor, esp if lacking an in situ component, positivity strongly supports breast primary, further strengthened by other markersdiffuse strong CK7+, SOX10+ More sensitive and specific than mammoglobin and GCDFP 15 for dx BC esp in TNBC Rules out melanoma (at present) Metastasis Strongly supportive of breast origin in patient with known history of ER+ or ER BC Suggests mammary origin in CK7+/CK20 carcinoma of unk primary, req other markers to r/o other CK7+ adeno, TTF 1 and napsin lung, PAX8 renal & gyn, CDX2 GI GATA3+/CK7 broader ddx SCC Asch Kendrick Hum Path 2016;48:37 47 Miettinen Am J Surg Pathol 2014;38:13 22 Liu Am J Clin Patol 2014;141: Cimino Mathews Hum Pathol 2013;44: Voduc Cancer Epi Bio Prev 2008;17: Ciocca Hum Pathos 2009;40: Yang Mod Pathol 2010;23: Asch Kendrick Hum Path 2016;48:37 47 Miettinen Am J Surg Pathol 2014;38:13 22 Krings Hum Pathol 2014;45: Case #3 History and Presentation 74 year old female presented to her PCP with an inverted nipple PMH Right elbow melanoma Mammogram Photo Album Right breast, 12 o'clock 1.7 cm x 6.4 cm asymmetric density 2 cm from the nipple. by Sanders, Melinda Ultrasound 1.5 cm x 1.3 cm x 1.7 cm hypoechoic mass with posterior shadowing A right axillary ultrasound also revealed multiple morphologically abnormal lymph nodes. Ultrasound guided core needle biopsy performed. Breast Core Needle Biopsy 6












7 Hormone Receptor Immunohistochemistry HER2 FISH ER (3+, 100%) PR (2+, 85%) Not Amplified HER2/Cep17 ratio 1.0 Average HER2 copy # 1.9 Wire-Localized Partial Mastectomy 7





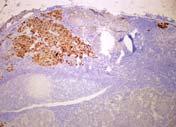
![[carcinoid-like]](/docs-images/77/76644513/images/8-5.jpg "neuroendocrine carcinoma")


8 surgery surgery surgery ER Immunohistochemistry Breast CK7 CK8/18 GATA3 MelanA S100 MITF SOX10 Synaptophysin Diagnosis Invasive mammary carcinoma, no special type with neuroendocrine differentiation WHO 2012 : well-differentiated [carcinoid-like] neuroendocrine carcinoma 24 mm Metastatic tumor involving 11 of 24 lymph nodes, largest focus measuring 35 mm with extracapsular extension. 8












9 Axillary Lymph node with Metastatic Breast Cancer Axillary lymph node CK 8/18 CK 7 ER GATA3 MelanA S100 SOX10 MITF Axillary Lymph Node Axillary Lymph node with Metastatic Melanoma CK8/18 CK7 ER GATA3 MelanA S100 SOX10 MITF Axillary Lymph Node Axillary Lymph Node with Metastatic BC and Melanoma GATA3 CK8/18 MelanA Sox10 9




 Luminal B 7 6 0 0 0 1 1 (14%) Her2 14 13 0 0 0 1 1 (7%) Basal like 32 10 0 3 4 15 22 (69%)* TNBC,NOS 13 3 0 2 2")
10 Diagnosis Invasive mammary carcinoma, no special type with neuroendocrine differentiation Metastatic mammary carcinoma involving 11 of 24 lymph nodes, largest focus measuring 35 mm with extracapsular extension. Metastatic melanoma involving 2 of 24 lymph nodes, 1.2 mm 0.5 mm. BC vs Melanoma Immunohistochemistry Case #1 Case #2 Case #3 Melanoma BC Melanoma BC Melanoma AE 1/3 + patchy weak mod + diffuse weak + CK7 + diffuse strong Breast ER ND + GATA3 + diffuse strong + CK 8/18 ND ND + S SOX Focal LN+ + Melanoma MITF + ND ND + MelanA + + Focal LN+ + HMB ND + GI CDX2 ND ND ND ND HER2 ND ND ND SOX10 Expression in Breast Cancer Transcription factor mediates differentiation of neural crest derived cells Most common clinical use IHC, support diagnosis of malignant melanoma Expressed by mammary myopepithelial cells and approximately 40% of breast cancers Most commonly expressed in TNBC Cimino-Mathews Human Pathol 2013;44: Mollaaghababa Oncogene 2003;22: Dravis et al. Cell Reports 2015;12: Nonaka Am J Surg Pathol 2008;32: Immunohistochemical labeling of Sox10 in breast carcinoma Tumor type n Intensity of Sox10 staining Total positive Luminal A (0%) Luminal B (14%) Her (7%) Basal like (69%)* TNBC,NOS (77%)* Metaplastic (46%)* Table 2 Cimino Mathews Hum Pathol 2013; 44: *P < % (35/40) Nuclear Sox10 labeling defined as 0, 1+ (1% 25%), 2+ (25% 50%), 3+ (50% 75%), 4+ (>75%) Subtypes determined by surrogate panel of IHC: LumA = >75% ER+/HER2 LumB = ER+/HER2+, Basal TNBC = ER /PR /HER2 / CK5/6 +/or EGFR+ TNBC, NOS = ER /PR /HER2 /CK5 6 /EGFR 10
11 Summary- What I learned from 3 cases and more than 3 antibodies: Melanoma - 2nd most common non-hematopoietic neoplasm to metastasize to the breast, and although rare, primary melanomas of the breast occur MM must be in ddx for woman presenting with an ER-/PR- breast or axillary mass, esp if unusual morph, nested and TILs Evidence of CK expression in a breast/axillary mass does not R/O MM Aberrant CK expression (esp. CK7/8/18, AE1/3, CAM5.2, MNF-116) in melanoma, especially metastatic, should prompt use of a battery of melanoma markers- MITF, HMB-45, MART-1 before excluding MM Summary- What I learned from 3 cases and more than 3 antibodies: Approx 10% BC CK7, further highlighting the unreliability of CKs in this distinction GATA3 most sensitive marker for BC in both in breast and metastases, ER+ and ER, most helpful in identification of CK7 TNBC GATA3 + excludes melanoma Important pitfall, SOX 10 expressed in 92% of melanomas also expressed in 40% breast cancers, most common in TNBC (>60%), inc. metaplastic carcinomas S100 most sensitive marker for MM (>95%), however, up to 50% of BC may express S100, thus ddx for S100+/SOX10+ neoplasm must inc. BC requiring additional w/u When evaluating metastatic biopsy, do not underestimate value of obtaining block of primary for comparison IHC testing Consider molecular testing in unresolvable cases THANK YOU 11
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016
 May 17, 2016") What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016 Outline IHC markers of metastatic carcinoma of breast origin Uses and limitations of e-cadherin IHC Breast neoplasms with limited metastatic
What s new in breast pathology? Penny Barnes MD, FRCP(C) May 17, 2016 Outline IHC markers of metastatic carcinoma of breast origin Uses and limitations of e-cadherin IHC Breast neoplasms with limited metastatic
Disclosure of Relevant Financial Relationships. Breast Pathology Evening Specialty Conference Case #4. Clinical Case: Pathologic Features
 Breast Pathology Evening Specialty Conference Case #4 K.P. Siziopikou, MD, PhD Professor of Pathology Director of Breast Pathology and Breast Pathology Fellowship Program Northwestern University Feinberg
Breast Pathology Evening Specialty Conference Case #4 K.P. Siziopikou, MD, PhD Professor of Pathology Director of Breast Pathology and Breast Pathology Fellowship Program Northwestern University Feinberg
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Case 18. M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is:
 Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
10/15/2012. Biologic Subtypes of TNBC. Topics. Topics. Histopathology Molecular pathology Clinical relevance
 Biologic Subtypes of TNBC Andrea L. Richardson M.D. Ph.D. Brigham and Women s Hospital Dana-Farber Cancer Institute Harvard Medical School Boston, MA Topics Histopathology Molecular pathology Clinical
Biologic Subtypes of TNBC Andrea L. Richardson M.D. Ph.D. Brigham and Women s Hospital Dana-Farber Cancer Institute Harvard Medical School Boston, MA Topics Histopathology Molecular pathology Clinical
Case 1. ACCME/Disclosure. Clinical History. Dr. Mulligan has nothing to disclose
 Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
Breast Evening Specialty Conference USCAP, 2016 Case 1 Anna Marie Mulligan University Health Network, Toronto University of Toronto ACCME/Disclosure Dr. Mulligan has nothing to disclose Clinical History
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Disclosure of Relevant Financial Relationships
 Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference - Genitourinary Pathology Case 2 Disclosure of Relevant Financial Relationships Sean R Williamson, MD Henry Ford Health System, Detroit, MI @Williamson_SR USCAP requires that
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Carcinoma of unknown primary origin (CUP) is defined
 is defined") REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Reporting of carcinoma of unknown primary tumour (CUP)
") Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
NEW IHC A n t i b o d i e s
 NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Technology from Abcam
 CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Contents 1 The Windows of Susceptibility to Breast Cancer 2 The So Called Pre-Neoplastic Lesions and Carcinoma In Situ
 Contents 1 The Windows of Susceptibility to Breast Cancer... 1 1.1 Introduction... 1 1.2 Risk Factor and Etiological Agents... 2 1.3 The Concept of the Windows of Susceptibility to Carcinogenesis... 5
Contents 1 The Windows of Susceptibility to Breast Cancer... 1 1.1 Introduction... 1 1.2 Risk Factor and Etiological Agents... 2 1.3 The Concept of the Windows of Susceptibility to Carcinogenesis... 5
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas
 Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA
 + NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
+ NEUROENDOCRINE DIFFERENTIATED BREAST CARCINOMA + INTRODUCTION + NEUROENDOCRINE FEATURES IN BREAST CARCINOMA Incidence of 2-5% Seen in various histopathological types of breast carcinoma Seen in both
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors
 Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Bartholin Gland Carcinomas
 Bartholin Gland Carcinomas Hugo Horlings MD PhD The Netherlands Cancer Institute Amsterdam, The Netherlands Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
Bartholin Gland Carcinomas Hugo Horlings MD PhD The Netherlands Cancer Institute Amsterdam, The Netherlands Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
Question 1 A. ER-, PR-, HER+ B. ER+, PR+, HER2- C. ER-, PR+, HER2- D. ER-, PR-, HER2- E. ER-, PR+, HER2+
 Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
Triple Negative Breast Cancer Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Question 1 The tumor depicted on the next slide
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Prostate Immunohistochemistry. Literature Interpretation: Caveats. Must be aware of staining pattern of antibody in the relevant tissue
 IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
IHC Interpretation: General Principles (1) Prostate Immunohistochemistry Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Must be aware of staining pattern of antibody in the relevant tissue Nuclear/cytoplasmic/membranous
ACCME/Disclosures. Case 4 USCAP Pulmonary Panel Case 4 History
 Case 4 USCAP Pulmonary Panel 2016 Andrew Churg, MD Department of Pathology Vancouver General Hospital & University of British Columbia Vancouver, BC achurg@mail.ubc.ca. ACCME/Disclosures The USCAP requires
Case 4 USCAP Pulmonary Panel 2016 Andrew Churg, MD Department of Pathology Vancouver General Hospital & University of British Columbia Vancouver, BC achurg@mail.ubc.ca. ACCME/Disclosures The USCAP requires
Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens
 Original Article Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens Tamar C. Brandler, MD, MS 1 ; Mohamed S. Aziz, MD 1 ; Lisa M. Rosen,
Original Article Usefulness of GATA3 and p40 Immunostains in the Diagnosis of Metastatic Urothelial Carcinoma in Cytology Specimens Tamar C. Brandler, MD, MS 1 ; Mohamed S. Aziz, MD 1 ; Lisa M. Rosen,
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
TEST MENU BY SPECIALTY
 1 TEST MENU BY SPECIALTY Breast Pathology Surgical excisions, needle core biopsies, and plastic surgery accepted from all sites Assessment of margins Axillary lymph node dissections Sentinel lymph nodes
1 TEST MENU BY SPECIALTY Breast Pathology Surgical excisions, needle core biopsies, and plastic surgery accepted from all sites Assessment of margins Axillary lymph node dissections Sentinel lymph nodes
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Single and Multiplex Immunohistochemistry
 Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
C.L. Davis Foundation Descriptive Veterinary Pathology Course
 C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Barriers to Understanding
 Behind the Scenes: The Critical Importance of Cancer Cell Pathology and the Pathologist Sherry T. Emery, M.D., Chief of Pathology Northeast Health System Barriers to Understanding Questions for 2010 What
Behind the Scenes: The Critical Importance of Cancer Cell Pathology and the Pathologist Sherry T. Emery, M.D., Chief of Pathology Northeast Health System Barriers to Understanding Questions for 2010 What
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY
 CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
A 60-year old Man with Left Jaw Mass. Simon Chiosea, MD University of Pittsburgh medical Center 3/15/2016
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma?
 Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma? skin Jane L. Messina, MD Interna0onal Melanoma Pathology Working Group 4 th annual mee0ng Tampa, Florida November 14, 2011
Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma? skin Jane L. Messina, MD Interna0onal Melanoma Pathology Working Group 4 th annual mee0ng Tampa, Florida November 14, 2011
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
ISSN X (Print) Original Research Article. DOI: /sjams
 Original Research Article. DOI: /sjams") DOI: 10.21276/sjams.2016.4.7.33 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2016; 4(7C):2468-2473 Scholars Academic and Scientific Publisher (An International Publisher
DOI: 10.21276/sjams.2016.4.7.33 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2016; 4(7C):2468-2473 Scholars Academic and Scientific Publisher (An International Publisher
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
USCAP 2012: Companion Meeting of the AAOOP. Update on lacrimal gland neoplasms: Molecular pathology of interest
 USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
USCAP 2012: Companion Meeting of the AAOOP Vancouver BC, Canada, March 17, 2012 Update on lacrimal gland neoplasms: Molecular pathology of interest Valerie A. White MD, MHSc, FRCPC Department of Pathology
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
BSD 2015 Case 19. Female 21. Nodule on forehead. The best diagnosis is:
 BSD 2015 Case 19 Female 21. Nodule on forehead. The best diagnosis is: A. mixed tumour of skin B. porocarcinoma C. nodular hidradenoma D. metastatic adenocarcinoma BSD 2015 Case 19 Female 21 Nodule on
BSD 2015 Case 19 Female 21. Nodule on forehead. The best diagnosis is: A. mixed tumour of skin B. porocarcinoma C. nodular hidradenoma D. metastatic adenocarcinoma BSD 2015 Case 19 Female 21 Nodule on
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Classification of the unknown primary tumour: the primary IHC panel
 CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Immunohistochemistry and Bladder Tumours
 Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Rare Breast Cancers and Male Breast Cancer
 Johns Hopkins Hospital, Baltimore MD Rare Breast Cancers and Male Breast Cancer David Euhus, MD, FACS Professor of Surgery (PAR) Division of Surgical Oncology Breast Cancer Primary Cancers (97% of breast
Johns Hopkins Hospital, Baltimore MD Rare Breast Cancers and Male Breast Cancer David Euhus, MD, FACS Professor of Surgery (PAR) Division of Surgical Oncology Breast Cancer Primary Cancers (97% of breast
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Cytokeratin 20 negative Merkel cell carcinoma consistent with negative Merkel cell polyomavirus
 CASE REPORT eissn 2384-0293 Yeungnam Univ J Med 2017;34(2):293-297 https://doi.org/10.12701/yujm.2017.34.2.293 Cytokeratin 20 negative Merkel cell carcinoma consistent with negative Merkel cell polyomavirus
CASE REPORT eissn 2384-0293 Yeungnam Univ J Med 2017;34(2):293-297 https://doi.org/10.12701/yujm.2017.34.2.293 Cytokeratin 20 negative Merkel cell carcinoma consistent with negative Merkel cell polyomavirus
Enterprise Interest None
 Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology
 XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology NUEVOS FENOTIPOS DEL CÁNCER DE MAMA: NUEVOS PROBLEMAS PARA EL PATÓLOGO? Tienen actualmente
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Molecular classification of breast cancer implications for pathologists. Sarah E Pinder
 Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Molecular classification of breast cancer implications for pathologists Sarah E Pinder Courtesy of CW Elston Histological types Breast Cancer Special Types 17 morphological special types 25-30% of all
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction