Advanced Prostate Cancer
|
|
|
- Myles Justin Barrett
- 6 years ago
- Views:
Transcription

1 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University of Windsor
2 Disclosures Honoraria from Janssen, Astellas, Sanofi
3 Objectives 1. Review natural history of advanced prostate cancer 2. Metastatic disease in castrate sensitive setting 1. Early Chemotherapy 3. Metastatic disease in castrate resistant setting 1. Androgen inhibitors 2. Chemotherapy 3. Bone directed therapy 4. Future directions
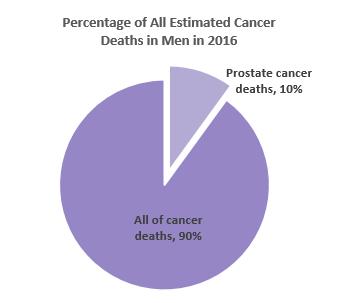
4 Background In Canada, Prostate Cancer is the most common cancer among men 3 rd most common cause of cancer death in men prostate cancer that recurs after local treatment usually responds at least temporarily to androgen deprivation therapy (ADT) Most patients experience disease progression on ADT within 18-24m
5




6 PSA

7 Androgen drives PC growth Androgen can come from testicular (90%) non-testicular (10%) Extra-testicular androgen production plays an important role in resistance of PC cells to medical or surgical castration ADT orchiectomy LHRH agonists/antagonists Androgen receptor antagonists
 Disease progression despite castrate levels of testosterone: rising PSA, progression of pre-existing disease or new metastases Extra-testicular androgen production plays significant role in")
8 Castrate Resistance NEW Definitions Hormone Resistance Castrate sensitive prostate cancer (CSPC) disease progression in the setting of normal testosterone levels Castrate resistant prostate cancer (CRPC) Disease progression despite castrate levels of testosterone: rising PSA, progression of pre-existing disease or new metastases Extra-testicular androgen production plays significant role in resistance of PC cells to medical castration Castrate=testosterone level <1.7nmol/L (8-28) or <50ng/dL Androgen receptor remains active in CRPC so ADT is continued indefinitely



9 Prostate Cancer Progression Primary localized disease PSA-only relapse Metastatic disease Castrate Sensitive Castrate Resistant
10

11 Case 1: (Metastatic Castrate Sensitive) 50 yo man previously well Had PSA in 2012 was normal In the fall 2013 was a little tired, had some hip pain and shoulder pain PSA=100 then PSA=125 Rectal exam:hard nodular prostate gland TRUS biopsy:gleason score 9 in 10/12 cores Bone scan showed extensive bone mets CT normal except bone mets
12 Case 1 (metastatic castrate sensitive) Started on ADT by urologist with improvement in bone pain PSA down to 13 in couple of months Referred to Medical Oncology What next?

13 Metastatic Prostate Cancer

14 Early Chemo+ADT: A debate in one slide a need for randomized phase 3 trial Presented By Christopher Sweeney at 2014 ASCO Annual Meeting

15 E3805 CHAARTED Treatment Presented By Christopher Sweeney at 2014 ASCO Annual Meeting

16 Primary endpoint: Overall survival Presented By Christopher Sweeney at 2014 ASCO Annual Meeting

17 OS by extent of metastatic disease at start of ADT Presented By Christopher Sweeney at 2014 ASCO Annual Meeting
18 Other studies GET-UG (France) n=385 OS HR=1.01 Chaarted (US) n=790 OS HR=0.61 Stampede (UK) n=1817 OS HR=0.76 Gravis G, et al. Lancet Oncol. 2013;14: Sweeney CJ, et al. N Engl J Med. 2015;373: James ND, et al. Lancet. 2016;387:
19 Case 1A (Metastatic castrate sensitive ) Pt had high burden of metastatic disease Good PS once ADT started and bone pain controlled Recommended 6 cycles docetaxel chemotherapy then continue with ADT until PSA rises or progression of metastases (castrate resistance)
20 Case 1B 12m later:rising PSA (metastatic castrate resistant-crpc) Still on ADT PSA was 2 now rising PSA=15 then 40 Testosterone=0.1nmol/dL Secondary hormonal treatment did not affect PSA addition of casodex or withdrawl/ketoconozole/prednisone: no survival advantage-transient PSA response in ~30% of patients
21 Case 1B 12m later: Rising PSA (metastatic castrate resistant-crpc) Restaging bone scan and shows progression of bone mets Treatment Options?
22 Metastatic Prostate Cancer
 Potent multi-targeted androgen signaling pathway inhibitor Abiraterone or enzalutamide are recommended as first line for minimally symptomatic met CRPC or if")
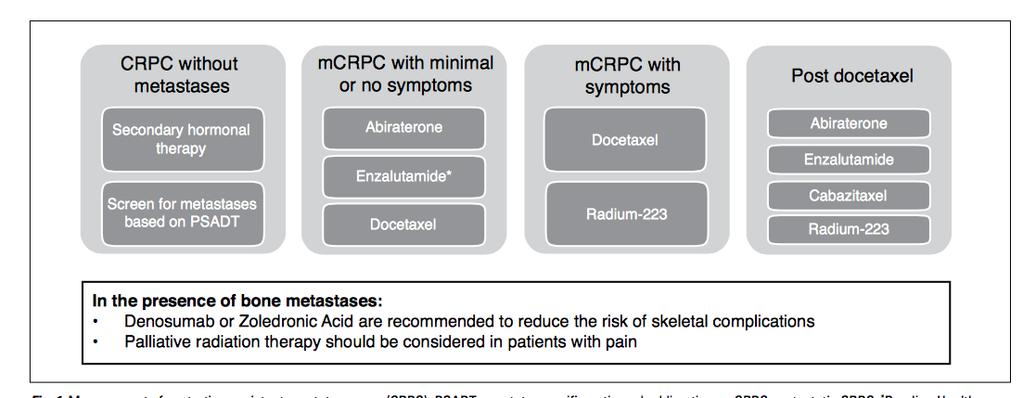
23 Androgen Receptor signaling inhibit androgen biosynthesis block androgen receptor activation Abiraterone Acetate (Zytiga) Potent irreversible inhibitor of CYP- 17 critical enzyme in androgen biosynthesis Enzalutamide (Xtandi) Potent multi-targeted androgen signaling pathway inhibitor Abiraterone or enzalutamide are recommended as first line for minimally symptomatic met CRPC or if progressing after docetaxel based chemotherapy (Level 1,grade A)
24 Abiraterone Acetate Cholesterol + Prednisone Desmolase Renin Pregnenolone Progesterone Deoxy- Corticosterone corticosterone X CYP17 17α-hydroxylase 11β- Hydroxylase Aldosterone 17α-OHpregnenolone X CYP17 C17,20-lyase 17α OHprogesterone 11-Deoxycortisol DHEA Androstenedione Testosterone 5α-reductase Cortisol DHT CYP19: aromatase ACTH Autocrine and paracrine (adrenal) pathways Attard G, et al. JCO. 2008;26: Estradiol
25 Abiraterone Acetate in Chemo-Naive mcrpc OS 30.3 mos (PBO) 34.7 mos (ABI); HR 0.81; P =.0033 Ryan CJ, et al. Lancet Oncol. 2015;16: Ryan CJ, et al. N Engl J Med. 2013;368:

26 Abiraterone Acetate: Safety Profile Ryan CJ, et al. Lancet Oncol. 2015;16:
27 PREVAIL: Enzalutamide in Chemo-Naive CRPC Overall Survival rpfs N = 1717; randomized 1:1 ENZ vs PBO Asymptomatic minimally symptomatic rpfs reduced by 81% Risk of death reduced by 29% Significantly delayed time to opiate initiation Beer TM, et al. N Engl J Med. 2014;371: Beer TM, et al. ASCO Abstract Loriot Y, et al. Lancet Oncol. 2015;16:

28 PREVAIL: Enzalutamide Safety Beer TM, et al. N Engl J Med. 2014;371:
29 Differences in drug characteristics Abiraterone Enzalutamide Oral yes yes Prednisone required yes no Drug interactions (CYP) yes yes Lowers seizure threshold no yes Potential liver toxicity yes less Risk for hypertension yes yes Risk for CV events, atrial fib Dose 250 mg x 4 40 mg tablets x 4 Empty stomach yes no yes yes
30 Timing and Selection of Secondary AR- Directed Therapies Similar OS, PFS from cross-trial comparisons Both are category 1 recommendations in NCCN guidelines Therefore choice is based on differential toxicity Abiraterone acetate for seizure-prone men and those more frail, elderly (> 75 years old) men at high risk for falls Enzalutamide for men with significant CV risk factors, contraindications to prednisone, brittle diabetes, and metabolic syndrome Significant cross-resistance, so initial choice is likely most important one
31 Bone targeted therapy Denosumab (Xgeva) or Zoledronic Acid (Zometa) inhibits osteoclast activity prevents SREs (Level 1,Grade A) Does not improve OS Watch for ONJ ~2%(appears time dependent) Only if bone mets present Castrate resistant PC Radium-223 (XOFIGO) recommended in patients with pain due to bone metastases and no visceral mets (Level 1,Grade A) Improves OS


32 Mechanism of Action of and Administration of Radium-223 Radium-223 is a short-range but high-energy alpha-emitting particle It targets osteoblastic bone metastases by acting as a calcium mimetic 2-10 cell diameter range of alpha-particle Radium-223 Perez et al. Principles and Practice of Radiation Oncology. 5th ed. Lippincott Williams & Wilkins; 2007.
33 Phase III ALSYMPCA Trial Eligibility (n = 921) Confirmed symptomatic CRPC 2 bone metastases 2:1 R Radium Best supportive care (n = 614) No visceral metastases Post docetaxel/unfit for docetaxel Placebo + Best supportive care (n = 307) Median overall survival: 14.9 versus 11.3 months Time to first skeletal-related event: 15.6 versus 9.8 months Bone pain Grade >3: 18% versus 23% Parker C et al. Proc ESMO 2012;Abstract 898PD.
34 Parker C, et al. New Engl J Med. 2013;369: ALSYMPCA: Predictors of Radium-223 Benefit?
35 ALSYMPCA Updated Analysis: Select Adverse Events All Grades Grades 3 or 4 Patients with AEs n, (%) Radium-223 n = 600 Placebo n = 301 Radium-223 n = 600 Placebo n= 301 Hematologic Anemia 187 (31) 92 (31) 77 (13) 39 (13) Neutropenia 30 (5) 3 (1) 13 (2) 2 (1) Thrombocytopenia 69 (12) 17 (6) 38 (6) 6 (2) Non-Hematologic Bone pain 300 (50) 187 (62) 125 (21) 77 (26) Diarrhea 151 (25) 45 (15) 9 (2) 5 (2) Nausea 213 (36) 104 (35) 10 (2) 5 (2) Vomiting 111 (18) 41 (14) 10 (2) 7 (2) Constipation 108 (18) 64 (21) 6 (1) 4 (1) Safety of taxane chemotherapy following radium-223 not well characterized Parker C, et al. New Engl J Med. 2013;369: Parker et al NEJM 2013
36 Radium-223: Summary Administration: Once every 4 wks for 6 infusions 60-second IV infusion Given by radiation oncologist or nuclear medicine radiologist Enteric excretion No pre-medication, no post-medication CBC check before each treatment Clinical Benefit: Primary endpoint of improvement in symptomatic SRE 3.6-mo benefit in OS Should be considered in symptomatic men with bone-predominant mcrpc Consider spinal imaging for epidural disease in men with high burden of disease and rapid progression; palliative EBRT should be used if high risk for spinal cord compression
37 Case 1C 12m later (metastatic CRPC progression on 1 st line) Pt doing well on AI and monthly denosumab minimal S/E but new hip pain Restaging bone scan and CT shows progression of bone mets Options? Radium 223-bone only disease docetaxel Cabazitaxel (post docetaxel) Palliative RT
38 Metastatic Prostate Cancer
39 Metastatic CRPC Phase III Trials Agent Setting Comparator Arm in Trial OS Benefit, Months (HR) Docetaxel Mitoxantrone 2.4 (0.76) Abiraterone Chemotherapy- Naïve Prednisone 4.4 (0.81) Enzalutamide Placebo 2 (0.70) Cabazitaxel Mitoxantrone 2.4 (0.70) Abiraterone Post-Docetaxel Prednisone 4.6 (0.74) Enzalutamide Placebo 4.8 (0.63) Radium-223 Placebo 3.6 (0.70) +/- Chemotherapy Sipuleucel-T Placebo 4.1 (0.78) 39
 Mitoxantrone has not shown any survival advantage, but may give")
40 Chemotherapy Docetaxel 75mg/m2 q3weeks with prednisone for met CRPC (Level 1, grade A) Cabazitaxel is recommended for mcrpc patients progressing on or following docetaxel (Level 1, Grade A) For patients who have had a good response to first-line docetaxel re-treatment with docetaxel can be considered (Expert Opinion) Mitoxantrone has not shown any survival advantage, but may give symptomatic relief. Of note in the second-line setting, mitoxantrone has limited activity and increased toxicity (Grade C).
41 Case 1D 12 months later (metastatic CRPC progressing on 2 nd line) Was doing OK after receiving radium 223 then was started on cabazitaxel chemotherapy but CT shows new adenopathy and liver lesion To recap: 1. Continuous ADT 2. Early docetaxel chemotherapy 3. AI therapy 4. Bone protective therapy 5. Bone targeted therapy 6. 2 nd line chemotherapy Wants something else
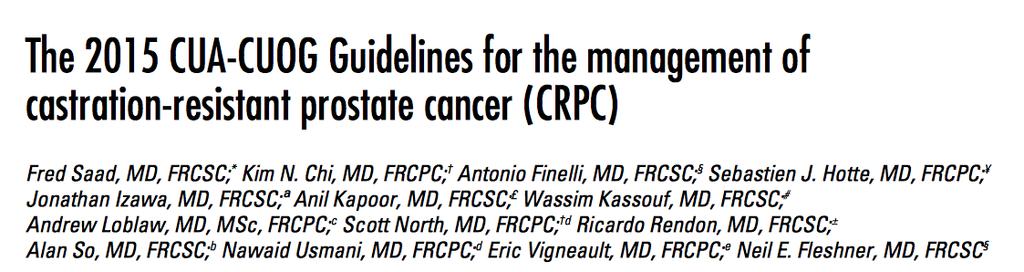
![Immuno-Oncology Atezolizumab Inhibits the Binding of PD-L1 to PD-1 and B7.1 can restore antitumor T-cell activity and enhance T-cell priming [1] 1. Petrylak DP, et al. ASCO 2015. Abstract 4501. 2. Akbari O, et al.](/docs-images/80/80917316/images/42-1.jpg "Mucosal Immunol. 2010;3:81-91. 3. Matsumoto et al. Biochem Biophys Res Commun. 2008;365:170-175. 4. Brown JA, et al. J Immunol. 2003;170:1257-1266. 5. Latchman Y, et al. Nat Immunol. 2001;2:261-268.")
42 Immuno-Oncology Atezolizumab Inhibits the Binding of PD-L1 to PD-1 and B7.1 can restore antitumor T-cell activity and enhance T-cell priming [1] 1. Petrylak DP, et al. ASCO Abstract Akbari O, et al. Mucosal Immunol. 2010;3: Matsumoto et al. Biochem Biophys Res Commun. 2008;365: Brown JA, et al. J Immunol. 2003;170: Latchman Y, et al. Nat Immunol. 2001;2: Slide credit: clinicaloptions.com

43 Genomic targeted therapy

44 Genomics to classify based on actionable mutation
45 Target Matched to Drug

46 Approach to Metastatic PC 1. Maintain castrate levels testosterone 2. Bone-directed therapy 3. Androgen Receptor Inhibition 4. Chemotherapy 5. Palliative RT if indicated 6. Clinical trials
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD
 Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS.
 ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE
 mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER
 INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
The Role of the Medical Oncologist in the Treatment of Prostate Cancer. Alireza saadat hematologist and oncologist
 The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
ESMO SUMMIT AFRICA Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit
 ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
SUMMARY. 3. Emerging understanding of mechanisms of resistance to current treatments
 SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
Castrate-resistant prostate cancer: Bone-targeted agents. Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia
 Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Elderly men with prostate cancer + ADT
 Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
Bone targeting: bisphosphonates, RANK-ligands and radioisotopes. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Bone targeting: bisphosphonates, RANK-ligands and radioisotopes Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee
Bone targeting: bisphosphonates, RANK-ligands and radioisotopes Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee
Developmental Therapeutics for Genitourinary Malignancies
 Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Present and Future Perspectives in Treatment of mcrpc Patients
 Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena
 Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Board Review 2017: Prostate Cancer. Dana Rathkopf, MD Associate Attending
 Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
A Forward Look at Options for. In Prostate Cancer
 A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Bone-targeted therapies for prostate cancer in Institut Gustave Roussy Villejuif, France
 Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
Alpha-emitting Radionuclides: Ra-223
 Alpha-emitting Radionuclides: Ra-223 prof. dr. K. Goffin Nuclear Medicine and Molecular Imaging Department of Imaging & Pathology UZ Leuven KU Leuven Belgium International Course on Theranostics and Molecular
Alpha-emitting Radionuclides: Ra-223 prof. dr. K. Goffin Nuclear Medicine and Molecular Imaging Department of Imaging & Pathology UZ Leuven KU Leuven Belgium International Course on Theranostics and Molecular
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER. ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA
 ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA MAY 2018 DISCLAIMER Please note: The views expressed within
ADVANCES IN METASTATIC HORMONE-SENSITIVE PROSTATE CANCER ALICIA K. MORGANS, MD, MPH Associate Professor of Medicine Northwestern University, USA MAY 2018 DISCLAIMER Please note: The views expressed within
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
MÉTASTASES OSSEUSES ET RADIUM 223
 MÉTASTASES OSSEUSES ET RADIUM 223 Marie-Laure Amram Service d oncologie Hôpitaux Universitaires de Genève Forome du 21.05.2015 Radium-22:3:mécanisme d action Mécanisme d action Mécanisme d action Radium-223
MÉTASTASES OSSEUSES ET RADIUM 223 Marie-Laure Amram Service d oncologie Hôpitaux Universitaires de Genève Forome du 21.05.2015 Radium-22:3:mécanisme d action Mécanisme d action Mécanisme d action Radium-223
PRO STATE of the art. METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature
 PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
Convegno Nazionale AIOM Giovani 2016: News in Oncology. Daniele Alesini. Istituto Nazionale dei Tumori Regina Elena
 Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE
 NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
mcrpc in 2016 How to decide the optimal treatment? N. Mottet
 mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
Prostate Cancer: Castrate Resistant
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Prostate Cancer: Castrate Resistant Andrew J. Armstrong, MD, ScM Duke Cancer Institute Bridget Koontz, MD Duke
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Prostate Cancer: Castrate Resistant Andrew J. Armstrong, MD, ScM Duke Cancer Institute Bridget Koontz, MD Duke
Radiopharmaceuticals for treating CRPC patients with metastatic bone disease 2014/6/27
 Radiopharmaceuticals for treating CRPC patients with metastatic bone disease 和信醫院黃玉儀 2014/6/27 Bone metastases in prostate cancer The most common site of metastasis in prostate cancer In >90% patients
Radiopharmaceuticals for treating CRPC patients with metastatic bone disease 和信醫院黃玉儀 2014/6/27 Bone metastases in prostate cancer The most common site of metastasis in prostate cancer In >90% patients
Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies. Michael J. Morris, MD
 Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies Michael J. Morris, MD www.mskcc.org Disclosures Research funding (institutional contracts): Sanofi
Management of chronic pre-existing or treatment-emergent adverse events of the other systemic therapies Michael J. Morris, MD www.mskcc.org Disclosures Research funding (institutional contracts): Sanofi
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi?
 ADT e Terapia ormonale: quando e a chi?") Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
Dr. Tia Higano University of Washington Seattle, USA
 AN UPDATE ON THE TREATMENT OF PATIENTS WITH mcrpc WITH RA-223 PLUS AAP Dr. Tia Higano University of Washington Seattle, USA AAP, Abiraterone Acetate and Prednisone/Prednisolone; mcrpc, metastatic Castration-Resistant
AN UPDATE ON THE TREATMENT OF PATIENTS WITH mcrpc WITH RA-223 PLUS AAP Dr. Tia Higano University of Washington Seattle, USA AAP, Abiraterone Acetate and Prednisone/Prednisolone; mcrpc, metastatic Castration-Resistant
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP)
") Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Professor of Urology Vice Chair Department of Urology UMassMemorial
Advanced Therapeutic Strategies in the Successful Management of Patients with Castrate Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Professor of Urology Vice Chair Department of Urology UMassMemorial
Novel Agents in the Treatment of Metastatic Castration-Resistant Prostate Cancer (CRCP)
") Novel Agents in the Treatment of Metastatic Castration-Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Vice Chair, Dept. Urology Professor of Urology UMassMemorial Medical Center/ U Mass Medical
Novel Agents in the Treatment of Metastatic Castration-Resistant Prostate Cancer (CRCP) Pamela Ellsworth, MD Vice Chair, Dept. Urology Professor of Urology UMassMemorial Medical Center/ U Mass Medical
SAMPLE ONLY. Your Health Matters. Advanced Prostate Cancer and its Treatment A Patient Guide. Please order from Documents and Media: 415/
 Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media: