Management of castrate resistant disease; after first line hormone therapy fails
|
|
|
- Jordan Skinner
- 5 years ago
- Views:
Transcription
1 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge Centre for Oncology Syed.Hussain@liverpool.ac.uk
 Docetaxel chemotherapy The Nobel Prize in Physiology or Medicine")

2 Treatment of Advanced PCa Few Advances Before 2010 Only two therapies proven to improve survival Blockers of testicular testosterone synthesis (first line) Docetaxel chemotherapy The Nobel Prize in Physiology or Medicine 1966 was divided equally between Peyton Rous "for his discovery of tumour-inducing viruses" and Charles Brenton Huggins "for his discoveries concerning hormonal treatment of prostatic cancer". Charles Huggins: Nobel Prize 1966
![Advanced Prostate Cancer Unprecedented Progress In the last 2 years, 5 treatments shown to improve OS Abiraterone [a] Sipuleucel-T [b] Cabazitaxel [c] Alpharadin [d] MDV3100 [e] a. de Bono JS, et al.](/docs-images/85/93019198/images/3-1.jpg "N Engl J Med. 2011;364:1995-2005. b. Kantoff PW, et al. N Engl J Med. 2010;363:411-422. c. de Bono JS, et al. Lancet. 2010;376:1147-1154. d. Parker C, et al. ESMO 2011. e. de Bono JS et al, Proceedings of ASCO 2012")
3 Advanced Prostate Cancer Unprecedented Progress In the last 2 years, 5 treatments shown to improve OS Abiraterone [a] Sipuleucel-T [b] Cabazitaxel [c] Alpharadin [d] MDV3100 [e] a. de Bono JS, et al. N Engl J Med. 2011;364: b. Kantoff PW, et al. N Engl J Med. 2010;363: c. de Bono JS, et al. Lancet. 2010;376: d. Parker C, et al. ESMO e. de Bono JS et al, Proceedings of ASCO 2012
 Median Survival Benefit = 4.1 months Sipuleucel-T (n = 341) Median Survival: 25.8 mo.")

4 Sipuleucel T Cellular immunotherapy 36.5 mo median f/u HR = (95% CI: 0.606, 0.951) P =.017 (Cox model) Median Survival Benefit = 4.1 months Sipuleucel-T (n = 341) Median Survival: 25.8 mo. 36 mo. survival: 32.1% Placebo (n = 171) Median Survival: 21.7 mo. 36 mo. survival: 23.0% No. at Risk Sipuleucel-T Placebo Kantoff PW, et al. N Engl J Med. 2010;363:
5 Cabazitaxel: Tubulin binding drug Activity in docetaxel treated patients Median OS benefit 2.4 months de Bono J et al, The Lancet 2010

6 Abiraterone: CYP17 inhibitor Updated Analysis (775 Events) Median OS Benefit: 4.6 Months Median duration of follow-up: 20.2 months Median duration of treatment: AA, 8 months vs placebo, 4 months de Bono et al, NEJM 2011
 OS Benefit: 2.8 months (final analyses: 3.")
7 Radium 223 Phase III trial Alpha particle emitting radio-isotope Median (interim) OS Benefit: 2.8 months (final analyses: 3.6m) Parker C et al, ESMO 2012
8 Survival (%) MDV3100: Novel AR antagonist HR = (0.529, 0.752) P < % Reduction in Risk of Death MDV3100: 18.3 months (95% CI: 17.3, NYR) Placebo: 13.6 months (95% CI: 11.3, 15.8) Duration of Overall Survival, Months MDV Placebo Median OS Benefit: 4.8 Months de Bono et al, ASCO 2012
9 Presentation Overview Insight into disease biology: key therapeutic targets Improving treatment: changing landscape Future challenges

10 Prostate Cancer Biology Yap TA, et al. Nat Rev Clin Oncol. 2011;8:
 AR mutations that increase AR (transcriptional) activity AR (< 2x) expression (ligand driven) in")
11 Androgen Receptor Addiction Hard Habit to Break Hormonal treatments continue to have antitumor activity High levels of intratumoral androgens despite castration Preclinical and clinical evidence of intracrine synthesis Castration resistance associated with AR amplification (increased gene dose) AR mutations that increase AR (transcriptional) activity AR (< 2x) expression (ligand driven) in isogenic resistant lines AR still switched on in Abiraterone- and MDV3100- resistant PCa Identification of oncogenic translocations/fusions driven by androgens + estrogen-response elements (ETS genes; TMPRSS2/ERG in 50% to 70% of PCa) Attard G, et al. Cancer Cell. 2009;16:
12 Abiraterone Acetate Oral potent, selective + irreversible inhibitor of CYP17 Inhibits testosterone production in testis, adrenal glands and prostate Inhibition of CYP17 lowers androgens Produces super-castrate levels >10-fold more potent than ketoconazole

13 MDV 3100 Novel AR antagonist Blocks nuclear translocation of AR and its binding to DNA. Phase I/II trial; n=140; 7 dose levels CTC counts: Favourable >90%maintained; Unfavourable 50-60% converted Phase III (AFFIRM study): Post-docetaxel MDV3100 vs. Placebo


14 a. Attard G, et al. J Clin Oncol. 2008;26: ; b. Attard G, et al. J Clin Oncol. 2009;27: ; c. Reid AH, et al. J Clin Oncol. 2010;28: ; d. Ryan C, et al. J Clin Oncol. 2010;28: ; e. Danila D, et al. J Clin Oncol. 2010;28: Abiraterone Acetate Androgen Biosynthesis Inhibitor Androgens produced at 3 critical sites lead to tumor proliferation Testes Adrenal gland Prostate tumor cells Abiraterone inhibits biosynthesis of androgens that stimulate tumor cell growth PSA and radiographic responses in phase 1-2 studies Chemotherapy-naive and postchemotherapy patients [a-e]

15 Abiraterone Mechanism of Action ACTH Positive drive x 5 Hypokalemia Hypertension Fluid overload Suppression of renin Negative feedback Pregnenolone Deoxycorticosterone x 10 Corticosterone x 40 Aldosterone x 1.5 CYP17: 17α-hydroxylase 17OH-Pregnenolone 17OH-Progesterone x 3 11-deoxycortisol x 4 Cortisol x 2 CYP17: C17,20-lyase Testosterone < 1 ng/dl DHEA x 3 Androstenedione < 2 ng/dl Estradiol < 80 ng/dl Attard G, et al. J Clin Oncol. 2008;26:
16 Abiraterone Phase 1 Study in CRPC Continuous daily dosing (N = 21) mg daily to fasted chemotherapy-naive patients Abiraterone administered without steroids Mineralocorticoid antagonist eplerenone utilized No dose-limiting toxicity Satisfactory dose-proportional pharmacokinetics Pharmacodynamic endocrine data Suppression of hormone levels downstream of CYP17; increases in hormone levels upstream of CYP17; PSA decline; CTC decline Attard G, et al. J Clin Oncol. 2008;26:
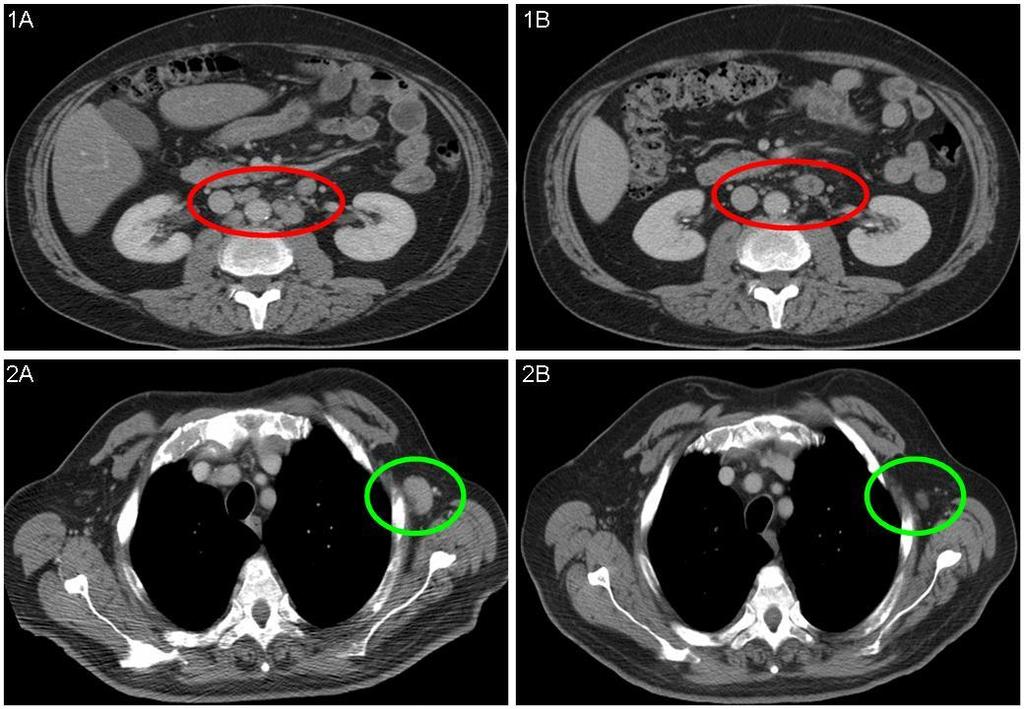
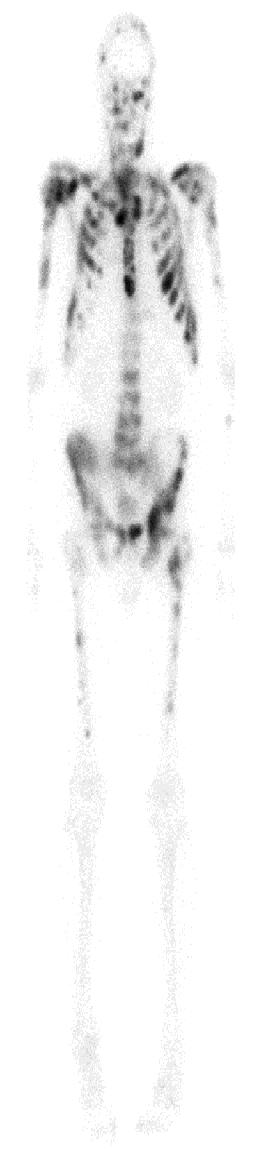

17 Abiraterone Acetate Antitumor Activity


 within 3 mos Shrinkage of")
18 Patient Receiving Abiraterone Regressing Pelvic Nodes Prestudy: 20 mm After 6 mos: 4 mm Previous progression on several hormone treatments PSA decline from 34.3 ng/ml 0.21 ng/ml (99%) within 3 mos Shrinkage of lymph glands shown above on CT scan
 pain over previous 24 hrs, previous Placebo chemotherapy, + Prednisone type of progression 5 mg BID (n = 398) de Bono J, et al.")
19 COU-AA-301 Phase 3 Study of Abiraterone in mcrpc Patients with mcrpc progressing after 1-2 chemotherapy regimens, 1 of which contained docetaxel (N = 1195) Randomized 2:1 Abiraterone acetate 1000 mg/day + Stratified Prednisone by ECOG 5 mg BID PS, worst (n = 797) pain over previous 24 hrs, previous Placebo chemotherapy, + Prednisone type of progression 5 mg BID (n = 398) de Bono J, et al. N Engl J Med. 2011;364:
 40 20 0 Placebo: 10.9 mos (95% CI: 10.2-12.0) Median OS with 2 prior chemo: 14.0 mos AA vs 10.")
20 Survival (%) de Bono J, et al. N Engl J Med. 2011;364: COU-AA-301 Improved OS at Interim Analysis HR: (95% CI: ; P <.0001) Abiraterone acetate: 14.8 mos (95% CI: ) Placebo: 10.9 mos (95% CI: ) Median OS with 2 prior chemo: 14.0 mos AA vs 10.3 mos placebo Days From Randomization AA Placebo Median OS with 1 prior chemo 15.4 mos AA vs 11.5 mos placebo
21 COU-AA-301 Updated Analysis (775 Events) OS Benefit Increased From 3.9 to 4.6 Months Median duration of follow-up: 20.2 months Median duration of treatment: AA, 8 months vs placebo, 4 months
22 COU-AA-301 Survival Across Patient Subgroups Variable Subgroup n HR 95% CI All subjects All Baseline ECOG Baseline BPI < No. of prior chemo regimens Type of progression PSA only Radiographic Baseline PSA above median Yes Visceral disease at entry Yes Baseline LDH above median Yes Baseline ALK-P above median Yes Region North America Other Favors abiraterone Favors placebo de Bono J, et al. N Engl J Med. 2011;364:
 PSA response rate, % HR (95% CI) P Value <.0001 <.0001 Total 38.0 10.1 <.0001 Confirmed 29.1 5.5 <.0001 de Bono J, et al. N Engl J Med.")
23 COU-AA-301 Secondary Endpoints Endpoint Characteristic Abiraterone (n = 797) Placebo (n = 398) TTPP, mos ( ) rpfs, mos ( ) PSA response rate, % HR (95% CI) P Value <.0001 <.0001 Total <.0001 Confirmed <.0001 de Bono J, et al. N Engl J Med. 2011;364:

24 COU-AA-301 Summary of AEs AE, % Abiraterone (n = 791) All Grades Grades 3/4 All Grades Placebo (n = 394) Grades 3/4 All treatment-emergent AEs Serious AEs AEs leading to discontinuation AEs leading to death Deaths within 30 days of last dose Underlying disease Other specified cause de Bono J, et al. N Engl J Med. 2011;364:
25 COU-AA-301 AEs of Special Interest Abiraterone (n = 791) Placebo (n = 394) AE, % All Grades Grades 3/4 All Grades Grades 3/4 Fluid retention Hypokalemia LFT abnormalities Hypertension Cardiac disorders de Bono J, et al. N Engl J Med. 2011;364:
26 Patients Without Progression (%) QOL Time to FACT-P Deterioration AA + prednisone Placebo + prednisone p < Days on Study 500 The median time to functional status degradation (FACT-P total score) was 12.1 months in the AA + prednisone group vs 8.4 months in the placebo + prednisone group
27 AFFIRM Phase 3 Registration Trial of MDV3100 in Chemotherapy CRPC Patients Post- 2 MDV3100 QD R 1 Placebo QD Primary Endpoint: 25% survival increase (12 to 15 months) Sample size: ~1170 (780 and 390) Statistics: 85% Power; p=0.05, two-sided Scher, H. (North America) and De Bono, J. Co-PI, Medivation
28 Survival (%) MDV3100: Novel AR antagonist HR = (0.529, 0.752) P < % Reduction in Risk of Death MDV3100: 18.3 months (95% CI: 17.3, NYR) Placebo: 13.6 months (95% CI: 11.3, 15.8) Duration of Overall Survival, Months MDV Placebo Median OS Benefit: 4.8 Months de Bono et al, ASCO 2012
29 OS Benefit in Recent Post-Chemotherapy CRPC Trials Trial/ Agent/ Date Approved Mechanism Comparator Survival (months) Hazard Ratio P-value Reference AFFIRM Enzalutamid e Androgen Receptor Signaling Inhibitor Placebo 18.4 vs < de Bono et al, ASCO 2012 COU-AA-301 Abiraterone + prednisone 2011 CYP17 Inhibitor Placebo + prednisone 14.8 vs < de Bono et al, NEJM 2011 TROPIC Cabazitaxel + prednisone 2010 Cytotoxic Mitoxantrone + prednisone 15.1 vs < de Bono et al, Lancet 2010 Radium 223* Alpha-particle emitting radionuclide Placebo 14.9 vs Parker et al, ESMO 2011 * Only 60% of these patients were post-docetaxel patien
 Asymptomatic or mildly symptomatic R A N D O M I Z E D 1:1 AA 1000 mg daily")
 Time to initiation of")

30 Ryan, Smith, de Bono et al, Proc ASCO 2012 Overall Study Design of COU-AA-302 Patients Progressive chemonaïve mcrpc patients (Planned N = 1088) Asymptomatic or mildly symptomatic R A N D O M I Z E D 1:1 AA 1000 mg daily Prednisone 5 mg BID (Actual n = 546) Placebo daily Prednisone 5 mg BID (Actual n = 542) Efficacy end points Primary: rpfs by central review OS Secondary: Time to opiate use (cancer-related pain) Time to initiation of chemotherapy Time to ECOG-PS deterioration TTPP Phase 3 multicenter, randomized, double-blind, placebo-controlled study conducted at 151 sites in 12 countries; USA, Europe, Australia, Canada Stratification by ECOG performance status 0 vs 1
31 Progression Free (%) Statistically Significant Improvement in rpfs Primary End Point AA + P (median, mos): NR PL + P (median, mos): 8.3 HR (95% CI): 0.43 ( ) P value: < AA Placebo Time to Progression or Death (Months) AA Placebo Data cutoff 12/20/2010. NR, not reached; PL, placebo. Ryan, Smith, de Bono et al, Proc
32 Survival (%) Strong Trend in OS Primary End Point* AA Placebo Time to Death (Months) AA + P (median, mos): NR PL + P (median, mos): 27.2 HR (95% CI): 0.75 ( ) P value: AA Placebo *O Brien-Fleming boundary used; Data cut off 12/20/2011; Nominal significance level
33 Safety Profile Consistent Despite Longer Duration of Exposure AA + P (n = 542) % Placebo + P (n = 540) % All Grades Grades 3/4 All Grades Grades 3/4 Fatigue Fluid retention Hypokalemia Hypertension Cardiac disorders Atrial fibrillation ALT increased AST increased Most of the ALT and AST increases occurred during the
34 Consistent Pattern of Benefit Delays disease progression Statistically significant improvement in rpfs Improves survival OS trend (p = ) favors AA 27.2 month OS in control arm Extensive subsequent therapy Maintains quality of life Extend time with minimal or no symptoms Full QOL analysis ongoing Ryan, Smith, de Bono et al, Proc ASCO 2012
35 Combining Abiraterone and MDV3100 Resistance mechanisms to abiraterone Residual steroids can activate promiscuous AR Upstream of CYP17 Eplerenone Prednisolone, dexamethasone Increased androgenic steroid levels induce resistance to MDV3100
36 AR Signaling as Therapeutic Target Conclusion Advanced prostate cancer Not hormone refractory Nor androgen independent Remains nuclear steroid receptor driven even after AA and MDV3100 Hormone therapy works after chemotherapy Important since OS remains only robust registration endpoint Maximal androgen blockade is a misnomer
37


38 Mitoxantrone and Prednisone Response % p= p=ns 0 Pain Response M & P Prednisone PSA Response Tannock et al., JCO 14: , 1996
39 Mitoxantrone and Prednisone Pain Relief Duration p< Weeks Prednisone M & P Tannock et al., JCO 14: , 1996
40 Efficacy analysis (Intent to treat; p-values and hazard ratios vs. Arm C): Arm A (D q3wk+p)n=335 Arm B (D qwk+p)n=334 Arms A+B N=669 Arm C (MTZ+P)N= 337 Median Survival 18.9 mo 17.4 mo 18.3 mo 16.5 mo Hazard Ratio (95% CI) 0.76 ( ) p= ( )p= ( )p=0.04 NA Pain Response* 35%p= %p= %p= % PSA Response** 45%p= %p< %p< % * Pts with baseline present pain intensity 2 (A/153; B/154; C/157). ** Pts with baseline PSA 20ng/ml (Arm/pts: A/291; B/282; C/300). Conclusions: The D q3wk +P schedule improved overall survival and increased pain response and PSA response vs MTZ+P. It was well tolerated, but with more grade 3/4 neutropenia than MTZ+P. This is the first phase III study to show a significant survival benefit in HRPC. (Supported by Aventis) Tannock IF et al, N Engl J Med Oct 7;351(15):

 19.2 0.79.004 Weekly: 285 (85.")

41 Proportion Alive TAX 327 Long-Term Overall Survival Taxotere q 3 wk Weekly Taxotere* Mitoxantrone* Events (%) Median Survival (mo) Hazard Ratio P- Value Weekly: 285 (85.1%) Weekly: 285 (85.4%) Mitoxantrone: 297 (88.1%) Year Berthold DR, et al. J Clin Oncol 2008;26
42 Rate (%) TAX 327 Efficacy * 60 * Docetaxel q3w (n=335) Docetaxel qw (n=334)* Mitoxantrone q3w (n=337)* PSA response Pain relief Improved QOL P values are comparisons with mitoxantrone group; *P<0.001; P= QOL = quality of life. Tannock et al. N Engl J Med. 2004;351:1502. *Not a licensed indication in the UK
43 TAX 327 Docetaxel 3 Weekly Safe Significantly improves: - Survival (18.9 vs 16.5 months) 24% reduction in the risk of death ( 95% CI , p=.009) - PSA decline - 45% vs. 32%, p= Pain response - 35% vs. 22%, p=.01 - Quality of life response 22% vs 13%
44 Cabazitaxel: A Next-Generation Taxane New semi-synthetic taxane Selected to overcome the emergence of taxane resistance¹ Microtubule stabilizer² Preclinical data As potent as docetaxel against sensitive cell lines and tumor models¹, ² Activity against tumor cells and tumor models that are resistant to, or not sensitive to currently available taxanes¹, ² Clinical data In Phase I trials DLT was neutropenia Antitumor activity in mcrpc in Phase I including docetaxel-resistant disease 3 ¹Attard G, Greystoke A, Kaye S, De Bono J. Pathol Biol (Paris). 2006;54(2): ²Pivot X, Koralewski P, Hidalgo JL, et al. Ann Oncol. 2008;19(9): Mita AC, Denis LJ, Rowinsky EK, de bono JS et al. Clin Can Res. 2009; Jan 15;15(2):
45 TROPIC: Phase III Registration Study 146 Sites in 26 Countries mcrpc patients who progressed during and after treatment with a docetaxel-based regimen (N=755) Stratification factors ECOG PS (0, 1 vs. 2) Measurable vs. non-measurable disease cabazitaxel 25 mg/m² q 3 wk + prednisone* for 10 cycles (n=378) *Oral prednisone/prednisolone: 10 mg daily. Primary endpoint: OS Secondary endpoints: Progression-free survival (PFS), response rate, and safety mitoxantrone 12 mg/m² q 3 wk + prednisone* for 10 cycles (n=377) Inclusion: Patients with measurable disease must have progressed by RECIST; otherwise must have had new lesions or PSA progression 45
46 Primary Endpoint: Overall Survival (ITT Analysis) Proportion of OS (%) Median OS (months) Hazard Ratio 95% CI P-value MP CBZP < Number at risk 0 0 months 6 months 12 months 18 months 24 months 30 months MP CBZP
47 Progression-Free Survival (PFS) Results Proportion of PFS (%) Median PFS (months) Hazard Ratio 95% CI P-value MP <.0001 CBZP PFS composite endpoint: PSA progression, pain progression, tumor progression, symptom deterioration, or death Number at risk 0 0 months 3 months 6 months 9 months 12 months 15 months 18 months 21 months MP CBZP
48 Most Frequent Grade 3 Treatment-Emergent AEs* Safety Population MP (n=371) CBZP (n=371) All grades (%) Grade 3 (%) All grades (%) Grade 3 (%) Any adverse event Febrile neutropenia Diarrhea Fatigue Asthenia Back pain Nausea Vomiting Hematuria Abdominal pain *Sorted by decreasing frequency of events grade 3 in the CBZP arm. 48
49 Conclusions Cabazitaxel demonstrated a statistically and clinically significant OS improvement compared with mitoxantrone in study population 30% risk reduction of death (HR = 0.70, P<.0001) Median OS improvement in favor of CBZP: 15.1 months vs 12.7 months OS benefit was consistent across subgroups Secondary endpoints of PFS, RR, and TTP were also significantly improved Safety profile was predictable and manageable Neutropenia, diarrhea, fatigue and asthenia were the most common adverse events Cabazitaxel is a potential new therapeutic option for the treatment of patients with mcrpc after failure of docetaxel-based therapy 49
50


51 Docetaxel/Prednisolone Re-treatment- Birmingham, UK First-line treatment- 107 patients 650 cycles Median no 6 (1-10) Second-line 22 patients 119 cycles Median no- 6 (2-10) Third-line 7 patients 38 cycles Median no-5 (3-10)
52 % of cycles Haematological toxicity Gr 3/4 Neutropenia 1 0 1st line 2nd line 3rd line Docetaxel chemotherapy

53 Cabozantinib Demonstrated Unique Clinical Activity in Phase 2 Studies in mcrpc Clinical activity in mcrpc 1 PFS improvement Bone scan images High rates of bone scan improvement Pain improvement and narcotics reduction Reduction in bone markers Regression of soft tissue disease PSA changes discordant with other measures of antitumor activity Baseli ne Follow -up Interim Jul-13Results Phase 2 RDT Cohort (M. Hussain, ASCO 2011) 53
54 % Change from Baseline 40 Change in Pain Scores Patients with baseline score 4 (n=39) C * * * * C C C C C C C C Prior therapies: Docetaxel Docetaxel + Abiraterone or MDV3100 C Cabazitaxel Radionuclide * 64% had a pain decrease 30% Median change in pain: 46% reduction 56% decreased narcotics use, including 31% who discontinued narcotics Interim Jul-13Results Phase 2 NRE Cohort (M. Smith, ASCO 2012) 54
55 Best % Change in CTCs C 300 Change in Circulating Tumor Cells Baseline CTCs 5 and Week 6 and/or Week 12 assessment (n=62) C * Prior therapies: Docetaxel Docetaxel + Abiraterone or MDV3100 C Cabazitaxel Radionuclide * CC C C C C CC C C C C * * * % demonstrated best CTC decrease 30% Median best CTC change: 86% decrease Conversion to <5 CTCs: 39% at Week 6 Interim Jul-13Results Phase 2 NRE Cohort (M. Smith, ASCO 2012) 55
56 Cabozantinib in chemotherapy-pretreated mcrpc Most Frequently Reported Adverse Events (N=93) 84% of patients experienced at least one dose reduction due to AE with 100 mg starting dose Adverse Event All Grades, n (%) Grade 3, n (%) Grade 4, n (%) Fatigue 77 (83) 24 (26) 2 ( 2) Decreased appetite 68 (73) 6 (6) Diarrhea 65 (70) 10 (11) Nausea 62 (67) 9 (10) Vomiting 35 (38) 4 (4) Dysgeusia 35 (38) Weight decreased 34 (37) 3 (3) Dysphonia 33 (35) Back pain 32 (34) 5 (5) 2 (2) Dyspnea 30 (32) 4 (4) 1 (1) Hypothyroidism 29 (31) Adverse Events of Interest Hand-foot syndrome 23 (25) 5 (5) Hypertension 22 (24) 8 (9) Thrombosis venous 12 (13) 1 (1) 5 (5) One patient with extensive liver disease experienced a related Grade 3 portal vein thrombosis with Grade 5 liver failure Interim Jul-13 Results Phase 2 NRE Cohort (M. Smith, ASCO 2012) 56
57 Clinical trials in advanced CRPC SOTIO: Docetaxel plus DC Vaccine versus Docetaxel plus placebo ASTEX STUDY: ABIRATERONE /HSP90 Inhibitor TOPARP COMET-1 COMET-2

")
58 CRPC Current Landscape Multiple lines of treatment for advanced prostate cancer that improve OS: Sipuleucel-T, docetaxel, abiraterone, cabazitaxel, MDV3100, alpharadin Optimal sequence of administration now needs defined: Combinations! Cross-resistance: taxanes, abiraterone and MDV3100? Abiraterone will move into prechemotherapy space and now also being evaluated in large adjuvant trial (STAMPEDE) MDV ara Yap TA, et al. Nat Rev Clin Oncol. 2011;8:
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
A Forward Look at Options for. In Prostate Cancer
 A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD
 Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
SUMMARY. 3. Emerging understanding of mechanisms of resistance to current treatments
 SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
- La Terapia Farmacologica -
 XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
Evolution of Chemotherapy for. Cancer
 Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia
 Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER
 INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
The Role of the Medical Oncologist in the Treatment of Prostate Cancer. Alireza saadat hematologist and oncologist
 The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer. Michal Mego
 National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Published on The YODA Project (
 Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Developmental Therapeutics for Genitourinary Malignancies
 Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Convegno Nazionale AIOM Giovani 2016: News in Oncology. Daniele Alesini. Istituto Nazionale dei Tumori Regina Elena
 Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Convegno Nazionale AIOM Giovani 2016: News in Oncology Daniele Alesini Istituto Nazionale dei Tumori Regina Elena Something Old Something New Something Borrowed Something Blue DOCETAXEL: BACK AND FORTH
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T
 Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Advances in Chemotherapy for Castration Resistant Prostate Cancer
 Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
Prostate Cancer: Vision of the Future By: H.R.Jalalian
 1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, Nasdaq: DNDN
 Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Current Chemotherapy for Castration Resistant Prostate Cancer
 Current Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine at Columbia University Medical Center/NY Presbyterian Hospital Disclosure Consultant: Sanofi Aventis,
Current Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine at Columbia University Medical Center/NY Presbyterian Hospital Disclosure Consultant: Sanofi Aventis,
ESMO SUMMIT AFRICA Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit
 ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
ESMO SUMMIT AFRICA 2018 Practice changing studies in Prostate Cancer in 2016 and 2017 and cost-effectiveness Ronald de Wit CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche Merck Lilly 14 years of
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
Management Options in Advanced Prostate Cancer: What is the Role for Sipuleucel-T?
 Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
January Abiraterone pre-docetaxel for patients with asymptomatic or minimally symptomatic metastatic castration resistant prostate cancer
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
Tubulin-binding drug In prostate cancer
 Tubulin-binding drug In prostate cancer Dr Christophe Massard Institut Gustave Roussy, Department of Cancer Medicine christophe.massard@igr.fr TAT Meeting, Paris, 2011 U981 Chemotherapy in Prostate Cancer
Tubulin-binding drug In prostate cancer Dr Christophe Massard Institut Gustave Roussy, Department of Cancer Medicine christophe.massard@igr.fr TAT Meeting, Paris, 2011 U981 Chemotherapy in Prostate Cancer
Michiel H.F. Poorthuis*, Robin W.M. Vernooij*, R. Jeroen A. van Moorselaar and Theo M. de Reijke
 First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
First-line non-cytotoxic therapy in chemotherapynaive patients with metastatic castration-resistant prostate cancer: a systematic review of 10 randomised clinical trials Michiel H.F. Poorthuis*, Robin
pan-canadian Oncology Drug Review Final Clinical Guidance Report Abiraterone Acetate (Zytiga) for Metastatic Castration-Resistant Prostate Cancer
 for Metastatic Castration-Resistant Prostate Cancer") pan-canadian Oncology Drug Review Final Clinical Guidance Report Abiraterone Acetate (Zytiga) for Metastatic Castration-Resistant Prostate Cancer October 22, 2013 DISCLAIMER Not a Substitute for Professional
pan-canadian Oncology Drug Review Final Clinical Guidance Report Abiraterone Acetate (Zytiga) for Metastatic Castration-Resistant Prostate Cancer October 22, 2013 DISCLAIMER Not a Substitute for Professional
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena
 Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Il Trattamento della Malattia CRPC metastatica Terapie Radiometaboliche Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena AIOM: Gestione ottimale del Paziente con Carcinoma della
Con$nuing Care for Your Pa$ents with Metasta$c CRPC
 27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
FUJI study: Follow-Up of Jevtana in real life
 Pharmacologie médicale Bordeaux PharmacoEpi CIC Bordeaux CIC1401 FUJI study: Follow-Up of Jevtana in real life French retrospective and protective multicenter observational study describing the survival,
Pharmacologie médicale Bordeaux PharmacoEpi CIC Bordeaux CIC1401 FUJI study: Follow-Up of Jevtana in real life French retrospective and protective multicenter observational study describing the survival,
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Present and Future Perspectives in Treatment of mcrpc Patients
 Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
mcrpc in 2016 How to decide the optimal treatment? N. Mottet
 mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
mcrpc in 2016 How to decide the optimal treatment? N. Mottet Disclosures Conflict of interest Chairman EAU PCa guidelines..... Therefore I'm 100% biased Castrate-resistant prostate cancer (CRPC) Definition
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center