Disclosures for Ayalew Tefferi
|
|
|
- Duane Watson
- 5 years ago
- Views:
Transcription
1 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte None None None None None Presentation includes discussion of the following off-label use of a drug or medical device: Hydroxyurea, Interferon-alpha, Busulfan, Thalidomide, Lenalidomide, Pomalidomide, Ruxolitinib, Androgen preparations, Erythropoiesis stimulating agents
2 Myeloproliferative neoplasms other than PV, ET and PMF: CMML: chronic myelomonocytic leukemia Mastocytosis Eosinophilic disorders CNL: chronic neutrophilic leukemia Ayalew Tefferi, MD Professor of Medicine and Hematology Mayo Clinic College of Medicine 2015 MFMER slide-2
3 Objectives Disease definitions Diagnosis Current prognostication Treatment
4 2016 WHO Classification of Myeloid Malignancies Acute Myeloid Leukemia (AML) Myelodysplastic Syndromes (MDS) Myeloproliferative Neoplasms (MPN) MDS/MPN overlap Myeloid/Lymphoid neoplasms with eosinophilia and PDGFR/FGFR1/ PCM1-JAK2 mutation CMML Molecularly-defined eosinophilia Chronic Myeloid Leukemia (CML) BCR-ABL1 100% mutated Chronic Neutrophilic Leukemia (CNL) CSF3R % mutated Chronic Eosinophilic Leukemia Not Otherwise Specified (CEL-NOS) Polycythemia vera (PV) Essential Thrombocythemia (ET) Primary Myelofibrosis (PMF) MPN Unclassifiable (MPN-U) CNL Vs. HES The JAK2/CALR/MPL mutated MPNs 97% JAK2 V617F 3% other JAK2 mutations 60% JAK2 mutated 22% CALR mutated 3% MPL mutated 15% triple-negative Mastocytosis no longer under the WHO MPN category 60% JAK2 mutated 23% CALR mutated 7% MPL mutated 10% triple-negative
5 Acquired eosinophilia Secondary Primary Drugs Infections Parasites Allergy Inflammations Kimura s CSS Well s Neoplasia Hodgkins NHL Solid tumor Clonal Cytogenetic, molecular or bone marrow morphologic evidence of an otherwise defined myeloid malignancy -PDGFRA/PDGFRB mutated (imatinib sensitive) -FGFR1 rearranged (urgent transplant) -PCM1-JAK2 (ruxolitinib) -Abnormal karyotype, non-specific (CEL-NOS) -Excess blasts (CEL-NOS) -AML/ALL/CML/MDS/CMML/SM/unclassifiable Idiopathic Neither reactive nor clonal HES if AEC > 1500/micL x 6 months and organ damage 20% of HES pts may display a T cell clone/abnormal phenotype (lymphocytic variant hyper-eosinophilia)
6 Primary eosinophilia diagnostic algorithm 1st step Peripheral blood screening for FIP1L1-PDGFRA using FISH or RT-PCR Mutation present PDGFRA mutated clonal eosinophilia (Imatinib 100 mg/day) PDGFRB mutated clonal eosinophilia (Imatinib 100 mg/day) 2nd step Bone marrow biopsy with cytogenetics 8p11 translocation present FGFR1 mutated clonal eosinophilia (Hyper-CVAD + Allo-transplant) CEL-NOS (Allo-transplant) 3rd step Peripheral blood lymphocyte phenotyping and TCR gene rearrangement studies Abnormal or clonal lymphocytes present lymphocytic variant hypereosinophilia (Treat like HES) Mayo Clin Proc 85:158, 2010 All the above negative Idiopathic eosinophilia including HES
7 Hyper-eosinophilic syndrome/idiopathic eosinophilia 98 Mayo Clinic patients with WHO-defined HES/IH (Leukemia 2016;30:1924) NGS revealed 11% harbored pathogenic mutation; TET2=3, ASXL1 =2, KIT=2, and IDH2, JAK2, SF3B1 and TP53=1 each. 15% harbored a variant of unknown significance (VUS); TET2=8, ASXL1=2, SETBP1=2, and CALR, CEBPA and CSF3R=1 each. NO DIFFERENCE IN MUTATED VS NON-MUTATED IN PHENOTYPE MUTATED PATIENTS HAD INFERIOR SURVIVAL IN UNIVARIATE ANALYSIS Risk factors for survival: Low risk: 0-1 risk points N=60 5-year survival 98% Hepatosplenomegaly (3 points) Advanced age (2 points) Hgb <10 g/dl (one point) Cardiac involvement (one point) High risk: 2 or more risk points N=38 5-year survival 62%
8 HES treatment algorithm Urgent treatment needed Treatment not urgent Do you even need to treat? -Asymptomatic AEC <50 x 10 9 /l -Serum troponin normal -Echocardiogram normal HES Prednisone 1-2 mg/kg/day with taper T clone present CSA MTX Cytoxan Low-dose prednisone (10 mg/day or less) Low-dose prednisone + hydroxyurea Low-dose prednisone + pegasys Imatinib 400 mg/day trial x 1 month Mepolizumab (Nucala ; biweekly injections) Benralizumab (Fasenra ; monthly injections) Midostaurin 100 mg BID

9 Novel targeted therapies for eosinophilic disorders Anti-IL-5 Mepolizumab Reslizumab Anti-IL-5Rα Benralizumab Eotaxin receptor LMW CCR3 inhibitors Eosinophil inhibitory receptor Anti-Siglec-8 Ab Anti-CD52 Alemtuzumab Anti-IgE Omalizumab Multi-targeted TKI Midostaurin Prostaglandin D 2 receptor LMW CRTH2 inhibitors Wechsler et al. J Allergy Clin Immunol Sep;130(3):

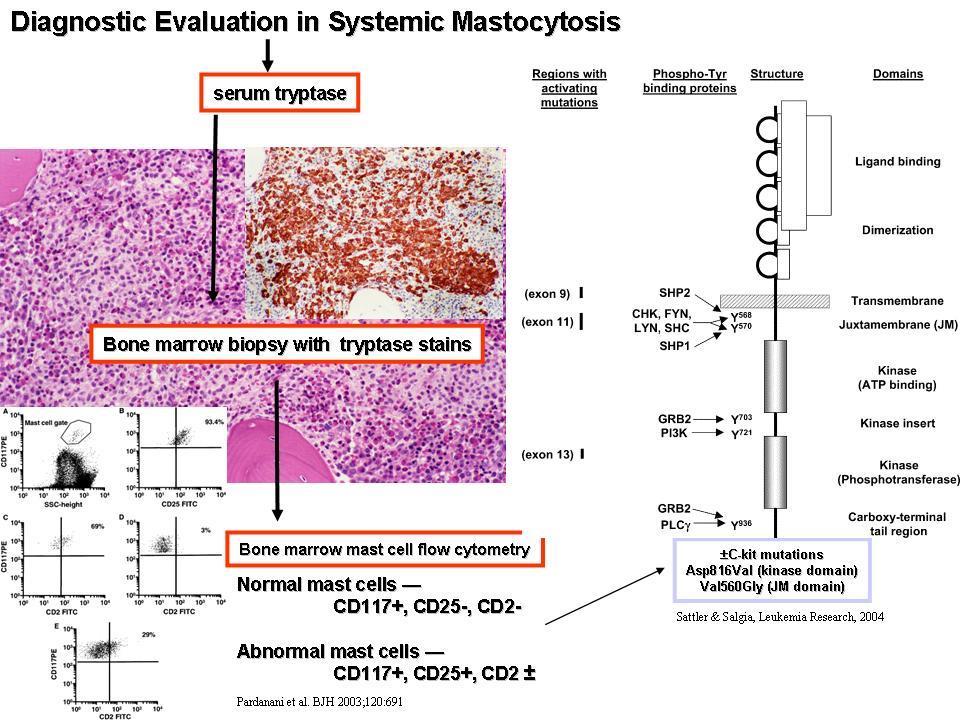
10 When should you suspect mastocytosis? Urticaria pigmentosa Mast cell mediator symptoms -Anaphylactoid -Diarrhea -Flushing/urticaria Osteopenia/unexplained fractures
11
 i Indolent SM ii Aggressive SM (cytopenia, bone disease, organomegaly, etc.) Medicine 1988;67:345 Leukemia Research 2001;25:603 1.")
12 Practical classification of mast cell disease 1 Cutaneous mastocytosis (skin-only disease) Both can manifest mast cell mediator release symptoms Hartmann. & Henz, Br J Derm 2001;144:682 2 Systemic mastocytosis (SM) i Indolent SM ii Aggressive SM (cytopenia, bone disease, organomegaly, etc.) Medicine 1988;67:345 Leukemia Research 2001;25: SM without associated 2 nd myeloid neoplasm 2. SM with associated 2 nd myeloid neoplasm 3. Mast cell leukemia
13 Survival for 342 systemic mastocytosis patients classified by disease type compared with the expected age and gender matched US Population s survival Expected US Survival compared to WHO classification Survival ISM, (n=159) ASM, (n=41) AHD, (n=138) MCL, (n=4) Expected US Survival Blood 2009;113:5727. Years from Dx 01Oct08
14 Mutation-augmented prognostic scoring system (MAPSS) in 94 patients with advanced mastocytosis ISM (n=44) KIT 73% TET2 7% No other mutations ASM (n=25) KIT 84% TET2 20% ASXL1 16% AHN (n=80) KIT 75% TET2 45% ASXL1 26% CBL 19% JAK2 DNMT3A U2AF1 RUNX1 SF3B1 Others One risk factor other than platelet count 2-3 risk factors or low platelet count 4 or more risk factors or low platelet count Risk factors: Platelet count <150 albumin <3.5 age >60 ASXL1/CBL mutated Hgb <10 AJH 2016;91:888 BJH 2016;175:531
15 Treatment for Systemic mastocytosis Indolent Aggressive Associated with MDS or CMML Mast cell leukemia H1 and H2 blockers Cromolyn Phototherapy Topical steroids If this fails, OK to try IFN-α or cladribine Cladribine 5 mg/m2 x 5 days; monthly x 4 (first choice) Midostaurine 100 mg BID (second choice) Avapritinib (BLU-285) 300 mg once-daily 32 treated OR 72% at 9 months 56% CR/PR Edema, fatigue, GI toxicity 50% grade 3 AEs Treat as MDS or CMML Midostaurine or Avapritinib or Cladribine or AML-like therapy followed by Transplant? J Clin Oncol ;32:3264
16 Phase-2 study of midostaurin 10-year follow-up (N=26; responders = 18 (69%; major response 50%) SM-AHN = 17 (13 responders); ASM = 3 (1 responder), MCL = 6 (4 responders) Median OS 40 months 92% treatment discontinuation rate at median 5 months of treatment Nauseas 88% Vomiting 69% Diarrhea 27% Fatigue 35% Headache 31% Edema 35% Bonus effects: -Complete resolution of eosinophilia in 7 of 7 evaluable patients -Improvement in monocytosis in all 14 patients with baseline increase -Major response -Major response -Major response Leukemia 2018
17 Allogeneic hematopoietic stem-cell transplantation (allohct or HCT) outcomes in 57 patients with advanced systemic mastocytosis (SM): 38 SM-AHNMD; 12 MCL and 7 aggressive SM. JCO 2014;32:3264
 Hereditary neutrophilia")
18 CSF3R mutations Chromosome 1p exons 813 amino acids Extracellular domain D771fs S783fs Y752X W791X Membrane proximal T615A CNL (exon 14) Hereditary neutrophilia (exon 16) Cytoplasmic domain Kosmider et al. Leukemia Acquired mutations in severe congenital neutropenia
19 WHO diagnostic criteria for CNL 1. Leukocytosis > 25 x 10 9 /L Neutrophils plus bands >80% Neutrophil precursors < 10% Myeloblasts rarely observed No dysgranulopoiesis 2. Hypercellular bone marrow Neutrophil granulocytes increased Neutrophil maturation normal Myeloblasts < 5% 3. Not meeting WHO criteria for BCR-ABL1+ CML, PMF, PV or ET WHO diagnostic criteria for acml Leukocytosis with >10% precursors Dysgranulopoiesis Basophils <2% Monocytes <10% Hypercellular bone marrow with dysgranulopoiesis <20% blasts in the blood and bone marrow No PDGFRA/PDGFRB/FGFR1/PCM1-JAK2 4. No PDGFRA/PDGFRB/FGFR1/PCM1-JAK2 5. CSF3RT618I or other activating CSF3R mutation Not meeting WHO criteria for BCR-ABL1+ CML, PMF, PV or ET or no identifiable cause of reactive neutrophilia
20 Risk-stratified Kaplan Meier survival curves for 19 CSF3R-mutated CNL patients. Treatment: High-risk: ASCT Low risk: Hydroxyurea (first) Ruxolitinib (second) Transient response Risk points: platelet count < /L (2 points); leukocyte count > /L (1 point); ASXL1 mutation (1 point)

21 CMML 2016 WHO Diagnostic Criteria AMC >1 x 10(9) /L and monocytes >10% Dysplasia in one or more myeloid lineages Not meeting WHO criteria for CML, PV, ET or MF No PDGFRA/PDGFRB/FGFR1/PCM1-JAK2 <20% blasts in the blood and BM Blood 2016 In the absence of dysplasia, a diagnosis of CMML can still be made if: -An acquired clonal cytogenetic or molecular genetic abnormality can be documented. these include ASXL1, TET2, SRSF2 and SETBP1 mutations -Monocytosis has persisted for >3 months -Other causes of reactive monocytosis have been ruled out
22 Differential diagnosis of Monocytosis Reactive 1. Viral infections. 2. Recovering bone marrow. 3. Connective tissue disorders. 4. Sarcoidosis 5. Tuberculosis, Brucellosis, Leishmaniasis. 6. SABE. Clonal 1. CMML 2. JMML 3. AML with monocytic differentiation. 4. MDS/MPN overlap syndromesunclassifiable. BJH 2014





23 CMML- Peripheral Blood and Bone Marrow Findings Peripheral Blood Smear Bone Marrow Aspirate Core Biopsy Dual Esterase Stain
24 WHO CMML Subcategories CMML-0 Blasts + promonocytes <2% in PB. Blasts + promonocytes <5% in BM. CMML-1 Blasts + promonocytes 2-4% in PB. Blasts + promonocytes 5-9% in BM CMML-2 Blasts + promonocytes 5-19% in PB. Blasts + promonocytes 10-19% in BM. Presence of Auer rods, irrespective of blast count. Blood 2016

25 Survival Proliferative vs Dysplastic CMML Survival data for 435 patients with WHO defined chronic myelomonocytic leukemia stratified by Proliferative versus Dysplastic sub-types. 1 CMML patients with dysplastic phenotype, n=226, median survival ~30 months..8.6 CMML patients with proliferative phenotype, n=209, median survival ~19 months Months Figure 2: Heat map of an unsupervised differential gene expression profile in peripheral blood CMML samples, demonstrating two predominantly unique clusters, segregating dysplastic (cluster 1) from proliferative (cluster 2) CMML subtypes. ASH 2016
, EZH2 Spliceosome components SRSF2 (~45%), SF3B1, U2AF1, ZRSR2 Transcription factors")
, PHF6, BCOR, Tp53 > 90% CMML patients have 1 somatic mutations Leukemia 2014 B Cancer")
26 CMML Genomics Epigenetic regulators TET2 (~60%), IDH1, IDH2, DNMT3A Chromatin modeling ASXL1 (~40%), EZH2 Spliceosome components SRSF2 (~45%), SF3B1, U2AF1, ZRSR2 Transcription factors RUNX1 (~15%) Signal pathways JAK2, KRAS, NRAS, CBL, PTPN11 (RAS pathway ~30%) Others SETBP1 (~15%), PHF6, BCOR, Tp53 > 90% CMML patients have 1 somatic mutations Leukemia 2014 B Cancer Journal 2015
27 Cytogenetic abnormalities in CMML Cytogenetic abnormalities seen in 20-40% of cases Most common are +8, chromosome 7 abnormalities and 12p deletions Spanish Cytogenetic Risk Stratification. Low: Normal, -Y Intermediate: all others High: +8, chromosome 7 abnormalities and complex changes 5 year OS- 35%, 26% and 4%. Haematologica 2011 AJH 2013
28 CMML Prognostic Models Variables Mayo Model Molecular Mayo Model GFM Model CPSS- Molecular HB < 10 gm/dl Red blood cell transfusion dependance High WBC + (>15) + (>13) AMC > Platelets < Circulating IMC + + BM blasts + (>5%) Age >65 + Cytogenetic risk groups Molecular genetics Blood 2002; Blood 2012; JCO 2013; Leukemia 2013; Leukemia 2014; Blood 2016 ASXL1 ASXL1 ASXL1/ NRAS/ RUNX1 and SETBP1 +
29 Survival Survival Survival data for 420 patients with CMML stratified by the Molecular Mayo Model. Survival data for 420 patients with CMML stratified by the GFM Model. 1 MMM low risk patients, n= 64, median survival 97 months. 1 GFM low risk patients, n= 188, median survival 65 months..8 MMM intermediate-1 risk patients, n= 128, median survival 59 months. MMM intermediate-2 risk patients, n= 118, median survival 31 months..8 GFM intermediate risk patients, n= 154, median survival 28 months. GFM high risk patients, n= 78, median survival 17 months..6 MMM high risk patients, n= 110, median survival 16 months..6.4 P=< P=< Months Months Leukemia 2014
30 CMML Therapeutics Supportive care Transfusions Hydroxyurea ESA Iron chelation therapy Directed Therapies Hypomethylating agents Allogeneic SCT Clinical trials
31 Hypomethylating (HMA) Agents in CMML Study N Median Age (years) Phase Drug used Response rates (%). Median survival (months) Wijermans 2008 Costa 2011 Braun 2011 Thorpe 2012 Ades 2013 Wong 2013 Fianchi II Decitabine CR-10 PR-16 HI II Azacitidine CR-11 PR- 3 HI II Decitabine CR-10 PR-20 HI II Azacitidine CR-20 HI II Azacitidine CR-17 PR-1 HI II Azacitidine CR-9 PR-9 HI II Azacitidine CR-45 PR-3 HI NR BJH 2014
32 Role for Allogeneic SCT in CMML Study N Age median (range) Donor Source Conditioning regimen Relapse rate and TRM Outcome OS & DFS Kroger (19-61) MRD-43 MUD-7 MAC- 50 RR-28% TRM-52% 5 yr DFS-18% 5 yr OS-21% Symeonidis MRD-160 MUD-85 MAC-152 RIC-87 RR-25% TRM-37% 5 yr DFS-38% 5 yr OS-42% Eissa (21-66) MRD-38 MUD-47 MAC- 58 RIC- 27 RR-27% TRM-35% 10 yr DFS-40% 10 yr OS-40% Park (27-66) MRD-41 MUD-32 MAC- 30 RIC- 43 RR-35% 3 yr DFS-29% 3 yr OS-32% BJH 2014
33 Novel Agents- Clinical Trials. MEK inhibitors. Hedgehog pathway inhibitors. GM-CSF monoclonal antibody (KB003). Neddylation inhibitors. MAP kinase inhibitor. P38/Tie-2 inhibitor. Aminopeptidase inhibitors.
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Angela Fleischman
 Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Presenter Disclosure Information
 Welcome to Master Class for Oncologists Session 3: 2: PM 3:3 PM Pasadena, CA May 1, 21 Myeloproliferative Neoplasms 21 Speaker: Ayalew Tefferi Mayo Clinic, Rochester, MN Presenter Disclosure Information
Welcome to Master Class for Oncologists Session 3: 2: PM 3:3 PM Pasadena, CA May 1, 21 Myeloproliferative Neoplasms 21 Speaker: Ayalew Tefferi Mayo Clinic, Rochester, MN Presenter Disclosure Information
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Pathogenesis and management of CMML
 Pathogenesis and management of CMML Raphaël Itzykson, Hôpital Saint-Louis, Paris International Conference of the Korean Society of Hematology March 29th 2018 대한혈액학회 Korean Society of Hematology COI disclosure
Pathogenesis and management of CMML Raphaël Itzykson, Hôpital Saint-Louis, Paris International Conference of the Korean Society of Hematology March 29th 2018 대한혈액학회 Korean Society of Hematology COI disclosure
Hypereosinophili c syndrome
 Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
ASBMT MDS/MPN Update Sunil Abhyankar, MD
 ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
9/25/2017. Disclosure. I have nothing to disclose. Young S. Kim MD Dept. of Pathology
 Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Fortgeschrittene systemische Mastozytose Hintergrundinformationen zu einer seltenen Erkrankung und zur ersten zugelassenen Therapie
 Fortgeschrittene systemische Mastozytose Hintergrundinformationen zu einer seltenen Erkrankung und zur ersten zugelassenen Therapie Georgia Metzgeroth Hämatologie und Onkologie III. Medizinische Klinik
Fortgeschrittene systemische Mastozytose Hintergrundinformationen zu einer seltenen Erkrankung und zur ersten zugelassenen Therapie Georgia Metzgeroth Hämatologie und Onkologie III. Medizinische Klinik
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms
 Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Session 4: Summary and Conclusions
 Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome
 RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated
 Updated") Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Disclosures. I do not have anything to disclose. Shared Features of MPNs. Overview. Diagnosis and Molecular Monitoring in the
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
MDS/MPN: What it is and How it Should be Treated?
 MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
JAK inhibitors in Phmyeloproliferative
 Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Supervisor: Prof. Dr. P Vandenberghe Dr. C Brusselmans
 Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Introduction of an NGS gene panel into the Haemato-Oncology MPN service
 Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
The Evolving Role of Transplantation for MPN
 The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
What are myeloproliferative neoplasms??
 Welcome to Master Class for Oncologists Session 3: 2:45 PM - 3:30 PM New York, NY October 24, 2008 Myeloproliferative Neoplasms Speaker: Ayalew Tefferi, MD Professor of Medicine, Mayo Clinic, Rochester,
Welcome to Master Class for Oncologists Session 3: 2:45 PM - 3:30 PM New York, NY October 24, 2008 Myeloproliferative Neoplasms Speaker: Ayalew Tefferi, MD Professor of Medicine, Mayo Clinic, Rochester,
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later
 Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
Should Intermediate-I risk PMF be transplanted immediately or later? Position: Later Vikas Gupta, MD, FRCP, FRCPath Associate Professor Department of Medicine Leukemia/BMT Programs Princess Margaret Cancer
SUPPLEMENTARY INFORMATION
 Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!!
 Guide Therapy..YES!!!") Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!! Lindsay Anne Magura Rein, MD Division of Hematologic Malignancies and Cellular Therapy/BMT A Little Bit of History.. 1665 Advanced
Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!! Lindsay Anne Magura Rein, MD Division of Hematologic Malignancies and Cellular Therapy/BMT A Little Bit of History.. 1665 Advanced
Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models
 REGULAR ARTICLE Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models Animesh Pardanani, 1 Sahrish Shah, 1 Francesco Mannelli, 2 Yoseph C. Elala, 1 Paola Guglielmelli,
REGULAR ARTICLE Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models Animesh Pardanani, 1 Sahrish Shah, 1 Francesco Mannelli, 2 Yoseph C. Elala, 1 Paola Guglielmelli,
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update
 Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
MDS/MPN MPN MDS. Discolosures. Advances in the Diagnosis of Myeloproliferative Neoplasms. Myeloproliferative neoplasms
 Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms
 Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms Version: MPNBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is NOT required for accreditation
Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms Version: MPNBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is NOT required for accreditation
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
MPL W515L K mutation
 MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
Chronic myelomonocytic leukemia. Lymphoma Tumor Board. May 26, 2017
 Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Winship Cancer Institute of Emory University New Determinants and Approaches for MPN
 Winship Cancer Institute of Emory University New Determinants and Approaches for MPN Elliott F. Winton August 8, 2014 Sea Island, Georgia Outline: MPN Determinants, Approaches Diagnosis Prognosis Treatment
Winship Cancer Institute of Emory University New Determinants and Approaches for MPN Elliott F. Winton August 8, 2014 Sea Island, Georgia Outline: MPN Determinants, Approaches Diagnosis Prognosis Treatment
ASBMT MDS/MPN UPDATE
 ASBMT MDS/MPN UPDATE Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN UPDATE Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Let s Look at Our Blood
 Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation
 Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Laboratory Service Report
 Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-ih2xuglwpq.ashx Indication for Test DS CR Pathogenic utations Detected CR 1. JAK2: c.1849g>t;p.val617phe
Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-ih2xuglwpq.ashx Indication for Test DS CR Pathogenic utations Detected CR 1. JAK2: c.1849g>t;p.val617phe
Myelodysplastic Syndromes. Post-ASH meeting 2014 Marie-Christiane Vekemans
 Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CME Information: Chronic Myelomonocytic Leukemia: 2016 Update on Diagnosis, Risk Stratification and Management
 CME ARTICLE AJH CME Information: Chronic Myelomonocytic Leukemia: 2016 Update on Diagnosis, Risk Stratification and Management CME Editor: Ayalew Tefferi, M.D. Author: Mrinal Patnaik, M.D. If you wish
CME ARTICLE AJH CME Information: Chronic Myelomonocytic Leukemia: 2016 Update on Diagnosis, Risk Stratification and Management CME Editor: Ayalew Tefferi, M.D. Author: Mrinal Patnaik, M.D. If you wish
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
Intro alla patologia. Giovanni Barosi. Fondazione IRCCS Policlinico San Matteo Pavia
 Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
ASH 2013 Analyst & Investor Event
 ASH 2013 Analyst & Investor Event December 9, 2013 John A. Scarlett, MD President & CEO Forward-Looking Statements Except for the historical information contained herein, this presentation contains forward-looking
ASH 2013 Analyst & Investor Event December 9, 2013 John A. Scarlett, MD President & CEO Forward-Looking Statements Except for the historical information contained herein, this presentation contains forward-looking
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology
 Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia
 Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
WHO 2016/17 update on Myeloproliferative Neoplasms. Anna Ruskova Auckland City Hospital New Zealand
 WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE?
 NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and management
 Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias
 Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
JAK2 V617F analysis. Indication: monitoring of therapy
 JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
Case #1. 65 yo man with no prior history presented with leukocytosis and circulating blasts: Bone marrow biopsy was performed
 Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Guidelines for the diagnosis and treatment of Myelodysplastic Syndrome and Chronic Myelomonocytic Leukemia. Nordic MDS Group
 Guidelines for the diagnosis and treatment of Myelodysplastic Syndrome and Chronic Myelomonocytic Leukemia Nordic MDS Group 8th update, May 2017 1 WRITING COMMITTEE... 4 CONTACT INFORMATION... 4 EVIDENCE
Guidelines for the diagnosis and treatment of Myelodysplastic Syndrome and Chronic Myelomonocytic Leukemia Nordic MDS Group 8th update, May 2017 1 WRITING COMMITTEE... 4 CONTACT INFORMATION... 4 EVIDENCE
Supplemental Material. The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia
 Supplemental Material The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia Torsten Haferlach, 1 Anna Stengel, 1 Sandra Eckstein, 1 Karolína
Supplemental Material The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia Torsten Haferlach, 1 Anna Stengel, 1 Sandra Eckstein, 1 Karolína
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
JAK2 Inhibitors for Myeloproliferative Diseases
 JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Myelodysplastic syndromes Impact of Biology. Lionel Adès Hopital Saint Louis Groupe Francophone des SMD. Épidémiologie
 Myelodysplastic syndromes Impact of Biology Lionel Adès Hopital Saint Louis Groupe Francophone des SMD Épidémiologie Incidence : 3 à 6 / 100 000 hab. / An Prédomine chez les sujets âgés Augmentation de
Myelodysplastic syndromes Impact of Biology Lionel Adès Hopital Saint Louis Groupe Francophone des SMD Épidémiologie Incidence : 3 à 6 / 100 000 hab. / An Prédomine chez les sujets âgés Augmentation de
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs
 MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Out-Patient Billing CPT Codes
 Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Chronic Neutrophilic Leukaemia (CNL)
") Chronic Neutrophilic Leukaemia (CNL) A Guide for Patients Introduction Being diagnosed with chronic neutrophilic leukaemia (CNL) can be a shock, particularly when you may never have heard of it. If you
Chronic Neutrophilic Leukaemia (CNL) A Guide for Patients Introduction Being diagnosed with chronic neutrophilic leukaemia (CNL) can be a shock, particularly when you may never have heard of it. If you