Case Report Clonal Hypereosinophilia with ETV6 Rearrangement Evolving to T-Cell Lymphoblastic Lymphoma: A Case Report and Review of the Literature
|
|
|
- Grant Craig
- 5 years ago
- Views:
Transcription
1 Case Reports in Hematology Volume 2013, Article ID , 4 pages Case Report Clonal Hypereosinophilia with ETV6 Rearrangement Evolving to T-Cell Lymphoblastic Lymphoma: A Case Report and Review of the Literature Filipa Moita, Isabel Bogalho, Helena Alaiz, Joana Parreira, Maria Jesus Frade, Albertina Nunes, and Maria Gomes da Silva Hematology Department, Instituto Português de Oncologia de Lisboa, Francisco Gentil, Rua Professor Lima Basto, Lisbon, Portugal Correspondence should be addressed to Filipa Moita; filipamoita@gmail.com Received 12 March 2013; Accepted 3 April 2013 Academic Editors: E. Arellano-Rodrigo, M.-C. Kyrtsonis, A. Ohsaka, and S. D. Wagner Copyright 2013 Filipa Moita et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Hypereosinophilia, either clonal or reactive, has been described in association with multiple hematological malignancies. We describe a case of a patient presenting with hypereosinophilia that evolved into T-cell lymphoblastic lymphoma. Complete remission was achieved with chemotherapy; however, hypereosinophilia recurred 5 months later in association with myeloblastic bone marrow infiltration and without evidence of lymphoblastic lymphoma relapse. Cytogenetic analysis of the bone marrow showed a complex translocation involving chromosomes 7, 12, and 16. A rearrangement of ETV6 gene (12p13) was demonstrated by FISH studies, thus confirming the clonality of this population. The association of lymphoblastic lymphoma, eosinophilia, and myeloid hyperplasia has been described in disorders with FGFR1 rearrangements. We hypothesize that other clonal eosinophilic disorders lacking this rearrangement could behave in a similar fashion through different pathogenic mechanisms. 1. Background Hypereosinophilia (HE) can be associated with a wide range of both reactive and malignant disorders. In hematologic malignancies, HE may appear in disorders where the eosinophils are a part of the malignant clone, such as the myeloproliferative neoplasms, or result from stimulation by growth factors or cytokines produced by the malignant clone. These include lymphoproliferative neoplasms, particularly T-cell non-hodgkin lymphoma, and Hodgkin lymphoma. Eosinophilia has also been described in association with acute lymphoblastic leukemia, more frequently of B-cell origin [1, 2]. Its appearance sometimes precedes the diagnosis of malignancy by several years [3], and thus, after the exclusion of reactive causes, the presence of eosinophilia should lead to the investigation of an underlying clonal disease. 2. Case Report We report the case of a 58-year-old female, with a known history of multiple sclerosis that was at the time asymptomatic and under no specific therapy. She was otherwise healthy, not taking any medication. Her family history was unremarkable. The patient was referred to the hematology department with the diagnosis of T-cell lymphoblastic lymphoma. She had been observed in her local hospital two months earlier, after the incidental discovery of leukocytosis with eosinophilia,bicytopenia,andelevatedlactatedehydrogenase (LDH) (Table 1). At the time, a bone marrow aspirate was performed and revealed a hypercellular bone marrow (BM) with marked hypereosinophilia, no increase in the number of blasts, and no specific morphologic alterations. Immunophenotyping and cytogenetic studies were not conducted at this point. The patient was kept under observation and remained asymptomatic, with spontaneous normalization of the hematological parameters and LDH. Two months later a cervical enlarged lymph node appeared. The excisional biopsy showed lymphoblastic lymphoma of T-cell lineage, andshewasreferredtoourhospitalforfurthermanagement. At admission, the patient presented with fatigue but was otherwise asymptomatic. Specifically, she denied respiratory, gastrointestinal, or other symptoms suggestive of a reactive
 (diagnosis of ALL) (after induction) (D16 SNC prophylaxis) 12th July 2012 WBC (/mm 3 ) 97.700 11.350 3.650 37.900 159.")
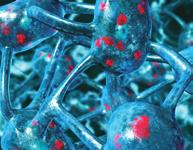
2 2 Case Reports in Hematology Table 1: Laboratory data. December 2011 February 2012 March th July 2012 (local hospital) (diagnosis of ALL) (after induction) (D16 SNC prophylaxis) 12th July 2012 WBC (/mm 3 ) (8% myeloblasts) (19% myeloblasts) Neutrophils (/mm 3 ) Eosinophils (/mm 3 ) Hb (g/dl) Platelets (/mm 3 ) LDH (UI/L) WBC: white blood cell; Hb: hemoglobin; LDH: lactate dehydrogenase. eosinophilia. She was not a smoker and had no history of allergies. Physical examination revealed enlarged bilateral cervical, supraclavicular, and axillary lymph nodes and an enlarged spleen. Laboratory abnormalities included anemia, a slight leukocytosis with eosinophilia, and a normal LDH (Table 1). The cervical lymph node biopsy was reviewed, and the diagnosis of T-cell lymphoblastic lymphoma was confirmed. A fine needle aspirate was conducted and flow cytometry studies showed infiltration by 92% aberrant immature T-cells that were Tdt/CD99/cCD3/CD5/CD2/CD1a/CD4 positive. The fluorescent in situ hybridization (FISH) analysis for BCR- ABLgenefusioninthelymphnodeaspiratewasnegative. The BM aspirate revealed a normocellular BM with 45.8% eosinophils, relative granulocytic hyperplasia, and no lymphoblastic or myeloblastic infiltration. No dysplastic changeswerefound.flowcytometricanalysisdidnotidentify an aberrant lymphoid or myeloid population; 0.3% CD34+ precursors were present. BM biopsy findings were interpreted as reactive. The investigation of PDGFRA rearrangements by FISH andpolymerasechainreaction(pcr)inthebonemarrow wasnegativeatthistimepoint.cytogeneticstudiesshowed a normal karyotype in the 20 metaphases analyzed. As part of the lymphoma staging procedures, a computed tomography (CT) scan was performed showing multiple enlarged lymph nodes (cervical, supraclavicular, axillary, mediastinal, abdominal, iliopelvic, and inguinal) as well as splenomegaly. The PET scan revealed some adenopathies with an increased metabolism. Neoplastic cells were not found in the spinal tap. Treatment was started according to the CALGB 9111 protocol for lymphoblastic lymphoma/leukemia [4], with complete remission documented after induction. The patient proceeded with the early intensifications, according to schedule, without significant toxicities, except for an allergic reaction to thee.coli asparaginase requiring a switch to Erwinase. Central nervous system prophylaxis was performed with high dose methotrexate (MTX), and radiotherapy was not administeredduetotheknownhistoryofmultiplesclerosis. Sixteen days after MTX administration, the patient was admitted with fever without an obvious infectious cause. A progressive increase in the leukocytosis, with neutrophilia, eosinophilia (Table 1), monocytosis, and the appearance Figure 1: Bone marrow aspirate at relapse showing infiltration by myeloblasts, left shifted granulopoiesis, and marked hypereosinophilia. of immature myeloid precursors in the peripheral blood (myeloblasts 8%, promyelocytes 3%, myelocytes 3%, and metamyelocytes 4%) followed, as well as a raise in LDH levels. This picture resembled the alterations that occurred two months prior to diagnosis. At this time, a repeated BM aspirate showed a hypercellular marrow, with myeloid hyperplasia, and infiltration by 11% of myeloblasts (Figure 1). This finding was confirmed by flow cytometry that identified 10% myeloblasts expressing CD34, CD117, HLA-DR, CD33, and CD13. Prominent eosinophilia was also present, and phenotypic aberrations in the granulocytic maturation were evident. There was no evidence of lymphoblastic infiltration either in morphology or in flow cytometry. Conventional cytogenetic analysis showed 10 metaphases with t(7;12)(q22;p13) as well as the addition of unknown genetic material to the short arm of chromosome 16 (Figure 2(a)). FISH studies using a dual color break-apart probe were positive for the ETV6 (12p13) rearrangement (Figure 2(b)). To further characterize these alterations, whole chromosome painting of chromosomes 7 and 12 was conducted (Figure 2(c)) and revealed a complex pattern of rearrangements involving chromosomes 7, 12, and 16: 46, XX,del(7)(q22),der(12)t(7;12)(q22;p13)t(12;16)(p13;p13), der(16)t(12;16). The BM samples were also retested for PDGFRA, PDGFRB, and BCR-ABL rearrangements by FISH, with repeated negative results.
 (c) whole chromosome painting of chromosomes 7 (red) and 12 (green) showing 46,XX,")


3 Case Reports in Hematology 3 (a) (b) (c) Figure 2: Cytogenetics of the patient s bone marrow (a) G-banded karyotype showing 46,XX,t(7;12)(q22;p13),add(16)(p13); (b) fluorescence in situ hybridization using a dual-color break-apart probe showing rearrangement of ETV6 (12p13) (c) whole chromosome painting of chromosomes 7 (red) and 12 (green) showing 46,XX, del(7)(q22),der(12)t(7;12)(q22;p13)t(12;16)(p13;p13);der(16)t(12;16). A PET scan was repeated at this time point and showed only splenic caption (SUV 4.55). An abdominal ultrasound showed a heterogeneous splenomegaly without nodular lesions, suggesting a spleen infiltrative process. Despite the introduction of high dose of steroid therapy, there was a progressive increase of leukocytosis with 19% circulating myeloblasts, thrombocytopenia, and anemia, possibly reflecting progression to acute myeloid leukemia, although this finding was not confirmed by bone marrow evaluation. Cytoreduction with hydroxyurea was attempted with a slow but steady decrease in the leukocyte counts. Eight days later, the patient developed sudden dyspnea with severe respiratory failure. Bilateral pulmonary infiltrates present on chest X-ray and high resolution pulmonary CT scan raised the hypothesis of an infectious process. In spite of antimicrobial therapy, the patient progressed to acute respiratory distress syndrome requiring invasive mechanical ventilation and eventually died in the ICU, about 4 weeks after the febrile episode and 6 months after the diagnosis of lymphoblastic lymphoma. Autopsy was not conducted, so the exact cause of death (infection/disease progression) was not determined. 3. Discussion The association between acute lymphoblastic leukemia (ALL) and eosinophilia was first described by Spitzer and Garson in 1973 [2]. The most common cytogenetic abnormality associated with this presentation is t(5;14)(q31;q32) resulting in an overproduction of IL-3; this entity has been recently recognized as a distinct subtype among B-cell ALL in the 2008 WHO classification [1]. However, t(5;14)(q31;q32) translocation is only present in about 10% of cases of ALL with eosinophilia [5], and several case reports with the same clinical phenotype but lacking the rearrangement have been described [6 9]. The association between lymphoblastic lymphoma (LBL) and eosinophilia appears to be less common. However, the concomitant presence of T-LBL, eosinophilia, and myeloid hyperplasia is known to occur in patients carrying the t(8;13)(p11;q11) translocation [10]. This distinct pathological entity is characterized by the rearrangement of the fibroblast growth factor receptor 1 (FGFR1) gene located at chromosome 8p11 [11]. Other rearrangements may be associated with eosinophilia. Recent reports of ALL with this presentation have implicated chromosomes 7 and 12, namely-7, add(12)(p13) [7] and del(7)(q22) [8]. Recently Bhatti et al. [6] described a patient with B-cell lymphoblastic leukemia/lymphoma and severe eosinophilia and splenomegaly carrying a chromosomal translocation t(7;12)(q22;p13). The karyotype analysis in the current case demonstrated a similar rearrangement. Additionally, the presence of a rearrangement involving the ETV6 gene was demonstrated by FISH. The ETV6 gene, located at 12p13, belongs to a large family of transcription factors and has been previously implicated in thepathogenesisofmultiplehematologicalmalignancies[12], occasionally related with eosinophilia [13]. Many translocation partners to ETV6 have been characterized at the molecular level, with the identification of 30 ETV6 partner genes [12]. In our case, we were unable to identify the translocation partner to ETV6. The association of eosinophilia with immature lymphoidneoplasmscouldbeexplainedbythepresenceofan underlying clonal disease affecting a stem cell or even a more mature myeloid precursor that could transform into acute lymphoblastic leukemia/lymphoma [7]. This behavior issimilartowhatisseeninchronicmyeloidleukemiablast crisis or in leukemias/lymphomas associated with FGFR1 rearrangement [1, 10, 11]. We favor this explanation in our patient, in whom the presence of eosinophilia was not concomitant with the lymphoblastic lymphoma and who had a clonal cytogenetic alteration only detected at the time of the bone marrow infiltration by immature myeloid cells. The absence of chromosomal rearrangements in the initialbonemarrowanalysiscouldbeduetoaputativesmallsize of the malignant clone but may also indicate that the clinical course of our patient was part of the clonal evolution of a chronic disorder, with the appearance of de novo cytogenetic alterations in the acute phase. This is in agreement with findings in recently published series, where transformation into acute leukemia was described as a frequent event [13]in patients with the diagnosis of chronic eosinophilic leukemia. Moreover, chromosome 7 abnormalities, particularly at 7q22,
4 4 Case Reports in Hematology have been commonly associated with myelodysplastic syndromes and acute myeloid leukemia [14]. Our patient was treated according to the CALGB protocol, which includes drugs that are active in myeloid malignancies such as daunorubicin in the induction phase and cytarabin in the intensification. We could hypothesize that the proliferation of myeloid clone occurred after these drugs were no longer administered. In conclusion, our finding of an association between a myeloid clonal proliferation with t(7;12)(q22;p13), ETV6 rearrangement, and eosinophilia in a patient previously diagnosed with LBL is in agreement with the findings of other authors [6 8] and supports the diagnosis of a hematopoietic neoplasm originating in very immature cells with the ability to differentiate in myeloid and lymphoid lineages at different moments. We could hypothesize that this entity behaves in a similar way as the disorders with FGFR1 rearrangements and myeloid hyperplasia, eosinophilia, and lymphoblastic lymphoma, but further studies should be pursued aiming to identify other genes involved in this translocation and the underlying mechanism that leads to eosinophilia. Consent Written informed consent was obtained from the patient s next of kin for the publication of this case report. Conflict of Interests The authors declare that they have no conflict of interests. [8] S. Rezk, L. Wheelock, J. Fletcher et al., Acute lymphocytic leukemia with eosinophilia and unusual karyotype, Leukemia and Lymphoma,vol.47,no.6,pp ,2006. [9]F.WilsonandA.Tefferi, Acutelymphocyticleukemiawith eosinophilia: two case reports and a literature review, Leukemia and Lymphoma, vol. 46, no. 7, pp , [10]R.C.Inhorn,J.C.Aster,S.A.Roachetal., Asyndromeof lymphoblastic lymphoma, eosinophilia, and myeloid hyperplasia/malignancy associated with t(8;13)(p11;q11): description of a distinctive clinicopathologic entity, Blood, vol. 85, no. 7, pp , [11] D. Macdonald, A. Reiter, and N. C. P. Cross, The 8p11 myeloproliferative syndrome: a distinct clinical entity caused by constitutive activation of FGFR1, Acta Haematologica,vol.107, no. 2, pp , [12] E. De Braekeleer, N. Douet-Guilbert, and F. Morel, ETV6 fusion genes in hematological malignancies: a review, Leukemia Research,vol.36,no.8,pp ,2012. [13]G.Helbig,A.Soja,A.Bartkowska-Chrobok,andS.Kyrcz- Krzemień, Chronic eosinophilic leukemia-not otherwise specified has a poor prognosis with unresponsiveness to conventional treatment and high risk of acute transformation, American Hematology, vol.87,no.6,pp , [14] K. Fischer, S. Fröhling, S. W. Scherer et al., Molecular cytogenetic delineation of deletions and translocations involving chromosome band 7q22 in myeloid leukemias, Blood, vol. 89, no. 6, pp , References [1] S. H. Swerdlow, E. Campo, N. L. Harris et al., WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues,IARC Press, Lyon, France, 4th edition, [2] G. Spitzer and O. M. Garson, Lymphoblastic leukemia with marked eosinophilia: a report of two cases, Blood, vol.42,no. 3, pp , [3]M.Ayyub,M.Anwar,M.Luqman,W.Ali,M.Bashir,and B. J. Bain, A case of hypereosinophilic syndrome developing Hodgkin s disease after 4 years, British Haematology, vol. 123, no. 5, pp , [4] R. A. Larson, R. K. Dodge, C. A. Linker et al., A randomized controlled trial of filgrastim during remission induction and consolidation chemotherapy for adults with acute lymphoblastic leukemia: CALGB study 9111, Blood,vol.92,no.5,pp , [5] F. Roufosse, S. Garaud, and L. De Leval, Lymphoproliferativedisordersassociatedwithhypereosinophilia, Seminars in Hematology,vol.49,no.2,pp ,2012. [6] F.A.Bhatti,I.Hussain,andM.Z.Ali, AdultBlymphoblastic leukaemia/lymphoma with hypodiploidy (-9) and a novel chromosomal translocation t(7;12)(q22;p13) presenting with severe eosinophilia case report and review of literature., Hematology and Oncology,vol.2,p.26,2009. [7]G.A.Follows,R.G.Owen,A.J.Ashcroft,andL.A.Parapia, Eosinophilic myelodysplasia transforming to acute lymphoblastic leukaemia, Clinical Pathology,vol.52,no. 5, pp , 1999.
















5 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Correspondence should be addressed to Anas Khanfar;
 Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute leukemia
 Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation
 Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
Case #1. 65 yo man with no prior history presented with leukocytosis and circulating blasts: Bone marrow biopsy was performed
 Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Role of FISH in Hematological Cancers
 Role of FISH in Hematological Cancers Thomas S.K. Wan PhD,FRCPath,FFSc(RCPA) Honorary Professor, Department of Pathology & Clinical Biochemistry, Queen Mary Hospital, University of Hong Kong. e-mail: wantsk@hku.hk
Role of FISH in Hematological Cancers Thomas S.K. Wan PhD,FRCPath,FFSc(RCPA) Honorary Professor, Department of Pathology & Clinical Biochemistry, Queen Mary Hospital, University of Hong Kong. e-mail: wantsk@hku.hk
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Supervisor: Prof. Dr. P Vandenberghe Dr. C Brusselmans
 Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
Contribution of molecular diagnosis in eosinophilia/hypereosinophilia Eosinophilia Hypereosinophilia Hypereosinophilic syndrome Immune mediated hypereosinophilia Chronic eosinophilic leukemia (NOS)/ Idiopathic
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
BCR-ABL1 positive Myeloid Sarcoma Nicola Austin
 BCR-ABL1 positive Myeloid Sarcoma Nicola Austin Cytocell UK & Ireland User Group Meeting Jesus College, Cambridge 4 th - 5 th April 2017 Myeloid Sarcoma WHO Classification Tumours of Haematopoietic and
BCR-ABL1 positive Myeloid Sarcoma Nicola Austin Cytocell UK & Ireland User Group Meeting Jesus College, Cambridge 4 th - 5 th April 2017 Myeloid Sarcoma WHO Classification Tumours of Haematopoietic and
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia
 Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
MS.4/ 1.Nov/2015. Acute Leukemia: AML. Abdallah Abbadi
 MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
MS.4/ 1.Nov/2015. Acute Leukemia: AML Abdallah Abbadi Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising and hemorrhagic spots on her trunk
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Case Report Chronic Eosinophilic Leukemia Not Otherwise Specified (NOS) in the Background of a Large Cell Lymphoma
 in the Background of a Large Cell Lymphoma") Case Reports in Hematology Volume 2013, Article ID 458303, 4 pages http://dx.doi.org/10.1155/2013/458303 Case Report Chronic Eosinophilic Leukemia Not Otherwise Specified (NOS) in the Background of a Large
Case Reports in Hematology Volume 2013, Article ID 458303, 4 pages http://dx.doi.org/10.1155/2013/458303 Case Report Chronic Eosinophilic Leukemia Not Otherwise Specified (NOS) in the Background of a Large
Case Report Myeloid Sarcoma Presenting with Leukemoid Reaction in a Child Treated for Acute Lymphoblastic Leukemia
 Case Reports in Hematology, Article ID 757625, 5 pages http://dx.doi.org/10.1155/2014/757625 Case Report Myeloid Sarcoma Presenting with Leukemoid Reaction in a Child Treated for Acute Lymphoblastic Leukemia
Case Reports in Hematology, Article ID 757625, 5 pages http://dx.doi.org/10.1155/2014/757625 Case Report Myeloid Sarcoma Presenting with Leukemoid Reaction in a Child Treated for Acute Lymphoblastic Leukemia
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation
 Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Case Report T-Cell Lymphoblastic Leukemia/Lymphoma: Relapse 16 Years after First Remission
 Case Reports in Hematology, Article ID 359158, 4 pages http://dx.doi.org/10.1155/2014/359158 Case Report T-Cell Lymphoblastic Leukemia/Lymphoma: Relapse 16 Years after First Remission Lauren Elreda, 1
Case Reports in Hematology, Article ID 359158, 4 pages http://dx.doi.org/10.1155/2014/359158 Case Report T-Cell Lymphoblastic Leukemia/Lymphoma: Relapse 16 Years after First Remission Lauren Elreda, 1
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Katrina L. Lancaster-Shorts, Joanna Chaffin, Natasha M. Savage. Department of Pathology, Augusta University, Augusta, GA, USA;
 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Katrina L. Lancaster-Shorts, Joanna Chaffin, Natasha M. Savage Department of Pathology,
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Katrina L. Lancaster-Shorts, Joanna Chaffin, Natasha M. Savage Department of Pathology,
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Reactive and Neoplastic Lymphocytosis
 Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Reactive and Neoplastic Lymphocytosis Koranda A. Walsh, VMD, BS Assistant Professor, Clinical Pathobiology University of Pennsylvania School of Veterinary Medicine PLEASE NOTE: These notes are meant as
Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study
 Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
ABERRANT EXPRESSION OF CD19 AND CD43
 ABERRANT EXPRESSION OF CD19 AND CD43 IN A PATIENT WITH THERAPY-RELATED ACUTE MYELOID LEUKEMIA AND A HISTORY OF MANTLE CELL LYMPHOMA Yen-Chuan Hsieh, 1 Chien-Liang Lin, 2 Chao-Jung Tsao, 2 Pin-Pen Hsieh,
ABERRANT EXPRESSION OF CD19 AND CD43 IN A PATIENT WITH THERAPY-RELATED ACUTE MYELOID LEUKEMIA AND A HISTORY OF MANTLE CELL LYMPHOMA Yen-Chuan Hsieh, 1 Chien-Liang Lin, 2 Chao-Jung Tsao, 2 Pin-Pen Hsieh,
June 11, Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI
 June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
89 Beaumont Avenue, Given E-214-UVM363, Burlington, VT 05405, USA
 Case Reports in Medicine Volume 2016, Article ID 8324791, 4 pages http://dx.doi.org/10.1155/2016/8324791 Case Report Myeloid Neoplasms with t(5;12) and ETV6-ACSL6 Gene Fusion, Potential Mimickers of Myeloid
Case Reports in Medicine Volume 2016, Article ID 8324791, 4 pages http://dx.doi.org/10.1155/2016/8324791 Case Report Myeloid Neoplasms with t(5;12) and ETV6-ACSL6 Gene Fusion, Potential Mimickers of Myeloid
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Fluorescence in-situ Hybridization (FISH) ETO(RUNX1T1)/AML1(RUNX1) or t(8;21)(q21.3;q22)
 ETO(RUNX1T1)/AML1(RUNX1) or t(8;21)(q21.3;q22)") PML/RARA t(15;17) Translocation Assay Result : nuc ish(pml 2)(RARA 2)[200] : 200/200(100%) interphase nuclei show normal 2O 2G signals for PML/RARA : is Negative for t(15;17)(q22;q21.1) 2 Orange 2 Green
PML/RARA t(15;17) Translocation Assay Result : nuc ish(pml 2)(RARA 2)[200] : 200/200(100%) interphase nuclei show normal 2O 2G signals for PML/RARA : is Negative for t(15;17)(q22;q21.1) 2 Orange 2 Green
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328
 Rearrangement Following Therapy for APL Case 0328") Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Bumps on the Neck and Groin of a 2-Year-Old Male. Laboratory Findings: Table 1, Table 2; Figure 1; Image 1, Image 2, Image 3
 Bumps on the Neck and Groin of a 2-Year-Old Male 1 Erikakelly Strand, BS* Clinical History Patient: 2-year-old white male. Chief Complaint: Bumps on neck and groin. History of Present Illness: A 2-year-old
Bumps on the Neck and Groin of a 2-Year-Old Male 1 Erikakelly Strand, BS* Clinical History Patient: 2-year-old white male. Chief Complaint: Bumps on neck and groin. History of Present Illness: A 2-year-old
Relapsed acute lymphoblastic leukemia. Lymphoma Tumor Board. July 21, 2017
 Relapsed acute lymphoblastic leukemia Lymphoma Tumor Board July 21, 2017 Diagnosis - Adult Acute Lymphoblastic Leukemia (ALL) Symptoms/signs include: Fever Increased risk of infection (especially bacterial
Relapsed acute lymphoblastic leukemia Lymphoma Tumor Board July 21, 2017 Diagnosis - Adult Acute Lymphoblastic Leukemia (ALL) Symptoms/signs include: Fever Increased risk of infection (especially bacterial
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Hypereosinophili c syndrome
 Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
Hypereosinophili c syndrome Eosinophilia Eosinophilia is commonly defined as an elevated percentage of eosinophils, with an absolute eosinophil count > 500 cells per cubic millimeter Secondary Primary
Case Report Transformation of a Cutaneous Follicle Center Lymphoma to a Diffuse Large B-Cell Lymphoma An Unusual Presentation
 Case Reports in Medicine Volume 21, Article ID 296523, 5 pages doi:1.1155/21/296523 Case Report Transformation of a Cutaneous Follicle Center Lymphoma to a Diffuse Large B-Cell Lymphoma An Unusual Presentation
Case Reports in Medicine Volume 21, Article ID 296523, 5 pages doi:1.1155/21/296523 Case Report Transformation of a Cutaneous Follicle Center Lymphoma to a Diffuse Large B-Cell Lymphoma An Unusual Presentation
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Case 1. Sa A.Wang, MD UT MD Anderson Cancer Center Houston, TX
 Case 1 Sa A.Wang, MD UT MD Anderson Cancer Center Houston, TX Disclosure of Relevant Financial Relationships The USCAP requires that anyone in a position to influence or control the content of all CME
Case 1 Sa A.Wang, MD UT MD Anderson Cancer Center Houston, TX Disclosure of Relevant Financial Relationships The USCAP requires that anyone in a position to influence or control the content of all CME
Case Report Synchronous Occurrence of Chronic Myeloid Leukemia and Mantle Cell Lymphoma
 Hindawi Case Reports in Hematology Volume 2017, Article ID 7815095, 4 pages https://doi.org/10.1155/2017/7815095 Case Report Synchronous Occurrence of Chronic Myeloid Leukemia and Mantle Cell Lymphoma
Hindawi Case Reports in Hematology Volume 2017, Article ID 7815095, 4 pages https://doi.org/10.1155/2017/7815095 Case Report Synchronous Occurrence of Chronic Myeloid Leukemia and Mantle Cell Lymphoma
Acute Promyelocytic Leukemia with i(17)(q10)
(q10)") CASE REPORT Acute Promyelocytic Leukemia with i(17)(q10) Junki Inamura 1, Katsuya Ikuta 2, Nodoka Tsukada 1, Takaaki Hosoki 1, Motohiro Shindo 2 and Kazuya Sato 1 Abstract We herein report a rare chromosomal
CASE REPORT Acute Promyelocytic Leukemia with i(17)(q10) Junki Inamura 1, Katsuya Ikuta 2, Nodoka Tsukada 1, Takaaki Hosoki 1, Motohiro Shindo 2 and Kazuya Sato 1 Abstract We herein report a rare chromosomal
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Test Name Results Units Bio. Ref. Interval. Positive
 LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
Case Report. Introduction. Mastocytosis associated with CML Hematopathology - March K. David Li 1,*, Xinjie Xu 1, and Anna P.
 Mastocytosis associated with CML Hematopathology - March 2016 Case Report Systemic mastocytosis with associated clonal hematologic non-mast cell lineage disease (SM-AHNMD) involving chronic myelogenous
Mastocytosis associated with CML Hematopathology - March 2016 Case Report Systemic mastocytosis with associated clonal hematologic non-mast cell lineage disease (SM-AHNMD) involving chronic myelogenous
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Juvenile Myelomonocytic Leukemia Pre-HCT Data
 Instructions for Juvenile Myelomonocytic Leukemia Pre-HCT Data (Form 2015) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the JMML Pre-HCT Form. E-mail
Instructions for Juvenile Myelomonocytic Leukemia Pre-HCT Data (Form 2015) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the JMML Pre-HCT Form. E-mail
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
بسم هللا الرحمن الرحيم WBCs disorders *Slide 2: - we will focus on the disorders that are related to the # of WBCs - in children the # of lymphocyte is more than it in adults,sometimes more than neutrophils
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Flow Cytometry. Leukemia and Myelodysplastic Syndromes. Bone Marrow Aspirate and Biopsy
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Conditions that mimic neoplasia in the bone marrow. Kaaren K. Reichard Mayo Clinic Rochester
 Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in
Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in