Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine
|
|
|
- Myles Fleming
- 6 years ago
- Views:
Transcription

1 Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine

2 none
3

4 none
5 Reserved for pts: Complications from GERD Refractory esophagitis** Stricture Barrett s Persistent reflux symptoms despite acid suppression Asthma ** most frequent Surgical therapy is generally not recommended in patients who do not respond to PPI therapy. (Strong recommendation, high level of evidence) ACG
6 No consensus Useful tests in making surgical decisions Egd Esophageal manometry All patients should undergo preoperative manometry to rule out achalasia or scleroderma-like esophagus hour ph probe Preoperative ambulatory ph monitoring is mandatory in patients without evidence of erosive esophagitis. (Strong recommendation, moderate level of evidence) ACG
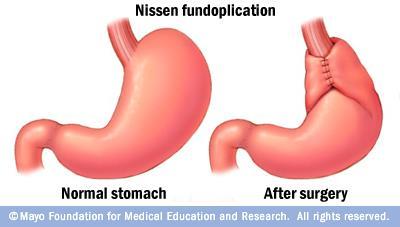
7 For most pts with GERD laparoscopic Nissen fundoplication Several advantages with similar efficacy and safety as an open procedure Surgical therapy is as effective as medical therapy for carefully selected patients with chronic GERD when performed by an experienced surgeon. (Strong recommendation, high level of evidence) ACG
8
9 Dysphagia Occurs in most pts dilatation Gas bloat Most pt improve over time Mild simethicone or charcoal tablets, avoid carbonation Trial of metoclopramide Persistent symptoms consider gastroparesis
10 Laparoscopic fundoplication 90-95% of patients satisfied with the results Experienced surgeons
11 Indications Failure of non-operative management of ulcer complication Suspicion of malignancy (usually gastric ulcer)
12 based on reduction of acid secretion Sectioning of vagus (vagotomy) Eliminating hormonal stimulation from the antrum (antrectomy) Decreasing the number of parietal cells (gastric resection)


13 I: pyloris removed II: greater curvature of stomach connected to the jejunum in end-toend anastomosis
14 Difference from duodenal is that gastric ulcer may harbor malignancy and therefore must be excised or generously biopsied.
15 Postvagotomy diarrhea Dumping syndrome Alkaline reflux gastritis Early satiety
16 30% of pts Most self limiting Pathogenesis poorly understood?rapid passage of unconjugated bile salts Oral cholestyramine
17 ~20% pts after gastrectomy or vagotomy and drainage Symptoms: Postprandial Gi discomfort +/- nausea, vomiting, diarrhea and cramps Vasomotor symptoms Diaphoresis Palpitations flushing
18 Precise mechanism not completely understood Attributed to rapid emptying of hyperosmolar chyme (particularly carbs) into the small bowel Leads to net fluid retention Leads to vasoactive hormone release Serotonin and VIP
19 Treatment Dietary changes Rarely operative therapy needed Octreotide may help with severe symptoms

20
21 Typical presentation RUQ pain Fever Leukocytosis Associated with gallbladder inflammation, Usually due to gallstone disease Complications (can be life-threatening) Gangrene Gallbladder perforation
22 Supportive Antibiotics Secondary infection from cystic duct obstruction and bile stasis Guidelines Start antibiotics if infection suspected based on: Lab (WBC >12,500) Clinical (temp >38.5C) Radiographic findings (air in gallbladder or wall) Advanced age, diabetes, immunodeficiency Infectious Diseases Society of America
23 Asymptomatic gallstones should not be treated Low risk pts with clinical improvement Elective cholecystectomy same hospitalization Low risk pts with deterioration Emergent cholecystectomy High risk(asa 3 and >) mortality 5-27% Clinical deterioration percutaneous cholecystostomy

24

25 Serious complications Result in part from patient selection Surgical inexperience Technical constraints of minimally invasive approach
26 Classified A-E based on type of injury Repair should always be approached by an experienced multidisciplinary team Surgeon Diagnostic radiologist Interventional gastroenterologist Interventional radiologist

27 Suspect in pts with fever, abdominal pain, bilious ascites Large loculated collections Percutaneous drainage, with catheter left in place for drainage ERCP: define leak and place stent Severe pain, progressive intraabdominal sepsis Operative exploration and washout
28 Bleeding Bowel injury Postcholecystectomy syndrome Complex of symptoms including Abdominal pain dyspepsia
29 56 yo obese female presents for gastric bypass surgery. She has failed multiple diets and medications. She doesn t have psychiatric issues other than depression due to condition. She has osteoarthritis of hips and knees, heartburn after large meals. PE: ht: 65 wt: 230lb BMI: 38.3kg/m2. BP:150/100. abd: obese w/ palpable liver edge. Lab normal CBC, HgA1C 6.9, triglyceride 250mg/dL, AST 65, AlkPh0s: 140 US: hepatomegaly and fatty changes
30 a. Her BMI alone b. Obesity related joint dz, with reduced mobility and quality of life c. Her BMI together with the features of metabolic syndrome d. Probable obesity-related liver disease e. Probable obesity-related GERD
31 BMI >40kg/m2 OR >35kg/m2 with additional evidence for metabolic syndrome: DM type II Hypertension And/or hyperlipidemia Failure of prior medical management Absence of significant psychiatric condition Answer: c

32 ~ 6 months after surgery she had lost a significant amount of weight, but was found to have significant normocytic anemia, with low levels of both serum B12 and iron. What is the likely mechanism for the development of both these micronutrient deficiencies? a. Anastomatic ulcer with blood loss b. Post-op dietary restrictions c. Small intestinal bacterial overgrowth d. Mechanical bypass of the gastroduodenal segment

33 a. Anastomatic ulcer with blood loss May account for iron losses but not B12 b. Post-op dietary restrictions c. Small intestinal bacterial overgrowth A possibility with surgically altered bowel. B12 def so macrocytic anemia d. Mechanical bypass of the gastroduodenal segment
34 Iron Bypassing of the duodenum Dominant site of iron absoption Lack of gastric acid Decrease absorption of iron B12 Decreased gastric acid liberates B12 to bind R- protein which allows B12 to bind to intrinsic factor Less acid = suboptimal absorption
35 Bleeding Wound infection Leaks PE/DVT CV complications Pulmonary complications Early Complications Roux-en-Y: gastric remnant distension stomal stenosis marginal ulcers cholelithiasis ventral incisional hernia internal hernia short bowel syndrome Dumping syndrome Late Complications
36 6-20%?etiology Ischemia or increased tension on anastomosis Nausea, vomiting, dysphagia, GERD Several weeks after surgery Endoscopic balloon dilation usually successful
37 1-16% Near gastrojejunostomy Causes Poor perfusion, foreign material (staples), excess acid exposure, NSAIDs, H.pylori, smoking Nausea, pain, bleeding or perforation Tx: acid suppression +/- sucralfate (95% successful)
 and mortality (0.")
38 sleeve of stomach Removes large portion of greater curvature Produces a decrease in ghrelin levels Reduce desire for food Low complications (3-24%) and mortality (0.4%)
39 Most common complications Bleeding Usually at staple line Most surgeons reinforce staple line Stenosis Can create gastric outlet obstruction May be able to treat with endoscopic dilation May need surgical intervention Gastric leaks One of most serious complication (5.3%) GERD

40

41 Transient inhibition of normal GI motility in the post op setting. Presumably, the muscle of the bowel wall is transiently impaired and fails to transport intestinal contents. Typically lasts 3-5 days.
42 Worse pain Nausea and vomiting Delay in enteral nutrition Prolonged hospitalization Increased risk of complications Increased health care costs
43 Poorly understood 1. Neural reflexes involving the sympathetic nervous system may inhibit motility 1. Epidural anesthetic agents decreased duration of post op ileus. 2.? Due to blockade of neural reflexes at the spinal cord level.
44 2. Local and systemic inflammatory mediators may play a role. 1. NSAIDs decrease POI
45 3. Exacerbating factors 1. Opioid analgesics 2. Intraperitoneal surgery 3. Degree of bowel manipulation 4. Open vs. laparoscopic surgery 5. hypokalemia
46 Abdominal pain Nausea/vomiting Anorexia Abdominal bloating/distension Absent bowel sounds Lack of passage of flatus or stool Tympanic abdomen No visible peristalsis
47 Pain is typically mild and constant Mechanical obstruction usually severe

48 Lack of bowel sounds Increase abdominal girth Lack of visible peristalsis Tympanic abdomen Xray: air-fluid levels or nonspecific patterns


49
50 Metoclopramide, cisapride, erythromycin RCT don t show benefit Laxatives Possible benefit Opiate antagonists May show benefit, but more studies needed
51 Epidural anesthesia NSAIDs Probable benefit Need to be cautious of SE Multimodality therapy
52 Nasogastric tube No evidence of benefit, may increase pulmonary complication. Early enteral nutrition Appears safe and well tolerated. Early mobilization No change, but may decrease other complication OMM Chew gum
53
Lecture Goals. Body Mass Index. Obesity Definitions. Bariatric Surgery What the PCP Needs to Know 11/17/2009. Indications for bariatric Surgeries
 Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Postoperative Ileus. UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011
 Postoperative Ileus UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Hobart W. Harris, MD, MPH Introduction Pathophysiology Clinical Research Management Summary Postoperative Ileus:
Postoperative Ileus UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Hobart W. Harris, MD, MPH Introduction Pathophysiology Clinical Research Management Summary Postoperative Ileus:
ADVANCE AT YOUR OWN PACE
 ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Complications After Bariatric Surgery. Kunoor Jain-Spangler, MD
 Complications After Bariatric Surgery Kunoor Jain-Spangler, MD Disclaimer This topic could be a 2-3 day course. Will focus on common clinical conditions seen by Primary Care Physicians in the office setting.
Complications After Bariatric Surgery Kunoor Jain-Spangler, MD Disclaimer This topic could be a 2-3 day course. Will focus on common clinical conditions seen by Primary Care Physicians in the office setting.
SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS
 SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS 55 years old male, Farm worker, married, from Ibb Heavy Smoker, Khat chewer non-alcohol
SARCINA VENTICULARI IS A POSSIBLE CAUSATIVE MICROORGANISM OTHER THAN H.PYLORI IN GASTRIC OUTLET OBSTRUCTION PATHOGENESIS 55 years old male, Farm worker, married, from Ibb Heavy Smoker, Khat chewer non-alcohol
GI -A & P Review Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas 8/11/2011
 Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
Bariatric Surgery Risk Education Packet Walter J. Chlysta MD, FACS
 Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Weight Loss Surgery. Outline 3/30/12. What Every GI Nurse Needs to Know. Define Morbid Obesity & its Medical Consequences. Treatments for Obesity
 3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Adipocytes, Obesity, Bariatric Surgery and its Complications
 Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
GI -A & P Review PUD. Peptic Ulcer Disease (PUD) Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer
 Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer") GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Technique. Matthew Bettendorf, MD Essentia Health Duluth Clinic. Laparoscopic approach One 12mm port, Four 5mm ports
 Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Benefits of Bariatric Surgery
 Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor
 Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Functional Dyspepsia. Norbert Welkovics Heine van der Walt
 Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
SURGICAL MANAGEMENT OF OBESITY. Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery
 SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
MBSAQIP Complex Clinical Scenarios & Variable Review
 MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Viriato Fiallo, MD Ursula McMillian, MD
 Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
See Policy CPT CODE section below for any prior authorization requirements
 Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Constipation An Overview. Definition Physiology of GI tract Etiology Assessment Treatment
 CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
Managing Complications of Bariatric Surgery. Objectives
 Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Goals 1/9/2018. Obesity over the last decade Surgery has become a safer management strategy Surgical options for management
 The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
Informed Consent for Laparoscopic Vertical Sleeve Gastrectomy. Please read this form carefully and ask about anything you may not understand.
 Maryland Bariatric & Laparoscopic Surgeons Dr Andrew Averbach & Dr Isam Hamdallah 700 Geipe Road, Suite 274 Catonsville, MD,21228 Tel 667 234 8725 Fax 667 234 8726 Informed Consent for Laparoscopic Vertical
Maryland Bariatric & Laparoscopic Surgeons Dr Andrew Averbach & Dr Isam Hamdallah 700 Geipe Road, Suite 274 Catonsville, MD,21228 Tel 667 234 8725 Fax 667 234 8726 Informed Consent for Laparoscopic Vertical
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Laparoscopic Gastric Bypass Information
 1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
BARIATRIC SURGERY. Weight Loss Surgery. A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female
 BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease
 ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE
 INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor
INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Dr. Patsy Smyth, FNP-BC
 Dr. Patsy Smyth, FNP-BC Gastroparesis literally translated means stomach paralysis. Gastroparesis is a syndrome characterized by delayed gastric emptying in absence of mechanical obstruction of the stomach.
Dr. Patsy Smyth, FNP-BC Gastroparesis literally translated means stomach paralysis. Gastroparesis is a syndrome characterized by delayed gastric emptying in absence of mechanical obstruction of the stomach.
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
PATIENT CONTRACT LAPAROSCOPIC VERTICAL SLEEVE GASTRECTOMY
 PATIENT CONTRACT LAPAROSCOPIC VERTICAL SLEEVE GASTRECTOMY This contract is supported by my surgeon,, and will be effective and ongoing from the initial evaluation for a laparoscopic vertical sleeve gastrectomy.
PATIENT CONTRACT LAPAROSCOPIC VERTICAL SLEEVE GASTRECTOMY This contract is supported by my surgeon,, and will be effective and ongoing from the initial evaluation for a laparoscopic vertical sleeve gastrectomy.
In the Name of God. Refractory GERD
 In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
Bariatric Surgical Complications and Recent Trends in Outcome Data
 Bariatric and Metabolic Conference Bariatric Surgical Complications and Recent Trends in Outcome Data Daniel A.P. Smith, MD Bariatric Surgery Director Essentia Health Park Rapids St. Joseph s Center for
Bariatric and Metabolic Conference Bariatric Surgical Complications and Recent Trends in Outcome Data Daniel A.P. Smith, MD Bariatric Surgery Director Essentia Health Park Rapids St. Joseph s Center for
Objectives. Identify age-related changes in the gastrointestinal tract
 The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
UPPER GI DISEASES 11/15/2014. Lesson Objectives. GI Tract Review. NUTR 2050 Nutrition for Nursing Professionals. Mrs. Deborah A. Hutcheon, MS, RD, LD
 UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
CHRONIC DIARRHEA DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS
 DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS") DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know
 Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know Valerie J. Halpin Legacy Weight and Diabetes Institute November 3, 2017 Surgical Overview Indications Contraindications
Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know Valerie J. Halpin Legacy Weight and Diabetes Institute November 3, 2017 Surgical Overview Indications Contraindications
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Paraoesophageal Hernia
 Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
LAPAROSCOPIC GALLBLADDER SURGERY
 LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
Here are some types of gastric bypass surgery:
 Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
The Aging Digestive System
 The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
Morbid Obesity A Curable Disease?
 Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes. Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018
 WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
Overview. Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco
 GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
INFORMED CONSENT FOR LAPAROSCOPIC ADJUSTABLE GASTRIC BAND
 INFORMED CONSENT FOR LAPAROSCOPIC ADJUSTABLE GASTRIC BAND It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor is providing for you
INFORMED CONSENT FOR LAPAROSCOPIC ADJUSTABLE GASTRIC BAND It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor is providing for you
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Propulsion and mixing of food in the alimentary tract Chapter 63
 Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Propulsion and mixing of food in the alimentary tract Chapter 63 Types of GI movements: Propulsive movement-peristalsis Propulsion: controlled movement of ingested foods, liquids, GI secretions, and sloughed
Imaging findings in complications of bariatric surgery.
 Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
Commonly Performed Bariatric Procedures in Singapore. Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital
 Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Gastroenterology Fellowship Program
 Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS
 Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
Effective Health Care
 Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
Not over when the surgery is done: surgical complications of obesity
 Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Demographics. MBSAQIP Case Number: *ACS NSQIP Case Number: *LMRN: *DOB: / / *Gender: Male Female
 Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Form 1: Demographics
 Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
INFORMED CONSENT FOR LAPAROSCOPIC ADJUSTABLE GASTRIC BAND. Please read this form carefully and ask about anything you may not understand.
 Please read this form carefully and ask about anything you may not understand. I consent to undergo laparoscopic placement of a laparoscopic Adjustable Gastric Band for the purposes of weight loss. I met
Please read this form carefully and ask about anything you may not understand. I consent to undergo laparoscopic placement of a laparoscopic Adjustable Gastric Band for the purposes of weight loss. I met
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
10/16/2014. Normal Weight: BMI Overweight: BMI >25 Obese: BMI >30 Morbidly Obese: BMI >40 or >35 with 2 comorbidities
 Brinton Clark, MD, MPH Department of Medical Education Providence Portland Medical Center October 25 th, 2014 Oregon Society of Physician Assistants Fall Conference 45 yo woman with BMI=40kg/m2 (weight
Brinton Clark, MD, MPH Department of Medical Education Providence Portland Medical Center October 25 th, 2014 Oregon Society of Physician Assistants Fall Conference 45 yo woman with BMI=40kg/m2 (weight
INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE
 *Denis J. Halmi, MD, FACS *Daniel D. Tran, MD, FACS * Amir Moazzez, MD, FACS Yohannes Mahtemework, INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to
*Denis J. Halmi, MD, FACS *Daniel D. Tran, MD, FACS * Amir Moazzez, MD, FACS Yohannes Mahtemework, INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to
Enhanced Recovery after Surgery - A Colorectal Perspective. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid