Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions
|
|
|
- Britton Underwood
- 6 years ago
- Views:
Transcription
1 Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions Bernard A. Cohen, M.D. Johns Hopkins Children s Center Baltimore, Maryland (NO disclosures) American Epilepsy Society Annual Meeting
2 Learning Objectives Survival dermatology: Primer on systematic approach *Clues: gestsalt, distribution, pattern recognition, anatomic depth, distribution, setting, other clues Pattern recognition: viral exanthem models Pattern recognition: specific drug reactions Management Risk factors and prevention
3 Drug Reactions: Epidemiology Cutaneous reactions cause 3% of disabling injuries during hospitalization % associated with mortality Risk factors: female, increasing age, number of drugs, immunosuppression Eg. HIV 10-15X risk with sulfonamides Resources:Boston Collaborative Drug Surveillance Program
4 Drug Reactions: Pathogenesis Hypersensitivity reactions/immunologic? IgE dependent (type I) Cytotoxic (type II) Immune compelx (type III) Cell mediated (IV) Non-immunologic Overdose, pharmacologic side effects, cumulative/delayed toxicity, drug-drug interaction, alteration in metabolism, exacerbation of disease Idiosyncratic (possible immunologic) DRESS, TEN/SJS, in HIV setting, Drug-induced lupus Importance of Immunologic parameters and genetic predisposition (stay tuned)

5

6
7

8

9
10 Systematic Evaluation:History How long, chronology? Does it itch, hurt? Self treatment? Other drugs? Myths?
11
12 Systematic Evaluation:Exam Good light Good skin exposure Good eye Good book

13
14 Systematic Evaluation:General Considerations General health, chronology Distribution PATTERN Organization Morphology Anatomic depth Tumor v inflammatory

15

16
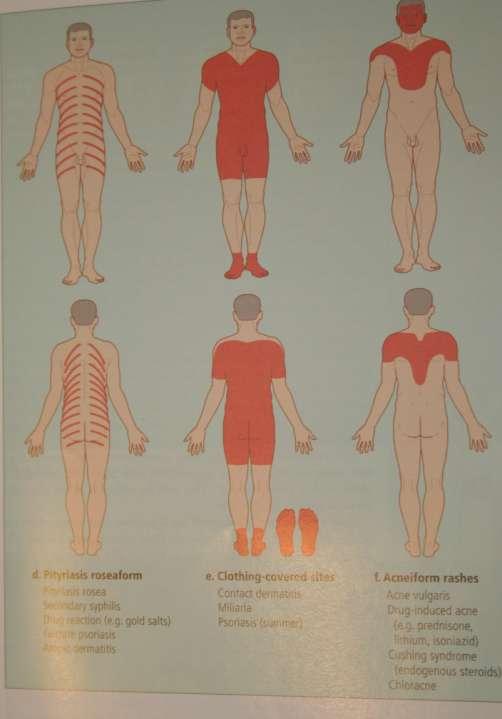
17 Sun Exposed Sites Phototoxic reactions (sun burn, eg.valproic acid) Photoallergic reactions (eg. drug) Psoriasis (isomorphic phenomenon) Polymorphous light eruption Porphyria Lupus erythematosus

18

19 Anatomic Depth
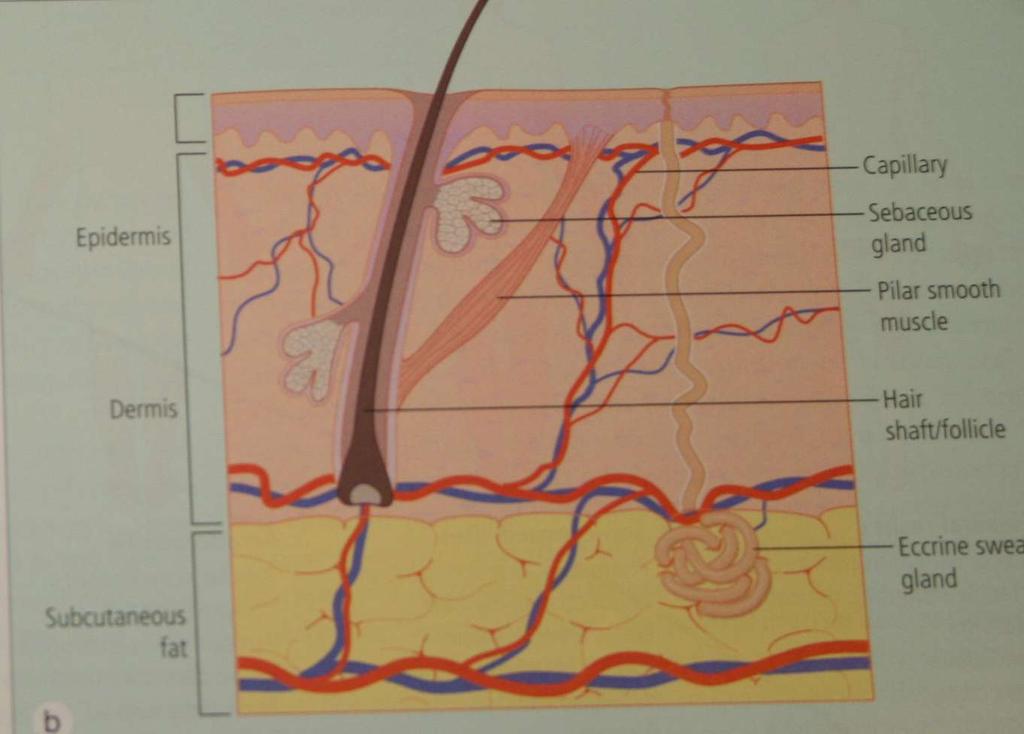
20 Anatomical Depth


21 and the age of the patient Variable morphology of the rash Variable course Variable exposure/susceptibility Variable incidence of disease



22 Scabies in an adolescent



23 Immunologic Parameters Hereditary immunodeficiency Acquired immunodeficiency Drug induced immunosuppression Cutaneous disease in transplantation

24 Inside v Outside Job How did the eruption get there? Localized? Contact reaction Primary cutaneous innoculation Local reactivation Disseminated? Reactive process (viral, drug, immunologically mediated) Embolic Toxin mediated


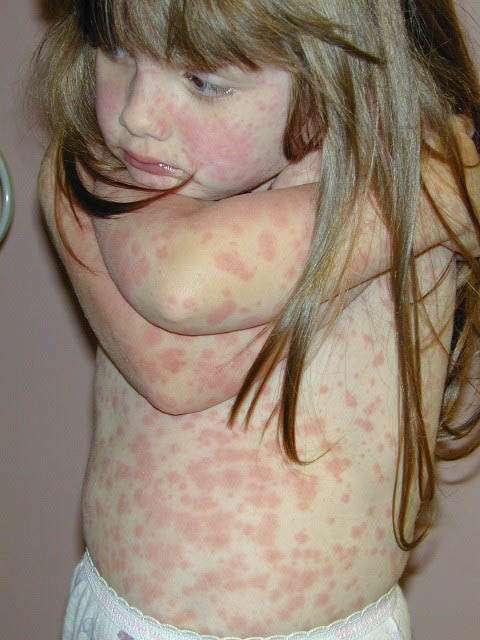
25 Measles=morbilliform
26 Although morbilliform=exanthematous= maculopapular Never, never, never, never, never,never, never, never, never, never, never, never, never, never, never never use the term maculopapular.
27 Measles Measles virus, genus Morbillivirus, family Paramyxoviridae Respiratory droplet spread 7-10 day incubation 2-4 day prodrome cough, coryza, conjunctivitis, Koplik spots 10 day skin eruption DEFINES MOST COMMON DRUG REACTION PATTERN

28 Amoxicillin induced morbilliform eruption
29 Enteroviral exanthem morbilliform eruption
 7-14 days after initiation of med 1%")
30 Morbilliform (Exanthematous) Drug Reactions Most common cause cutaneous reactioms Typer IV?, drug or metabolite binds? MHC II-peptide complexes, cytotoxicity results in keratinocyte necrosis May be potentiated by viral infections (HHV6, HIV, adenovirus, EBV, CMV, Parvovirus B19) 7-14 days after initiation of med 1% of most drugs, but increased with aminopenecillins, sulfonamides, cephalosporins, ANTICONVULSANTS Usually resolve, occasionally marker for more severe reaction

31 Urticaria
32 urticaria

33 Urticaria, Angioedema, Anaphylaxis IgE mediated type I reaction Edematous papules, expanding plaques, angioedema with deeper lesions Transient <24 hours, migratory Urticarial vasculitis >24 hours Acute < 6 wks v chronic Drugs: aminopenecillins, cephalosporins, sulfonamides, erythromycin, tetracycline Skin testing for PCN only




34 Graft v host disease sort of morbilliform too

35 Scarlet fever
36 Scarlet Fever-2nd Disease Pyrogenic exotoxin producing group A betahemolytic streptococcal infection Early 20 th century-toxin A 1950 s-toxin types C and B Risk of Rheumatic fever/serious complications declined before introduction of antibiotics DEFINES <5% OF DRUG REACTION PATTERNS
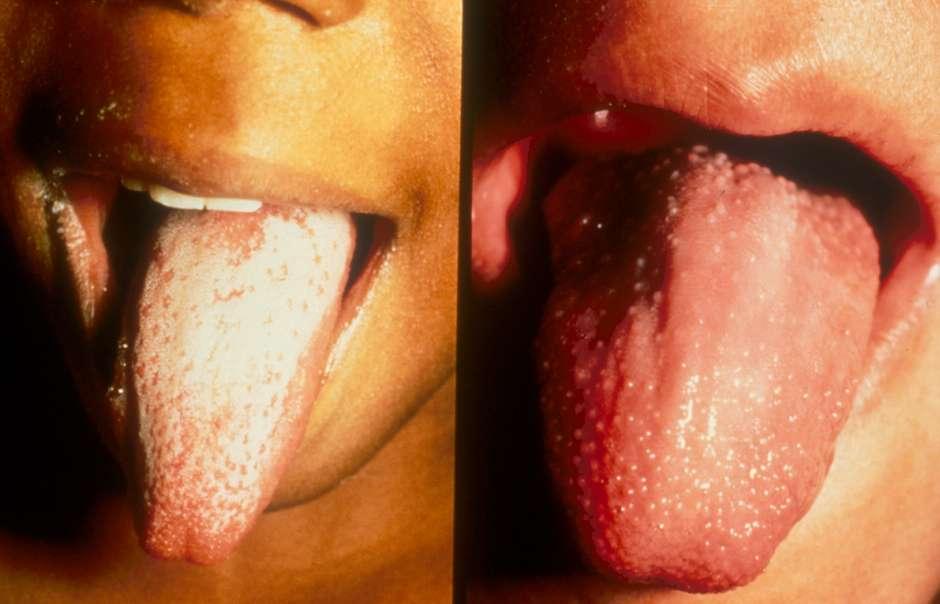
37 Enanthem-strawberry tongue
38 What else can give you a scarlatiniform eruption and a strawberry tongue? Staphylococcal infection (Staph/strep TSS) Viral exanthem Drug reaction Kawasaki syndrome


39 Leukocytoclastic Vasculitis
40 Vasculitis-Clinical pattern that you must know! Palpable purpura-destruction of small vessels Infectious (and non-infectious) Infections=fever, sick patient (usually) May be life-threatening Early recognition and treatment life-saving DEFINES <5% OF DRUG REACTION PATTERNS, BUT IMPORTANT TO MAKE DX, RECOGNIZE SYSTEMIC SX S


41 Leukocytoclastic vasculitis.
42 Leukocytoclastic Vasculitis 7-21 days after initiation of med 3-5 days on rechallenge Penecillins, NSAID s, sulfonamides, cephalosporins, PTU, thiazide diuretics, allopurinol, PHENYTOIN, biologic agents, hydralazine, minocycline Often restricted to skin but may be systemic

43 Recurrent itchy rash on the ankle of a 40- year-old man

44 Fixed Drug Eruption Recurrent itchy violaceous plaques/target lesions with admin of same drug NSAID s, sulfonamides, BARBITURATES, tetracyclines, CARBAMAZEPINE Red acutely, PIH following D/C of drug Lips, trunk, legs, arms, genitals Systemic reactions unusual More common in adults Cause unclear but memory T-cell resides in dermis Tx: stop the drug


45 Staphylococcal scalded skin syndrome exfoliative toxin superficial epidermal cleavage, mucous membranes spared

46 v. Stevens-Johnson syndrome (or TEN) drug-induced injury with skin cleavage at basement membrane zone, severe mucous membrane involvement
 80-95% assoc with drugs 1-8 weeks after initiation of drug, within hours on reexposure Morbilliform, atypical targetoid lesions")
47 SJS/TEN Spectrum of ds or distinctive? SJS:at least 2 mucous membranes,<10-30% BSA SJS 1.2-6/million people/yr TEN /million people/yr HIV 1/thousand people/yr (antiretroviral use) 80-95% assoc with drugs 1-8 weeks after initiation of drug, within hours on reexposure Morbilliform, atypical targetoid lesions Widespread flaccid bullae, erosions, ulceration of skin, inflammation and ulceration of mouth/mmm

48 SJS/TEN Systemic Disease Conjunctivae, trachea, bronchi, gut, kidney Acute renal failure, ATN 25% pulmonary dysfunction, adult RDS, fibrosis Anemia, keukopenia, hepatitis Abdominal pain, diarrhea Encephalopathy, myocarditis

49 SJS/TEN:Pathogenesis T-cell mediated process CD8+ trigger keratinocyte necrosis Drug noncovalently bind to MHC and TCR vs metabolites of drugs binding covalently to cellular peptides that stimulate immune sys Apoptosis causes cell death with upregulation of CD8+ cells and granzyme B/perforin, soluble Fas ligant, NO, TNFalpha

50 Highest Risk Drugs Nevirapine Lamotrigine Carmazepine Phenytoin Antibiotic sulfonamides Allopurinol Oxicam NSAID s Also Aminopenecillins, cephalo, quinolones (European SCAR, Roujeau et al, Mockenhaupt et al)
51 SJS/TEN Prevention! Relationship to MHC allotype For aromatic seizure meds (carbamazepine, pehnytoin, oxcarbazapine, lamotrigine and HLA- B*1502 and allopurinol and HLA-B*5801 in Han Chinese HLA-B*1502 and carbamazepine in Thai, Malaysian, South Indians HLA-B*5801 and allopurinol in W Europeans HLA-B*5701 and abacavir HLA-A*3101 and carbamazepine in Europeans
52 SJS/TEN: Managment Systemic steroids, IVIG, cyclosporine, etc not proven better than supportive measures No repeat exposures Genetic HLA testing for East Asians before starting aromatic meds or abacavir Immediate cessation of med Burn unit management


53 19-year-old girl with 2 week history of high fever increasing white count, eosinophilia, hepatitis. Drug reaction with eosinophilia and systemic symptoms DRESS Old phenytoin reaction/anticonsulsant hypersensitivity reaction Dramatic elevation of HHV6
54 DRESS Drug eruption: generalized edema, morbilliform rash, tense bullae, lip erosions No epidermal sloughing Fever, multiorgan involvement Pharyngitis, cervical adenopathy Atypical lymphocytosis, eosinophilia Hepatitis, interstitial nephritis, pneumonitis, encephalitis and (thyroiditis, carditis, pancreatitis, epididymitis, myositis, etc)
55 DRESS:Epidemiology On first exposure to med 1-6 weeks post exposure 1:3,000 exposures Aromatic anticonvulsants, lamotrigine, sulfonamide antibiotics, dapsone, minocycline allopurinol, mevaripine
56 DRESS: Management Family history (possibly AD inheritance) Stop drug asap, supportive care Role of systemic steroids? Symptoms may persist or recur for months Complications (renal, hepatic, pulmonary)

57 Acute Generalized Exanthematous Pustulosis (AGEP) Acute onset of nonfollicular pustules on edematous red base, fever, facial edema, target lesions, purpura, vasculitis, blisters, Mucosal erosions in 50% Short period of sensitization, topical or systemic Clinical findings and course overlap with DRESS, TEN
 TEN with some features of AGEP. Kiyohara T. Acta Derm Venereol 2013;27:212-4. May overlap with TEN.")
58 AGEP and Anticonvulsants Phenytoin-induced AGEP. Aziz N.JAAD 2010;62: AGEP:analysis of cases managed in a tertiary hospital in Singapore. Lee HY.Intl J Dermatol 2010;49: (1/8 induced by phenytoin, some evolved to DRESS.) TEN with some features of AGEP. Kiyohara T. Acta Derm Venereol 2013;27: May overlap with TEN.) Tx: stop med Systemic steroids? HLA-B5, -DR11, -DRQ Release of neurtophil-activating cytokines? Beta-lactam antibiotics, calcium channel blockers, hydroxychloroquine, CARBAMAZEPINE, PHENYTOIN, other antimicrobials
59 Take home! Know your drug eruptions especially markers for severe reactions Know you skin exam: full skin exam including mucous membranes, palms and soles, genitals Know your patients: risk factors, HLA markers, personal or family history of reactions When in doubt stop the drug, sooner the better Know when to call your friendly neighborhood dermatologist
60 Bibliography: General Cutaneous Drug Eruptions:A 5-year Experience. Gerson D, et al. J Am Acad Dermatol 2008;59: Cutaneous Drug Reactions in Children: An Update. Paediatr Drugs 2013 Jul 11. A Review of Cutaneous Drug Eruptions. Ahmed AM, et al. Clinics in Geruatric Medicine 2013;29: Cutaneous Drug Reactions. Khan D. J Aller Clin Immunol 2012;1225.
61 Bibliography SJS/TEN Toxic Epidermal Necrolysis:Part I. Introduction, History Schwartz RA, McDonough PH, Lee BW. J Am Acad Dermatol 2013;69: (Part II follows). TEN: the year in review. Lee HY, Chung WH. Curr Opin Allergy Clin Immunol 2013;13: Pharmacogenetics of cutaneous drug reactions. Alhara M. J Dermatol 2011:38: SJS and TEN:what do we know? Tartarone A, Lerose R. Ther Drug Monit 2010;32:669-72
62 Bibliography DRESS DRESS: a clinical review and review of current thinking. Wash SA. Creamer D. Clin Exp Dermatol 2011;36:6-11. DRESS syndrome:part I Clinical Perspectives. Hussain Z, Reddy BY, Schwartz RA. J Am Acad Dermatol 2013;68:693. (Part II follows) AGEP AGEP Fermamdp SL. Australas J Dermatol 2012;53:87-92 (Review).
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Herbal and homeopathic products, often considered natural and non-toxic, can also cause adverse drug reactions.
 Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
Big rashes in little patients:
 ! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
Bugs and Drugs: What s New in Hypersensitivity Reactions?
 Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES. R e g i S C A R PATIENT'S DATA. Age country of birth
 REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
DERMATOLOGIC EMERGENCIES. Mary Evers D.O., F.A.O.C.D. Georgetown, Texas
 DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
An Evidenced-Based Approach to the Adult with a Morbilliform Eruption
 Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Drug Allergy A Guide to Diagnosis and Management
 Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
AOU Ospedali Riuniti - Ancona
 AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
Goals of this talk. Morbilliform. Common Morphologies in the Hospital 11/7/2017. Hospital Based Dermatology: Common and Tough Consult Cases
 Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
GOOD MORNING! AUGUST 5, 2014
 GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
Cutaneous drug reactions
 Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
Skin Manifestations of Drug Reactions
 Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions
 PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
EXANTHEMATOUS ILLNESS. IAP UG Teaching slides
 EXANTHEMATOUS ILLNESS 1 DEFINITIONS Exanthema eruption of the skin Exanthema eruption of mucosae Macule flat nonpalpable lesion Papule small palpable lesion Nodule large palpable lesion Vesicle small fluid
EXANTHEMATOUS ILLNESS 1 DEFINITIONS Exanthema eruption of the skin Exanthema eruption of mucosae Macule flat nonpalpable lesion Papule small palpable lesion Nodule large palpable lesion Vesicle small fluid
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW
 SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
Dilantin (phenytoin) ROBERT A. SCHWARTZ
 ROBERT A. SCHWARTZ") Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update
 Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Syndrome de Lyell Approche diagnostique. seminaires iris. Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme.
 Syndrome de Lyell Approche diagnostique Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme Serge Jennes Hôpital Militaire Rash benign Pustulose exanthematique Aigue et généralisée
Syndrome de Lyell Approche diagnostique Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme Serge Jennes Hôpital Militaire Rash benign Pustulose exanthematique Aigue et généralisée
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Mechanisms of Drug Hypersensitivity Reactions
 18/5/213 Mechanisms of Drug Hypersensitivity Reactions Munir Pirmohamed NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology Institute of Translational Medicine University of
18/5/213 Mechanisms of Drug Hypersensitivity Reactions Munir Pirmohamed NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology Institute of Translational Medicine University of
To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving
 Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive Patients
 Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Five things not to miss in Dermatology. Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine
 Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
D.R.E.S.S. Syndrome An update. David H. Peng MD MPH Department of Dermatology Keck School of Medicine of USC
 D.R.E.S.S. Syndrome An update David H. Peng MD MPH Department of Dermatology Keck School of Medicine of USC I have no disclosures I will be discussing off label uses for medications Maculopapular Morbilliform
D.R.E.S.S. Syndrome An update David H. Peng MD MPH Department of Dermatology Keck School of Medicine of USC I have no disclosures I will be discussing off label uses for medications Maculopapular Morbilliform
OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT
 OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT Lung-Chang Lin, 1,2 Ping-Chin Lai, 3 Sheau-Fang Yang, 4 and Rei-Cheng Yang 1,5 Departments of 1 Pediatrics and 4 Pathology, Kaohsiung Medical
OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT Lung-Chang Lin, 1,2 Ping-Chin Lai, 3 Sheau-Fang Yang, 4 and Rei-Cheng Yang 1,5 Departments of 1 Pediatrics and 4 Pathology, Kaohsiung Medical
Cutaneous Conditions Associated with Systemic Disease
 Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center
 Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Bacteria: Scarlet fever, Staph infection (sepsis, 4S,toxic shock syndrome), Meningococcemia, typhoid Mycoplasma Rickettsial infection
, Meningococcemia, typhoid Mycoplasma Rickettsial infection") Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
An unpredictable, dose-independent adverse drug reaction which is immunologically or IgEmediated.
 R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
Emergency Dermatology. Emergency Dermatology
 Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Managing Penicillin Allergy
 Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening
 CMAJ Cases Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening Suran L. Fernando MB BS PhD, Andrew J. Broadfoot MB BS Previously published at www.cmaj.ca
CMAJ Cases Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening Suran L. Fernando MB BS PhD, Andrew J. Broadfoot MB BS Previously published at www.cmaj.ca
A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome
 Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review
 Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
The mechanisms of common drug hypersensitivities and implications for testing
 The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
Goals of this lecture. Case 2/24/2012. Drug eruptions. The red leg. Pyoderma gangrenosum
 Goals of this lecture Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Drug eruptions Tell the difference between
Goals of this lecture Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Drug eruptions Tell the difference between
Adverse Drug Reactions. Navigating the World of. Adverse Drug Reactions. Definition. Essential History Taking. Essential History Taking
 Adverse Drug Reactions Navigating the World of Adverse Drug Reactions Jason Knuffman, M.D. Quincy Medical Group Quincy, IL Allergy and Immunology Section Upon completion of this activity, the participant
Adverse Drug Reactions Navigating the World of Adverse Drug Reactions Jason Knuffman, M.D. Quincy Medical Group Quincy, IL Allergy and Immunology Section Upon completion of this activity, the participant
Objectives 8/30/2012. How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Adverse Drug Reactions
 Drug Allergies? Adverse Drug Reactions") How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
Kawasaki Disease. 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD. Children s Specialty Group. All rights reserved.
 Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
Infectious Disease. Chloe Duke
 Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
allergy Asia Pacific Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from
 pissn -876 eissn -868 Original Article Asia Pac Allergy 6;6:-7 Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from 9 Oki Suwarsa *, Wulan
pissn -876 eissn -868 Original Article Asia Pac Allergy 6;6:-7 Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from 9 Oki Suwarsa *, Wulan
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes
 Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Concentrate on Descriptors. An Approach to Skin Diseases in the ER
 Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
Prevalence and pattern of adverse cutaneous drug reactions presenting to a tertiary care hospital
 International Journal of Research in Dermatology Janardhan B et al. Int J Res Dermatol. 2017 Mar;3(1):74-78 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20164248
International Journal of Research in Dermatology Janardhan B et al. Int J Res Dermatol. 2017 Mar;3(1):74-78 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20164248
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
Patricia A. Treadwell, M.D. Professor of Pediatrics
 EXANTHEMS Patricia A. Treadwell, M.D. Professor of Pediatrics Indiana University School of Medicine FACULTY DISCLOSURE I have the following financial relationships with the manufacturer(s) of any commercial
EXANTHEMS Patricia A. Treadwell, M.D. Professor of Pediatrics Indiana University School of Medicine FACULTY DISCLOSURE I have the following financial relationships with the manufacturer(s) of any commercial
MEASLES (campak, rubeola, gabak, kerumut) Infectious and Tropical Pediatric Division Department of Child Health, Medical Faculty, University of Sumate
 Infectious and Tropical Pediatric Division Department of Child Health, Medical Faculty, University of Sumate") MEASLES (campak, rubeola, gabak, kerumut) Infectious and Tropical Pediatric Division Department of Child Health, Medical Faculty, University of Sumatera Utara 1 Maculapapular eruption : 1. Measles 2. Atypical
MEASLES (campak, rubeola, gabak, kerumut) Infectious and Tropical Pediatric Division Department of Child Health, Medical Faculty, University of Sumatera Utara 1 Maculapapular eruption : 1. Measles 2. Atypical
Learning Objectives. History 8/1/2016. An Approach to Pediatric Rashes
 An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Hospital-based Dermatopathology. Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM
 Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
Dermatology Pearls for Inpatient Medicine. Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University
 Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Drug Allergy: A Rash ionale for Treatment
 Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
Adverse drug reactions
 Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
VARICELLA. Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara
 VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
FIT Board Review Corner April 2017
 FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
ANTIBIOTICS ACUTE RHINOSINUSITIS IN CHILDREN
 MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.
MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.
Cutaneous drug eruptions are seen commonly
 REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
Visual Diagnosis. Q-PEM: Jan Dr. Rafah F. Sayyed PEC - Al Sadd, Doha
 Visual Diagnosis Q-PEM: Jan 2017 Dr. Rafah F. Sayyed PEC - Al Sadd, Doha DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Introduction Speed and Accuracy
Visual Diagnosis Q-PEM: Jan 2017 Dr. Rafah F. Sayyed PEC - Al Sadd, Doha DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Introduction Speed and Accuracy
Cutaneous drug reactions to antiepileptic drugs and relation with HLA alleles in the Turkish population
 O R I G I N A L A R T I C L E Eur Ann Allergy Clin Immunol Vol 50, N 1, 36-41, 2018 S. Büyüköztürk 1, Ç. Kekik 2, A.Z. Gökyiğit 3, F.İ. Tezer Filik 4i, G. Karakaya 4, S. Saygı 4i, A.B. Dursun 5, S. Kirbaş
O R I G I N A L A R T I C L E Eur Ann Allergy Clin Immunol Vol 50, N 1, 36-41, 2018 S. Büyüköztürk 1, Ç. Kekik 2, A.Z. Gökyiğit 3, F.İ. Tezer Filik 4i, G. Karakaya 4, S. Saygı 4i, A.B. Dursun 5, S. Kirbaş
Discussion. Infection & ER combine meeting. Fever and rash. Fever and rash. Fever and skin rash Measles
 Discussion Infection & ER combine meeting Fever and skin rash Measles Reporter R2 李尚 Supervisor VS 陳威宇洪世文 Date 99/03/20 Fever and rash Age of the patient Season of the year Travel history, Geographic location
Discussion Infection & ER combine meeting Fever and skin rash Measles Reporter R2 李尚 Supervisor VS 陳威宇洪世文 Date 99/03/20 Fever and rash Age of the patient Season of the year Travel history, Geographic location
New product information wording Extracts from PRAC recommendations on signals
 20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
10/25/2018. Autoimmunity and how to treat it. Disclosure. Why do we get autoimmunity? James Verbsky MD/PhD Pediatric Rheumatology/Immunology
 Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Correspondence should be addressed to Wanjarus Roongpisuthipong; rr
 Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
Dermatologic drug reactions
 Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Fever and rash in children. Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program
 Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
DERMATOLOGICAL EMERGENCIES. DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE
, DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE") DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
Drug induced allergy and hypersensitivity
 Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek
 Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek Viral: Exanthema subitum (Roseaola infantum) Herpetic stomatitis Measles Rubella Chickenpox Erythema infectious (5th Disease, Slapped cheec disease)
Infectious diseases Dr n. med. Agnieszka Topczewska-Cabanek Viral: Exanthema subitum (Roseaola infantum) Herpetic stomatitis Measles Rubella Chickenpox Erythema infectious (5th Disease, Slapped cheec disease)
Danger Signs in Drug Hypersensitivity
 Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
CARBAMAZEPINE INDUCED STEVENS JOHNSON SYNDROME- A CASE STUDY
 WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Ragesh SJIF Impact Factor 2.786 Volume 3, Issue 6, 1599-1604. Case Study ISSN 2278 4357 CARBAMAZEPINE INDUCED STEVENS JOHNSON SYNDROME- A CASE STUDY
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES Ragesh SJIF Impact Factor 2.786 Volume 3, Issue 6, 1599-1604. Case Study ISSN 2278 4357 CARBAMAZEPINE INDUCED STEVENS JOHNSON SYNDROME- A CASE STUDY
SJS/TEN spectrum. Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) 10/7/2016
 /Toxic Epidermal Necrolysis (TEN) 10/7/2016") Jesse Keller MD Assistant Professor Oregon Health & Science University Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) Drug induced dermemergencies that exist on a spectrum Delayed reaction:
Jesse Keller MD Assistant Professor Oregon Health & Science University Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) Drug induced dermemergencies that exist on a spectrum Delayed reaction:
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms
 Review Int Arch Allergy Immunol 2016;171:166 179 Published online: December 14, 2016 Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms Werner J. Pichler a Oliver Hausmann
Review Int Arch Allergy Immunol 2016;171:166 179 Published online: December 14, 2016 Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms Werner J. Pichler a Oliver Hausmann
Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course
 Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 12-4-2015 Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course Sharon K. Hart Southern Adventist University,
Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 12-4-2015 Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course Sharon K. Hart Southern Adventist University,
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123
 BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Drug Allergy HSJ 19/09/2011
 Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
Pathomechanism of Severe Drug Allergy
 Pathomechanism of Severe Drug Allergy Werner J. Pichler, MD Division Allergology, RIA, Inselspital, University of Bern, CH 3010 Bern Switzerland ADR-AC GmbH Adverse Drug Reactions Analysis and Consulting
Pathomechanism of Severe Drug Allergy Werner J. Pichler, MD Division Allergology, RIA, Inselspital, University of Bern, CH 3010 Bern Switzerland ADR-AC GmbH Adverse Drug Reactions Analysis and Consulting
EFAVIRENZ ASSOCIATED STEVENS-JOHNSON SYNDROME
 EFAVIRENZ ASSOCIATED STEVENS-JOHNSON SYNDROME To the Editor: Persons with human immunodeficiency virus (HIV) infection are highly susceptible to adverse dermatological reactions to specific medications
EFAVIRENZ ASSOCIATED STEVENS-JOHNSON SYNDROME To the Editor: Persons with human immunodeficiency virus (HIV) infection are highly susceptible to adverse dermatological reactions to specific medications
International Journal of Basic & Clinical Pharmacology. Profile of cutaneous adverse drug reactions of carbamazepine
 Print ISSN: 2319-2003 Online ISSN: 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology DOI: http://dx.doi.org/10.18203/2319-2003.ijbcp20175211 Original Research Article Profile of cutaneous
Print ISSN: 2319-2003 Online ISSN: 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology DOI: http://dx.doi.org/10.18203/2319-2003.ijbcp20175211 Original Research Article Profile of cutaneous
Immunology. Lecture- 8
 Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
DERMATOLOGY FOR THE INTERNIST. Emilie Chow, MD 8/2017
 DERMATOLOGY FOR THE INTERNIST Emilie Chow, MD 8/2017 GOALS ALL SLIDES ARE FOCUSED ON CLINICAL CASES IN THE FORM OF QUESTIONS AND MKSAP COVERED TOPICS USING POLLEV.COM Reference for material is MKSAP 17
DERMATOLOGY FOR THE INTERNIST Emilie Chow, MD 8/2017 GOALS ALL SLIDES ARE FOCUSED ON CLINICAL CASES IN THE FORM OF QUESTIONS AND MKSAP COVERED TOPICS USING POLLEV.COM Reference for material is MKSAP 17
Didactic Series. Primary HIV Infection. Greg Melcher, M.D. UC Davis AETC 8 Nov 2012
 Didactic Series Primary HIV Infection Greg Melcher, M.D. UC Davis AETC 8 Nov 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Primary HIV Infection Greg Melcher, M.D. UC Davis AETC 8 Nov 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital
 Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Infection Control Manual Residential Care Part 3 Infection Control Standards IC6: Additional Precautions
 IC6: 0110 Appendix I Selection Table Infection Control Manual esidential Care IC6: Additional Legend: outine Practice * reportable to Public Health C - Contact ** reportable by Lab D - Droplet A - Airborne
IC6: 0110 Appendix I Selection Table Infection Control Manual esidential Care IC6: Additional Legend: outine Practice * reportable to Public Health C - Contact ** reportable by Lab D - Droplet A - Airborne
International Consensus (ICON) on Drug Allergy
 on Drug Allergy") International Consensus (ICON) on Drug Allergy Allergy 2014; 69: 420 437 Pascal Demoly, N. Franklin Adkinson, Knut Brockow, Mariana Castells, Anca M. Chiriac, Paul A. Greenberger, David A. Khan, David
International Consensus (ICON) on Drug Allergy Allergy 2014; 69: 420 437 Pascal Demoly, N. Franklin Adkinson, Knut Brockow, Mariana Castells, Anca M. Chiriac, Paul A. Greenberger, David A. Khan, David
8/8/2016. Overview. Back to Basics: Immunology. Adverse Reactions to Drugs: Dispelling Myths
 Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Chapter 65 Allergy and Immunology for the Internist. ingestion provoke an IgE antibody response and clinical symptoms in sensitive individuals.
 Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke