Syndrome de Lyell Approche diagnostique. seminaires iris. Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme.
|
|
|
- Aleesha Cunningham
- 5 years ago
- Views:
Transcription

1 Syndrome de Lyell Approche diagnostique Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme Serge Jennes Hôpital Militaire



2 Rash benign



3 Pustulose exanthematique Aigue et généralisée AGEP Benign versus severe DRESS

4 Benign versus severe?



5 Versus severe rash
6 Drug induced Rash The skin is one of the most common targets for adverse drug reactions To determine the cause of the eruption, a logical approach based on clinical characteristics, chronologic factors and a literature search is required Exanthematous eruptions and urticaria are the two most common forms of cutaneous drug reactions
7 Viral versus Drug induced exantheme Viral infection is the most important differential diagnosis. Drugs were responsible for 25% of the exanthems (more commonly in adults) of which antibiotics and NSAIDs were most frequently implicated. It is useful in differentiating exanthematic drug eruptions from viral exanthems to remember that viral rashes tend to start on the face and acral sites with subsequent progression to involve the trunk, and are more often accompanied by fever, sore throat, gastrointestinal symptoms, conjunctivitis, cough and insomnia. Pruritus is typically associated with drug causes in adults.

8 Viral exanthemes
9 Clinical characteristics Type of primary lesion (e.g. urticaria, erythematous papule, pustule, purpuric papule, vesicle or bulla) Distribution and number of lesions Mucous membrane involvement, facial edema Associated signs and symptoms: fever, pruritus, lymph node enlargement, visceral involvement
10 Chronological factors Document all drugs to which the patient has been exposed and the dates of administration Date of eruption Time interval between drug introduction (or reintroduction) and skin eruption Response to removal of the suspected agent Consider excipients (e.g. soybean oil)
11 Benign drug eruption The latency from drug initiation to onset of rash ranges from 5 to 21 days, but typically occurs at 7 10 days. A drug induced exanthem may be accompanied by pruritus. The clinical features are variable; lesions may be scarlatiniform, rubelliform or morbilliform, or may consist of a profuse eruption of small pink papules showing no close resemblance to any infective exanthem. There is a broad spectrum of phenotypes encountered in cutaneous adverse reactions and many can mimic other inflammatory rashes. Rarely, drug hypersensitivity dermatoses can be life threatening and involve internal organs; however, most eruptions are mild, affect the skin only and are self limiting on drug withdrawal. These disorders can be considered as the benign cutaneous adverse reactions
12 Alerting Clinical features Clinical features that can alert the clinician to the possibility of a more severe drug-induced eruption include edema of the face or a marked peripheral blood hypereosinophilia (suggestive of DRESS [DIHS]) mucous membrane lesions or painful or dusky skin, which may announce TEN or SJS
13 Drug reactions including Severe drug reaction acute generalized exanthematous pustulosis (AGEP), Stevens Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) and drug reaction with eosinophilia and systemic symptoms (DRESS) Are severe cutaneous adverse reactions to drugs acknowledged to be dominantly T cell mediated
14 Immunologically Mediated Drug Reactions IgE-dependent drug reactions (formerly type I, Gell Coombs classification): urticaria, angioedema and anaphylaxis. Cytotoxic drug-induced reactions (antibody against a fixed antigen; formerly type II): petechiae secondary to drug-induced thrombocytopenia. Immune complex-dependent drug reactions (formerly type III): vasculitis, serum sickness and certain types of urticaria. Possible delayed-type, cell-mediated drug reactions (formerly type IV; sometimes not well defined) exanthematous, fixed and lichenoid drug eruptions, as well as Stevens Johnson syndrome (SJS) and TEN.

15 Forms of type 4 hypersensitivity reaction: mechanisms and clinical correlations Adapted from Pichler, 2007 Rook textbook of dermatology, 9th edition, 2016
16 Drug reaction Immunologically Mediated Drug Reactions Non-immunologic Mechanisms Overdose Pharmacological effects Cumulative toxicity Delayed toxicity Drug-drug interctaction Alteration in metabolism Exacerbation of disease Idiosyncratic with Possible Immunologic Mediation
17 Idiosyncratic with Possible Immunologic Mediation Idiosyncratic drug eruptions represent reactions that are unpredictable and cannot be explained on the basis of the pharmacologic properties of the drug. Reactive metabolites of drugs can bind covalently to proteins, and the altered protein, considered as foreign, then induces an immune response. However, the way in which a drug is metabolized into a reactive species (or fails to be metabolized) differs in nature and amount depending upon the patient s specific metabolic pathways. These variations are genetically influenced
18 Idiosyncratic with Possible Immunologic Mediation Examples would be the increased incidences of the procainamideinduced systemic lupus syndrome and sulfonamide-induced TEN in slow acetylators as opposed to rapid acetylators. In addition, certain HLA alleles increase the risk of adverse drug reactions, e.g. the association of HLA-B*5701 with hypersensitivity reactions to abacavir and HLA B*1502 with SJS/TEN in Han Chinese. The pathophysiology of drug-induced skin reactions such as exanthematous drug eruptions, DRESS (DIHS), acute generalized exanthematous pustulosis (AGEP) and TEN, as well as the increased susceptibility of HIV-infected patients, may be partially explained by an interplay between immune mechanisms and genetic predisposition.

19 HLA and drug reactions The association of drug induced adverse reactions with particular HLA alleles is increasingly well recognized
 and toxic epidermal necrolysis (TEN)")
 is a distinct disorder with")

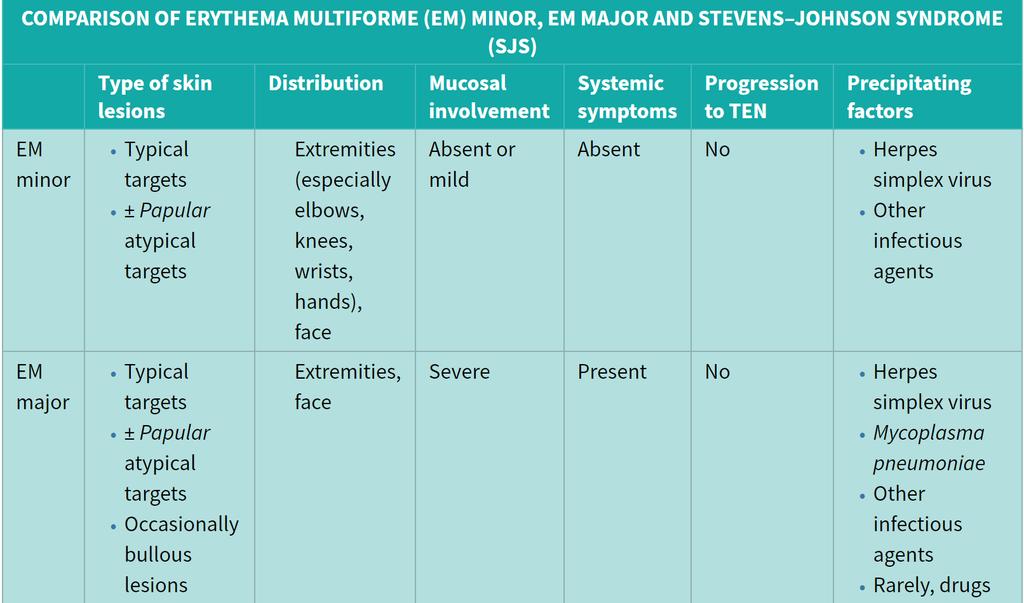
20 Erythema Multiform vs SJS-TEN It has now become clear that Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are variants within a continuous spectrum of adverse drug reactions, Whereas erythema multiforme (EM) is a distinct disorder with different clinical signs and precipitating factors, e.g. herpes simplex virus (HSV) infections. Therefore, EM will be discussed separately from SJS and TEN.


21 The characteristic elementary skin lesion of EM is the typical target lesion. The latter measures <3 cm in diameter, has a regular round shape and a well-defined border, and it consists of at least three distinct zones, The vast majority of lesions appearing within 24 hours Erythema Multiform- Target lesions favor acrofacial sites, but the palms, neck, face and trunk are common locations as well. Involvement of the legs is seen less frequently. EM lesions may also appear within areas of sunburn
22 Erythema Multiform- Minor and Major Erythema multiforme minor: typical and/or occasionally atypical papular target lesions with little or no mucosal involvement and no systemic symptoms Erythema multiforme major: typical and/or occasionally atypical papular target lesions with severe mucosal involvement and systemic features A preceding HSV infection is the most common precipitating factor; occasionally, there are other preceding infections or, rarely, drug exposure Diagnosis of erythema multiforme requires clinicopathologic correlation and is not based solely on histologic findings Erythema multiforme does not carry the risk of progressing to toxic epidermal necrolysis
23

24 Erythema multiform-infection

25 Erythema multiform drugs and others
26 Erythema Multiform- SJS-TEN Differentiation of SJS from erythema multiforme major (EMM) is difficult: In both EMM and SJS, there is mucous membrane involvement and cutaneous blistering with epidermal detachment of less than 10% body surface area (BSA). However, in EMM the lesions consist of typical targets or raised atypical targets, predominantly localized on the limbs and extremities; in SJS, the lesions are atypical targets with predilection for the torso.

27 SJS-Lyell (TEN) Lyell? Rare! 1,89 case for 1 million
28 Etiology : drugs! Risque Excès de risque b relatif Sulfamides antibactériens 172 4,5 Triméthoprime-sulfaméthoxazole 160 4,3 Aminopénicilline 6,7 0,2 Quinolones 10 0,3 Céphalosporines 14 0,4 Tétracyclines 8,1 0,2 Phénobarbital a 45 1,2 Carbamazépine a 90 2,5 Phénytoïne a 53 1,5 Acide valproïque a 25 0,7 AINS oxicams a 72 2,0 Allopurinol a 52 1,5 Chlormézanone a 62 1,7 Corticoïdes a 54 1,5 [a] MÉDICAMENT PRIS PENDANT UNE DURÉE INFÉRIEURE OU ÉGALE À 2 MOIS. [b] NOMBRE DE CAS DE LYELL ATTRIBUABLES À UN MÉDICAMENT PAR MILLION D'UTILISATEURS EN 1 SEMAINE.


29 Physiopathogeny The keratinocyte, major target and actor - The target is the keratinocyte, and more specifically the multistratified epithelium, keratinized or not. Oral cavity, larynx, conjoncitiva, but also trachea and bronchial tree The Continundrun of toxic epidermal necrolysis. G Pierard, P Paquet, S Jennes, C Franchimont The noval biomedical, 2015-Nova Sciences publishers, Inc -White K, Chung WH, et al, J Allergy Clin Immunol, 2015


30 Physiopathogeny Exfoliation is due to extensive death of keratinocytes via apoptosis; Appears to be a MHC-I restricted specific drug sensitivity resulting in clonal expansion of CD8 cytotoxic Lymphocytes The latter is mediated via the cytotoxic secretory proteins perforin granzyme and granulysin, and interaction of the death receptor ligand pair Fas FasL Fas Ligand is likely to be particularly important, and TNF contributes via the TNF receptor
31 Clinical diagnosis? Mucosal involvment Nikolski Sign Atypical targets Purpuric macules Palmoplantar lesions Confluent erythema



32 Nikolsky sign In SJS/TEN, lesional necrolytic epidermis readily peels back to reveal the dermis

33 There are multiple discrete red macules each has a darker centre and a slightly paler outer ring Atypical targets

34 The dusky, purpuric lesions on this patient's skin are coalescing and blistering. Purpuric macules

 the palms and (b)")

35 Palmo plantar lesions Palmoplantar involvement. Multiple circular lesions are present on(a) the palms and (b) the soles. Blistering is occurring at both sites, but prominently on the feet.


36 Confluent erythema. Individual lesions may coalesce to form large areas of erythema, Confluent Erytema




37 Mucosal involvment Eye eyelid oedema, conjunctivitis and keratitis Urogenital symptoms During the acute phase, urogenital pain is prominent and urinary dysfunction (dysuria or retention) is common.

38 Mucosal involvment Lips oral cavity oropharynx,
39 Clinical manifestations Brutal opening with Non specific symptoms: Pseudo-grippal syndrom which can appear before cutaneous symptoms Mucosal symptoms that appears first (90%) : Erosions/ulcérations which appears 1 to 3 days before cutaneous manifestations for 1/3 of the patients Cutaneous manifestation : confluent macular rash in the presternal region and the face appearing in 2 to 5 days with vesiculae and flat bullae ( sign of the wet laudry) wet Nikolsky sign The association of cutaneous rash and mucosal symptoms should induce an urgent histological confirmation! Harr T and French L, Orphanet, J of Rare Diseases, 2010, S: 39
40 Diagnostic procedure Classical histology? Histology with immediate cryosection? Classical histology, with cryosection and direct immunofluresence?
41 Diagnostic procedure Classical histology? Biopsy with immediate cryosection? Classical histology, with cryosection and direct immunofluorescence
42 Diagnostic procedure Histology with immediate cryosection : skin biopsy sample sent on physiological serum that will be immediately preceded on the cryo section Classical histology : a good sample and be able to identify the infiltrate Direct immunofluresce : to complete the differential diagnosis
43 Differential diagnosis SJS and TEN should also be distinguished from dermatoses such as Staphylococcal scalded skin syndrome, Generalized fixed drug eruption, drug-induced Linear IgA bullous dermatosis, Toxic erythema of chemotherapy, and acute generalized exanthematous pustulosis, As their management and prognosis are also quite different.


44 SJS SJS-TEN- TEN
45 Prise en charge: Arbre décisionnel d après Mo Ellis MW et al. Mil Med 2002;167:701-4
46 Historique!! Beningn rash versus severe Approche clinique-diagnostique Antecedents? Début de la localisation du rash, Type de rash? Aspect circiné? Pustules, fragilité cutanée? Atteinte muqueuse,..? Origine infectieuse? virale? les identifier via l anamnese, vérifier la présence de vésicules,..herpes? Mycoplasme? Médicaments? Même occasionnels, infections précédemment? Signes généraux? Fièvre, arthralgies, état général Biologie : lymphocytose, éosinophilie, atteinte hépatique,..
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
Skin Manifestations of Drug Reactions
 Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Drug Allergy A Guide to Diagnosis and Management
 Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Herbal and homeopathic products, often considered natural and non-toxic, can also cause adverse drug reactions.
 Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
GOOD MORNING! AUGUST 5, 2014
 GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
Danger Signs in Drug Hypersensitivity
 Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
AOU Ospedali Riuniti - Ancona
 AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
DERMATOLOGIC EMERGENCIES. Mary Evers D.O., F.A.O.C.D. Georgetown, Texas
 DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
Cutaneous drug reactions
 Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW
 SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
Pathophysiology of autoimmune and allergic diseases. Hypersensitivity reactions type II type IV
 Pathophysiology of autoimmune and allergic diseases Hypersensitivity reactions type II type IV Audrey NOSBAUM, Florence HACARD, Marc VOCANSON, Frédéric BERARD, Jean François NICOLAS Allergologie et Immunologie
Pathophysiology of autoimmune and allergic diseases Hypersensitivity reactions type II type IV Audrey NOSBAUM, Florence HACARD, Marc VOCANSON, Frédéric BERARD, Jean François NICOLAS Allergologie et Immunologie
Cutaneous Conditions Associated with Systemic Disease
 Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
Toxic Epidermal Necrolysis and SJS : Case Reports & Brief Review
 Case Report Toxic Epidermal Necrolysis and SJS : Case Reports & Brief Review Deepali P. Mohite*, Satyajitraje Tekade*, Amol Gadbail*, M. S. Chaudhary** Abstract : Toxic epidermal necrolysis (TEN) and Stevens
Case Report Toxic Epidermal Necrolysis and SJS : Case Reports & Brief Review Deepali P. Mohite*, Satyajitraje Tekade*, Amol Gadbail*, M. S. Chaudhary** Abstract : Toxic epidermal necrolysis (TEN) and Stevens
Dilantin (phenytoin) ROBERT A. SCHWARTZ
 ROBERT A. SCHWARTZ") Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
An Evidenced-Based Approach to the Adult with a Morbilliform Eruption
 Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Mechanisms of Drug Hypersensitivity Reactions
 18/5/213 Mechanisms of Drug Hypersensitivity Reactions Munir Pirmohamed NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology Institute of Translational Medicine University of
18/5/213 Mechanisms of Drug Hypersensitivity Reactions Munir Pirmohamed NHS Chair of Pharmacogenetics Department of Molecular and Clinical Pharmacology Institute of Translational Medicine University of
Adverse drug reactions
 Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
Medications William Smith Adverse drug reactions Allergy? Side-effect? Intolerance? Background Adverse drug reactions (ADRs) vary from life-threatening anaphylaxis to minor common side-effects. Objective
Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions
 Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions Bernard A. Cohen, M.D. Johns Hopkins Children s Center Baltimore, Maryland (NO disclosures)
Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions Bernard A. Cohen, M.D. Johns Hopkins Children s Center Baltimore, Maryland (NO disclosures)
Five things not to miss in Dermatology. Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine
 Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Big rashes in little patients:
 ! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
Emergency Dermatology. Emergency Dermatology
 Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome
 Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
Skin Manifestations of Systemic Disease. Approach to Dermatalogic Diagnosis 9/6/2016. Go Ahead---Judge a Book by its Cover!
 Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions
 PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases
 10.5005/jp-journals-10011-1189 CASE REPORT JIAOMR Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases 1 M Venkateshwarlu, 2 B Radhika 1 Professor and Head, Department
10.5005/jp-journals-10011-1189 CASE REPORT JIAOMR Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases 1 M Venkateshwarlu, 2 B Radhika 1 Professor and Head, Department
A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive Patients
 Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Bugs and Drugs: What s New in Hypersensitivity Reactions?
 Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening
 CMAJ Cases Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening Suran L. Fernando MB BS PhD, Andrew J. Broadfoot MB BS Previously published at www.cmaj.ca
CMAJ Cases Prevention of severe cutaneous adverse drug reactions: the emerging value of pharmacogenetic screening Suran L. Fernando MB BS PhD, Andrew J. Broadfoot MB BS Previously published at www.cmaj.ca
Visual Diagnosis: A Review of Pediatric Rashes
 Visual Diagnosis: A Review of Pediatric Rashes Frank J. Sloan, MD FAAP Emergency Services Department Thank you to VisualDX for allowing the use of their images for educational purposes. 1 Modern Medicine
Visual Diagnosis: A Review of Pediatric Rashes Frank J. Sloan, MD FAAP Emergency Services Department Thank you to VisualDX for allowing the use of their images for educational purposes. 1 Modern Medicine
allergy Asia Pacific Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from
 pissn -876 eissn -868 Original Article Asia Pac Allergy 6;6:-7 Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from 9 Oki Suwarsa *, Wulan
pissn -876 eissn -868 Original Article Asia Pac Allergy 6;6:-7 Stevens-Johnson syndrome and toxic epidermal necrolysis in Dr. Hasan Sadikin General Hospital Bandung, Indonesia from 9 Oki Suwarsa *, Wulan
A Middle-Aged Man with Newly Diagnosed HIV Infection and Rash
 CLINICAL CASE OF THE MONTH A Middle-Aged Man with Newly Diagnosed HIV Infection and Rash Patrick Njoku, MD; Temeka Tate, MD; Sousan Zadeh, MD; Erin Hauck, MD; Anila Chaudhry, MD; Betty Lo-Blais, MD; Lee
CLINICAL CASE OF THE MONTH A Middle-Aged Man with Newly Diagnosed HIV Infection and Rash Patrick Njoku, MD; Temeka Tate, MD; Sousan Zadeh, MD; Erin Hauck, MD; Anila Chaudhry, MD; Betty Lo-Blais, MD; Lee
Drug induced allergy and hypersensitivity
 Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
Drug induced allergy and hypersensitivity Yunita Sari Pane, Aznan Lelo Dept. Pharmacology & Therapeutic School of Medicine Universitas Sumatera Utara 13 Mei 2009, KBK-FK USU, Medan Drug Allergy Adverse
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD
 CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
New product information wording Extracts from PRAC recommendations on signals
 12 October 2017 EMA/PRAC/610988/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 25-29 September 2017
12 October 2017 EMA/PRAC/610988/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 25-29 September 2017
Objectives 8/30/2012. How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Adverse Drug Reactions
 Drug Allergies? Adverse Drug Reactions") How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
International Consensus (ICON) on Drug Allergy
 on Drug Allergy") International Consensus (ICON) on Drug Allergy Allergy 2014; 69: 420 437 Pascal Demoly, N. Franklin Adkinson, Knut Brockow, Mariana Castells, Anca M. Chiriac, Paul A. Greenberger, David A. Khan, David
International Consensus (ICON) on Drug Allergy Allergy 2014; 69: 420 437 Pascal Demoly, N. Franklin Adkinson, Knut Brockow, Mariana Castells, Anca M. Chiriac, Paul A. Greenberger, David A. Khan, David
Bacterial Infections in Pediatric Dermatology. Patrick McMahon, MD Children s Hospital of Philadelphia
 Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course
 Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 12-4-2015 Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course Sharon K. Hart Southern Adventist University,
Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 12-4-2015 Stevens Johnson Syndrome: How Diagnosis Impacts Disease Course Sharon K. Hart Southern Adventist University,
8/8/2016. Overview. Back to Basics: Immunology. Adverse Reactions to Drugs: Dispelling Myths
 Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
International Journal of Basic & Clinical Pharmacology. Profile of cutaneous adverse drug reactions of carbamazepine
 Print ISSN: 2319-2003 Online ISSN: 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology DOI: http://dx.doi.org/10.18203/2319-2003.ijbcp20175211 Original Research Article Profile of cutaneous
Print ISSN: 2319-2003 Online ISSN: 2279-0780 IJBCP International Journal of Basic & Clinical Pharmacology DOI: http://dx.doi.org/10.18203/2319-2003.ijbcp20175211 Original Research Article Profile of cutaneous
OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT
 OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT Lung-Chang Lin, 1,2 Ping-Chin Lai, 3 Sheau-Fang Yang, 4 and Rei-Cheng Yang 1,5 Departments of 1 Pediatrics and 4 Pathology, Kaohsiung Medical
OXCARBAZEPINE-INDUCED STEVENS-JOHNSON SYNDROME: A CASE REPORT Lung-Chang Lin, 1,2 Ping-Chin Lai, 3 Sheau-Fang Yang, 4 and Rei-Cheng Yang 1,5 Departments of 1 Pediatrics and 4 Pathology, Kaohsiung Medical
Lecture 03: Drug allergy
 Lecture 03: Drug allergy 1. Basic Information Author: Netherlands Pharmacovigilance Centre Lareb Version date: 17 Nov 2017 Content: This hand-out describes Drug allergy and provides background information
Lecture 03: Drug allergy 1. Basic Information Author: Netherlands Pharmacovigilance Centre Lareb Version date: 17 Nov 2017 Content: This hand-out describes Drug allergy and provides background information
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES. R e g i S C A R PATIENT'S DATA. Age country of birth
 REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
VARICELLA. Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara
 VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
Cutaneous drug eruptions are seen commonly
 REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center
 Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
BJD. Summary. British Journal of Dermatology THERAPEUTICS
 THERAPEUTICS BJD British Journal of Dermatology Drug reaction with eosinophilia and systemic symptoms: is cutaneous phenotype a prognostic marker for outcome? A review of clinicopathological features of
THERAPEUTICS BJD British Journal of Dermatology Drug reaction with eosinophilia and systemic symptoms: is cutaneous phenotype a prognostic marker for outcome? A review of clinicopathological features of
New product information wording Extracts from PRAC recommendations on signals
 20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
DERMATOLOGICAL EMERGENCIES. DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE
, DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE") DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
Drug Allergy: A Rash ionale for Treatment
 Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes
 Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Genetic susceptibility for Stevens-Johnson syndrome/toxic epidermal necrolysis with mucosal involvements
 249 Special Issue: Inflammation in Ophthalmology Review Article Genetic susceptibility for Stevens-Johnson syndrome/toxic epidermal necrolysis with mucosal involvements 1, 2, ) Mayumi Ueta 1) Department
249 Special Issue: Inflammation in Ophthalmology Review Article Genetic susceptibility for Stevens-Johnson syndrome/toxic epidermal necrolysis with mucosal involvements 1, 2, ) Mayumi Ueta 1) Department
Managing Penicillin Allergy
 Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Exanthematous drug eruptions
 Exanthematous drug eruptions Werner J. Pichler, M.D. Clinc for Rheumatology and clinical Immunology/Allergology, Inselspital, University of Bern Switzerland E-mail: werner.pichler@insel.ch Disclosure slide
Exanthematous drug eruptions Werner J. Pichler, M.D. Clinc for Rheumatology and clinical Immunology/Allergology, Inselspital, University of Bern Switzerland E-mail: werner.pichler@insel.ch Disclosure slide
Adverse Drug Reactions (ADRs) Outline
 Outline") Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
STEVENS-JOHNSON SYNDROME: A CASE REPORT
 STEVENS-JOHNSON SYNDROME: A CASE REPORT Castana O., Rempelos G., Anagiotos G., Apostolopoulou C., Dimitrouli A., Alexakis D. Department of Plastic and Reconstructive Surgery, Evangelismos General Hospital,
STEVENS-JOHNSON SYNDROME: A CASE REPORT Castana O., Rempelos G., Anagiotos G., Apostolopoulou C., Dimitrouli A., Alexakis D. Department of Plastic and Reconstructive Surgery, Evangelismos General Hospital,
Correspondence should be addressed to Wanjarus Roongpisuthipong; rr
 Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
The mechanisms of common drug hypersensitivities and implications for testing
 The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Dermatologic drug reactions
 Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Package leaflet: Information for the user
 Package leaflet: Information for the user Dalacin C 150mg Capsules clindamycin hydrochloride PFIZER Read all of this leaflet carefully before you start taking this medicine because it contains important
Package leaflet: Information for the user Dalacin C 150mg Capsules clindamycin hydrochloride PFIZER Read all of this leaflet carefully before you start taking this medicine because it contains important
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
Hospital-based Dermatopathology. Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM
 Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving
 Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Bacteria: Scarlet fever, Staph infection (sepsis, 4S,toxic shock syndrome), Meningococcemia, typhoid Mycoplasma Rickettsial infection
, Meningococcemia, typhoid Mycoplasma Rickettsial infection") Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
Exanthematous Fever objectives FEVER WITH RASH 1 Determine the feature of skin rashes 2 Enumerate the most common causes of skin rashes in children (measles, chicken pox, rubella,erythema infectiosum,
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update
 Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
DERMATOLOGY FOR THE INTERNIST. Emilie Chow, MD 8/2017
 DERMATOLOGY FOR THE INTERNIST Emilie Chow, MD 8/2017 GOALS ALL SLIDES ARE FOCUSED ON CLINICAL CASES IN THE FORM OF QUESTIONS AND MKSAP COVERED TOPICS USING POLLEV.COM Reference for material is MKSAP 17
DERMATOLOGY FOR THE INTERNIST Emilie Chow, MD 8/2017 GOALS ALL SLIDES ARE FOCUSED ON CLINICAL CASES IN THE FORM OF QUESTIONS AND MKSAP COVERED TOPICS USING POLLEV.COM Reference for material is MKSAP 17
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Citation The Journal of Dermatology, 37(8), available at
, available at") NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
Cutaneous Reactions to Drugs in Children
 REVIEW ARTICLE Cutaneous Reactions to Drugs in Children Alissa R. Segal, PharmD, PhC a, Kevin M. Doherty, PharmD b, John Leggott, MD c, Barrett Zlotoff, MD d a Department of Pharmacy Practice, Massachusetts
REVIEW ARTICLE Cutaneous Reactions to Drugs in Children Alissa R. Segal, PharmD, PhC a, Kevin M. Doherty, PharmD b, John Leggott, MD c, Barrett Zlotoff, MD d a Department of Pharmacy Practice, Massachusetts
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg Tablets sodium fusidate Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg Tablets sodium fusidate Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India.
 Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
9/9/17. Disclosures" Dermatology in Primary Care: Recognition and treatment of common disorders of the skin" A preview" Classic skin infections"
 Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
SEVERE CUTANEOUS ADVERSE DRUG REACTIONS: STEVENS-JOHNSON SYNDROME AND TOXIC EPIDERMAL NECROLYSISA, A REPORT OF 4 CASES SEEN AT UMMC
 SEVERE CUTANEOUS ADVERSE DRUG REACTIONS: STEVENS-JOHNSON SYNDROME AND TOXIC EPIDERMAL NECROLYSISA, A REPORT OF 4 CASES SEEN AT UMMC Shasha Khairullah, Rokiah Che Ismail Department of Medicine, Faculty
SEVERE CUTANEOUS ADVERSE DRUG REACTIONS: STEVENS-JOHNSON SYNDROME AND TOXIC EPIDERMAL NECROLYSISA, A REPORT OF 4 CASES SEEN AT UMMC Shasha Khairullah, Rokiah Che Ismail Department of Medicine, Faculty
Erythema Multiforme with Reference to Atypical Presentation in an HIV-Positive Patient Following Antiretroviral Therapy Discontinuation
 2009;17(1):9-15 CLINICAL ARTICLE Erythema Multiforme with Reference to Atypical Presentation in an HIV-Positive Patient Following Antiretroviral Therapy Discontinuation Liborija Lugović Mihić, Marija Buljan,
2009;17(1):9-15 CLINICAL ARTICLE Erythema Multiforme with Reference to Atypical Presentation in an HIV-Positive Patient Following Antiretroviral Therapy Discontinuation Liborija Lugović Mihić, Marija Buljan,
What's New in Oncodermatopathology: Immunotherapy Reactions
 What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
TOXIC EPIDERMAL NECROLYSIS AND CLARITHROMYCIN
 TOXIC EPIDERMAL NECROLYSIS AND CLARITHROMYCIN Nadia Khaldi 1, Alain Miras 1, Sophie Gromb 1,2 1 Forensic Science Laboratory, Pellegrin Hospital, University Teaching Hospital Bordeaux, France, 2 Forensic
TOXIC EPIDERMAL NECROLYSIS AND CLARITHROMYCIN Nadia Khaldi 1, Alain Miras 1, Sophie Gromb 1,2 1 Forensic Science Laboratory, Pellegrin Hospital, University Teaching Hospital Bordeaux, France, 2 Forensic
건강한성인에서의오진하기쉬운포도구균성열상피부증후군의치험례. Staphylococcal Scalded Skin Syndrome in a Healthy Adult: Easy to Misdiagnose
 Archives of Hand and Microsurgery Arch Hand Microsurg 2018;23(4):271-276. https://doi.org/10.12790/ahm.2018.23.4.271 pissn 2586-3290 eissn 2586-3533 Case Report 건강한성인에서의오진하기쉬운포도구균성열상피부증후군의치험례 김홍일ㆍ곽찬이ㆍ박언주
Archives of Hand and Microsurgery Arch Hand Microsurg 2018;23(4):271-276. https://doi.org/10.12790/ahm.2018.23.4.271 pissn 2586-3290 eissn 2586-3533 Case Report 건강한성인에서의오진하기쉬운포도구균성열상피부증후군의치험례 김홍일ㆍ곽찬이ㆍ박언주
Pathomechanism of Severe Drug Allergy
 Pathomechanism of Severe Drug Allergy Werner J. Pichler, MD Division Allergology, RIA, Inselspital, University of Bern, CH 3010 Bern Switzerland ADR-AC GmbH Adverse Drug Reactions Analysis and Consulting
Pathomechanism of Severe Drug Allergy Werner J. Pichler, MD Division Allergology, RIA, Inselspital, University of Bern, CH 3010 Bern Switzerland ADR-AC GmbH Adverse Drug Reactions Analysis and Consulting
Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms
 Review Int Arch Allergy Immunol 2016;171:166 179 Published online: December 14, 2016 Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms Werner J. Pichler a Oliver Hausmann
Review Int Arch Allergy Immunol 2016;171:166 179 Published online: December 14, 2016 Classification of Drug Hypersensitivity into Allergic, p-i, and Pseudo-Allergic Forms Werner J. Pichler a Oliver Hausmann
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg/5 ml Oral Suspension fusidic acid Read all of this leaflet carefully before you start taking this medicine because it contains important information
PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg/5 ml Oral Suspension fusidic acid Read all of this leaflet carefully before you start taking this medicine because it contains important information
An unpredictable, dose-independent adverse drug reaction which is immunologically or IgEmediated.
 R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
Goals of this talk. Morbilliform. Common Morphologies in the Hospital 11/7/2017. Hospital Based Dermatology: Common and Tough Consult Cases
 Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Case No. 5; Slide No. B13/8956/2
 Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review
 Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Case Reports and Images (IJCRI) Type of Article: Case Report Title: A Case
: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Case Reports and Images (IJCRI) Type of Article: Case Report Title: A Case
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3