Chronic pancreatitis an increasing Indian Problem
|
|
|
- Joel Harvey
- 5 years ago
- Views:
Transcription
1 Chronic pancreatitis an increasing Indian Problem Dr Ramesh Ardhanari M.S; MCh.(SGE); FRCS (Hon)(G) Medical Director, Sr. Consultant & Head Dept. of Surgical Gastroenterology Meenakshi Mission Hospital,Madurai Past President Association of Minimal Access Surgeons India President Elect Indian Association of Surgical Gastroenterology
2 Disclosure On the Speaker s Bureau of Ethicon Endosurgery Covidien Stryker Karl Storz Olympus
3 Some history Alexander the Great Cawley (1788) described a thirty four year old free living man with several corporeal exertions who died of diabetes and emaciation and at necropsy had pancreas studded with calculi Friedrich (1878) called this drunkard s pancreas
4 Introduction Pancreatitis is an inflammation of glandular parenchyma leading to injury or possibly irreversible destruction of acinar components. This inflammation can Self limited disease which may even be subclinical Acute disease leading to systemic manifestations and life threatening complications Chronic form with fibrosis, calcification and organ insufficiency and irreversible damage to function.
5 The development of CP depends upon the Host Environment (Toxin and cofactors) In every patient each may contribute to varying levels.
6 Toxic and Metabolic (A, N Alcohol and Nicotine) Most common cause of chronic pancreatitis in Western countries. (Alcohol : 50 60%; Smoking : 25 30%) Average threshold 80 g/day (40 g/day in women) for 5 years. It has been demonstrated that acute attacks precede the development of chronic disease. Necrosis and pseudocyst formation are more common.
7 Cofactors in alcohol induced pancreatitis genetics, smoking, intestinal infection, high-fat diet, compromised immune function, gallstones, gender, hormonal factors, and drinking patterns
8 Role of smoking Independently associated with increased risk of chronic pancreatitis (OR 17.3). Smoking cessation reduces the risk by 50% Pathway Increases oxidative stress (UGT1A7 mutation) Alters the secretion and composition of the pancreatic juice Causes inflammation
9 Others Hypercalcemia as a result of primary or secondary hyperparathyroidism. Calcium increases trypsinogen activation, increases intraductal stone formation, Modifies pancreatic secretion leading to increased protein plug formation.
10 Idiopathic As there is greater research this category is expected to shrink in the future. Most common cause in INDIA and CHINA. Mutations of SPINK1 gene may contribute to 25% of these patients. Bimodal age of distribution early onset and late onset.
11 Indian type or idiopathic Early onset Within the first two decades, with considerable delay (around 13 years) in onset of diabetes and exocrine insufficiency. Late onset Higher proportion of organ insufficiency which appears earlier (<5 years). Pain is uniformly present in both the groups
12 Genetic causes early activation or failure to inhibit the activated enzyme SPINK1-N34S gene mutation found to be positive in nearly 42% patients of idiopathic chronic pancreatitis in INDIA. The progression of CP is faster in patients with SPINK-N34S mutation than in patients with PRSS1 mutations
13 Recurrent and Severe Acute Pancreatitis recurrent attacks precipitated by genetic, hereditary, anatomic (pancreas divisum, pancreatic duct stenosis), functional (sphincter of Oddi dysfunction), toxic (alcohol, nicotine), and microlithiasis of the bile ducts
14 Obstructive (E - Efferent Duct Factors) scars of the pancreatic duct, tumors of the ampulla of Vater, mucinous duct ectasia, tumors of head of the pancreas, trauma sphincter of Oddi dysfunction pancreas divisum,
15 Obstructive causes Obstructive factors can lead to stagnation and stone formation of pancreatic juice (stone and duct obstruction theory) acute recurrent pancreatitis and periductular fibrosis (necrosis-fibrosis theory) a form of compartment syndrome, due to decreased tissue compliance and increased interstitial pressures
16 Pathogenesis Necrosis-Fibrosis Hypothesis Protein-Plug (Stone/Ductal Obstruction) Hypothesis Oxidative Stress Theory Toxic-Metabolic Theory Primary Duct Hypothesis Sentinel Acute Pancreatitis Event Hypothesis Sustained Intraacinar Nuclear Factor-κB Activation
17
18 INDIAN perspective Recently, Bal Krishnan et al reported on 1,086 patients hailing from all parts of the country. Idiopathic pancreatitis was the most common form 60.2% followed by alcoholic pancreatitis 38.7%. Only 3.8% patients could be clubbed under the traditional banner of tropical chronic pancreatitis.
19 Present status of TCP First described by Zuidema from Indonesia. Geevarghese described a large series of pancreatic diabetes in association with malnutrition from Kerala state. Based on observations in the 1960s and 1970s predominantly in the Indian subcontinent
20 Classical clinical description a child, adolescent or young adult, who presented with recurrent upper abdominal pain, often with diabetes mellitus had signs of malnutrition, cyanotic hue of the lips, bilateral enlargement of parotid glands, a pot belly and, sometimes, nutritional edema. Demonstration of high blood sugar level and of pancreatic calculi 90% of patients required insulin, aggressive course of the disease vis-à-vis development of pancreatic cancer
21 Changing scenario Malnutrition is an effect and not a cause of idiopathic CP, cassava is not an aetiology SPINK1 gene mutation is associated with TCP in approximately 40% of cases phenotype (incidence of DM, requirement of insulin) of Indian patients with ICP is somewhat similar to that reported from other countries prognosis of ICP is good both in regards to the pain relief and survival
22 TCP a misnomer? This change may be due to changing socioeconomic scenario of our country Tropical pancreatitis has a geographical rather than etiological connotation idiopathic CP in India has a strong genetic predisposition prognosis is good with the majority of patients experiencing pain relief and reasonably good life expectancy
23 Clinical manifestations CP may be asymptomatic over long periods of time and can then present with exacerbations. Abdominal pain is the commonest symptom. It is epigastric in position radiating to the back. Generally presents about minutes. Early on, it occurs in discreet intervals, later on it becomes continuous. In very late burnout phase, pain reduces. Change in character of pain, especially cessation should raise suspicion of malignancy.
24 Exocrine insufficiency generally comes only after 90% of the gland has been destroyed. Steatorrhea occurs prior to protein insufficiency as lipolysis is affected more. Also deficiency of Vit A, D, E, K, B12 may be seen. Endocrine Patients with calcifying disease develop DM more than noncalcifying patients. This diabetes generally requires insulin for treatment. Also since α cells are affected there is increased chance of hypoglycemia.
25 Weight loss is caused by two factors: at first, patients fear eating because of the accompanying pain weight loss results from malabsorption related to pancreatic insufficiency Having said that any recent change in the character of symptoms including appearance of new ones warrants investigations to rule out malignancy
26 Stage Pain CLINICAL PICTURE Complications Morphology Pancreatic Function Diagnostics A: Early Recurrent acute attacks No complications Morphologic changes detectable with imaging procedures directed to pancreatic parenchyma and ductal system Normal pancreatic endocrine and exocrine function EUS, ERP/MRP, CT, secretin B: Moderate Increasing number of attacks and increased intensity Pseudocysts, cholestasis, segmental portal hypertension Progredient morphologic changes detectable in several imaging procedures Impairment of pancreatic function in several degrees, but rarely steatorrhea Transabdominal US, ERP/MRP, EUS, CT, fasting blood glucose, oral glucose tolerance test C: Advanced Decreasing pain ( burnout of the pancreas) Pseudocysts, cholestasis, segmental portal hypertension Calculi Marked impairment of pancreatic function, more often steatorrhea than in other stages; diabetes mellitus Transabdominal US, ERP/MRP, CT, FE-1, fasting blood glucose, oral glucose tolerance test
27 Diagnosis of CP In advanced stages the diagnosis is easy, but it is challenging in the early stages. Laboratory investigations such as amylase and lipase are of limited use as they are neither diagnostic nor therapeutic. For many years, the gold standard for diagnosing CP has been ERCP, but now EUS has largely supplanted ERCP as the imaging method of choice.
28 Comparison of various modalities Imaging Method Sensitivity (%) Specificity (%) Transabdominal ultrasound Computed tomography Endoscopic retrograde pancreatography Endoscopic ultrasound
29 USG Diagnostic criteria for CP irregular contour (lobulation), pancreatic duct dilation and irregularity of the main pancreatic duct, loss or reduction of pancreatic parenchyma echogenicity (echo-poor or echo-rich areas), cysts or cavities, pancreatic calcifications
30 Computed Tomography After oral and i.v. administration of contrast medium, the pancreas can be completely visualized with spiral CT using a slice thickness of 5 mm. most sensitive method to detect calculi early stages of CP can be easily missed. It is important to differentiate CP from pancreatic cancer, a task that may be challenging. CT is useful as an initial radiologic test and is helpful to visualize calcifications and duct abnormalities, to exclude complications and other, non-cp etiologies for pain or weight loss
31 favor CP are intraductal or parenchymal calcifications, lack of obstructing mass, irregular dilation of the pancreatic duct, relatively limited atrophy of the gland favor neoplasia include pancreatic duct dilation with associated mass at the site of obstruction, with associated atrophy of the pancreas, vascular invasion, metastases


32 Calculi in the MPD

33 Chronic calcific pancreatitis with a mass
34 ERP Endoscopic retrograde pancreatography (ERP) is the gold standard among all imaging methods for diagnosis and staging of CP, because it has 90% sensitivity and 100% specificity in diagnosis era of high-quality imaging tests such as CT and MRI/MRCP, the role of ERP for the diagnosis of CP has greatly decreased. Currently, ERP is mainly used as a therapeutic tool in patients with CP and its complications invasive method with a low but important rate of post-erp pancreatitis in 3% to 7% of patients
35 Cambridge Criteria of Chronic Pancreatitis (1984) Stage Normal Equivocal Mild Moderate Severe Typical Changes Normal appearance of side branches and main pancreatic duct Dilation or obstruction of less than three side branches; normal main pancreatic duct Dilation or obstruction of more than three side branches; normal main pancreatic duct Additional stenosis and dilation of main pancreatic duct Additional obstructions, cysts, and stenosis of main pancreatic duct; calculi

36 Dilated MPD

37 MPD communicating with pseudocysts in head

38 Deployment of bumpy stent
39 EUS Endoscopic ultrasonography (EUS) visualizes both the pancreatic ducts and the parenchyma The main disadvantage is that, there is often relatively poor interobserver agreement for EUS, even among expert endosonographers, which limits the diagnostic accuracy and overall utility of EUS for diagnosing CP
40 EUS Milwaukee Criteria of Chronic Pancreatitis Parenchymal Features Gland size, cysts Echo-poor lesions (focal areas of reduced echogenicity) Echo-rich lesions >3 mm in diameter Accentuation of lobular pattern Ductal Features Increased duct wall echogenicity Narrowing or dilation (main pancreatic duct, side branches) Calculi
41 Magnetic Resonance Imaging and Cholangiopancreatography More sensitive for the diagnosis of CP than CT or US. MRI/MRCP detects early parenchymal changes of CP and ductal abnormalities. Use of secretin-stimulated MRI/MRCP provides a dynamic test to characterize the pancreatic duct and pancreatic parenchyma. Useful to detect early parenchymal changes suggestive of CP, such as abnormal decreased signal intensity on fat-suppressed T1-weighted images and delayed or limited enhancement after gadolinium administration


42 MRI with MPD calculi MRI in pancreatic divisum
43 Treatment The goals of treatment include pain management, correction of pancreatic insufficiency, and management of complications The natural history of chronic pancreatitis cannot be altered by any specific procedure/agent, all treatment is in a sense palliative
44 Pain management Source of pain pancreatic hyper stimulation, ischemia and acidosis, obstruction of larger or small ducts, inflammation or neuropathic mechanisms The first step in alleviating pain is to recognize the underlying cause of chronic pancreatitis and to treat the underlying etiology to reduce progressive pancreatic damage.
45 Step wise approach Cessation of alcohol intake Imperative, particularly if this is the underlying etiology of pancreatitis. Patients continue drinking have increased mortality. Small meals and hydration Small meals that are low in fat may help. Keeping patients well hydrated may help prevent flares of pancreatitis. Supplementation with medium chain triglycerides (MCTs) and hydrolyzed peptides, resulted in improvement in pain, which in some patients was sustained after stopping this oral supplement. This mixture resulted in a minimal increase in plasma CCK levels. Cessation of smoking


46 Enzyme supplements Suppresses pancreatic exocrine secretion by breaking the feedback loop to relieve pain in some patients. High doses of the non-enteric coated enzymes were used in the clinical trials. They should also be treated with acid suppression. Generally about 10% of pancreatic lipase is sufficient prevent steatorrhea.
47 Analgesia A short course of opiates coupled with low dose amitriptyline (10 mg nightly for three weeks to determine efficacy) and a NSAID will break the pain cycle. Chronic opioid analgesia may be required in patients with persistent significant pain - morphine sulfate continuous release or fentanyl patches; pregabalin has been shown to be effective in some trials.
48 Antioxidant therapy Conflicting evidence A trial from AIIMS shows positive results. The antioxidant supplementation included daily doses of 600 g organic selenium, 0.54 g ascorbic acid, 9000 IU -carotene, 270 IU - tocopherol and 2 g methionine. After 6 months, the reduction in the number of painful days per month was significantly higher in the antioxidant group compared with the placebo group.
49 Endoscopy The rationale for this approach is based upon the hypothesis that ductal hypertension due to sphincter of Oddi dysfunction or strictures of the main pancreatic duct lead to pain. Decompressing an obstructed pancreatic duct can be associated with pain relief in some patients. A small RCT found that surgical drainage was more effective in relieving obstruction and achieving pain relief however many centers use endoscopy as first line.
50 Recommendations Patients with proximal stenosis and no calcifications or inflammatory mass may be treated endoscopically. If two to three repetitive endoscopic treatments fail, the option of surgery must be evaluated. In patients with distal duct obstruction, calcifications, or local complications, surgery is superior to endoscopic treatment. Pancreatic pseudocysts may be treated endoscopically. If endoscopic treatment fails, a surgical drainage procedure is recommended.
51 Options Interventional External Drainage Indications Temporary treatment infected pseudocyst Frequently followed by definitive surgical treatment if internal drainage is not possible Internal Drainage Effective therapy of pseudocysts Endoscopic cystogastrostomy/endoscopic cystoduodenostomy If anatomically possible: less invasive than surgery Problems with recurrence and catheter dislocation Endoscopic Ductal Drainage ept ept + dilation + stenting of pancreatic duct ept + lithotripsy and stone extraction ept + bile duct stenting Pancreas divisum, sphincter of Oddi dysfunction Proximal stenosis of PD Pancreatolithiasis Bile duct stenosis Caution: Poor outcome of endoscopic treatment if: Distal stenosis of pancreatic duct Parenchymal calcifications
52 ESWL No clear role, no definite trials. ESWL is used mostly in Europe. Many patients with stones (even with ductal dilation) are asymptomatic, while those with symptoms generally have pain due to small duct obstruction and other factors such as parenchymal inflammation and ischemia.
53 Surgery Surgery has generally been considered for patients who fail medical therapy, or as first line therapy if there is suspicion of pancreatic cancer. Upto 15 percent of patients in surgical series had unrecognized pancreatic cancer at the time of the procedure Three broad types decompression/drainage operations pancreatic resections denervation procedures
54 Indications for Surgery in Chronic Pancreatitis Intractable pain Symptomatic local complications Unsuccessful endoscopic management Suspicion of malignancy
55 Decompression procedures Patients with refractory pain who have a dilated main pancreatic duct The data suggest that short-term pain relief is achieved in approximately 80 percent of patients. Morbidity and mortality related to the operation are generally low when the procedure has been performed by experienced surgeons (0 to 5 percent).

56 Freys procedure

57 Stone extraction and head coring

58 Completed head coring

59 Pancreaticojejunostomy in progress
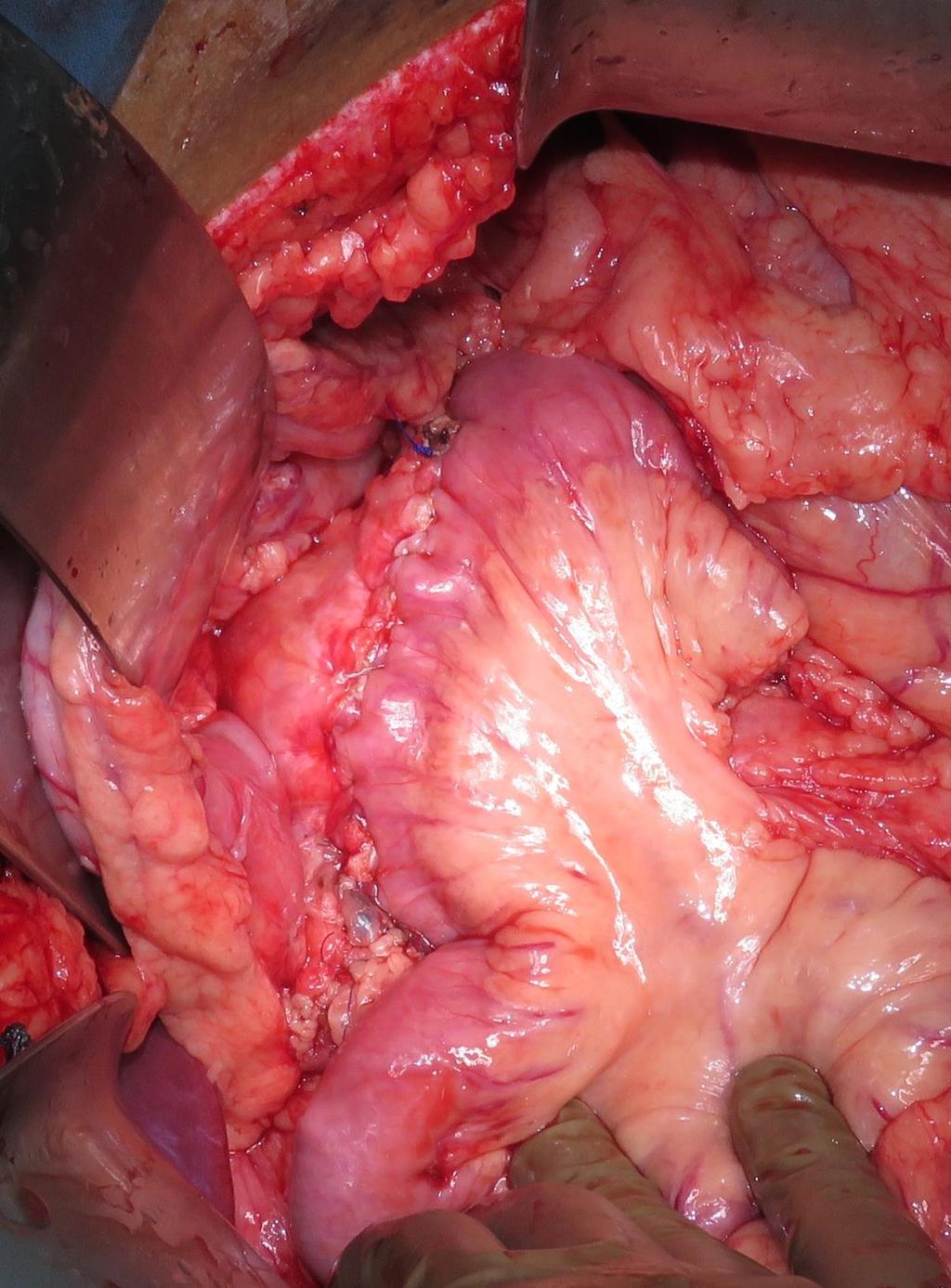
60 Completed pancreatojejunostomy
61 Resection Vast majority of patients are seen with a ductal obstruction in the pancreatic head, frequently associated with an inflammatory mass. In these patients, pancreatic head resection is the procedure of choice. In patients with small-duct disease (diameter of the pancreatic duct <3 mm) and no mass in the pancreatic head, a V-shaped excision of the anterior aspect of the pancreas is a safe approach, with effective pain management
62 Surgical Techniques Indications and Recommendations Pure Drainage Operations Surgical procedure of choice for isolated pseudocysts Cystojejunostomy Caution: Intraoperative frozen section to exclude a cystic neoplasm! Laterolateral pancreaticojejunostomy Ductal dilation > 7 mm, without inflammatory mass Partington-Rochelle procedure Caudal drainage: Puestow-procedure Rare indications, replaced by other procedures Resection Procedures Pancreatic head resections PD and pppd DPPHR Techniques DPPHR, Beger V-shaped excision Segmental resection Total pancreatectomy Always include a ductal drainage Procedures of choice if inflammatory mass in the head of the pancreas All techniques have comparable results Procedure of choice in suspected malignancy and in irreversible duodenal stenosis Caution: Intraoperative frozen section to exclude malignancy! Procedures of choice if inflammatory mass in the head of the pancreas Small-duct disease (diameter of pancreatic duct < 3 mm) Rare cases, e.g., isolated ductal stenosis in the body (e.g., posttraumatic) in patients without diabetes Rare cases with severe changes in the entire pancreas and preexisting IDDM
63 Our data See 150 new cases of CP yearly Operate about 55 cases annually now Total operated cases are now over 1000 We see an incidence of 6% of cancer in operated cases Mortality of surgery is 1 case in 25 years
64 Our data We prefer to do head coring with Roux en Y lateral pancreaticojejunostomy. On long term follow up we have seen that surgery basically has a role in pain relief, about 70% of the patients are completely pain free and another 20 %have reduced frequency and intensity. There is no change in the progression of the disease i.e., incidence diabetes mellitus in the patients is not changed About 2-3% patients develop benign CBD stricture after surgery which may require a hepaticojejunostomy.
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Prof. (DR.) MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet
 MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet") Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
CLASSIFICATION OF CHRONIC PANCREATITIS
 CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Diseases of pancreas - Chronic pancreatitis
 Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Chronic Pancreatitis
 Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Magnetic resonance cholangiopancreatography (MRCP) is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,
 is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,") SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Chronic Pancreatitis
 Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Treatment of chronic calcific pancreatitis endoscopy versus surgery
 Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION
 IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018
 Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018 This document is only a SHORT PREVIEW of the Medifocus Guidebook on Chronic Pancreatitis. It is intended primarily to give
Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018 This document is only a SHORT PREVIEW of the Medifocus Guidebook on Chronic Pancreatitis. It is intended primarily to give
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
What Is Pancreatitis?
 What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Evidence based imaging of the pancreas
 Evidence based imaging of the pancreas D.Vanbeckevoort, D.Bielen, K.Op de beeck, R.Vanslembrouck Department of Radiology Chairman Prof. Dr. R.Oyen Non-invasive imaging tests available for the diagnosis
Evidence based imaging of the pancreas D.Vanbeckevoort, D.Bielen, K.Op de beeck, R.Vanslembrouck Department of Radiology Chairman Prof. Dr. R.Oyen Non-invasive imaging tests available for the diagnosis
Causes of pancreatic insufficiency. Eugen Dumitru
 Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Chronic Pancreatitis: Surgical Options. W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA
 Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
Chronic Pancreatitis: Surgical Options W. Charles Conway MD, FACS Upper GI/HPB Surgical Oncology Ochsner Medical Center New Orleans, LA Chronic Pancreatitis Recurrent, debilitating abdominal pain with
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Diseases of exocrine pancreas
 Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
New developments in diagnosis and non-surgical treatment of chronic pancreatitis
 bs_bs_banner doi:10.1111/jgh.12250 NUTRITIONAL FACTORS IN PANCREATOBILIARY DISORDERS New developments in diagnosis and non-surgical treatment of chronic pancreatitis Kazuo Inui, Junji Yoshino, Hironao
bs_bs_banner doi:10.1111/jgh.12250 NUTRITIONAL FACTORS IN PANCREATOBILIARY DISORDERS New developments in diagnosis and non-surgical treatment of chronic pancreatitis Kazuo Inui, Junji Yoshino, Hironao
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
CHAPTER TWENTY-EIGHT. Chronic pancreatitis INTRODUCTION PATHOGENESIS SECTION FIVE MANAGEMENT OF PANCREATICOBILIARY DISORDERS
 Ch028-V.qxd 30/3/05 4:38 PM Page 1 SECTION FIVE MANAGEMENT OF PANCREATICOBILIARY DISORDERS 28 CHAPTER TWENTY-EIGHT Chronic pancreatitis Julia Mayerle and Markus M. Lerch INTRODUCTION Definition of chronic
Ch028-V.qxd 30/3/05 4:38 PM Page 1 SECTION FIVE MANAGEMENT OF PANCREATICOBILIARY DISORDERS 28 CHAPTER TWENTY-EIGHT Chronic pancreatitis Julia Mayerle and Markus M. Lerch INTRODUCTION Definition of chronic
Virtual MR Pancreatoscopy in the Evaluation of the Pancreatic Duct in Chronic Pancreatitis
 MULTIMEDIA ARTICLE - Videoclips Virtual MR Pancreatoscopy in the Evaluation of the Pancreatic Duct in Chronic Pancreatitis Rakesh Kalapala 1, Lingareddy Sunitha 2, Reddy D Nageshwar 1, Guduru V Rao 1,
MULTIMEDIA ARTICLE - Videoclips Virtual MR Pancreatoscopy in the Evaluation of the Pancreatic Duct in Chronic Pancreatitis Rakesh Kalapala 1, Lingareddy Sunitha 2, Reddy D Nageshwar 1, Guduru V Rao 1,
ESPEN Congress Brussels 2005
 ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Chronic Pancreatitis
 Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
Index (SIRS), 158, 173
, 158, 173") Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
Index A Acute pancreatitis surgery abdominal compartment syndrome, 188 adjuvant treatment, 194 anterior approach, 175 antibiotic prophylaxis, 166 167, 197 Atlanta classification, 181 classification of
PANCREATITIS: MEDICAL AND TRANSPLANT CONSIDERATIONS, DHIRAJ YADAV, MD 1
 DHIRAJ YADAV, MD 1 Good afternoon. This is actually an interesting time of the day to do pancreas topic since you just had lunch and this is the time when the pancreas is the most active with a lot of
DHIRAJ YADAV, MD 1 Good afternoon. This is actually an interesting time of the day to do pancreas topic since you just had lunch and this is the time when the pancreas is the most active with a lot of
Etiology of chronic pancreatitis I. ALCOHOL Long-term alcohol abuse: Men 80g, women 40-50g/day for years Fatty food, coffee, smoking, concent
 Chronic pancreatitis Definition: Chronic pancreatitis Irreversible destruction of parenchyma Increase of the amount of connective tissue Signs of inflammation Signs of regeneration Decrease of exocrine
Chronic pancreatitis Definition: Chronic pancreatitis Irreversible destruction of parenchyma Increase of the amount of connective tissue Signs of inflammation Signs of regeneration Decrease of exocrine
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome
 PancreasFest 2017 Precision Medicine Approach For Benign Pancreatic Disease Friday, July 28, 2017 Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome David C Whitcomb MD PhD Director,
PancreasFest 2017 Precision Medicine Approach For Benign Pancreatic Disease Friday, July 28, 2017 Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome David C Whitcomb MD PhD Director,
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated.
 A-Z of medical words This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated. Absorption: once your food has been broken down,
A-Z of medical words This page explains some of the medical words that you may hear when you are finding out about pancreatic cancer and how it is treated. Absorption: once your food has been broken down,
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
Nutrition in Pancreatic Disease Topic 14
 Nutrition in Pancreatic Disease Topic 14 Module 14.2 Chronic Pancreatitis Learning objectives Johann Ockenga, MD, Prof. Dep. of Gastroenterology, Endocrinology & Nutrition, Klinikum Bremen Mitte, St. Juergensstrasse
Nutrition in Pancreatic Disease Topic 14 Module 14.2 Chronic Pancreatitis Learning objectives Johann Ockenga, MD, Prof. Dep. of Gastroenterology, Endocrinology & Nutrition, Klinikum Bremen Mitte, St. Juergensstrasse
A study of 50 cases in different modalities of treatment of chronic pancreatitis
 Different modalities of treatment of chronic pancreatitis Original Research Article ISSN: 2394-0026 (P) A study of 50 cases in different modalities of treatment of chronic pancreatitis Jayesh Gohil, Pallav
Different modalities of treatment of chronic pancreatitis Original Research Article ISSN: 2394-0026 (P) A study of 50 cases in different modalities of treatment of chronic pancreatitis Jayesh Gohil, Pallav
Autoimmune Pancreatitis: A Great Imitator
 Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Y A L E S C H O O L O F M E D I C I N E. This is a CME accredited activity. The presenters and there are no conflicts of interest.
 This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol
 Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Does Sphincter of Oddi Dysfunction Even Exist Anymore?
 Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Patient characteristics Intervention Comparison Length of follow-up. Endoscopic treatment. Endoscopic transampullary drainage of the pancreatic duct
 1) In patients with alcohol-related, what is the safety and efficacy of a) coeliac access block vs medical management b) thoracoscopic splanchnicectomy vs medical management c) coeliac access block vs
1) In patients with alcohol-related, what is the safety and efficacy of a) coeliac access block vs medical management b) thoracoscopic splanchnicectomy vs medical management c) coeliac access block vs
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Acute And Chronic Pancreatitis
 Acute And Chronic Pancreatitis Objectives: At the end of this lecture the student will be able to: Recognize the predisposing factors of pancreatitis. Describe the different types of pancreatitis. Understand
Acute And Chronic Pancreatitis Objectives: At the end of this lecture the student will be able to: Recognize the predisposing factors of pancreatitis. Describe the different types of pancreatitis. Understand
Case Report (1) Sphincter of Oddi Dysfunction. Case Report (3) Case Report (2) Case Report (4) Case Report (5)
 Sphincter of Oddi Dysfunction. Case Report (3) Case Report (2) Case Report (4) Case Report (5)") Dr David Westaby Imperial NHS Trust Imperial College Medical School London Case Report (1)! TD 33yr old male! Feb May 2010: Recurrent episodes of abdominal pain! June 2010 Episode severe abdominal pain
Dr David Westaby Imperial NHS Trust Imperial College Medical School London Case Report (1)! TD 33yr old male! Feb May 2010: Recurrent episodes of abdominal pain! June 2010 Episode severe abdominal pain
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram
 Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE
 ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
Yoshitsugu; Kanematsu, Takashi; Kur
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Clinical Profile of Idiopathic Chronic Pancreatitis in North India
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:594 599 Clinical Profile of Idiopathic Chronic Pancreatitis in North India DEEPAK K. BHASIN,* GURSEWAK SINGH,* SURINDER S. RANA,* SHOKET M. CHOWDRY,* NUSRAT
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:594 599 Clinical Profile of Idiopathic Chronic Pancreatitis in North India DEEPAK K. BHASIN,* GURSEWAK SINGH,* SURINDER S. RANA,* SHOKET M. CHOWDRY,* NUSRAT
PANCREATITIS. By April McMurray. March 14, 2013 NDFS 356
 PANCREATITIS By April McMurray March 14, 2013 NDFS 356 INTRODUCTION The pancreas is a small gland that sits behind the stomach and plays an important role in digestion (1). Its head is situated within
PANCREATITIS By April McMurray March 14, 2013 NDFS 356 INTRODUCTION The pancreas is a small gland that sits behind the stomach and plays an important role in digestion (1). Its head is situated within
SPHINCTER OF ODDI DYSFUNCTION (SOD)
") SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Surgical management of chronic pancreatitis: Our institutional experience
 Quest Journals Journal of Medical and Dental Science Research Volume 3~ Issue 1 (2016) pp:01-09 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Surgical management
Quest Journals Journal of Medical and Dental Science Research Volume 3~ Issue 1 (2016) pp:01-09 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Surgical management
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
A Wide Variation in Diagnostic and Therapeutic Strategies in Chronic Pancreatitis: A Dutch National Survey
 JOP. J Pancreas (Online) 212 Jul 1; 13(4):394-41. ORIGINAL ARTICLE A Wide Variation in Diagnostic and Therapeutic Strategies in Chronic Pancreatitis: A Dutch National Survey Aura AJ van Esch 1, Usama Ahmed
JOP. J Pancreas (Online) 212 Jul 1; 13(4):394-41. ORIGINAL ARTICLE A Wide Variation in Diagnostic and Therapeutic Strategies in Chronic Pancreatitis: A Dutch National Survey Aura AJ van Esch 1, Usama Ahmed
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
D DAVID PUBLISHING. Groove Pancreatitis: A Case Report. 1. Introduction. 2. Case Report
 Journal of Pharmacy and Pharmacology 6 (2018) 415-419 doi: 10.17265/2328-2150/2018.04.013 D DAVID PUBLISHING Luciana Leony Valente, Mariama Alves Dantas Fagundes, Camila Medrado Pereira Barbosa, Hélio
Journal of Pharmacy and Pharmacology 6 (2018) 415-419 doi: 10.17265/2328-2150/2018.04.013 D DAVID PUBLISHING Luciana Leony Valente, Mariama Alves Dantas Fagundes, Camila Medrado Pereira Barbosa, Hélio
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Chronic pancreatitis is characterized by continued inflammation
 Diagn Interv Radiol 2011; 17:249 254 Turkish Society of Radiology 2011 ABDOMINAL IMAGING REVIEW MRI assessment of chronic pancreatitis Cem Balcı ABSTRACT Magnetic resonance imaging (MRI) plays an important
Diagn Interv Radiol 2011; 17:249 254 Turkish Society of Radiology 2011 ABDOMINAL IMAGING REVIEW MRI assessment of chronic pancreatitis Cem Balcı ABSTRACT Magnetic resonance imaging (MRI) plays an important
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
MRI Abdomen Protocol Pancreas/MRCP with Contrast
 MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
MRI Abdomen Protocol Pancreas/MRCP with Contrast Reviewed By: Brett Mollard, MD; Anna Ellermeier, MD Last Reviewed: July 2018 Contact: (866) 761-4200 Standard uses: 1. Characterization of cystic and solid
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification