Kidney disease in people with diabetes. Ian Gallen
|
|
|
- Alexandra Grant
- 5 years ago
- Views:
Transcription
1 Kidney disease in people with diabetes Ian Gallen
2 Why is it important Major cause of early death in DM Major cause of amputation RRT is arduous for the patient and expensive Nephropathy is largely avoidable (or can be delayed) Local performance is poor compared with national data
3 Increased risk of renal replacement therapy for people with diabetes in Berkshire West (E+W average is 164%) CCG Excess over not diabetic Excess number of people Newbury 106% +7 Wokingham 247% +16 South Reading 198% +35 North and West Reading 181% +15
4 Key message Nephropathy in type Type 1 diabetes Nearly always due to hyperglycaemia Strong genetic predisposition Nephropathy in T2DM May be due to hyperglycaemia But often due to other causes particularly inflammation Frequently multi-factorial
5 Diabetic Nephropathy Diabetic kidney disease is defined by characteristic structural and functional changes. The predominant structural changes include mesangial expansion, glomerular basement membrane thickening, and glomerular sclerosis. The major clinical manifestations of diabetic nephropathy are albuminuria, hypertension and less often haematuria, and, in many patients, progressive chronic kidney disease, which can be slowed or prevented with optimal therapy. Diabetic nephropathy can occur in all forms of diabetes mellitus when the duration of diabetes is long-enough and level of glycaemia high enough to result in complications.
6 Pathology There are three major histologic changes in the glomeruli in diabetic nephropathy: mesangial expansion; glomerular basement membrane thickening; glomerular sclerosis (the Kimmelstiel-Wilson lesion) Other changes seen are hyaline deposits in the glomerular arterioles (infiltration of plasma proteins such as fibrin, albumin, immunoglobulins, and complement into the vascular wall) The mesangial expansion and glomerulosclerosis do not always develop in parallel, suggesting that they may have somewhat different underlying pathogenesis

7 A and B Glomerulus showing only mild ischemic changes C, D Class II glomeruli with mild and moderate mesangial expansion, respectively. E and F Kimmelstiel Wilson lesion. G is an example of glomerulosclerosis that does not reveal its cause
8 Epidemiology in T1DM Approximately 20 to 30 percent will have microalbuminuria, after a mean duration of diabetes of 15 years Less than half of these patients will progress to overt nephropathy Microalbuminuria may regress or remain stable with good glycaemicand BP control with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs). With intensive glycaemic control and the use of ACE inhibitors and ARBs to control BP, patients diagnosed with type 1 diabetes have lower rates of overt nephropathy and renal failure. The onset of overt nephropathy in type 1 diabetes is typically between 10 and 15 years after the onset of the disease. Those patients who have no proteinuria after 20 to 25 years have a low risk of developing overt renal disease.
9 Epidemiology int2dm The prevalence of progressive renal disease is lower in type 2 diabetes than in type 1 disease, but is higher in some ethnic groups. UKPDS data shows that at 10 years following diagnosis, the prevalence of moderately increased albuminuria, severely increased albuminuria, and either an elevated plasma creatinine concentration (defined as 175 micromol/l [2.0 mg/dl]) or requirement for renal replacement therapy was 25, 5, and 0.8 percent, respectively. The yearly rate of progression from diagnosis to moderately increased albuminuria, from moderately increased albuminuria to severely increased albuminuria, and from severely increased albuminuria to an elevated plasma creatinine concentration or renal replacement therapy was 2.0, 2.8, and 2.3 percent. Median time spent in each stage without progression to another nephropathy stage was 19, 11, and 10 years for those with no nephropathy, moderately increased albuminuria, and severely increased albuminuria, respectively. An creatinine >175 micromol/l]) required renal replacement therapy after a median period of only 2.5 years. This rate of progression is now slower with appropriate therapy (eg, angiotensin inhibition and rigorous blood pressure control)
10 Mechanism of diabetic kidney disease Glomerular hyperfiltration Hyperglycemia and Advanced Glycation products Hyperglycaemia may directly induce mesangial expansion and injury, perhaps in part via increased matrix production or glycation of matrix proteins Glycation of tissue proteins causes diabetic nephropathy and other microvascular complications by forming irreversible advanced glycation end products (AGEs). Activation of protein kinase C Activation of cytokines, profibrotic elements, inflammation, and vascular growth factors (vascular endothelial growth factor, VEGF)
11 Aetiolgy Results from hyperglycemia, advanced glycosylation products, and activation of cytokines. Inflammatory medium, resulting in activation of the innate immune system, which results in activation of the nuclear transcription factors-kappa B (NF-κB), and release of inflammatory mediators, including, interleukin (IL) 1β and tumor necrosis factor (TNF) α. Hyperglycemia also increases the expression of transforming growth factor-β (TGF-β) in the glomeruli and of matrix proteins, specifically stimulated by this cytokine. TGF-β and vascular endothelial growth factor (VEGF) may contribute to the cellular hypertrophy and enhanced collagen synthesis and may induce the vascular changes observed in persons with diabetic nephropathy. Hyperglycemia also may activate protein kinase C, which may contribute to renal disease and other vascular complications of diabetes. Familial or perhaps even genetic factors also play a role. Certain ethnic groups, particularly African Americans, persons of Hispanic origin, and American Indians, may be particularly disposed to renal disease as a complication of diabetes. Some evidence has accrued for a polymorphism in the gene for angiotensin-converting enzyme (ACE) in either predisposing to nephropathy or accelerating its course.

12 Formation and effect of advanced glycation endproduct Normal Protein Function None Time
13 Genetic risk of diabetic nephropathy Genetic susceptibility is an important determinant of both the incidence and severity of diabetic nephropathy with markedly increased in patients with a diabetic sibling or parent who has diabetic nephropathy. The likelihood of the offspring developing overt proteinuria was 14 percent if neither parent had proteinuria, 23 percent if one parent had proteinuria, and 46 percent if both parents had proteinuria. Proposed genes are The angiotensin-converting enzyme (ACE) gene genotype as a potential genetic risk factor with conflicting data: In patients with type 2 diabetes, the DD polymorphism has been associated with an increased risk for the development of diabetic nephropathy. In type 1 diabetes there is strong correlation between genetic variation in the ACE gene and the development of nephropathy T The angiotensin-ii type 2 receptor gene (AT2) on the X-chromosome is associated in males. The aldose reductase gene, the rate-limiting enzyme for the polyol pathway. Variants of the PKCb1 gene have been associated with kidney disease in Chinese patients
14 Other risks for diabetic nephropathy Duration of diabetes Blood pressure Prospective studies have noted an association between the subsequent development of diabetic nephropathy and higher systemic pressures Poor glycaemic control Diabetic nephropathy is more likely to develop in patients with worse glycaemic control Ethnicity The incidence and severity of diabetic nephropathy are increased in African/Afro-carribean (3- to 6-fold compared to Caucasians), Mexican-Americans, and Pima Indians with type 2 diabetes. This observation in such genetically disparate populations suggests a primary role for socioeconomic factors, such as diet, poor control of hyperglycemia, hypertension, and obesity Obesity A high body mass index (BMI) has been associated with an increased risk of chronic kidney disease among patients with diabetes Smoking Smoking is associated with a variety of adverse effects in patients with diabetes Oral contraceptives
15 Key question in diagnosis Does the patient have any symptoms or do they feel completely well? Diabetic nephropathy is commonly a completely asymptomatic condition until the patient has quite advanced renal impairment and it is therefore essential that annual screening by measuring Us and Es and performing urinalysis for microalbuminuria are undertaken. How long has the patient had diabetes? In general, the longer the patient has had diabetes the greater the risk of complications although this is a guide and it is possible to have had diabetes for only a few years and already developed complications (especially so for T2DM). Conversely, some patients can have diabetes for many decades and develop few or any complications. Does the patient have other microvascular complications? The presence of other microvascular complications such as retinopathy and neuropathy increases risks of nephropathy, Patients without other microvascular complications can develop nephropathy. How good has the glycaemic control been over the years? If there is a long history of poor glycaemic control with chronically high HbA1c then development of microvascular complications such as nephropathy is likely
16 Albuminuria Microalbuminuria Hyperfiltration in very early disease (primarily in type 1 diabetes); moderately increased albuminuria, or "microalbuminuria" (defined as urinary albumin excretion between 30 and 300 mg/day or between 30 and 300 mg/g creatinine on a random urine sample) Macroalbuminuria Is increased albuminuria, (defined as urinary albumin excretion above 300 mg/day or above 300 mg/g creatinine on a random urine sample). Moderately increased albuminuria precedes the development of severely increased albuminuria and is considered to be a finding that predicts high risk for future nephropathy. The onset of severely increased albuminuria is followed by a slowly progressive decline in glomerular filtration rate (GFR) and, given enough time, end-stage renal disease Note some people with diabetes can have progressive kidney disease with little albuminuria
17
18 Work-up to confirm DN Urinalysis Persistent albuminuria (>300 mg/d or >200 μg/min) that is confirmed on at least 2 occasions 3-6 months apart Blood Tests Serum and Urinary Electrophoresis Serum and urinary electrophoresis is performed mainly to help exclude multiple myeloma (in the appropriate setting) and to classify the proteinuria (which is predominantly glomerular in diabetic nephropathy). Renal Ultrasonography Observe for kidney size, which is usually normal to increased in the initial stages and, later, decreased or shrunken with chronic renal disease. Rule out obstruction. Renal Biopsy Renal biopsy is not routinely indicated in all cases of diabetic nephropathy, especially in persons with a typical history and a progression typical of the disease. It is indicated if the diagnosis is in doubt, if other kidney disease is suggested, or if atypical features are present. Histologic Findings Mesangial expansion is directly induced by hyperglycemia, perhaps via increased matrix production or glycosylation of matrix proteins. Thickening of the glomerular basement membrane (GBM) occurs. Glomerular sclerosis.

19
20 Drug History It is essential to ensure that a patient with deteriorating renal function is not on potentially nephrotoxic drugs such as non steroidal anti inflammatory agents. If there has been a sudden step-wise deterioration in renal function check changes in medication or X-ray contrast invsetigations egfr is <30 ml/min, metformin therapy should be withdrawn.
21 General Management Salt restriction Reducing dietary salt intake to less than 5-6 g/d and phosphorus and potassium restriction in advanced cases. Weight loss Bariatric surgery Smoking Cessation
22 Glycaemic control In persons with either type 1 or type 2 diabetes mellitus (DM), hyperglycemia has been shown to be a major determinant of the progression of diabetic nephropathy. The evidence is best reported for type 1 DM. Intensive therapy can partially reverse glomerular hypertrophy and hyperfiltration, delay the development of microalbuminuria, and stabilize or even reverse microalbuminuria. Pancreatic transplant recipients in whom true euglycaemia is restored suggest that strict glycaemic and metabolic control may slow the progression rate of progressive renal. Intensive blood glucose control in patients with type 2 DM significantly increased treatment costs but substantially reduced the cost of complications and increased the time free of complications. Kidney Int. Jun 1995;47(6): [Medline]. Lancet. Sep ;352(9131): [Medline].
23 Dipeptidyl peptidase inhibitors Sitagliptin-Approximately 80% of sitagliptin is cleared by the kidney; therefore, the standard dose of 100 mg daily should be reduced in patients with reduced glomerular filtration rates (GFRs). With an estimated GFR (egfr) of 30 or greater to less than 50 ml/min/1.73 m 2, the recommended dose is 50 mg once daily, and with an egfr less than 30 ml/min/1.73 m 2, a dose of 25 mg once daily is advised. Saxagliptin is mg daily in patients with an egfr greater than 50 ml/min, but dose adjustment is recommended in patients with an egfr of 50 ml/min/1.73 m 2 or less to 2.5 mg daily. Alogliptin also requires a dose reduction from 25 mg daily to 12.5 mg daily in patients with an egfr of less than 60 ml/min/1.73 m 2 and to 6.25 mg daily if the egfr is less than 30 ml/min/1.73 m 2. Linagliptin-no dose adjustment is necessary in patients with a reduced GFR. [21] Diabetes Care. Jul 2007;30(7): Expert Opin Drug Metab Toxicol. May 2013;9(5):
24 Sodium-glucose 2 (SGLT2) inhibitors Canagliflozin dose in patients with an egfr of 45 to less than 60 ml/min/1.73 m 2 is 100 mg once daily and it is not recommended in patients with an egfr of less than 45 ml/min/1.73 m 2. Dapagliflozin not recommended in patients with an egfr of less than 60 ml/min/1.73 m 2. Empagliflozin egfr of 45 to less than 60 ml/min/1.73 m 2 is 100 mg once daily and it is not recommended in patients with an egfr of less than 45 ml/min/1.73 m 2.
25 Glucagonlike peptide-1 (GLP-1) agents Exenatide clearance is GFR dependent and is reduced at low GFRs. GLP1 should be used with caution in patients with a GFR of ml/min and not be used at all if the egfr is less than 30 ml/min. Liraglutide is not metabolized by the kidney, and no dose adjustment is necessary in patients with a decreased GFR, including ESRD, although data in this population are limited. ABCD audit shows Liraglutide safe and effective with egfr>30 ml/min Br J Clin Pharmacol. Sep 2007;64(3): Endocr Pract. May-Jun 2011;17(3): Practical Diabetes 2013; 30(2): 71 76
26 RAS in T2DM RENAALStudy and IDNT demonstrated that angiotensin II receptor blockers (ARBs) are superior to conventional therapy and amlodipine in slowing the progression of overt nephropathy. No head-to-head comparison of ACE inhibitors and ARBs. MICRO-HOPE, ramipril reduced the risk for myocardial infarction, stroke, or cardiovascular death by 26% after 2 years. Combined treatment with ACE inhibitors and ARBs significantly decreased blood pressure, proteinuria, and rate of change of reciprocal serum creatinine however, higher cardiovascular death was reported among the olmesartan-treated patients compared with placebo. Hyperkalemia was more frequent in the olmesartan treated group than in the placebo group. Nephron-D trial, which evaluated the effect of adding losartan, an ARB, to the ACE inhibitor lisinopril on albumin-to-creatinine ratio in 1448 patients with type 2 diabetes was stopped early because of safety concerns. Combination therapy significantly increased the risk of hyperkalemia and acute kidney injury. Thus, the combination should be avoided as a strategy to reduce proteinuria with the hope of slowing progression of diabetic nephropathy, and should be reserved for individual situations in which optimal control of blood pressure may require it.
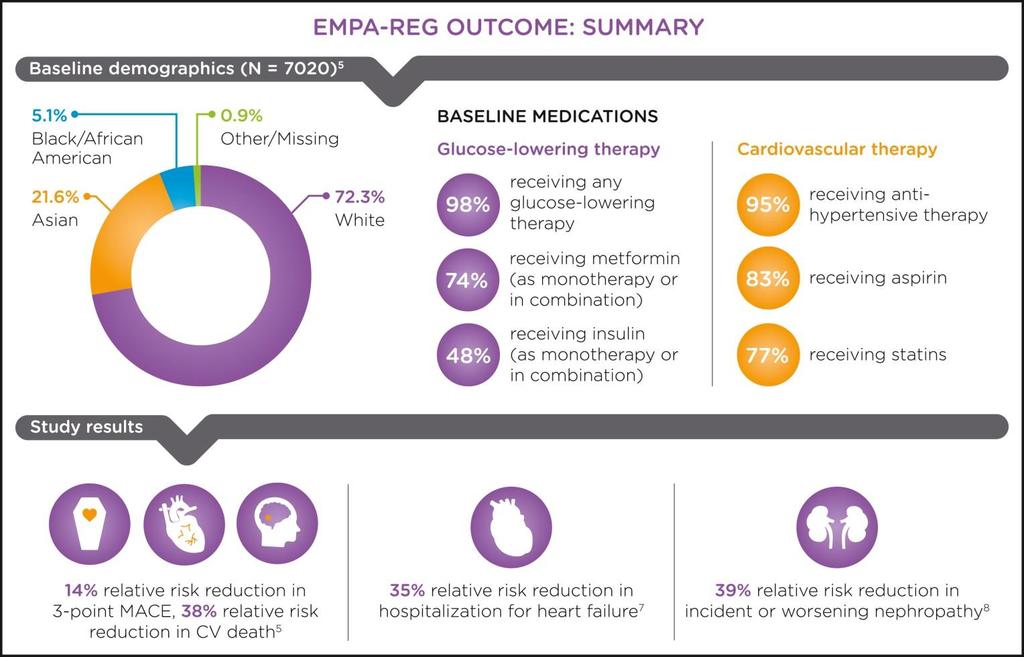
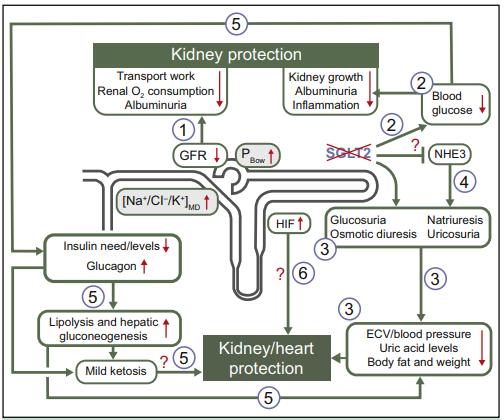
27 Dulaglutide protects against declining Renal function
28
29
30
31
32 Management of Hypertension Progression of kidney disease is best achieved with a blood pressure control. Long-term treatment with ACE inhibitors, usually combined with diuretics, reduces blood pressure and albuminuria and protects kidney function in patients with hypertension, type 1 DM, and nephropathy. ACE inhibition has been shown to delay the development of diabetic nephropathy. The beneficial effect of ACE inhibition on preventing progression from microalbuminuria to overt diabetic nephropathy is long-lasting (8 y) and is associated with the preservation of a normal glomerular filtration rate (GFR). Treatment with an ACE inhibitor for 12 months has significantly reduced mean arterial blood pressure and the urinary albumin excretion rate in type 2 DM patients who have microalbuminuria. ACE inhibitors are superior to beta-blockers, diuretics, and calcium channel blockers in reducing urinary albumin excretion in normotensive and hypertensive type 1 and type 2 DM patients. In addition to beneficial cardiovascular effects, ACE inhibition has also been demonstrated to have a significant beneficial effect on the progression of diabetic retinopathy and on the development of proliferative retinopathy.
33 Measures for Prevention of Diabetic Nephropathy Efforts should be made to modify and/or treat associated risk factors such as hyperlipidemia, smoking, and hypertension. Optimal blood glucose control (hemoglobin A 1c [HbA 1c ] < 7%) Control of hypertension (BP < 120/70 Hg) Avoidance of potentially nephrotoxic substances such as nonsteroidal anti-inflammatory medications and aminoglycosides Early detection and optimal management of diabetes, especially in the setting of family history of diabetes
34 Therapeutic targets Glycaemic targets Inidividualised targets should be set with each patient. A target of 6.5% (48 mmol/mol) without experiencing unacceptably frequent hypoglycaemia is a realistic aim. However, for a 75-year-old patient with a ten-year history of T2DM and an HbA1c of 9% (75 mmol/mol), attempting reduction to 6.5% (48 mmol/mol) will probably confer no survival advantage and may even increase mortality rate as shown by the recent ADVANCE, ACCORD and VADT trials. Caution in the elderly and those with frequent hypoglycaemia and hypoglycaemia unawareness and those who have had diabetes for many decades and have developed autonomic neuropathy, gastroparesis and other comorbidity that render coping with hypoglycaemia especially difficult. Blood pressure targets Control of blood pressure has been shown to be an effective way of reducing the risk of nephropathy. Use ACE inhibitors or angiotensin receptor blockers (ARBs) first. NICE recommends BP<140/80 mm Hg for people. ACCORD-BP study that in patients with T2DM who are at increased cardiovascular risk, BP lowering to target <120/80 conferred no survival benefit and some increased risk.
35 Practice based investigations Urine dipstick analysis Detect overt proteinuria, haematuria and infection. Haematuria is not a normal feature of diabetic nephropathy and its presence should alert the physician to the possibility of an alternative diagnosis. ACR Values of <3 are normal and >3, especially if persistent, may indicate early nephropathy Renal ultrasound scan Assessing renal size and ruling out obstruction or other structural lesions are important steps in making a diagnosis of diabetic nephropathy. What other investigations should be arranged? 1. Urinalysis to screen for haematuria and if haematuria is present (in the absence of infection) then urinary microscopy should be performed to look for other features of active sediment such as casts. If these are present, they indicate a glomerular lesion such as glomerulonephritis. 2. Other blood tests such as protein strip, immunoglobulins, complement levels, CRP, ESR, calcium and auto-antibodies if there are clinical indications to do these.
36 Active management in practice Check your practice systems for all patients with DM and EgFR<45 See if those patients are already known to renal team Review all medications Review investigations If not clear that it is diabetic nephropathy, refer For all, put care planning goals for glycaemic control, blood pressure, lipids, smoking and weight. Review peripheral pulses and refer if reduced
37 Treatment of End-Stage Renal Disease (ESRD) There are three primary treatment options for individuals who experience ESRD: 1. Hemodialysis 2. Peritoneal Dialysis 3. Kidney Transplantation
38 Procedure Hemodialysis A fistula or graft is created to access the bloodstream Wastes, excess water, and salt are removed from blood using a dialyzer Hemodialysis required approx. 3 times per week, each treatment lasting 3-5 hrs Can be performed at a medical facility or at home with appropriate patient training
39 Hemodialysis (cont.) Hemodialysis Diet Monitor protein intake Limit potassium intake Limit fluid intake Avoid salt Limit phosphorus intake Complications Infection at access site Clotting, poor blood flow Hypotension
40 Procedure Peritoneal Dialysis Dialysis solution is transported into the abdomen through a permanent catheter where it draws wastes and excess water from peritoneal blood vessels. The solution is then drained from the abdomen. Three Types of Peritoneal Dialysis Continuous Ambulatory Peritoneal Dialysis (CAPD) Continuous Cycler-Assisted Peritoneal Dialysis (CCPD) Combination CAPD and CCPD
41 Peritoneal Dialysis (cont.) Peritoneal Dialysis Diet Limit salt and fluid intake Consume more protein Some potassium restrictions Reduce caloric intake Complications Peritonitis
42 Kidney Transplant Procedure A cadaveric kidney or kidney from a related or nonrelated living donor is surgically placed into the lower abdomen. Three factors must be taken into consideration to determine kidney/recipient match: Blood type Human leukocyte antigens (HLAs) Cross-matching antigens
43 Kidney Transplant (cont.) Kidney Transplant Diet Reduce caloric intake Reduce salt intake Complications/Risk Factors Rejection Immunosuppressant side effects Benefits No need for dialysis fewer dietary restrictions higher chance of living longer
44 References American Diabetes Association: Nephropathy in Diabetes (Position Statement). Diabetes Care 27 (Suppl.1): S79-S83, 2004 National Kidney and Urologic Diseases Information Clearinghouse. Kidney Disease of Diabetes. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; United States Renal Data System. USRDS 2003 Annual Data Report. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; DeFronzo RA: Diabetic nephropathy: etiologic and therapeutic considerations. Diabetes Reviews 3: , 1995 National Kidney and Urologic Diseases Information Clearinghouse. Kidney Failure: Choosing a Treatment That s Right For You. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (NIH), DHHS; 2003.
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Risk Factors for Diabetic Nephropathy
 Risk Factors for Diabetic Nephropathy Amalkumar Bhattacharya Associate Professor in Medicine, Government Medical College, Surat - 395 001. 55 EPIDEMILGY AND DIABETES TYPE Diabetic nephropathy can occur
Risk Factors for Diabetic Nephropathy Amalkumar Bhattacharya Associate Professor in Medicine, Government Medical College, Surat - 395 001. 55 EPIDEMILGY AND DIABETES TYPE Diabetic nephropathy can occur
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Responding to the challenge of diabetic nephropathy: the historic evolution of detection, prevention and management
 (2000) 14, 667 685 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh REVIEW ARTICLE Responding to the challenge of diabetic nephropathy: the historic evolution of
(2000) 14, 667 685 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh REVIEW ARTICLE Responding to the challenge of diabetic nephropathy: the historic evolution of
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
An ebook on Type 2 Diabetes
 Chapter 4 Sagnik Mukherjee; Parijat De* Diabetic Nephropathy Department of Diabetes & Endocrinology, Sandwell & West Birmingham NHS Trust, UK. Email: p.de@nhs.net 1. Introduction ISBN: 978-93-87500-02-0
Chapter 4 Sagnik Mukherjee; Parijat De* Diabetic Nephropathy Department of Diabetes & Endocrinology, Sandwell & West Birmingham NHS Trust, UK. Email: p.de@nhs.net 1. Introduction ISBN: 978-93-87500-02-0
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence?
 Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Effective Health Care Program
 Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
For more information about how to cite these materials visit
 Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Chronic Kidney Disease. Basics of CKD Terms Diagnosis Management
 Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Chronic Kidney Disease Basics of CKD Terms Diagnosis Management Review the prevalence of chronic kidney disease (CKD) Review how CKD develops Review populations at risk for CKD Review CKD diagnosis Objectives
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
Reversal of Microalbuminuria A Causative Factor of Diabetic Nephropathy is Achieved with ACE Inhibitors than Strict Glycemic Control
 ISSN 0976 3333 Available Online at www.ijpba.info International Journal of Pharmaceutical & Biological Archives 2013; 4(5): 923-928 ORIGINAL RESEARCH ARTICLE Reversal of Microalbuminuria A Causative Factor
ISSN 0976 3333 Available Online at www.ijpba.info International Journal of Pharmaceutical & Biological Archives 2013; 4(5): 923-928 ORIGINAL RESEARCH ARTICLE Reversal of Microalbuminuria A Causative Factor
Understanding. Your Kidneys. Laurie Biel, RN,BSN, CNN The MGH Center For Renal Education March 28, 2016
 Understanding Your Kidneys Laurie Biel, RN,BSN, CNN The MGH Center For Renal Education March 28, 2016 Today s Discussion - The Role of your kidneys Common causes of kidney disease Treatment for kidney
Understanding Your Kidneys Laurie Biel, RN,BSN, CNN The MGH Center For Renal Education March 28, 2016 Today s Discussion - The Role of your kidneys Common causes of kidney disease Treatment for kidney
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Diabetic Nephropathy
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D.
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Chronic Kidney Disease: Optimal and Coordinated Management
 Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care
: Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
DIABETES AND CHRONIC KIDNEY DISEASE
 DIABETES AND CHRONIC KIDNEY DISEASE Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney Foundation's Kidney Disease Outcomes
DIABETES AND CHRONIC KIDNEY DISEASE Stages 1 4 www.kidney.org National Kidney Foundation's Kidney Disease Outcomes Quality Initiative Did you know that the National Kidney Foundation's Kidney Disease Outcomes
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Diabetes Mellitus. Eiman Ali Basheir. Mob: /1/2019
 Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
Diabetes Mellitus Eiman Ali Basheir Mob: 091520385 27/1/2019 Learning Outcomes Discuss the WHO criteria for Diabetes Mellitus diagnosis Describe the steps taken to confirm diagnosis Interpret GTT. Discuss
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
According to the US Renal Data System,
 DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
DIABETIC NEPHROPATHY * Mohamed G. Atta, MD ABSTRACT *Based on a presentation given by Dr Atta at a CME dinner symposium for family physicians. Assistant Professor of Medicine, Division of Nephrology, Johns
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Diabetes Renal Disease Management. Dr Paul Laboi Dr Vijay Jayagopal York Hospital
 Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
Diabetes Renal Disease Management Dr Paul Laboi Dr Vijay Jayagopal York Hospital 0 Diabetic Nephropathy Diabetic nephropathy is a clinical syndrome characterised by the following: Persistent albuminuria
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Lecture 19 Summary Gestational Diabetes and Complications of Diabetes. Gestational diabetes;
 Lecture 19 Summary Gestational Diabetes and Complications of Diabetes Gestational diabetes; - Type of diabetes that only develops during pregnancy Usually diagnosed in late pregnancy Causes high blood
Lecture 19 Summary Gestational Diabetes and Complications of Diabetes Gestational diabetes; - Type of diabetes that only develops during pregnancy Usually diagnosed in late pregnancy Causes high blood
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Chronic Kidney Disease. Dr Mohan B. Biyani A. Professor of Medicine University of Ottawa/Ottawa Hospital
 Chronic Kidney Disease Dr Mohan B. Biyani A. Professor of Medicine University of Ottawa/Ottawa Hospital Health Seminar Series Date 12 May 2013 Objectives Normal functioning of Kidneys. Risk factors to
Chronic Kidney Disease Dr Mohan B. Biyani A. Professor of Medicine University of Ottawa/Ottawa Hospital Health Seminar Series Date 12 May 2013 Objectives Normal functioning of Kidneys. Risk factors to
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
130/80 vs. 140/90 If nephropathy is present the target should be 120/ /10/07
 DG van Zyl Macro vascular Micro vascular Neuropathy Infections Genetic susceptibility *Repeated acute changes in cellular metabolism Hyperglycemia Tissue damage **Cumulative long term changes in stable
DG van Zyl Macro vascular Micro vascular Neuropathy Infections Genetic susceptibility *Repeated acute changes in cellular metabolism Hyperglycemia Tissue damage **Cumulative long term changes in stable
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification