Novel Resuscitation Strategies
|
|
|
- Logan Foster
- 6 years ago
- Views:
Transcription



1 Novel Resuscitation Strategies Hasan B Alam, MD Norman Thompson Professor of Surgery Head of General Surgery University of Michigan
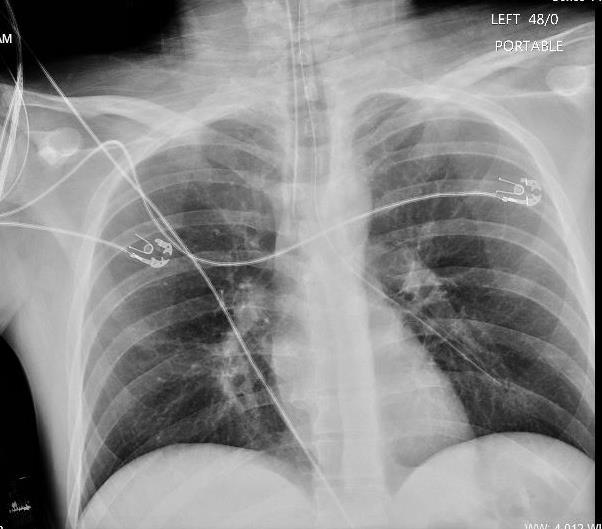
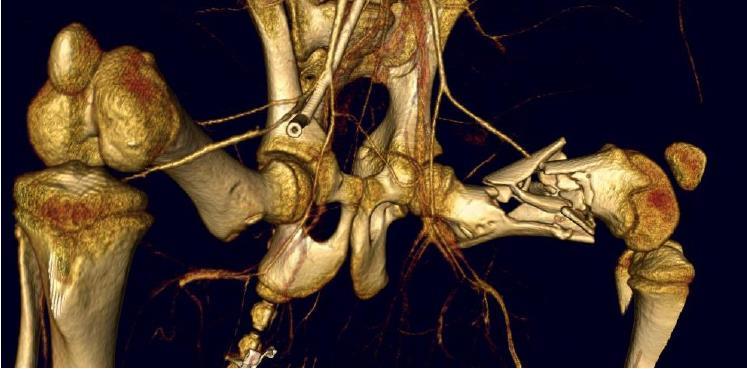
2 Case yrs old male. GSW x3, 10 min transport time SBP 70, HR 130, confused, diaphoretic GSW: arm, flank, and transpelvic Labs: Hg 10.4, ph 7.01, INR 1.0, PTT 21.9 ED Care: Intubation, groin lines, IVF 4-6L, PRBC 2 units Trauma team called
3 Triad of death Acidosis Coagulopathy Hypothermia
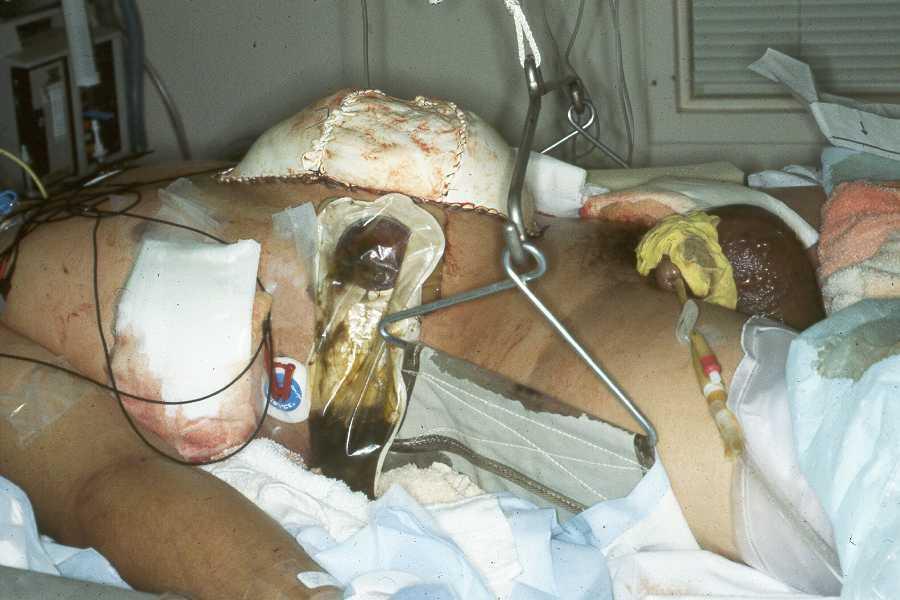
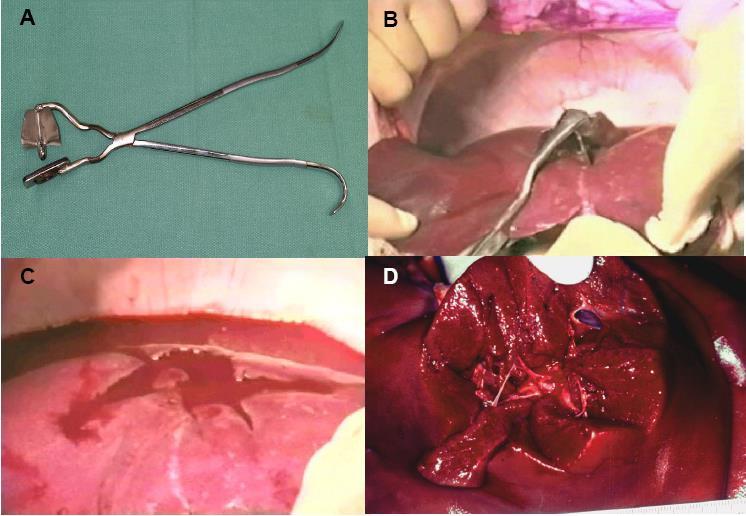
4 Back to our patient in the OR Abdomen full of blood + resuscitation fluids Damage control: Ligation iliac vein. Shunt iliac artery. Control of colon, small bowel injuries. Pelvic packing. No clot formation, high dose drugs Red blood cells 22, plasma 13, platelets 12 Diffuse bleeding
5 More data Hg: ph: INR: >10 PTT: >180 Increased peak airway pressures PEEP: cm H2O Bleeding from IV sites, ETT Efforts stopped- 4hrs-31min after arrival
6 Case yrs old No significant PMH Hit by a truck while riding a bicycle AAAx3. SBP ~50, HR 110/min Primary survey Secondary survey

7

8

9

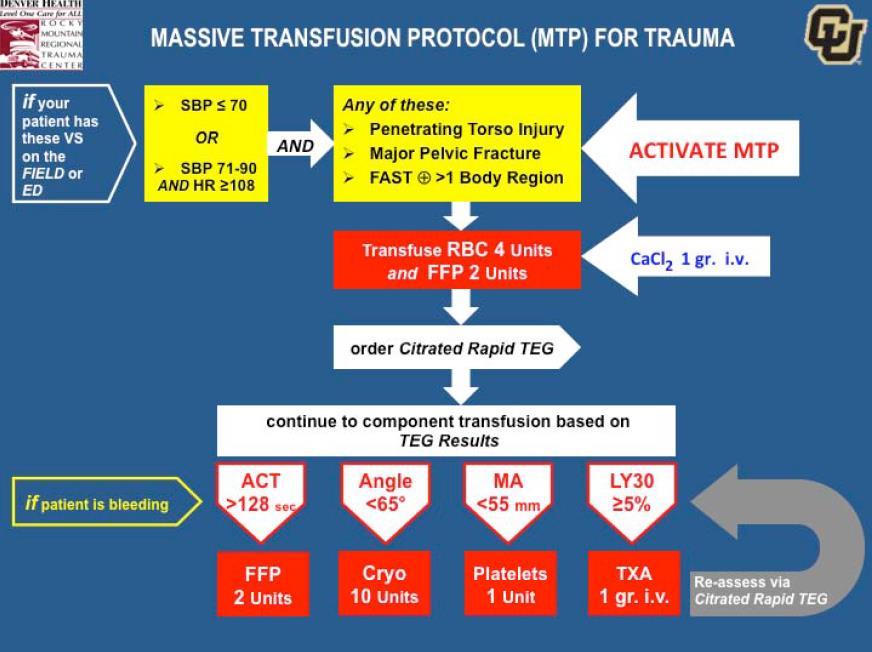
10 MTP 1:2 ratio; IR; multiple procedures; never coagulopathic
11 EMS: Case yr M, found in middle of a road after being hit by a car ~55mph At scene, hypotensive, tachycardic, GCS 4. bag mask ventilation Trauma Bay: A: Bag masking, unresponsive B: Bilateral breath sounds, 99% on NRB C: HR 120s, palpable femoral pulses, unable to obtain BP ph 6.9, lac 7.9, HCO3 11

12 Resuscitation Bay
13 Resuscitation Bay
14 MTP OR After transfer to OR bed, loss of pulses REBOA Pre-peritoneal packing + Damage control ex-lap IR Back to OR

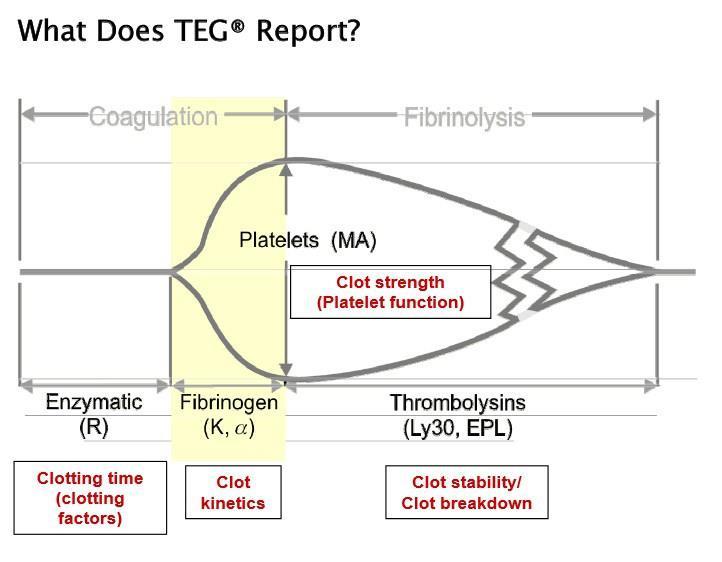
15 TEG/ROTEM


16 ROTEM Extem Fibtem Aptem Arrival Post-IR
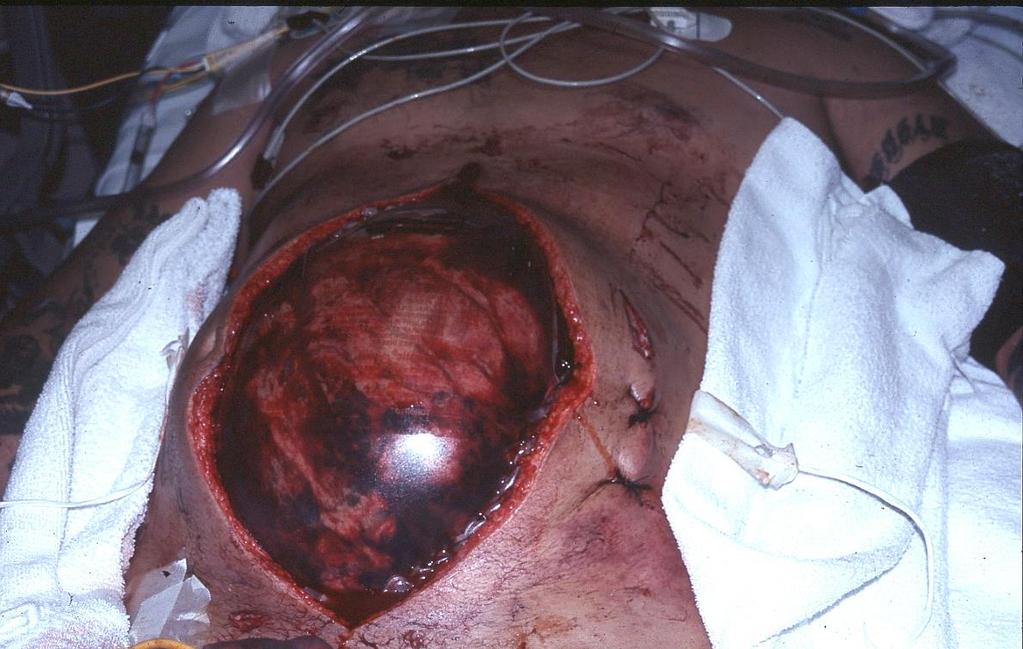
17 First, you must stop the bleeding


18 Goals of early trauma care Keep alive Minimize organ injury Decrease bleeding Keep alive Preserve key organs ABC s Fix injuries Resuscitate Support organs Pre-hospital ED OR/SICU
19
20 How much can you bleed? 100ml/minx15=1500 ml
21 Hemodynamic response to acute blood loss

22 The Trimodal Distribution Of Trauma Deaths The group that matters

23 #1 Cause of Preventable Death After Injury
24 Today: trauma deaths CRASH-2 trial Lancet RCT- 274 hospital, 40 countries, >20K patients Most died on the day of randomization Deaths due to MOF <2.5%
25 Clinical evidence Cochrane Review: Timing and volume of fluid administration for patients with bleeding 6 trials No evidence to support early or large volume resuscitation
26 Should resuscitation be delayed until control of hemorrhage? Prospective randomized (n=598) Mortality: Early 38%, Delayed 30% (RR 1.26, p=0.04) Hospital stay: Early 14 d, Delayed 11 d (p=0.006) No difference in multiple organ failure, infections
27 Is blunt trauma different? 20% have closed head injury Non surgically correctable sources Aggressive late resuscitation may worsen: Cerebral edema Pulmonary contusion Intra-abd hypertension/compartment syndrome


28
29

30 Excess fluids associated with worse outcomes in burn patients

31 Same is true for elective surgical patients

32 Impact of Resuscitation fluids on Cellular Functions Institute of Medicine 1999
33 Damage Control or Hemostatic Resuscitation Prioritize hemorrhage control Permissive hypotension Avoid crystalloids Early component therapy (protocol driven) Adjuncts: Correct hypothermia and acidosis Anti-fibrinolytics
34 Can you predict the need for massive transfusion?

35 Hgb, SBP, BD, HR, gender, +FAST, unstable pelvis, open femur fracture J Trauma, 2006


36
37
38 Early blood component therapy
39 BLEEDING PATIENTS

40 BLEEDING PATIENTS NEED BLOOD

41 RBC PLASMA PLATELETS

42

43

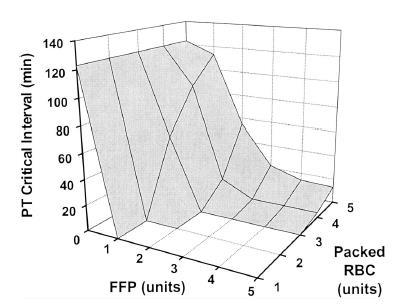
44 - Retrospective review of 246 pts - >10 units PRBC - Mortality due to hemorrhage= 93%, 78% & 38%
45

46 More FFP associated with better survival - Retrospective review of 708 patients



47 Protocol driven blood products: -Early component delivery without increasing total blood use - Better outcomes
48 Platelets are equally important (Inaba K et. al, JACS 2010)
 - Better 24 hrs and 30 day")
49 - Database study -MT from 22 level I centers over 12 mths (n=643) - Better 24 hrs and 30 day mortality


50 Prospective cohort study over 28 mths Single center (n=806) FFP to PRBC ratio not predictive
51 Can we use INR to determine who would benefit from FFP? Retrospective 437 MT patients INR correlates with mortality Benefits of FFP independent of INR How does FFP improve survival if not not due to less coagulopathy and less bleeding?


52 The Prospective, Observational, Multicenter, Major Trauma Transfusion (PROMMTT) Study: Comparative Effectiveness of a Time-varying Treatment with Competing Risks 10 centers with 1245 patients (905 > 3units PRBC) 3 fold lower death in the first 6 hrs if FFP:PRBC ratio <1:2 No difference in death after 24 hrs Holcomb JB et al. Archives Surg 2012;15:1-10
53 Limitations Potential survival bias Differences in care

54 First RCT examining ratios in trauma resuscitation with survival as endpoint



55 2015 1:1:1 vs 1:1:2 ratio level 1 trauma centers 24 hrs: Death 12.7 vs. 17% p=0.12 Exsanguination death 9.2 vs. 14.6% (p=0.03) More hemostasis in 1:1:1 24 hrs- 30 day No difference Rec: Massively bleeding patients need PRBC, FFP and Platelets in 1:1:1 ratio


56 More complications >6 units FFP: ARDS 12 fold MODS 6 fold Pneumonia/sepsis 4 fold Aggressive FFP harmful in patients without massive blood loss
57 Anti-fibrinolytics

58 EARLY SHOCK 1.5% survival advantage
59 All patients MT patients Mortality drop 28 to 14%. OR for Survival 7

60

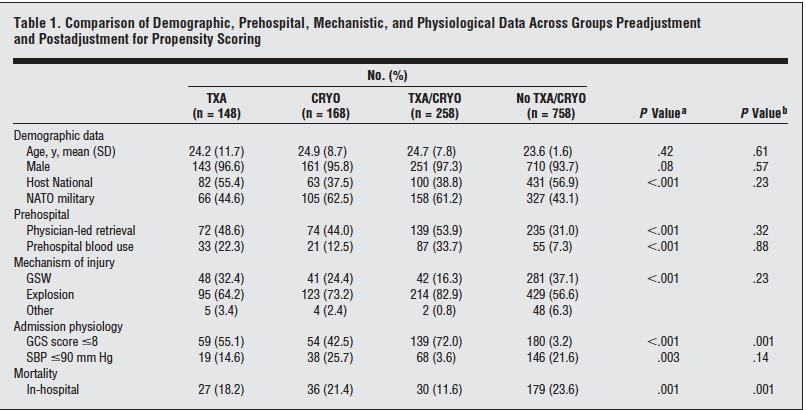
61 TXA/CRYO had higher ISS Got more PRBC No TXA/CRYO= 5 TXA= 8 CRYO= 20 TXA/CRYO= 22
62 Adult patients in severe hemorrhagic shock (SBP <75mmHg), known predictors of fibrinolysis, or TEG evidence (LY30>3%) Within 3 hrs 1 gm load (10 min) and 1 gm infusion x 8hr
63 Prothrombin Complex Concentrates (PCC)

64
65 For major bleeding related to vit K antagonists: 4 factor PCC rather than plasma (2 C) Plus, 5-10 mg vit K IV slow injection (2C)
66 Massive Transfusion Protocols Improvement in delivery Better utilization of products Improvement in outcomes
67

68 111 pts randomized to CCA and TEG Most deaths in the first 6 hrs TEG had better survival (19.6% vs. 36.4%) Similar PRBC use but lower platelet and plasma use in TEG group
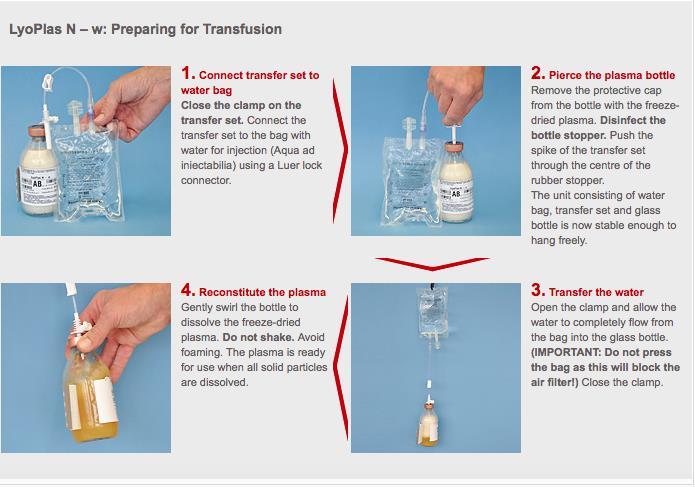
69
70 Recommendations Damage Control Resuscitation Prioritize hemorrhage control Avoid crystalloids and artificial colloids Permissive hypotension prior to hemorrhage control Early component therapy- delivered using a MT protocol Anti-fibrinolytic agents in severely injured
71 New developments



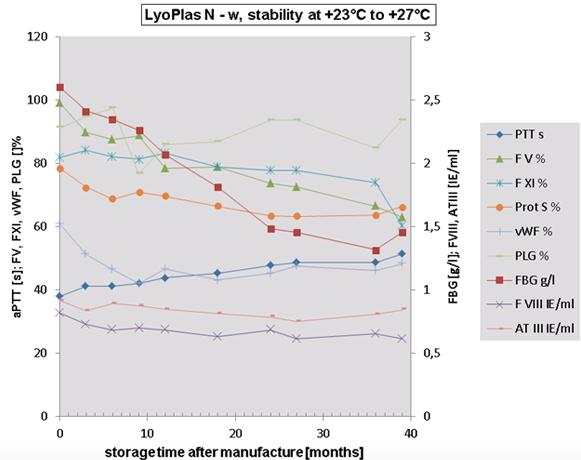
72 Plasma and red cells are good but

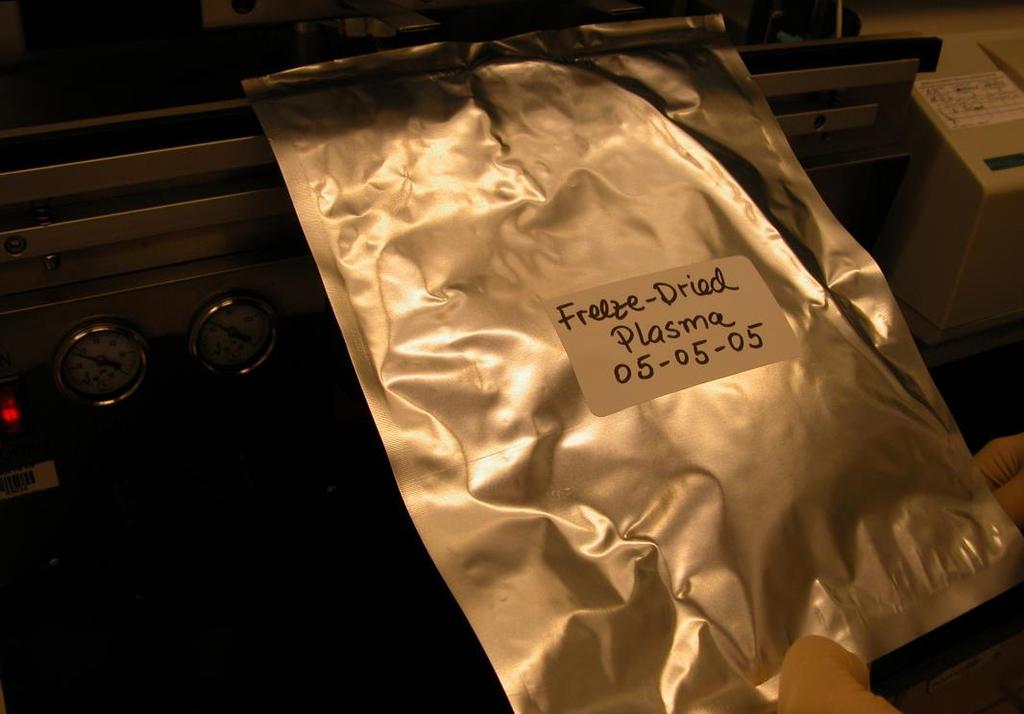
73 New approach Freeze dried plasma and platelets Combined with hemoglobin based solution, +/- factors +/- preserved platelets Low volume, hypertonic, hyperoncotic
74
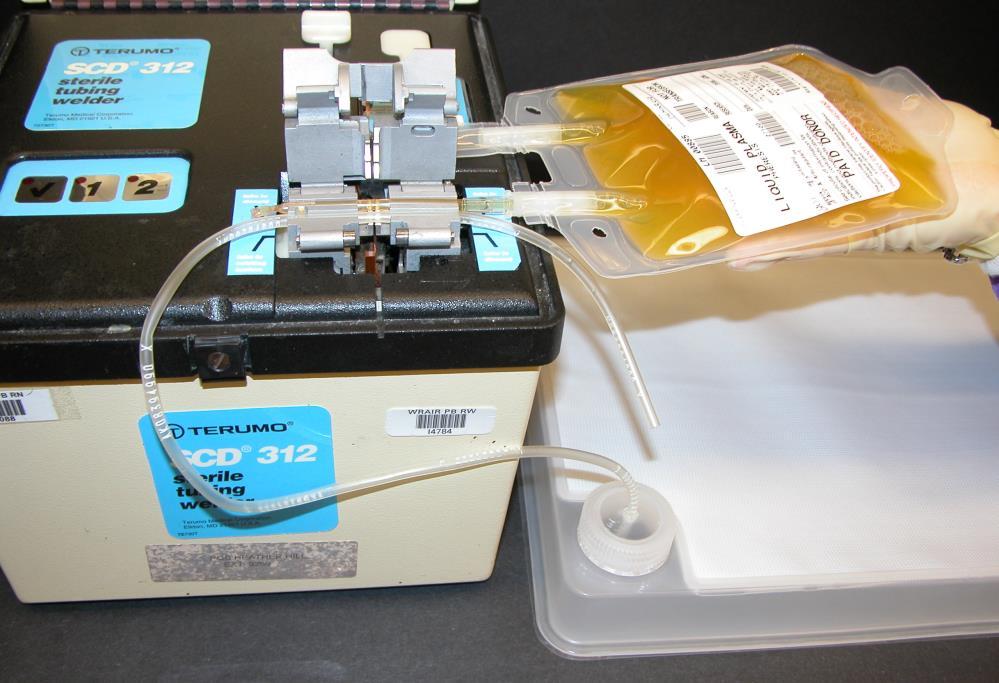

75 Irina Bakaltcheva, PhD (WRAIR)
76

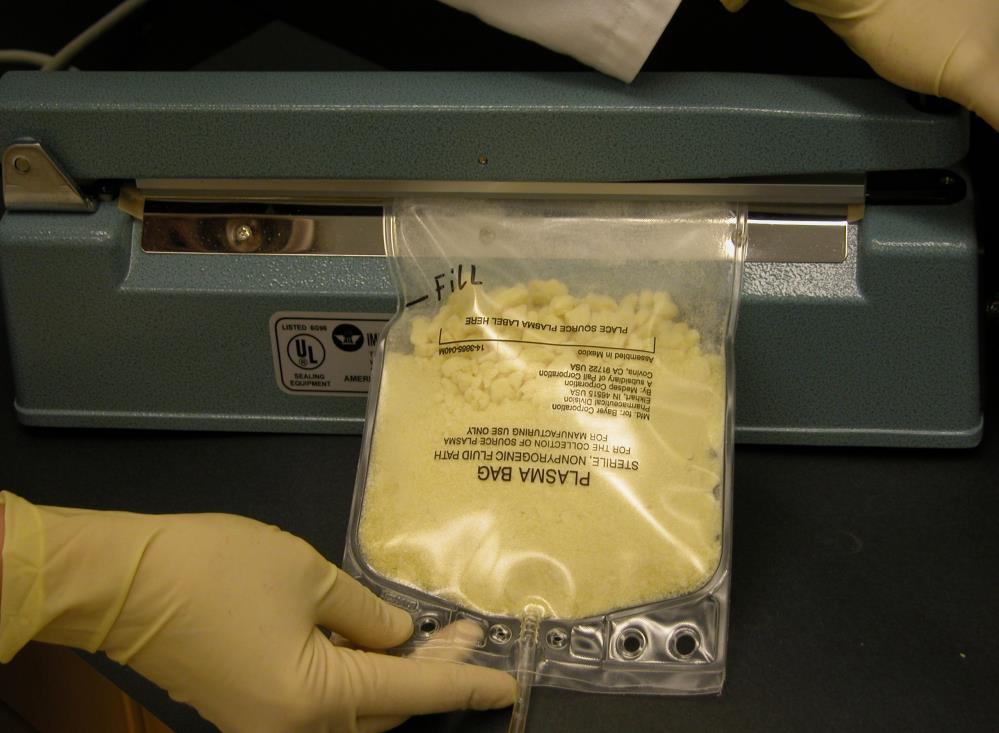
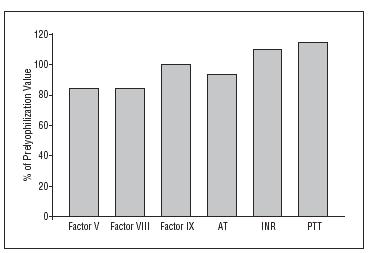
77 Spray dried 1/3 rd volume Just as good as FFP Easy to reconstitute

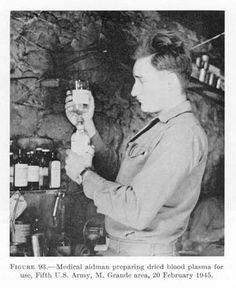
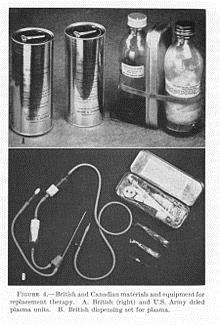
78 Not a new concept WWII

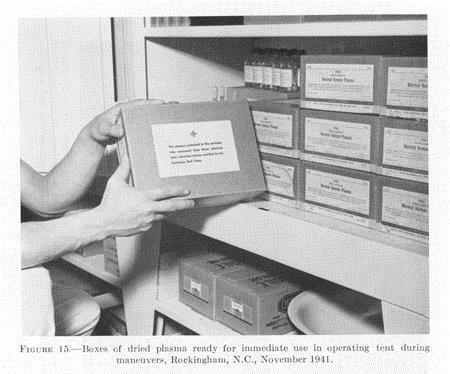
79


80 German LyoPlas Single donor Cellular reduction to improve compatibility Stored up to 15 months 350,000 units circulated No specific complications General complication rate 0.023%- similar to FFP
81
82

83 French LYophilised Plasma (FLYP) <10 donors/unit (minipool) Extensive quality control and testing Stored up to 24 months No major specific adverse events
84 South African Bioplasma FDP Pooled, solvent-detergent treated, universal plasma Screened and tested Recommended storage temp <25 o C In use since 1994 Solheim BG, Chetty R, Flesland O. Indications for use and cost-effectiveness of pathogen-reduced ABO-universal plasma. Curr Opin Hematol Nov;15(6):612-7.
85 USA Dried plasma not approved for use Options: FFP: Frozen within 8 hrs FP24: Frozen within 24 hours Pre thawed plasma: used up to 5 days Liquid plasma (aka never frozen plasma ): separated from whole blood 5 days before expiration. Kept at 1- o C for days Basic concept: Unfrozen = functional loss, especially factor VIII
86 Basu D, Kulkarni R. Overview of blood components and their preparation. Indian Journal of Anaesthesia. 2014;58(5):

87 Matijevic N, Wang YW, Cotton BA, Hartwell E, Barbeau JM, Wade CE, Holcomb JB. Better hemostatic profiles of never-frozen liquid plasma compared with thawed fresh frozen plasma. J Trauma Acute Care Surg Jan;74(1):84-90 Liquid plasma (26 days) superior to thawed FFP after 5 days
88 Fluidless Resuscitation



89 Making survivors out of non-survivors Surviving Blood Loss (SBL) Program Keep cells alive Fill the tank

90 Pharmacological treatment as a bridge to definitive care Desired properties: Should be safe and easy to administer & store Available Cost Valproic acid (VPA) Depakote or Depakene, Abbott Pharmaceuticals, Ltd. FDA approved Feb 1978 For seizure and mood disorders Numerous clinical trials for cancer treatment Generic available >80 trials ongoing
 &")

91 Histone modifications Deacetylases (HDACs) & Acetyltransferases (HATs) HDAC Inhibitors = Increased Protein Acetylation
 Histone deacetylase")
")

92 The Acetylome Minucci S (2006) Histone deacetylase inhibitors and the promise of epigenetic (and more) treatments for cancer Nat. Rev. Cancer. 6: doi: /nrc1779

93
94 Surgery 2009
95 Percent survival End of Hemorrhage Survival 100 * * Fresh w hole blood-100% (n=6) Valproic acid-85.7% (n=7) 50 Control-25% (n=8) *=Log-Rank (Mantel-Cox test), p<0.05 compared to control Alam et al. Surgery 2009 Minutes




96 HDACIs in Lethal Injuries Decreased apoptosis Activation of survival pathways Decreased inflammatory response >50 manuscripts Improved survival Decreased organ dysfunction Millions in NIH and DoD Funding Attenuation of coagulopathy FDA approved Clinical Trial

97 Hemorrhage + Traumatic Brain Injury



98 Lesion size (mm 3 ) Brain swelling (%) Decrease in Brain Lesion Size and Edema Within 6 hrs- High dose VPA (300 mg/kg) NS Hex Hex +VPA * * * NS Hex Hex+VPA Jin et al. J Trauma NS Hex Hex+VPA

99 Combination of VPA and FFP is the best Imam et al. Surgery August 2013


100 NSS NS NS+VPA 10 * p = Day
101 Georgoff PE et al. Pharmacokinetics and safety of high-dose intravenous valproic acid in healthy subjects: a dose escalation trial to support clinical translational studies. Clinical Pharmacokinetics 2017
102

103 Phase II and III trials- Hemorrhage $34.6 M

104 Massive blood loss and no pulse Emergency Department Thoracotomy

105

106 The ultimate resuscitation strategy
107

108


109 Cognitive function testing Alam et al, Surgery 132: , 2002 Operant conditioning Recognize and open color coded box Number of sessions, time to finish task, performance score
110 Emergency Preservation and Resuscitation Rate of induction Fast (2 o C/minute) Alam et al. J Trauma 2004 Optimal Depth Profound (10 o C) Alam et al. Surgery 2006 Rate of re-warming (0.5ºC/minute) Alam et al. J Trauma 2006 Duration short (60 minutes) Alam et al. J Trauma 2008 Poly-trauma feasible without complications Sailhamer et al. JACS 2007


111 October 2012 Sponsored by the NIH and the DoD Guidelines for future research
112
113 Goals of early trauma care Keep alive Minimize organ injury Decrease bleeding Keep alive Preserve key organs ABC s Fix injuries Resuscitate Support organs Pre-hospital ED OR/SICU Pro-survival drugs Freeze dried plasma EPR
114 The difficulty lies, not in the new ideas, but in escaping from the old ones.. John Maynard Keynes ( )

115 Funding acknowledgement: National Institutes of Health and the US Department of Defense
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
REBOA - Real World. Lena M. Napolitano, MD
 REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Resuscitation Update
 Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Resuscitation Update? Dr. Edward Pyun Jr., M.D. FACS Trauma Medical Director/Surgical ICU Director OSF St. Anthony Medical Center Trauma Services Perryville Surgical Associates November 10, 2012 2009 Recommendations
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
1/16/2014 NONE WILL BE TALKING ABOUT NON FDA APPROVED DRUGS WILL LET YOU KNOW WHEN NOT ENDORSING ANY PARTICULAR PIECE OF EQUIPMENT
 CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
CUTTING EDGE TACTICAL MEDICINE SECRETS FROM THE BATTLEFIELD Brendan Anzalone, DO, Maj, USAF, MC Emergency Physician Special Tactics Medicine USAF Special Operations Surgical/Critical Care Evacuation Team
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Strategies to Enhance Plasma Availability
 Strategies to Enhance Plasma Availability Andrew Bernard, MD Professor of Surgery Medical Director, Acute Care Surgery and Trauma Chief, Section on Trauma and Acute Care Surgery Paul A. Kearney, MD Endowed
Strategies to Enhance Plasma Availability Andrew Bernard, MD Professor of Surgery Medical Director, Acute Care Surgery and Trauma Chief, Section on Trauma and Acute Care Surgery Paul A. Kearney, MD Endowed
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
HYPOTHERMIA IN TRAUMA. Kevin Palmer EMT-P, DiMM
 HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
HYPOTHERMIA IN TRAUMA Kevin Palmer EMT-P, DiMM DISCLOSURE No Financial conflicts of interest Member of the Wilderness Medical Society Diploma in Mountain Medicine Fellowship in the Academy of Wilderness
Damage control resuscitation using blood component therapy in standard doses has a limited effect on coagulopathy during trauma hemorrhage
 Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
Intensive Care Med (2015) 41:239 247 DOI 10.1007/s00134-014-3584-1 ORIGINAL Sirat Khan Ross Davenport Imran Raza Simon Glasgow Henry D. De Ath Pär I. Johansson Nicola Curry Simon Stanworth Christine Gaarder
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Massive Transfusion Initiation & Implication
 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department
11/1/2014. Just The. Pearls. Everything I do is Off-Label! This is the ultimate lecture for the ADHD emergency physician.
 Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma
 Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
UPDATE IN TRAUMA ANESTHESIA ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR
 UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
UPDATE IN TRAUMA ANESTHESIA 2018 ARANA Spring Meeting May 5th, 2017 Joe Romero CRNA, MS, CPT USAR UPDATE IN TRAUMA ANESTHESIA 2018 - An overview of trauma demographics, mechanisms, and current literature
CRASH ing Trauma Patients: The CRASH trials. Tim Coats Professor of Emergency Medicine University of Leicester, UK
 CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
CRASH ing Trauma Patients: The CRASH trials Tim Coats Professor of Emergency Medicine University of Leicester, UK www.le.ac.uk/emag I DO NOT have an affiliation (financial or otherwise) with a pharmaceutical,
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
Clinical Overview of Coagulation Testing Issues
 Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Clinical Overview of Coagulation Testing Issues Adam M. Vogel, MD Assistant Professor, Division of Pediatric Surgery Washington University in St. Louis School of Medicine September 19, 2014 Disclosure
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Exsanguinating hemorrhage continues to be one of the
 ORIGINAL ARTICLE All Massive Transfusion Criteria Are Not Created Equal: Defining the Predictive Value of Individual Transfusion Triggers to Better Determine Who Benefits From Blood Rachael A. Callcut,
ORIGINAL ARTICLE All Massive Transfusion Criteria Are Not Created Equal: Defining the Predictive Value of Individual Transfusion Triggers to Better Determine Who Benefits From Blood Rachael A. Callcut,
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
The principle of 1:1:1 blood product use in the resuscitation of trauma victims. K. D. Boffard
 The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
The principle of 1:1:1 blood product use in the resuscitation of trauma victims K. D. Boffard Milpark Hospital Department of Surgery University of the Witwatersrand Johannesburg, South Africa Annual Controversies
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
No Disclosures OBJECTIVES. Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War
 Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Damage Control Resuscitation Lessons Learned and the Way Forward After More Than a Decade of War No Disclosures COL(ret) Michael M. Woll, MD, FACS Surgical Det. A, 249 th General Hospital 28 th Combat
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for External Hemorrhage Control
 Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Mechanisms of Trauma Coagulopathy. Dr B M Schyma Changi General Hospital Singapore
 Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Mechanisms of Trauma Coagulopathy Dr B M Schyma Changi General Hospital Singapore HAEMORRHAGE A continued cause of PREVENTABLE death. 24% of trauma patients are coagulopathic on arrival 1 56% of severe
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Prehospital Hemorrhage Control
 Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary)
") BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary) What s new at STARS? STARS bases and response areas Operations
BLOOD IN THE AIR: THE STARS EXPERIENCE Dr. Ryan Deedo MD DipAeroRT FRCPC Transport Physician STARS Medical Communications Lead (Calgary) What s new at STARS? STARS bases and response areas Operations
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
How can ROTEM testing help you in trauma?
 How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Trauma Resuscitation: more than just blood products
 Trauma Resuscitation: more than just blood products Benjamin T. Houseman, MD, PhD Assistant Professor in Residence Department of Anesthesia University of California San Francisco Traumatic injury Leading
Trauma Resuscitation: more than just blood products Benjamin T. Houseman, MD, PhD Assistant Professor in Residence Department of Anesthesia University of California San Francisco Traumatic injury Leading
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center
 ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE
 JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
JUNCTIONAL STAB WOUND SAVING THE UN-SAVABLE MARVIN WAYNE, MD, FACEP, FAAEM, FAHA ASSOCIATE CLINICAL PROF. DEPT. OF EM, UNIVERISTY OF WASHINGTON EMS MEDICAL DIRECTOR WHATCOM COUNTY WA EMERGENCY DEPT. PEACEHEALTH
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Abdominal V.A.C. Therapy in Trauma
 Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Blood Reviews 23 (2009) Contents lists available at ScienceDirect. Blood Reviews. journal homepage:
 Contents lists available at ScienceDirect. Blood Reviews. journal homepage:") Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Blood Reviews 23 (2009) 231 240 Contents lists available at ScienceDirect Blood Reviews journal homepage: www.elsevier.com/locate/blre REVIEW Resuscitation and transfusion principles for traumatic hemorrhagic
Hypotensive Resuscitation
 Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
Curr Anesthesiol Rep (2014) 4:209 215 DOI 10.1007/s40140-014-0064-7 ANESTHESIA FOR TRAUMA (J-F PITTET, SECTION EDITOR) Hypotensive Resuscitation Jeremy B. Smith Jean-Francois Pittet Albert Pierce Published
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey