Massive Transfusion Initiation & Implication
|
|
|
- Domenic Owens
- 6 years ago
- Views:
Transcription
1 Massive Transfusion Initiation & Implication Katayoun Fayaz MD Blood Bank Medical Director Northwell Health April 2017
2 Trauma Statistics/Facts Each year trauma accounts for 41 million emergency department visits and 2.3 million hospital admissions across the nation. Life Years Lost (2014) Trauma injury accounts for 30% of all life years lost in the U.S. Cancer accounts for 16% Heart disease accounts for 12% Economic Burden $671 billion a year, including both health care costs and lost productivity Deaths due to injury (2014) 192,000 Ranking as cause of death #1 for age group 1-46, or 47% of all deaths in this age range #3 as leading cause of death overall, across all age groups Receiving care for a severe injury at a designated/verified trauma center can lower risk of death by 25 percent, yet almost 45 million Americans do not have access to a trauma center within one hour of becoming injured (CDC).
3 Case 1 A 28-year-old white male with unknown medical history presented to the emergency room after suffering a gunshot wound to the right groin. Initial vital signs demonstrated a heart rate of 153 beats per minute, oxygen saturation 93%, and a thready pulse with an inability to detect a noninvasive blood pressure. The patient was confused and combative, and pertinent physical exam revealed an actively bleeding wound to the right inguinal region.
4 What are your initial priorities in managing this case? Is it time to start the massive transfusion protocol? Central venous access was obtained, Massive Transfusion Protocol (MTP) initiated, and 2 units of uncross-matched, O-negative blood were hung as the patient was rushed to the Level 1 trauma OR. Lab work had not been obtained prior to transport. Initial arterial blood gas analysis demonstrated: ph 6.622, pao mm Hg, paco mm Hg, HCO mmol/l, base excess 29.3 meq/l on 100% FiO 2, and a point of care hemoglobin 12.1 g/dl. Blood was sent to the laboratory for complete analysis and typing, but those results, as well as crossmatched blood products, were unavailable during the initial resuscitation. When lab results returned, the patient s coagulation panel demonstrated prothrombin time (PT) 22.4 seconds, partial thromboplastin time (PTT) 49.6 seconds, international normalized ratio (INR) 2.0, and fibrinogen 124 mg/dl. The patient s blood type was later determined as O-positive.
5 Which biochemical values require monitoring in the critically bleeding patient? Temperature, Acid-base status, Ionized calcium, Hemoglobin, Platelet count PT/INR APTT Fibrinogen level Values indicating critical physiological derangement include: Temperature <35 ph <7.2, base excess >-6, lactate >4mmol/L Ionized calcium <1.1mmol/L Platelet count <50 x 10/L PT > 1.5 X normal INR >.1.5 X normal Fibrinogen level <1 g/l
6 Questions! What is the most common cause of death within the first hour of arrival to a trauma center? Hemorrhage What is the definition of Massive Hemorrhage? Massive hemorrhage can be defined as follows: blood loss exceeding circulating blood volume within a 24-hour period, (ii) blood loss of 50% of circulating blood volume within a 3-hour period, (iii) blood loss exceeding 150 ml/min, or (iv) blood loss that necessitates plasma and platelet transfusion. What is the deadly triad? Acidosis, Hypothermia, Coagulopathy

7 Trauma Mortality and the Golden Hour Early Mortality CNS injury &Hemorrhage Prehospital period 33-56% Hemorrhage Operating room 80% Hemorrhage First 24 hours 50% Hemorrhage Late Mortality & Morbidity Acidosis/ Base deficit Multi-organ Failure Sepsis
8 Early recognition of major blood loss and effective resuscitation are essential to avoid unnecessary deaths. Delays to transfusion adversely affects outcome. Key element is effective communication between all staff involved in patient s care.

9 What classification tool can assist you in classifying hemorrhagic shock in the critically bleeding adult patient?
10
11 15 20% of the resulting deaths which occur within the first hours of hospital admission might be preventable. How? Prompt and aggressive administration of blood products: Massive transfusion protocols (MTPs) Resuscitation with damage control Permissive hypotension

12 The main mechanisms involved in acute trauma related coagulopathy and transfusion strategy

13 Flowchart of initial management of trauma related hemorrhagic shock
14 What is Damage Control Resuscitation ( DCR)? Patients die from a triad of coagulopathy, hypothermia and metabolic acidosis. Once this metabolic failure has become established it is extremely difficult to control hemorrhage and correct the derangements. If the patient is to survive, the operation must be foreshortened so that they can be transferred to a critical care facility where they can be warmed and the hypothermia and acidosis is corrected. Once this is achieved the definitive surgical procedure can be carried out as necessary - the 'staged procedure'. RBC and plasma should be delivered by a rapid transfuser and through a blood warmer Restore perfusion and permissive hypotension
 Integrated damage control resuscitation damage control surgery")
15 (a) Classical damage control resuscitation damage control surgery sequence (b) Integrated damage control resuscitation damage control surgery sequencing.
16 What is permissive hypotension? Systolic blood pressures of mm Hg are tolerated while bleeding is being controlled (without TBI). No need to normalize the blood pressure!
17 Back to our case! Is it time to start the massive transfusion protocol? A 28-year-old gun-shot wound Initial vital signs: HR 153 beats per minute, oxygen saturation 93%, an inability to detect a noninvasive blood pressure. The patient was confused and combative, and pertinent physical exam revealed an actively bleeding wound to the right inguinal region.
18 Triggers for Initiating MT Prediction Tools Predicting the need for MT The Assessment of Blood Consumption (ABC) score The Emergency Transfusion Score (ETS) The Trauma Associated Severe Hemorrhage (TASH) score
19
20 Criteria to trigger the activation of MTP include one or more of following: ABC score 2 or more Persistent hemodynamic instability Active bleeding requiring operation or embolization Blood transfusion in the trauma bay
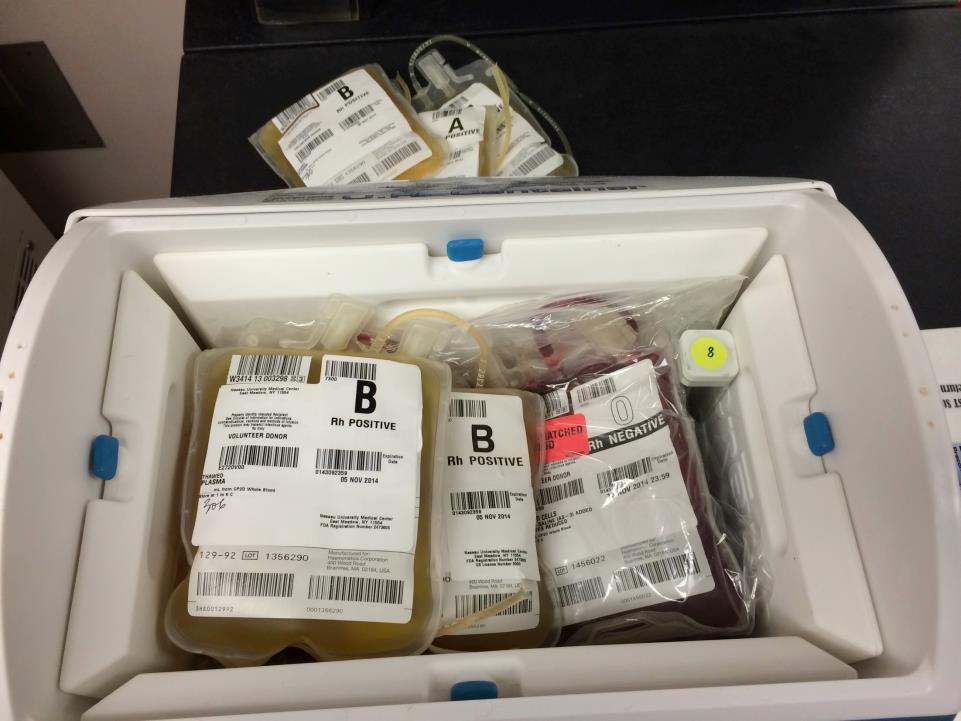
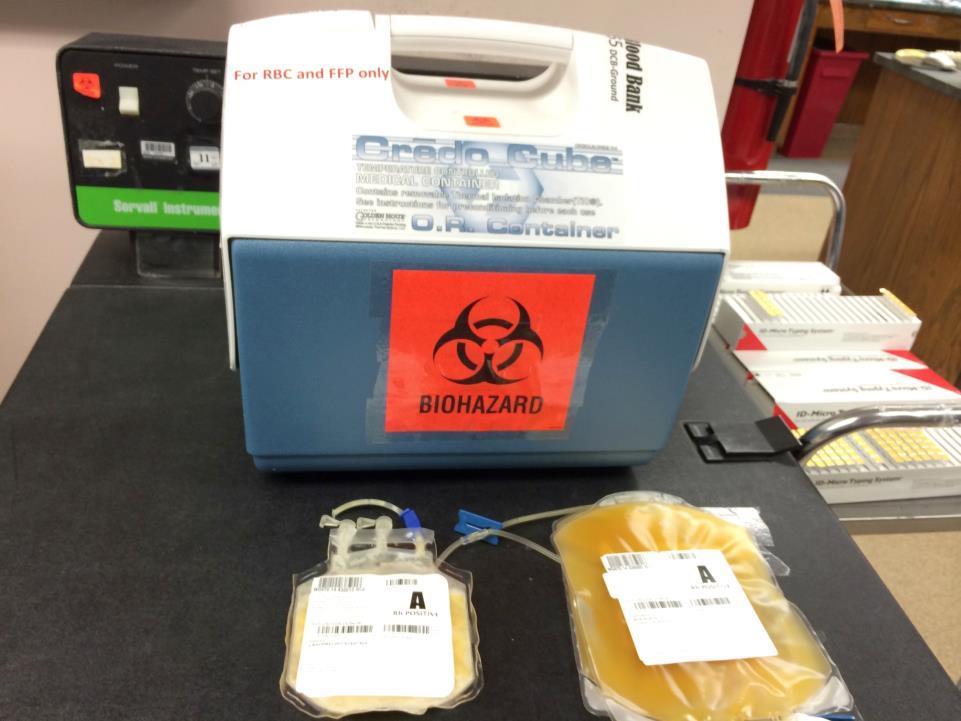
21 MTP triggers met, what do you do? Activate MTP Order MTP Begin universal blood product infusion rather than crystalloid or colloid solutions Transfuse universal RBC and plasma in a ratio of 1:1 Universally compatible RBC( O Rh negative and thawed plasma( AB plasma or low titer A plasma) Transfuse one Single Donor Platelet (SDP) or random donor platelet pool for each 6 units of RBC Blood products should be sent by the Blood Bank(BB) in established ratios Subsequent coolers should be delivered at 15-minutes intervals until MTP has been terminated The goal is to keep at least one MTP cooler ahead for the duration of the MTP activation

22


23

24
25
26

27
28 Route and Rate of Fluid Administration Standard, large (14- to 16-gauge) peripheral IV catheters are adequate for most fluid resuscitation. With an infusion pump, they typically allow infusion of 1 unit of packed RBCs in 20 min. For patients at risk of exsanguination, a large (8.5 French) central venous catheter provides more rapid infusion rates; a pressure infusion device can infuse 1 unit of packed RBCs in < 5 min.
29 Communication Notify the blood bank, when patient is transferred from ER to OR, or interventional radiology Once major bleeding has been controlled and the rate of transfusion has slowed it is appropriate to switch to a laboratory-or Point Of Care (POCT)-based transfusion For the performance improvement purposes the of ratio of blood product transfusion should be accessed at the time of bleeding cessation
30 Ending of MT Criteria and process for termination the MTP Anatomical ( control of bleeding) and physiological (normalizing hemodynamic status) criteria Further resuscitation is futile
31 Therapeutic Adjuncts in MTP Ant fibrinolytic medications ( Tranexamic acid TXA or Aminocaproic acid) Prothrombin Complex Concentrates Recombinant activated factor 7
32 Monitoring System Performance in Massive Transfusion Review cases of MTP with the following complications: Coagulopathy Thrombotic complications ARDS Other transfusion reactions: TACO, TRALI, and HTR Inappropriate FFP: RBC ratio Death
33 Performance Indicators for the process of MTP Time from calling MTP to infusion of first unit RBC Time from calling MTP to infusion of first unit of Plasma Adherence to predetermined ratio Informing the BB that MTP has been terminated within one hour of termination Wastage rate for blood products
34 Case 2 31-year-old male was rock-climbing with two friends at a national park 14 miles away from the nearest hospital when he suddenly lost his footing and fell 18 feet to the ground. Med-evac located and evacuated the man. A largebore IV was placed in each arm in-flight, and normal saline fluid was administered intravenously. The patient became increasingly disoriented during the flight, reaching the emergency room about 40 minutes after the fall.
35 Physical Examination The patient was lethargic but responsive to shouting and sternal pinch. He had multiple abrasions over his chin, neck, anterior thorax, and abdomen. A six-inch-long, half-inch deep laceration was noted in the right inguinal region, extending into the right, upper thigh. The tourniquet placed in this area was soaked with blood. Vital signs were as follows: HR = 112 (supine) and 128 (sitting), BP = 108 / 60 (supine) and 92 / 52 (sitting), RR = 32, rectal temp = 99.4 o F. Skin was cold and clammy.
36 Laboratory Studies Hematocrit = 46% Hemoglobin = 15.0 gm / dl Blood ph = 7.28 Urinary output in first 60 minutes in ER was 20 ml ECG revealed normal sinus rhythm with slight STdepression in most leads.
37 What is this patient's primary problem? This patient has lost a significant volume of blood due to a laceration of his right femoral artery. He is in danger of developing hemorrhagic shock.
38 List all of the evidence you can that supports your answer to #1 The history of a fall and the appearance of a bloodsoaked, right thigh tourniquet overlying the laceration in the right groin suggest that this patient lacerated his right femoral artery.
39 Is this patient's urinary output normal? Why is it important to monitor this patient's urinary output? This patient's urinary output is 20 ml per hour, which is below normal range of ml per hour. Severe hemorrhagic shock can reduce blood flow to the kidneys acute renal failure
40 What is the ABC Score? Do you activate MTP? How do you activate MTP?
 Call the Blood Bank (BB) x 26344 or Use Red Phone in Trauma Room to: Inform of the activation of the MTP Sunrise MTP1 order set : = 4 RBC + 4 FFP + 1 PLA & Type")
41 MTP Ordering Process Massive Transfusion Criteria & Consequences MTP Declared by authorized MD and/or resident (Team Leader) Pre-Identify Team Lead: Know the criteria Assign roles Ensure basic knowledge Track progress (way-points) Call the Blood Bank (BB) x or Use Red Phone in Trauma Room to: Inform of the activation of the MTP Sunrise MTP1 order set : = 4 RBC + 4 FFP + 1 PLA & Type and Screen + CBC, & ABG & electrolytes, & PT/PTT, Fibrinogen level, & TXA-tranexamic acid (Pharmacy) MTP order set 2 : 6 RBC+6 FFP+ 1PLA+ CRAYO Provide to Blood Bank: Team leader name pager # Patient s information Name, MR#, Gender, Age Limited Clinical History Track progress: Know where you are Keep up with plasma Order labs as you go
42 Suggested points for residents from blood bank techs! 1. Confirmatory specimens: a. There is no point in drawing a confirmatory specimen at the same time as the TNS. Tell them we KNOW they are doing this and it needs to stop! The patient must be re-identified before drawing the confirmatory sample. b. If a patient has a name (not Trauma name), they can call blood bank to see if a confirmatory is needed or not. (Even if a patient was born here and we have a type, it counts! and we do not need a confirmatory ever!) 2. Phlebotomist ID: First initial, Last name and Lawson number of the Phlebotomist (person who identifies the patient) must be LEGIBLE and on all specimens Submitted to the blood bank. If the required info is missing or illegible you will have to redraw the patient.
43 3. MTP vs ala carte product ordering: Please stress that you do not need to have an MTP, in order to get urgent blood products. If you know a patient will probably need blood, even a relatively large amount (not massive), this can be ordered ahead of time (for example: order 4 plasma and 4 RBC if there is a possibility it may be required). 4. Uncrossmatched vs Crossmatched blood: a. O negative, which is usually given for uncrossmatched blood is a very rare commodity and must be used judiciously (I like that word). Only approximately 7.5% of the population is this type. b. Crossmatched blood means that a sample of the donor unit is tested with the patients serum in a test tube a observe for any incompatibility. You do not have this assurance with uncrossmatched blood. c. Blood Bank is NOT WALMART. The staff does not just take the item out of the refrigerator and CHECK it out. RBC must be crossmatched. Plasma must be thawed. Orders must be accepted and filled and issued in the computer. All while assuring the safe transfusion for your patient.
44 5. ALLOCATED in the computer means ready to be picked up a. You should not have to call the blood bank to see if blood is ready. b. The blood bank does not have to be notified that you are coming/sending someone to pick up blood products. c. A pick up slip with patients full name and MR# is always required. Also remind them when the patient expired please let us know so units reserved on the patient can be made available. Also no CABD is not a reason to order uncrossmatched blood!
MASSIVE TRANSFUSION PROTOCOL
 MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last
 Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last Approved Time: 7/22/2016 12:44:54 PM Massive Transfusion
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: MTP 2016 Revision: 2.00 Created By: Admin, The Last Approved Time: 7/22/2016 12:44:54 PM Massive Transfusion
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors. THOR Collaboration
 Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Remote Damage Control Resuscitation: An Overview for Medical Directors and Supervisors THOR Collaboration Agenda What is Remote Damage Control Resuscitation? Putting RDCR into Practice Control Hemorrhage
Implementation and execution of civilian RDCR programs Minnesota RDCR
 Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Implementation and execution of civilian RDCR programs Minnesota RDCR Donald H Jenkins, MD FACS Associate Professor of Surgery and Director of Trauma Division of Trauma, Critical Care and Emergency General
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Major Haemorrhage Transfusion Pathway
 Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
Major Haemorrhage Transfusion Pathway SENIOR CLINICIAN ASSESSMENT: DECLARES MAJOR HAEMORRHAGE ( Call for help ( Telephone via switchboard: Consultant or Senior Clinician Duty Anaesthetist Porters (if will
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Emergency Blood and Massive Transfusion: The Surgeon s Perspective. Transfusion Medicine Update September 16 17, 2009
 Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
Transfusion Medicine Update September 16 17, 2009 Mandip S. Atwal, D.O. FACOS Carl M. Pesta, D.O. FACOS Agenda History Hemorrhagic shock Transfusion is Bad Transfusion Prevention Transfusion The Red Chest
anesthesia & mass casualty events
 anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
anesthesia & mass casualty events marc p steurer, md, desa president, trauma anesthesiology society (www.tashq.org) director, trauma anesthesiology UCSF/ SFGH associate professor UCSF faculty disclosure
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Hemostatic Resuscitation
 Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
Hemostatic Resuscitation 30 th David Miller Trauma Symposium Bill Beck, MD Assistant Professor of Surgery Trauma, Emergency General Surgery, Critical Care Disclosures None Again. Mac user. Why I Like Trauma?
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Unit 5: Blood Transfusion
 Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Unit 5: Blood Transfusion Blood transfusion (BT) therapy: Involves transfusing whole blood or blood components (specific portion or fraction of blood lacking in patient). Learn the concepts behind blood
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS
 GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
GUIDANCE DOCUMENT FOR MASSIVE HEMORRHAGE MANAGEMENT IN ADULTS 1.0 Definitions & Acronyms 1.1 Massive Hemorrhage Event (MHE): Transfusion of a volume of blood components equivalent to a patient s estimated
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
MASSIVE HAEMORRHAGE POLICY. ABMU HB Transfusion Team
 MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
TRANSFUSION REACTION EVALUATION
 Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
Lab Dept: Test Name: Transfusion Services TRANSFUSION REACTION EVALUATION General Information Lab Order Codes: Synonyms: CPT Codes: Test Includes: TRXR Transfusion Complication Workup; Hemolytic reaction
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Sign up to receive ATOTW weekly
 MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
MANAGEMENT OF MAJOR HAEMORRHAGE PART ONE: INITIAL RESPONSE ANAESTHESIA TUTORIAL OF THE WEEK 136 1 ST JUNE 2009 Katrina Webster (Senior Registrar in Anaesthesia) Royal Hobart Hospital, Tasmania, Australia.
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Massive Transfusion in Trauma
 Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
Page 1 Massive Transfusion in Trauma Robert S. Harris, M.D. Atlanta, Georgia Definitions and Demographics Hemorrhage is the second most common cause of death following injury and trauma, and is responsible
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Nursing Process Focus: Patients Receiving Heparin
 Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC. Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Obtain complete heath history including allergies, drug history and possible drug Assess baseline coagulation studies and CBC. Assess for history of bleeding disorders, GI bleeding, cerebral bleed, recent
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Trauma Care -- DH Lambert 02/04/07 Page 1 Revised 05/28/08 TRAUMA CARE
 Page 1 Revised 05/28/08 TRAUMA CARE If the patient arrives intubated that simplifies things. Quickly move the patient to the operating bed. The patient came to us for an operation and not for anesthesia,
Page 1 Revised 05/28/08 TRAUMA CARE If the patient arrives intubated that simplifies things. Quickly move the patient to the operating bed. The patient came to us for an operation and not for anesthesia,
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Battlefield Transfusions
 Battlefield Transfusions Chapter 33 Battlefield Transfusions Introduction About 87% of battlefield deaths occur in the prehospital environment. Of these, 24% have been deemed to be potentially survivable,
Battlefield Transfusions Chapter 33 Battlefield Transfusions Introduction About 87% of battlefield deaths occur in the prehospital environment. Of these, 24% have been deemed to be potentially survivable,
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
PEDIATRIC MASSIVE TRANSFUSION
 PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
PEDIATRIC MASSIVE TRANSFUSION CHELSEA RUNKLE RN, BSN, CCRN, SRNA CROZER-CHESTER MEDICAL CENTER/VILLANOVA UNIVERSITY NURSE ANESTHESIA PROGRAM LEADING CAUSE OF DEATH Trauma Motor vehicle accidents, nonaccidental
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
ORIGINAL RESEARCH. Effects of Intravenous Fluid Therapy on Clinical and Biochemical Parameters of Trauma Patients
 90 Emergency (2014); 2 (2): 90-95 ORIGINAL RESEARCH Effects of Intravenous Fluid Therapy on Clinical and Biochemical Parameters of Trauma Patients Shahram Paydar 1*, Hamid Bazrafkan 1, Nasim Golestani
90 Emergency (2014); 2 (2): 90-95 ORIGINAL RESEARCH Effects of Intravenous Fluid Therapy on Clinical and Biochemical Parameters of Trauma Patients Shahram Paydar 1*, Hamid Bazrafkan 1, Nasim Golestani
Implementation of massive transfusion protocol (MTP) for trauma
 for trauma") LEADING ARTICLE Implementation of massive transfusion protocol (MTP) for trauma 1,2 2 2 R.N. Ellawala, K. Gonsalkorala, I.S. Wijesiriwardena 1 Department of Surgery, Faculty of Medicine, General Sir John
LEADING ARTICLE Implementation of massive transfusion protocol (MTP) for trauma 1,2 2 2 R.N. Ellawala, K. Gonsalkorala, I.S. Wijesiriwardena 1 Department of Surgery, Faculty of Medicine, General Sir John
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Bleeding and Shock. Circulatory System
 Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER?
 TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
TRANSFUSION SAFETY 101 ARE YOU SMARTER THAN A BLOOD BANKER? 1. Fatal blood transfusion reactions are most likely the result of: a. Circulatory overload b. ABO incompatible blood due to patient identification
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
Where Have we Come From, and Where are we Going
 Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency
Where Have we Come From, and Where are we Going James Augustine, MD, FACEP Emergency Physician and Fire/EMS Medical Director Naples, Atlanta, and Dayton Clinical Professor, Wright State Univ. Dept of Emergency