Update on Agents for Type 2 Diabetes
|
|
|
- Janis Freeman
- 6 years ago
- Views:
Transcription
1 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific concerns, adverse drug reactions, and contraindications Discuss the role and timing of combination therapy in achieving A1C goals Explain the implications of recent, large randomized clinical trials on clinical decision-making
2 AACE Diabetes Algorithm Guide therapy based on A1C level Focus on lifestyle intensification at all levels Important tenets: Target A1C is <6.5% Based on associated lower risk of micro- and macrovascular complications Recommend monitoring A1C quarterly, along with fasting and postprandial blood glucose, with intensification of therapy until goal A1C is achieved Individualize A1C target based on comorbidities Patient should monitor fasting and postprandial blood glucose levels Use agents with maximal efficacy, associated with lowest risk of hypoglycemia Sulfonylureas are therefore much lower in algorithm Earlier use of incretin mimetics and DPP-4 inhibitors to stimulate insulin secretion without hypoglycemia A1C = glycated hemoglobin; DPP-4 = dipeptidyl-peptidase 4 AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2017,doi: /EP CS.

3

4 UKPDS: Benefits of Glycemic Control Every 1% decrease in A1C led to significant reductions in diabetes-related complications 14% Risk of myocardial infarction 21% Risk of diabetesrelated death Decrease was statistically significant for all comparisons shown 37% Risk of microvascular complications 43% Risk of amputation or PVD death Stratton IM et al. BMJ. 2000;321: PVD=Peripheral Vascular Disease


5 Pathogenesis of Type 2 Diabetes Insulin Resistance: Receptor And Post-receptor Defects Increased Glucose Production Insufficient Glucose Disposal Glucose X Liver Peripheral Tissues (skeletal muscle) Pancreas Impaired Insulin Secretion DeFronzo et al. Diabetes Care. 1992;15:
6 UKPDS: Beta-Cell Loss Over Time Dashed line shows extrapolation forward and backward from years 0 to 6 from diabetes diagnosis, based on Homeostasis Model Assessment (HOMA) data from UKPDS. -Cell Function (%) * l -12 Impaired Glucose Tolerance l -10 Postprandial Hyperglycemia l -6 Type 2 Diabetes Phase I: OAD l l l Years from Diagnosis Type 2 Diabetes Phase II: OAD ± Basal Insulin The data points for the time of diagnosis (0) and the subsequent 6 years are taken from the obese subset of the UKPDS population and were determined by the HOMA model. l 6 Late T2DM: Basal/Bolus l 10 l 14 HOMA = homeostasis model assessment; OAD = oral anti-diabetic; T2DM = type 2 diabetes mellitus; UKPDS = United Kingdom Prospective Diabetes Study Group. 1. Lebovitz HE. Diabetes Rev. 1999;7(3):

7 Current Antihyperglycemic Medications Glinides Sulfonylureas TZDs Insulin replacement therapy Restore postprandial insulin patterns Generalized insulin secretagogue Reduce peripheral insulin resistance Biguanide Reduces hepatic insulin resistance GLP-1 analogs Stimulate beta-cells Suppress glucagon 12 groups with different mechanisms of action SGLT-2 inhibitors Block renal glucose reabsorption DPP-4 inhibitors Restore GLP-1 Levels Amylin analog Suppresses glucagon -Glucosidase inhibitors Delay CHO absorption Colesevelam Bile acid sequestrant Bromocriptine Hypothalamic pituitary reset CHO = carbohydrate; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium-dependent glucose cotransporters-2; TZD = thiazolidinedione.

8

9 Algorithm to Achieve Glycemic Goals Baseline A1C 6.5% - 7.5% Monotherapy may be effective in this range Metformin first choice for monotherapy if no contraindications Consider DPP-4 if PP and FPG, GLP-1 if PP, TZD if metabolic syndrome or NAFLD, AGI if PP Do not recommend secretagogue (SU or glinide) in this range due to risk of hypoglycemia; short-lived effect If monotherapy is unsuccessful, move on to dual oral rx; often need to augment reduction in PP BG to get to goal in this A1C range DPP-4 = dipeptidyl peptidase-4; PP = post-prandial; FPG = fasting plasma glucose; GLP-1 = glucagon-like peptide-1; TZD = thiazolidinedione; NAFLD = non-alcoholic fatty liver disease; AGI = alpha-glucosidase inhibitor; SU = sulfonylurea; A1C = glycated hemoglobin; SGLT-2 = sodium glucose transport-2 AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2017,doi: /EP CS.

10 Algorithm to Achieve Glycemic Goals Baseline A1C 7.6%-9.0% Dual therapy with metformin provides superior glycemic control over metformin alone. If dual oral rx is unsuccessful, consider triple therapy If triple oral rx fails to achieve A1C goal, initiate insulin GLP-1 RA = glucagon-like peptide-1 receptor agonist DPP4-I = dipeptidyl peptidase 4 inhibitor TZD = thiazolidinedione SGLT-2 = sodium glucose cotransporter 2 inhibitor QR = quick-release AG-I = alpha-glucosidase inhibitor SU = sulfonylurea GLN = glinide AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2017,doi: /EP CS.

11 Algorithm to Achieve Glycemic Goals Baseline A1C >9.0% If patient is asymptomatic with recent onset of disease and drug naïve, may consider starting with dual or triple oral regimens If symptomatic, start insulin Once A1C has improved to <7.5%, consider initiation of dual oral therapy with tapering and possible discontinuation of insulin rx AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2017,doi: /EP CS.








12 Targeted Sites of Action of Oral Anti-Hyperglycemic Drug Classes Liver Skeletal Muscle Pancreas Gut Fat Kidney Brain Biguanides TZDs DPP-IV inhibitors Sulfonylureas TZDs Insulin DPP-IV Inhibitors Sulfonylureas Glinides TZDs Amylin α-glucosidase inhibitors Biguanides Colesevelam GLP-1 RA TZDs SGLT-2 inhibitors Bromocriptine Glucose production Glucose uptake Insulin release Glucose absorption Insulin sensitivity Glucose reabsorption Glucose production DPP = dipeptidyl peptidase; SGLT-2 = Sodium-glucose co-transporter 2; TZD = thiazolidinediones Fonseca V. Clin Ther. 2014;36: Sonne DP. Eur J Endocrinol Inzucchi S, et al. Diabetes Care. 2012;35: ; Diabetologia. 2012;55:
13 Clinical Considerations Combining therapeutic agents with different modes of action may be advantageous In many if not most patients (unless contraindicated or intolerance has been demonstrated), use metformin, which increases insulin sensitivity, and/or insulin sensitizers such as TZDs, as part of the therapeutic regimen Dosage of secretagogues or insulin should be adjusted as blood glucose levels decline when used in combination with metformin, TZD, DPP-4 inhibitors, and/or incretin mimetics (GLP-1 agonists) TZD = thiazolidinediones; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1 AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3): Sitagliptin [package insert]. Whitehouse Station, NJ; Merck Co. Inc.; Saxagliptin [package insert]. Princeton, NJ; Bristol Meyers Squibb; 2009; Linagliptin [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals
14 1. Precose [PI]. West Haven, CT: Bayer; 2003; 2. Hanefeld M et al. Diabetes Care. 2000;23: ; 3. Sitagliptin PI, Merck & Co, Inc, Whitehouse Station, NJ, 2010;1-23; 4. Kerr et al. Ann Pharm. 2010;44: ; 5. Blonde et al. Diab Obes Metab. 2009;11(S3):26-34; 6. Nelson P, et al. Diabetes Technol Ther. 2007;9: ; 7. Aronoff S, et al. Diabetes Care. 2000;23: ; 8. Lebovitz HE, et al. J Clin Endocrinol Metab. 2001;86: ; 9. Goldberg RB et al. Diabetes Care. 1996;19(8): ; 10. Simonson DC et al. Diabetes Care. 1997;20(4): ; 11. Garber AJ, et al. Am J Med. 1997;102: Invokana PI. Janssen Pharmaceuticals, Inc.Titusville, NJ Antihyperglycemic Monotherapy Maximum Therapeutic Effect, Dependent Upon Initial A1C Baseline A1C Acarbose Nateglinide Sitagliptin Bromocriptine Liraglutide Exenatide Pioglitazone Repaglinide Glimepiride Glipizide GITS Metformin Canagliflozin Insulin A1C = glycated hemoglobin; GITS = gastrointestinal therapeutic system. Reduction in A1C Level (%)
15 Effect of Glucose-lowering Drugs on Patient Weight Therapeutic Options Weight Sulfonylurea 1,2 TZD 3,4 Insulin 5,6 Metformin 7 DPP-4 inhibitor 8 GLP-1 receptor agonist 9 SGLT-2 Inhibitors 10 A1C = glycated hemoglobin; DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; SGLT-2 = sodium glucose co-transporter-2; TZD = thiazolidinedione 1. Malone M. Ann Pharmacother. 2005;39: Glipizide [package insert]. New York, NY; Pfizer; Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America; Rosiglitazone [package insert]. Research Triangle Park, NC; GlaxoSmithKline; Nathan DM, et al. Diabetes Care. 2008;31(1): Holman RR. NEJM. 2007;357(17): Metformin[package insert]. Princeton NJ; Bristol Meyers Squibb; Sitagliptin [package insert]. Whitehouse Station, NJ; Merck and Co.; Drucker DJ, et al. J Clin Invest. 2007;117(1): Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ
16 Risk of Hypoglycemia Plays a significant role in choice of agents in AACE algorithm For patients at highest risk of hypoglycemia, may consider close evaluation of agents chosen as well as therapeutic goal Patients with type 2 diabetes at highest risk of low blood glucose include those with: Diabetes duration >15 years Advanced macrovascular disease Hypoglycemia unawareness Limited life expectancy Severe comorbidities AACE Comprehensive Diabetes Management Algorithm Endocr Pract. 2013;19(3): ; AACE Algorithm for Glycemic Control, Endocr Pract. 2009;15(6):
17 Biguanides Metformin Mechanism Insulin sensitivity Hepatic glucose production FPG more than PPG Efficacy A1C 1%-2% Advantages Disadvantages Contraindications No weight gain or hypoglycemia, potential weight loss GI side effects Lactic acidosis (rare) Renal disease; CHF Combinations available with SU, TZD, repaglinide, and DPP-4 inhibitors A1C = glycated hemoglobin; CHF = congestive heart failure; DPP-4 = dipeptidyl peptidase-4; FPG = fasting plasma glucose; GI = gastrointestinal; PPG = post-prandial glucose; SU = sulfonylurea; TZD = thiazolidinedione Metformin [package insert]. Princeton NJ; Bristol Myers Squibb; 2009.
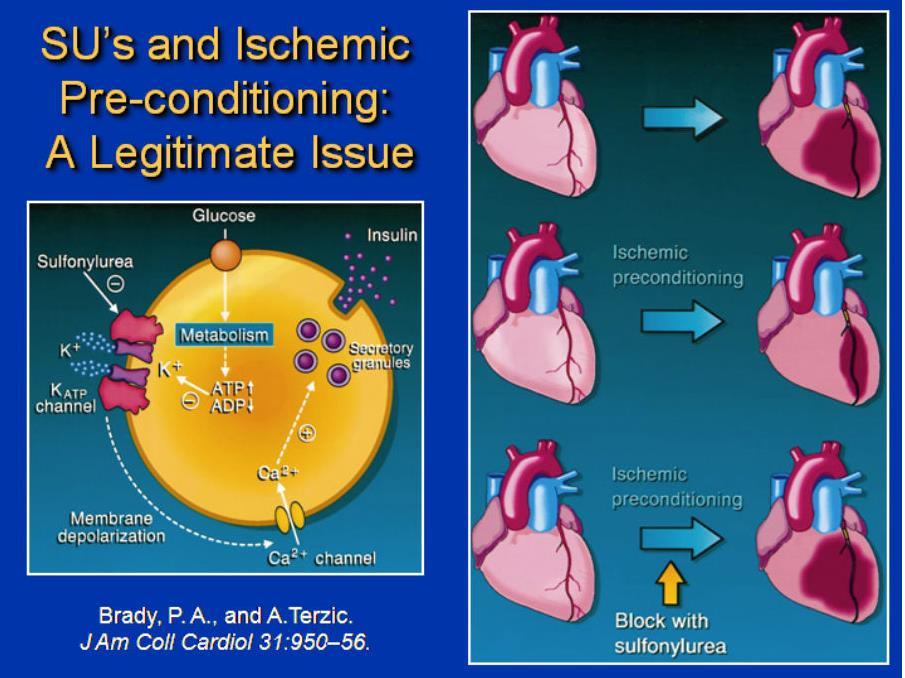
18 Mechanism Sulfonylureas and Glinides Glipizide, Glimepiride, Glyburide Repaglinide, Nateglinide Insulin secretion FPG PPG Efficacy Advantages Moderate Strong short term efficacy Disadvantages Contraindications Weight gain, hypoglycemia, tend to lose efficacy after several years Avoid in severe hepatic and renal impairment Combinations available with metformin, TZD FPG = fasting plasma glucose; PPG = post-prandial glucose; TZD = thiazolidinedione Glyburide [package insert]. New York, NY; Pfizer; Glipizide [package insert]. New York, NY; Pfizer; Glimepiride [package insert]. Scoppito, Italy; Aventis Pharma S.p.A; Kahn SE, et al. NEJM. 2006;355:23.
 Secretory granules GLUT 2 Glucose Brady PA, et al. J Am Coll Cardiol. 1998;31:950-956.")
19 Sulfonylurea-driven Insulin Secretion Is Not Glucose-sensitive SU Ca ++ ATP-sensitive K + channel SUR Depolarization Voltage-dependent Ca ++ channel K + h ATP mitochondrion Pyruvate Glucose-6-Phosphate Glucokinase Nucleus (islet transcription factors) Secretory granules GLUT 2 Glucose Brady PA, et al. J Am Coll Cardiol. 1998;31: Insulin and amylin


20
21 Thiazolidinediones Pioglitazone, Rosiglitazone Mechanism Insulin sensitivity, especially at muscle, lowers both FPG and PPG, but effect may be delayed Efficacy Moderate ( A1C 1.0%-1.5%) Advantages No hypoglycemia, no reliance on renal excretion Disadvantages Contraindications Fluid retention, edema, heart failure, weight gain, slow onset of action, bone fractures, macular edema, osteoporosis, anemia, and bladder cancer Class III or IV CHF or hepatic impairment w/alt >2.5 times upper normal limits Combinations available with metformin and sulfonylurea A1C = glycated hemoglobin; ALT = alanine aminotransferase; CHF = congestive heart failure; FPG = fasting plasma glucose; PPG = postprandial plasma glucose. Pioglitazone [package insert]. Deerfield, IL: Takeda Pharmaceuticals America, Rosiglitazone Prescribing Information. Research Triangle Park, NC: GlaxoSmithKline, 2013.

:S162-74, 2013.")
22 TZD Mechanism of Action Effect of Medications on Fat Topography IR, TG, FFA Insulin, BP, Inflammation Endo dysf Intra-muscular fat Intra-hepatic fat TZD Subcutaneous fat Intra-abdominal fat Direct PPAR effect on vascular cells to decrease endothelial dysfunction and inflammation IR, TG, FFA Insulin, BP Inflammation Endo dysf Eldor R, et al. Diabetes Care. 36(suppl 2):S162-74, TZD=Thiazolidinedione IR=Insulin Resistance TG=Triglycerides BP=Blood Pressure PPAR=Peroxisome Proliferator- Activated Receptors
23 PROactive Study >5,000 patients in 19 European countries involving over 320 investigators Investigated effect of insulin resistance on CV morbidity and mortality in patients with T2DM Investigated pioglitazone s ability to prevent the progression of macrovascular disease The primary endpoint was time to first occurrence of any of the following events from time of randomization: All-cause mortality Stroke Leg revascularization Non-fatal MI (including silent) CV = cardiovascular; T2DM = type 2 diabetes mellitus Major leg amputation (above the ankle) Acute coronary syndrome Cardiac intervention PROspective Actos Clinical Trial In macrovascular Events (PROactive) results. Accessed February 2011.
24 Kaplan-Meier Event Rate Kaplan-Meier Event Rate PROactive Study, Secondary Endpoints Pioglitazone Had No Significant Effect on Primary Composite CV Endpoints Time to ACS PIO Placebo Benefit Seen in Select Secondary Endpoints (35/1230) (54/1215) Time to Fatal/Nonfatal MI (excluding silent MI) PIO (65/1230) (88/1215) Placebo N at Risk: HR 95% CI P value PIO vs placebo , (139) N at (139) Risk: l l l l l l l l l l l l l 6 l 12 l 18 l 24 Time From Randomization (mo) CV = cardiovascular; ACS = acute coronary syndromes; MI = myocardial infarction The official PROspective Actos Clinical Trial In macrovascular Events (PROactive) results website. Available at Dormandy JA, et al. Lancet. 2005;366: PIO vs placebo HR 95% CI P value , Time From Randomization (mo) PROactive results Web site. Available at results.com /html/analysis.htm. October 10, 2006.
25 Alpha-Glucosidase Inhibitors Acarbose, Miglitol Mechanism Efficacy Advantages Disadvantages Contraindications Rate of gut polysaccharide breakdown, thereby slowing absorption Modest ( A1C 0.5%-1.0%), PPG lowering Weight-neutral, non-systemic drug, targets postprandial glucose Bloating, flatulence, diarrhea w/slow titration, frequent dosing Severe renal impairment, diabetic ketoacidosis, malabsorption, obstruction, inflammatory bowel, or conditions aggravated by gas production Combinations available with sulfonylureas A1C = glycated hemoglobin; PPG = post-prandial glucose Acarbose [package insert]. Wayne, NJ; Bayer HealthCare Pharmaceuticals Inc.; Miglitol [package insert]. Wayne, NJ; Bayer HealthCare Pharmaceuticals Inc.; 2010.
26 Mechanism Dopamine Receptor Agonist Bromocriptine QR Exact mechanism of action unclear, believed to reduce sympathetic tone, inflammation, and insulin resistance Efficacy Modest ( A1C 0.5%) Advantages Disadvantages Contraindications May decrease cardiovascular risk Hypotension, syncope, hypoglycemia, nausea History of psychosis or during breastfeeding. Use caution with renal or hepatic impairment. A1C = glycated hemoglobin; QR = quick-release Cincotta et al. Taylor and Francis, Eds Hansen, B Shafrir, E London, Defronzo RA et al. Diabetes Care Apr;34(4):
27 Bromocriptine QR: Proposed Mechanism of Action Morning administration (within 2 hours Corrects of waking) Low dopaminergic tone in hypothalamus in early morning in diabetes Restoration of morning peak in dopaminergic activity (via D2 receptor-mediated activity) Sympathetic tone HPA axis tone Hepatic gluconeogenesis FFA and TG Insulin resistance Inflammation/hypercoagulation Sympathetic tone HPA axis tone Hepatic gluconeogenesis FFA and TG Insulin resistance Inflammation/hypercoagulation Impaired glucose metabolism, hyperglycemia, and insulin resistance Adverse cardiovascular pathology FFA = free fatty acid; HPA = hypothalamic-pituitary-adrenal; TG = triglyceride Cincotta et al. Taylor and Francis, Eds Hansen, B Shafrir, E London, Defronzo RA et al. Diabetes Care Apr;34(4): Decreased postprandial glucose levels Reduction in insulin resistance Day-long reduction in plasma glucose, TGs, and FFAs 27

28 Ranolazine Can Be Used in Patients with Ranolazine does not increase the incidence of hypoglycemia vs placebo Indicated to treat chronic angina but does have glucose-lowering effects Does not increase incidence of: Weight gain Cardiovascular adverse events Dyslipidemia (LDL, HDL, total cholesterol, and triglycerides Clinically relevant changes in blood pressure or heart rate CAD and Diabetes CAD = coronary artery disease; HDL = high-density lipoprotein; LDL = low-density lipoprotein Timmis AD, et al. Eur Heart J 2006;27: Ranexa Prescribing Information.
29 Bays HE, et al. Arch Intern Med. 2008;168: Fonseca VA, et al. Diabetes Care. 2008; 31: Fonseca V, et al. Diabetes Obes Metab. 2010;12(5); Goldberg RB, et al. Arch Intern Med. 2008;168: ; Colesevelam [package insert]. Parsippany, NJ; Daiichi Sankyo, Mechanism Bile Acid Sequestrants Colesevelam Efficacy Modest ( A1C 0.5%) Advantages Disadvantages Raises cholecystokinin, which slows gastric emptying and post-prandial glucose Exact mechanism unknown, may be mediated via TGR5, and/or farnesoid X receptor (FXR/bile acid receptor) effects on intestinal glucose LDL-C (also FDA approved for LDL-C reduction) weight neutral, no hypoglycemia, can complement statin treatment in lowering LDL and cardiac event risk Constipation, nausea, dyspepsia, myalgia, pharyngitis, triglycerides, drug interactions Contraindications History of bowel obstruction, TGs >500 mg/dl; history of hypertriglyceridemiainduced pancreatitis A1C = glycated hemoglobin; LDL-C = low-density lipoprotein cholesterol; TG = triglyceride
 -0.")


30 Effects of Colesevelam on A1C Levels in Add-On Therapy Trials: 0.5% Reductions GLOWS Week 12 Metformin Week 26 Sulfonylurea Week 26 Insulin Week 16 Mean Change in A1C (%) * P n = >1, * -0.54* -0.54* -0.50* Zieve FJ et al. Clin Ther. 2007;29:74. Bays H et al. Presented at: AACE 16th Annual Meeting & Clinical Congress; April Abstract 204. Fonseca VA et al. Presented at: AACE 16th Annual Meeting & Clinical Congress; April Abstract 409. Goldberg RB et al. Presented at: AHA Scientific Sessions; November 2006; Chicago, IL. Poster
31 Strategies for Enhancing GLP-1 Action GLP-1 receptor agonists (injectable therapies) Short acting: exenatide BID, liraglutide, lixisenatide Long acting: exenatide QR, albiglutide, dulaglutide Under investigation: semaglutide and ITCA 650 DPP-4 inhibitors (oral therapies) Inhibit actions of DPP-4 Sitagliptin, saxagliptin, linagliptin, alogliptin
32 Rationale for Using Incretin-Based Therapies in the Treatment of Type 2 Diabetes Incretins play a key role in maintaining glucose homeostasis Incretin effects are diminished in patients with type 2 diabetes Incretin-based therapies Target multiple defects of type 2 diabetes, including those not addressed by traditional medications Do not cause hypoglycemia Have favorable effects on weight
 80 60 Incretin Effect 0.6 0.5 0.4 80 60 0.6 0.5 0.4 40 0.")

33 IR Insulin, mu/l IR Insulin, mu/l The Incretin Effect Control subjects (n=8) Type 2 diabetes (n=14) Incretin Effect nmol / L nmol/l Time, min Time, min 180 Nauck M et al. Diabetologia. 1986;29: Copyright 1986 Springer-Verlag.




34 GLP-1 Modulates Numerous Functions in Humans GLP-1: Secreted upon the ingestion of food Beta-cells: Enhances glucose-dependent insulin secretion Brain promotes satiety and reduces appetite Alpha cells: Glucose-dependent postprandial glucagon secretion Liver: Glucagon reduces hepatic glucose output Stomach: Helps regulate gastric emptying GLP-1 = glucagon-like peptide-1. Data from Flint A, et al. J Clin Invest. 1998;101: ; Data from Larsson H, et al. Acta Physiol Scand. 1997;160: Data from Nauck MA, et al. Diabetologia. 1996;39: ; Data from Drucker DJ. Diabetes. 1998;47:
35 Inhibition of DPP-4 Increases Active Incretin Levels, Enhancing Downstream Incretin Actions Active GIP Active GLP-1 Increased insulin secretion Decreased glucagon release DPP-4 DPP-4 inhibitor Inactive GIP Inactive GLP-1 Glucose control improved Umpierrez et al. Endocrine Practice 2014
36 Characteristics of DPP-4 Inhibitors Alogliptin, Linagliptin, Saxagliptin, Sitagliptin Mechanism Inhibit enzymatic degradation of GLP-1 and GIP; glucose-dependent Efficacy Decrease A1C levels 0.6% 0.9% Dosing Side effects Main risk Once daily Headaches, nasopharyngitis Viral infection; long-term safety unknown A1C = glycated hemoglobin; GIP = gastric inhibitory polypeptide; GLP-1 = glucagon-like peptide-1 Rosenstock J, et al. Curr Opin Endocrinol Diabetes Obes. 2007;14: Nathan DM, et al. Diabetes Care. 2008;31:
37 ΔHbA1C (%) Comparative Efficacies of DPP-4s Placebo-corrected Change From Baseline In A1C: Monotherapy Alogliptin mg 25mg 7.9% 7.9% Linagliptin 2 5mg 5mg 8.1% 8.0% Saxagliptin 2 5mg 5mg 7-10% 8.0% Sitagliptin 2 100mg 100mg 8.0% 8.0% Vildagliptin 3 50mg BID 50mg 8.6% 8.4% The current DPP-4s have comparative efficacy 1. DeFronzo R, et al. Diabetes Care 2008;31: Linagliptin Prescribing Information. 3. Saxagliptin Prescribing Information. 4. Sitagliptin Prescribing Information.5. Vildagliptin Summary of Product Characteristics.
38 Summary of DPP-4 Inhibitors Average A1C Change in Clinical Trials DPP-4 Inhibitor Monotherapy Initial with Metformi n Add-on to Metformin Add on to SU Add on to TZD Initial with TZD Alogliptin Linagliptin (SU + Met) Saxagliptin Sitagliptin Nesina (alogliptin) prescribing information. Deerfield, IL: Takeda Pharmaceuticals America, Inc.; 2013.
39 Injectable Therapies: GLP-1 RA Introduction to the incretin effect and GLP-1 Effects of GLP-1 on glucose regulation GLP-1 as a model therapy for diabetes Effects of GLP-1 on islet mass Non-glycemic effects of GLP-1 GLP-1 = glucagon-like peptide-1; GLP-1 RA = glucagon-like peptide-1 receptor agonist.

40 GLP-1 RA Increases Active Incretin Levels Normal Physiology Active GLP-1 DPP-4 Inactive GLP-1 DPP-4 inhibitor GLP-1 RA Resistance Increased circulating GLP-1 levels Increased insulin secretion Decreased glucagon release Umpierrez et al. Endocrine Practice 2014 Glucose control improved DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1; GLP-1 RA = glucagon-like peptide-1 receptor agonist.
41 Metabolic Effects of GLP-1 in Patients with Type 2 Diabetes Improves glucose-dependent insulin secretion Decreases plasma glucagon concentration Decreases fasting and postprandial glucose concentration Lowers A1C A1C = glycated hemoglobin; GLP-1 = glucagon-like peptide-1. Zander M et al, Lancet 2002, 359:
42 Characteristics of GLP-1 Agonists Exenatide, Liraglutide, Albiglutide, Dulaglutide Mechanism Efficacy Mimic prolonged action of GLP-1 Decrease A1C levels 0.5% 2.0% (depends on entry of glucose into bloodstream from gut) Dosing Once- or twice-daily injection, weekly * Side effects Main risk Associated with Nausea, vomiting, weight loss C-cell thyroid tumors**, long-term safety unknown Pancreatitis possible *Dosing depends on GLP-1 agonist **With liraglutide, in rodents only A1C = glycated hemoglobin; GLP-1 = glucagon-like peptide-1. Nathan DM, et al. Diabetes Care. 2008;31: ; Drucker DJ, et al. Lancet. 2006;368: Exenatide [package insert]. San Diego, CA; Amylin Pharmaceuticals; 2010.; Tanzeum (albiglutide) [prescribing information].

43 Exenatide (Exendin-4) Development of Exenatide: Synthetic version of salivary protein found in the Gila monster Approximately 50% identity with human GLP-1 Binds to known human GLP-1 receptors on β cells in vitro Resistant to DPP-4 inactivation Administered twice daily An Incretin Mimetic DPP-4 = dipeptidyl peptidase-4; GLP-1 = glucagon-like peptide-1. Nielsen LL, et al. Regul Pept. 2004;117: Fineman MS, et al. Diabetes Care. 2003;26:
44 GLP-1 Receptor Agonists Exenatide BID (twice daily) Liraglutide (once daily) Exenatide ER (weekly) Albiglutide (weekly) Dulaglutide (weekly) Lixisenatide (once daily) BID = twice daily; ER = extended release; GLP-1 = glucagon-like peptide-1.
45 Marketed GLP-1 RAs Exenatide BID Liraglutide Exenatide ER Albiglutide Dulaglutide Lixisenatide Initial U.S. approval Trade name Description Byetta Victoza Bydureon Tanzeum (US) Eperzan (EU) Synthetic exendin-4, a peptide identified in H. suspectum that activates GLP-1 and is resistant to DPP-4 degradation GLP-1 modified a to be resistant to DPP-4 degradation Exenatide contained in a hydrolyzable polymer microspheres for extended release An albumin fusion protein made of 2 copies of modified human GLP-1 Trulicity A fusion protein with 2 disulfidelinked human GLP-1 analog sequence chains, connected by a small peptide linker to human immunoglobulin G4 (IGG4) Adlyxin (US) Lyxumia (EU) A peptide containing 44 amino acids, amidated at the C-terminal amino acid (position 44) Half-life 2.4 hours 13 hours > 1 week 5 days 5 days 3 hours Dosing 2X daily, before meals 1X daily, any time 1X weekly 1X weekly 1X weekly a Amino acid substitution and addition of acyl chain. BID = twice daily; DPP-4 = dipeptidyl peptidase-4; ER = extended release; E.U. = European Union; GLP-1 = glucagon-like peptide-1; IGG4 = human immunoglobulin; U.S. = United States. Byetta (exenatide) [Prescribing Information (PI)]; Victoza (liraglutide) [PI]; Bydureon (exenatide extended-release for injectable suspension) [PI].; Neumiller JJ. J Am Pharm Assoc. 2009;49(S1):S16-S29.; DeYoung M, et al. Diabetes Technol Ther. 2011;13: ; Tanzeum (albiglutide) [PI]; Lyxumia (lixisenatide) [PI]; Trulicity (dulaglutide) [PI]; Kuritzky L, et al. PostGrad Med. 2014;126(6): X daily, before 1st meal
 are available in multi-dose pens Various studies have examined patient preferences Lixisenatide and liraglutide pens have higher patient satisfaction compared to")

46 GLP-1 Devices All GLP-1 RAs are available in pre-filled pens 1 Weekly GLP-1 RAs (exenatide ER, albiglutide, and dulaglutide) are available in single-dose pens Weekly GLP-1 RAs (exenatide BID, liraglutide, and lixisenatide) are available in multi-dose pens Various studies have examined patient preferences Lixisenatide and liraglutide pens have higher patient satisfaction compared to exenatide 2 Dulaglutide is the only weekly GLP-1 RA available in a ready-to-use formula that does not require reconstitution 3 New technology is being developed for an implantable, continuous subcutaneous delivery system for GLP-1 RAs 4 BID = twice daily; ER = extended release; GLP-1 = glucagon-like peptide-1 ; GLP-1 RA = glucagon-like peptide-1 receptor agonist. 1. MIMS. Diabetes Visual Guide Stauder U, et al. J Diabetes Sci Technol Jan; 8(1): Amblee A. Patient Prefer Adherence. 2016;10: Diabetes in Control. Intarcia Platform Technology
47 GLP-1 Analogues GLP-1-based therapies can be classified into 3 main types: Exendin-based 1 Includes exenatide and exenatide ER 1 Antibody development is most likely with this type due to lower sequence identity with native GLP-1 2 DPP-4 resistant 1 Includes lixisenatide and albiglutide Analogues of human GLP-1 1 Includes liraglutide and semaglutide, which are currently under development ER = extended release; GLP-1 = glucagon-like peptide-1 ; DPP-4 = dipeptidyl peptidase Gupta V. Indian J Endocrinol Metab. 2013;17(3): Garber AJ. Diabetes Care 2011;34(Supplement 2):S279-S284.
48 Exenatide Exenatide BID: 5 mcg SC 60 min AC BID After 1 month: 10 mcg SC 60 min AC BID Supplied as pen (use:1 per month) Exenatide ER: 2 mg SC QWK Available as single-dose tray or pen AC = before meals; BID = twice daily; ER = extended release; SC = subcutaneously; QWK = every week. Bydureon [package insert]. West Chester, OH: Amylin Ohio LLC; Byetta [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2015.
49 Exenatide ER 2 mg SC every 7 days, with or without food Reconstituted w/ diluent; 23G x 5/16 needle Microsphere release; steady state: 6-7 wks A1C reduction vs BID exenatide: ~0.7% Not recommended as first-line Rx Add on to MET, SU, TZD, or combination Less nausea vs exenatide BID weight loss vs exenatide BID: 3.53 lbs vs 1.98 lbs at 24 wks A1C = glycated hemoglobin; BID = twice daily; ER = extended release; lbs= pounds; MET = metformin; Rx = prescription; SC = subcutaneously; SU = sulfonylurea; TZD = thiazolidinedione. Bydureon [package insert]. West Chester, OH: Amylin Ohio LLC; 2015.
50 Injected SC once-daily Liraglutide Acylated GLP-1(C-16 fatty acid, palmitic acid, on position 26) Liraglutide is extensively bound to plasma protein (greater than 98%) 97% homology to GLP-1 Endogenously metabolized without specific organ as major route of elimination GLP-1 = glucagon-like peptide-1; SC = subcutaneously. Victoza [package insert]. Plainsboro, NJ: Novo Nordisk; 2016.
51 Liraglutide Liraglutide: 0.6 mg SC QD x 1 week then 1.2 mg SC QD increase to 1.8 mg SC QD if needed Supplied as pen Use: 2-3 pens per month QD = once daily; SC = subcutaneously. Victoza [package insert]. Plainsboro, NJ: Novo Nordisk; 2016.
52 Latest Once-weekly GLP-1 Receptor Agonists Albiglutide (modified GLP-1 fused to albumin) Dulaglutide (GLP-1 analog fused to IGG4) Semaglutide (structural analog of liraglutide) Not FDA approved, in Phase 3 clinical trials Resistant to DPP-4 degradation Similar efficacy as exenatide ER A1C reduction 0.8% 1.0% Studied with metformin, SU, pioglitazone, basal insulin Not recommended as first-line therapy A1C = glycated hemoglobin; DPP-4 = dipeptidyl peptidase-4; ER = extended release; FDA = U.S. Food and Drug Administration; GLP-1 = glucagon-like peptide-1; IGG4 = human immunoglobulin; SU = sulfonylurea.
53 Albiglutide 30 mg SC QWK Increase to 50 mg SC QWK if needed Supplied as single-dose prefilled pen QWK = every week ; SC = subcutaneously. Tanzeum [package insert]. Wilmington, DE: GlaxoSmithKline LLC; 2016.
54 Albiglutide is an GLP-1 agonist Albiglutide Efficacy - Approved by the U.S. FDA on April 15, 2014 The Harmony program, consisting of 8 phase III studies, evaluated safety and efficacy - Albiglutide causes significant reductions in A1C in patients with T2DM when used alone or as add-on therapy with combinations of metformin, pioglitazone, and glimepiride, with decreases from baseline A1C ranging from -0.75% to- 0.91% - Additionally, albiglutide produced superior A1C control to mealtime insulin lispro at 26 weeks Albiglutide use results in moderate weight loss A1C = glycated hemoglobin; FDA = Food and Drug Administration; GLP-1 = glucagon-like peptide-1; T2DM = type 2 diabetes mellitus. Woodward HN et al. Patient Prefer Adherence. 2014;8:
55 Dulaglutide 0.75 mg SC QWK Increase to 1.5 mg SC QWK if needed Supplied as single-dose prefilled pen or prefilled syringe QWK = every week; SC = subcutaneously. Trulicity [package insert]. Indianapolis, IN: Eli Lilly and Co.; 2015.
56 Dulaglutide Efficacy Dulaglutide is a GLP-1 agonist - Approved by the U.S. FDA on September 18, 2014 Six phase III clinical trials evaluated the safety and efficacy of dulaglutide as monotherapy or in combination with other diabetes medications - Dulaglutide causes significant reductions in A1C in patients with T2DM when used alone or as an add-on therapy with metformin, metformin + sulfonylurea, and metformin + thiazolidinedione - Additionally, dulaglutide produced superior A1C control to insulin glargine at 26 weeks Dulaglutide use results in moderate weight loss; up to 3.1% of body weight A1C = glycated hemoglobin; FDA = Food and Drug Administration; GLP-1 = glucagon-like peptide-1; T2DM = type 2 diabetes mellitus. Dulaglutide/Trulicity [package insert]. Indianapolis, IN: Eli Lilly; 2014.
57 Semaglutide Not FDA approved as of 11/2016 Under investigation in the SUSTAIN phase 3 clinical trial program Long-acting GLP-1, once-weekly dosing Structurally similar to liraglutide FDA = U.S. Food and Drug Administration; GLP-1 = glucagon-like peptide-1; SC = subcutaneously; SUSTAIN = Trial To Evaluate Outcomes with Semaglutide in Subjects with Type 2 Diabetes.
58 Semaglutide Efficacy Semaglutide is a long-acting GLP-1 agonist - Not approved by the FDA as of 11/2016 Six phase III clinical trials (the SUSTAIN phase III clinical trial program) examined semaglutide for safety and efficacy - Semaglutide causes significant reductions in A1C in patients with T2DM compared to sitagliptin, exenatide ER, and insulin glargine - Semaglutide reduced the risk of major CV events by 26% compared to placebo in patients with T2DM at high CV risk - In SUSTAIN 6, A1C was significantly lower in the semaglutide vs placebo group - Results confirmed semaglutide noninferiority Semaglutide use results in moderate weight loss; up to 5.3% of body weight A1C = glycated hemoglobin; ER = extended release; FDA = U.S. Food and Drug Administration; GLP-1 = glucagon-like peptide-1; SUSTAIN = Trial To Evaluate Outcomes with Semaglutide in Subjects with Type 2 Diabetes; T2DM = type 2 diabetes mellitus. Marso SP, et al. N Engl J Med. 2016;375:
59 Exenatide/Byetta PI Liraglutide/Victoza PI Trulicity [package insert]. Indianapolis, IN: Eli Lilly and Co.; Safety: Nausea Most frequent adverse effect of GLP-1 RAs is nausea, which occurs in up to one-third of patients and is usually self-limiting, although some patients cannot tolerate these agents. Nausea may be diminished by avoiding overeating and slowing the titration. Administering exenatide BID closer to mealtime can also decrease nausea. BID = twice daily; GLP-1 RA = glucagon-like peptide-1 receptor agonist.
60 Safety: Medullary Thyroid Cancer Risk All GLP-1 RAs are contraindicated in patients with a personal or family history of MTC or MEN2 because of the occurrence of c- cell tumors in rodents. The c-cell tumor risk in humans is unknown, because human relevance could not be determined in clinical trials. The value of routine calcitonin and/or ultrasound monitoring is uncertain. Patients with thyroid nodules or elevated serum calcitonin levels identified for other reasons should be sent to an endocrinologist. To monitor potential associations, report MTC to state cancer registry, regardless of treatment. GLP-1 RA = glucagon-like peptide-1 receptor agonist; MEN2 = multiple endocrine neoplasia 2; MTC = medullary thyroid cancer. Victoza PI 2013.; Bydureon PI Parks M, et al. N Eng J Med. 2010;362:
61 Safety: Renal Impairment Renal impairment affects the clearance of exenatide BID & ER, but not that of liraglutide, albiglutide or dulaglutide. Hypovolemia due to nausea and vomiting may worsen renal function. Renal impairment with GLP-1 RAs has been reported postmarketing, usually in association with nausea, vomiting, diarrhea, or dehydration. BID = twice daily; ER = extended release; GLP-1 RA = glucagon-like peptide-1 receptor agonist. Linnebjerg H, et al. Br J Clin Pharmacol. 2007;64: Jacobsen L, et al. Br J Clin Parmacol. 2009;68: ; Byetta PI 2013.
62 Safety: Pancreatitis Pancreatitis has been reported with all incretinbased therapies, although no causal relationship has been established. Patients should know signs and symptoms of pancreatitis and stop taking incretin-based therapies if signs and symptoms occur. If pancreatitis is confirmed, therapy should not be restarted. Ahmad SR, et al. N Engl J Med. 2008;358: ; Garg R, et al. Diabetes Care. 2010;33: ; Byetta PI 2013.; Victoza PI 2013.; Bydureon PI 2013.; Januvia PI 2013.; Onglyza PI 2013.; Tradjenta PI 2013.; Nesina PI 2013.
63 LEADER: Liraglutide Over 9,000 high-risk patients with T2D or previous CV events Liraglutide use led to significant CV events reduction CV = cardiovascular; LEADER = Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results; T2D = type 2 diabetes. Marso SP et al., NEJM 2016
64 Patients with an event (%) LEADER Trial: Primary Outcome First occurrence of CV death, nonfatal myocardial infarction, or nonfatal stroke in the time-toevent analysis in patients with type 2 diabetes and high CV risk Hazard ratio, 0.87 (95% CI, ) P<0.001 for noninferiority P=0.01 for superiority 10 5 Placebo Liraglutide 0 Marso SP et al., NEJM Months since randomization CI = confidence interval; CV = cardiovascular; LEADER = Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results.
65 Patients with an event (%) LEADER Trial: Death from Cardiovascular Causes 20 Hazard ratio, 0.78 (95% CI, ) P= Placebo Liraglutide Months since randomization CI = confidence interval; LEADER = Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results. Marso SP et al., NEJM 2016

66 LEADER: Number Needed to Treat to Prevent One CV = cardiovascular; MACE = major adverse cardiovascular event. Presented at the American Diabetes Association 76 th Scientific Sessions, Session 3-CT-SY24. June , New Orleans, LA, USA.
67 Summary: GLP-1 Receptor Agonists Good glycemic efficacy, glucose-dependent action Complement the actions of oral antihyperglycemic agents Can be used as monotherapy if MET is contraindicated and in combination with other oral agents and/or insulin Favorable weight effects and low hypoglycemic risk Consider patient risk factors and educate patients about potential risks and/or adverse effects (eg, nausea, history of thyroid tumors, pancreatitis) No increased risk of pancreatitis relative to other antihyperglycemic agents Potential for gastrointestinal side effects Cardioprotective (LEADER trial) GLP-1 = glucagon-like peptide-1; LEADER = Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results; MET = metformin.
68 Mechanism of action: SGLT2 Inhibitors Decrease re-absorption of glucose in the proximal convoluted tubule Decrease renal threshold so urinary glucose excretion occurs at lower plasma glucose concentration FDA-approved Canagliflozin Dapagliflozin Empagliflozin FDA = U.S. Food and Drug Administration; SGLT-2 = sodium-dependent glucose cotransporters-2. Bays, H. Diabetes Therapy, 2013.
69 Δ A1C, % 1. Stenlöf K, et al. Diabetes Obes Metab. 2013;15: Ferrannini E, et al. Diabetes Care. 2010;33: Roden M, et al. Lancet Diabetes Endocrinol. 2013;1: Efficacy of SGLT2 Inhibitors as Monotherapy a 0.5 CANA 1 PBO DAPA 2 PBO 5 10 EMPA 3 PBO a Phase 3 trials, BL A1C 7.8% to 8.1%, weeks. P<0.001 vs PBO for all

70 Weight Effects with SGLT2 Inhibitors a as Monotherapy Roden M et al. Lancet Diabetes Endocrinol. 2013;1: Stenlöf K et al. Diabetes Obes Metab. 2013;15: Ferrannini E et al. Diabetes Care. 2010;33: US FDA. Drugs@FDA.
71 Renal Glucose Transport in Type 2 Diabetes With increasing plasma glucose, filtered glucose increases in linear relationship When transport system becomes saturated, excess glucose is excreted in urine Renal threshold for glucose is 180 mg/dl in normal glucosetolerant individuals In patients with type 2 diabetes, transport maximum for glucose increases and glucosuria occurs at more elevated glucose levels Glucose reabsorption is enhanced, leading to worsening hyperglycemia Handelsman Y. Endocrine Pract, Bays, H. Diabetes Therapy, 2013; Goldstein DE et al. Diabetes Care, 2004.

72 Sodium Glucose Co-Transporter 2 Reabsorption of glucose is mediated by SGLTs in proximal convoluted tubule Independent of insulin SGLT2 and SGLT1 located on luminal surface of epithelial cells lining proximal convoluted tubule SGLTs in other organs 2: liver 1: small intestine S1 segment of proximal tubule: SGLT2 S3 segment of proximal tubule: SGLT1 90% reabsorption 10% reabsorption 90% glucose is reabsorbed in S1 by SGLT2 Low affinity, high capacity transporter 10% reabsorbed in S3 by SGLT1 High affinity, low capacity transporter Bays, H. Diabetes Therapy, 2013 Chao EC, et al. Nat Rev Drug Discovery. 2010;9:

73 SGLT 2 Inhibition: Meeting Unmet Needs in Diabetes Care Corrects a Novel Pathophysiologic Defect Reduces A1C Promotes Weight Loss Improves Glycemic Control and CVRFs Complements Action of Other Antidiabetic Agents Reduces Blood Pressure No Hypoglycemia Reversal of Glucotoxicity CVRF=Cardiovascular Risk Factor
74 Mechanism SGLT2 Inhibitors Canagliflozin, Dapagliflozin, Empagliflozin Inhibits sodium-glucose transport protein subtype 2 (SGLT2) which is responsible for at least 90% of glucose reabsorption in the kidney causing blood glucose is eliminated in the urine Efficacy Modest ( A1C %) Advantages Disadvantages Contraindications Insulin-independent glucose reduction, Low risk of hypoglycemia, Weight loss (to 4% BW), Blood pressure-lowering Osmotic diuresis causing Polyuria and lightheadedness, Bacterial urinary tract infections ( 5%), Fungal genital infections ( 10%), Increased LDL cholesterol, Hyperkalemia (canagliflozin), Bladder cancer concerns (dapagliflozin) History of genital fungal infections, caution in chronic kidney disease Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ.; Lavalle-gonzález FJ, Januszewicz A, Davidson J, et al. Diabetologia. 2013; Stenlöf K, Cefalu WT, Kim KA, et al. Diabetes Obes Metab. 2013;15(4):372-82; Burki TK. Lancet. 2012;379(9815):507.
75 SGLT2 Inhibitors Safety: Adverse Reactions The most frequent adverse effects of SGLT2 inhibitors (occurring in 5% patients) are female genital mycotic and urinary tract infections Patients may also experience increased urination, dehydration, or nasopharyngitis SGLT2 = sodium-glucose cotransporter-2 Empagliflozin/Jardiance PI 2016.; Dapagliflozin/Farxiga PI 2016.; Canagliflozin/Invokana PI 2016.
76 SGLT2 Inhibitors Safety: Warnings and Precautions SGLT2 inhibitor use may be associated with hypotension, ketoacidosis, impaired renal function, hypoglycemia, and increased LDL-C Patients should be closely monitored, particularly those with a history of, or at risk for, these conditions Dapagliflozin should not be used in patients with a history of bladder cancer Canagliflozin may be associated with hyperkalemia and bone fracture Bone fracture risk should be considered before use, and potassium levels should be monitored during use LDL-C = low-density lipoprotein cholesterol; SGLT2 = sodium-glucose cotransporter-2 Empagliflozin/Jardiance PI 2016.; Dapagliflozin/Farxiga PI 2016.; Canagliflozin/Invokana PI 2016.
77 Clear Findings from EMPA-REG EMPA-REG studied a high-risk group of people - Mean age 63 years - Type 2 diabetes X 10 years; mean A1C 8.1% - Proven CV disease with prior heart failure in 10% - egfr between ml/min in 20% - Cardioprotective Rx (statins 77%, ACEi 81%, ASA 83%) - MACE event rate ~ 4%/year, CV death rate ~ 1.8%/year In 7,020 such people, empagliflozin (10 or 25 mg/day) - Clearly reduces CV death and heart failure hospitalization - Starts to reduce these outcomes within 3 months There is no clear MI or stroke effect over 3 years of treatment - The composite outcome may not be relevant - The effect on its 3 components appears heterogeneous ASA = aspirin; ACEi = angiotensin-converting enzyme inhibitors; CV = cardiovascular; efgr = estimated glomerular filtration rate; MACE = Major Adverse Cardiac Events; MI = myocardial infarction. Zinman B et al. N Engl J Med 2015;373: Supplement to: Zinman B et al. N Engl J Med 2015;373:1-66.
 0.08 Death from any cause 32% 0.68 (0.57-0.82) <0.001 CV death 0.62 (0.49-0.77) <0.001 36% Fatal or nonfatal MI 0.87 (0.70-1.09) 0.")
78 EMPA-REG Clinical Outcomes with Empagliflozin EMPA-REG OUTCOME Pooled Analysis (N=7020) Hazard ratio (95% CI) P-value Primary composite endpoint* 0.86 ( ) % Secondary composite endpoint 0.89 ( ) 0.08 Death from any cause 32% 0.68 ( ) <0.001 CV death 0.62 ( ) < % Fatal or nonfatal MI 0.87 ( ) 0.23 Hospitalization for HF 35% 0.65 ( ) Hospitalization for HF or CV death 34% 0.66 ( ) <0.001 *CV death, nonfatal MI (excluding silent MI), or nonfatal stroke; CV death, nonfatal MI (excluding silent MI), nonfatal stroke, and hospitalization for unstable angina. CI = confidence interval; CV = cardiovascular; HF = heart failure; HR = hazard ratio; MI = myocardial infarction. Zinman B, et al. N Engl J Med. 2015;373: Favors empagliflozin
79 EMPA-REG Outcome: Therapeutic Considerations Empagliflozin, as used in this trial, for 3 years in 1,000 patients with type 2 diabetes at high cardiovascular risk: 25 lives saved (82 vs 57 deaths) 22 fewer cardiovascular deaths (59 vs 37) 14 fewer hospitalizations for heart failure (42 vs 28) 53 additional genital infections (22 vs 75) Zinman B et al. N Engl J Med 2015;373: Fitchett D. Asian Cardio Diabetes Forum
80 EMPA-REG: Renal Function Over Time Wanner C et al. N Engl J Med DOI: /NEJMoa
81 Synthetic Human Amylin Analog Pramlintide Mechanism Amylin mimetic: PPG, suppresses glucagon secretion, slows gastric emptying, promotes satiety Similar mechanism of action to exenetide, these 2 may be interchangeable for use, particularly with T1DM Efficacy Modest ( A1C 0.5%) Advantages Disadvantages Contraindications No dosage adjustment required in renal impairment Nausea, headaches, anorexia, vomiting, abdominal pain, fatigue, dizziness, severe hypoglycemia risk with insulin; Only approved in combination with prandial insulin but cannot be combined in the same syringe Confirmed diagnosis of gastroparesis, hypoglycemia unawareness A1C = glycated hemoglobin; PPG = postprandial plasma glucose. Pramlintide [package insert]. San Diego, CA; Amylin Pharmaceuticals, Inc; Renukuntla VS et al. J Diabetes Sci Technol. 2014;8(5):
82 Inhalable Insulin In June 2014, the FDA approved the first rapid-active, insulin human inhalation powder for glycemic control in adults with diabetes 1 Inhalable insulin is rapid-acting and should be administered at the start of each meal 2 In patients with T1DM, inhalable insulin should be used in combination with long-acting insulin 2 A black box warning cautions against use in patients with chronic lung disease, such as asthma or COPD 2 Use of inhalable insulin can cause acute bronchospasm in these patients 1. U.S. Food and Drug Administraion. News Release Afrezza Prescribing Information. MannKind. 2014
83 Insulin Human Insulin Inhalable Powder Mechanism Inhibits sodium-glucose transport protein subtype 2 (SGLT2) which is responsible for at least 90% of glucose reabsorption in the kidney causing blood glucose is eliminated in the urine Efficacy Modest ( A1C %) Advantages Disadvantages Contraindications Insulin-independent glucose reduction, Low risk of hypoglycemia, Weight loss (to 4% BW), Blood pressure-lowering Osmotic diuresis causing Polyuria and lightheadedness, Bacterial urinary tract infections ( 5%), Fungal genital infections ( 10%), Increased LDL cholesterol, Hyperkalemia (canagliflozin), Bladder cancer concerns (dapagliflozin) History of genital fungal infections, caution in chronic kidney disease Invokana [Package Insert] Janssen Pharmaceuticals, Inc. Titusville, NJ.; Lavalle-gonzález FJ, Januszewicz A, Davidson J, et al. Diabetologia. 2013; Stenlöf K, Cefalu WT, Kim KA, et al. Diabetes Obes Metab. 2013;15(4):372-82; Burki TK. Lancet. 2012;379(9815):507.
84 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific concerns, adverse drug reactions, and contraindications Discuss the role and timing of combination therapy in achieving A1C goals Explain the implications of recent, large randomized clinical trials on clinical decision-making
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Treatment of Type 2 Diabetes: What Have We Learned? AACE Diabetes Algorithm. ADOPT Trial 6/13/2012
 Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Update on Oral Agents for T2DM and Obesity
 Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Update on Oral Agents for T2DM and Obesity
 AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
 Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Exploring Non-Insulin Therapies in Type 1 Diabetes. Objectives. Pre-Assessment Question #1. Disclosures
 Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
2/9/2016. The Evolving Armamentarium for Type 2 Diabetes: Incorporating New Classes in the Treatment of Our Patients. Objectives: Pharmacists
 WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
Pharmacologic Agents for Treatment of Type 2 Diabetes
 Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes