Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
|
|
|
- Roy Bailey
- 5 years ago
- Views:
Transcription
1 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select therapeutic modalities available to practitioners to improve CV risk factors Recognize the implications of recent large trials on clinical decisions guiding choice and targets for blood pressure and lipid abnormalities Discuss other co-morbid/microvascular conditions seen in patients with type 2 diabetes Explain the role of pharmacologic intervention in the treatment of type 2 diabetes ACEi = angiotensin converting enzyme inhibitor; ARB = angiotensin II receptor blocker; CV = cardiovascular; CVD = cardiovascular disease
 6 4 2 20 19 6 3* 9 11 38 30 0 CHD Stroke Intermittent claudication Diabetes is a Vascular Disease Cardiac failure Total CVD Adapted from Wilson PWF, Kannel WB.")
2 Vascular Disease Events in Patients with Diabetes (Age 35-64): Framingham Heart Study, 30-year Follow-up Risk Ratio 10 8 Men Women Age-adjusted annual rate/1, (Relative to subjects without diabetes P<0.001 *P<0.05) * CHD Stroke Intermittent claudication Diabetes is a Vascular Disease Cardiac failure Total CVD Adapted from Wilson PWF, Kannel WB. In: Hyperglycemia, Diabetes and Vascular Disease. In Ruderman N et al, eds. Oxford; 1992.
3 Abdominal Obesity and Increased Risk of Cardiovascular Events: HOPE Study Adjusted Relative Risk 1.4 Waist circumference (in): 1.29 Tertile 1 Tertile 2 Tertile 3 Men < > Women < > Dagenais GR, et al. Am Heart J. Jan 2005;149(1): CVD death MI All-cause deaths *Adjusted for BMI, age, smoking, sex, CVD disease, DM, HDL-cholesterol, total-c BMI = body mass index; CVD = cardiovascular disease; DM = diabetes mellitus; HDL = high-density lipoprotein cholesterol; MI = myocardial infarction
4 NCEP-ATP III 2001 Guidelines: Clinical Identification of the Metabolic Syndrome 3 of the following are needed for diagnosis Risk Factor Abdominal obesity -men -women Triglycerides HDL -men -women Blood pressure Fasting glucose Defining Level Waist circumference >102 cm (>40 in) >88 cm (>35 in) 150 mg/dl <40 mg/dl <50 mg/dl 130/ 85 mmhg 110 mg/dl 100 mg/dl HDL = high density lipoprotein cholesterol; NCEP ATP III = Third Nation Cholesterol Education Program Adult Treatment Panel NCEP- Expert ATP III Report, JAMA. 2001;285(19):
5 Metabolic Syndrome and Risk of Incident Cardiovascular Events and Death: A Systematic Review and Meta-Analysis of Longitudinal Studies 37 eligible studies including 43 cohorts (inception 1971 to 1997; N=172,573), utilizing either the NCEP, WHO, or modified versions Outcome Studies (N) RR 95% CI CV event CHD event CV death CHD death Death CHD = coronary heart disease; CI = confidence interval; CV = cardiovascular; NCEP = National Cholesterol Education Program; RR = relative risk; WHO = World Heath Organization Decreased risk Increased risk Gami AS, et al. J Amer Coll Cardiology. 2007;49(4):
6
7 Benefits of Aggressive LDL-C Lowering in Diabetes (and Residual Risk) Primary Event Rate, % Treatment Control Aggressive Lipid-lowering Better Aggressive Lipid-lowering Worse P Difference in LDL-C, mg/dl TNT Diabetes, CHD * ASCOT-LLA Diabetes, HTN CARDS Diabetes, no CVD HPS All diabetes < Diabetes, no CVD Relative Risk *Atorvastatin 10 vs 80 mg/day Statin vs placebo Shepherd J, et al. Diabetes Care.2006;9: ; Sever PS,et al. Diabetes Care. 2005;28: ; Collins R, et al. Lancet. 2003;361: ; Colhoun HM, et al. Lancet. 2004;364:
8 Collaborative Atorvastatin Diabetes Study (CARDS) Consistent Statin Effects on Primary Endpoint Components n (% randomized) Event Placebo Atorvastatin Risk reduction (95% CI) Primary outcome 127 (9.0) 83 (5.8) 37% (17 52) p = Acute coronary events Coronary revascularization 77 (5.5) 51 (3.6) 36% (9 55) 34 (2.4) 24 (1.7) 31% ( 16 59) Stroke 39 (2.8) 21 (1.5) 48% (11 69) Favors Atorvastatin Hazard ratio Favors Placebo Colhoun HM, et al, for CARDS Investigators. Lancet. 2004;364:
9 PROVE-IT TIMI 22, Primary Endpoint All-cause Death or Major Cardiovascular Events Pravastatin 40mg (26.3%) 16% RRR (P = 0.005) % with event Atorvastatin 80mg (22.4%) Residual Risk Months of follow-up Cannon CP, Braunwald E, McCabe CH, et al. N Engl J Med 2004;350:15

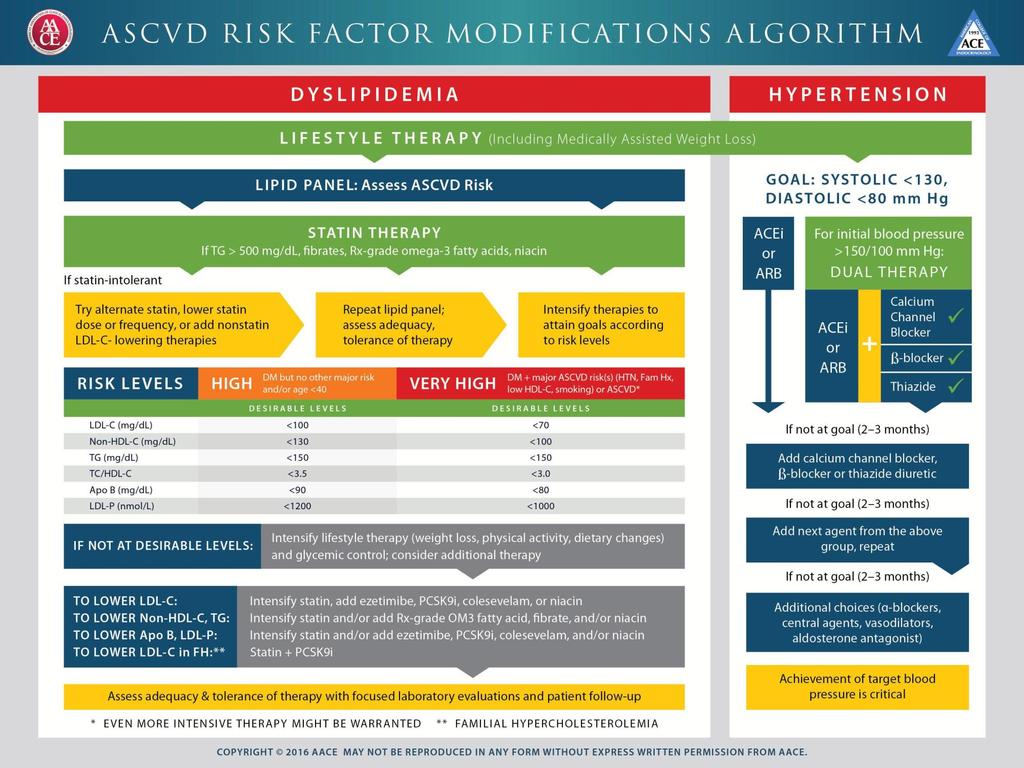
10 AACE 2013 Dyslipidemia Management Algorithm When Atherogenic Markers not at goal: To Lower LDL-C: To Lower Non-HDL-C, TG: Intensify statin and/or, add ezetimibe and/or colesevelam and/or niacin Intensify statin and/or Rx-grade omega-3 ethyl esters and/or fibrates and/or niacin To Lower Apo B, LDL-P: Intensify statin and/or add ezetimibe and/or colesevelam Apo B = apolipoprotein B; HDL-C = high density lipoprotein cholesterol; LDL-C = low density lipoprotein cholesterol; TG = triglyceride Garber AJ, Chair, Task Force, AACE Comprehensive Diabetes Management Algorithm 2013 Consensus Statement, Endocrine Practice. 2013;19(suppl 2):1-48.
11 Proprotein convertase subtilisin-kexitin 9 PCSK9 is widely distributed in Liver, Intestine, kidneys and CNS Regulates plasma LDL-C levels through increased degradation of LDL receptor proteins Overexpression of PCSK9 results in increased circulating levels of LDL-C Single point mutations associated with increased proprotein convertase function may result in familial autosomal dominant hyperlipidemia and increased risk of early MI and stroke New Eng J Med 2011;365:
12 PCSK9 Inhibitors Reduce LDL-C levels Have been shown to reduce Cardiovascular endpoints New Eng J Med 2015;372: New Eng J Med 2015;
13 PCSK9 inhibitors Indications Adjunct to diet and maximally tolerated statin therapy in adults Heterozygous familial hypercholesterolemia Clinical atherosclerotic CV disease who require additional lowering of LDL-C Side effects Injection site reactions Myalgias Neurocognitive (confusion,impaired memory) Dosage :Alirocumab (Praluent ) R Evolucumab (Repatha) R 75 mg/2 weeks or 150 mg / 2 weeks 140 mg /2 weeks or 420mg/month
14 Residual Cardiovascular Risk, Even After Treatment With Statins Despite high-dose statin therapy, there is high residual risk in patients with diabetes, low HDL, elevated triglycerides, and other risk factors Therefore, these other risk factors should be addressed HDL = high density lipoprotein cholesterol Davidson, M, AACE 2011, presentation; Garber AJ, Chair, Task Force, AACE Comprehensive Diabetes Management Algorithm 2013 Consensus Statement, Endocrine Practice. 2013;19(suppl 2):1-48








15 HDL s Complexity: Anti-Atherogenic Actions Reverse Cholesterol Transport Cellular Cholesterol Efflux Anti-infectious Anti-inflammatory Anti-thrombotic HDL-C Apo A-I / II Anti-oxidative Endothelial Repair Anti-apoptotic Vasodilatory Chapman MJ, et al. Curr Med Res Opin. 2004;20: Assmann G, et al. Annu Rev Med. 2003;53:
16 Niacin Despite high-dose statin therapy, there is high residual risk in patients with diabetes, low HDL, elevated triglycerides, and other risk factors Although niacin, or nicotinic acid (vitamin B 3 ) has been shown to increase HDL cholesterol, the results of recent large clinical trials have shown little cardiovascular protection for patients with diabetes Outcomes indicate that while low HDL is associated with poor outcomes, increasing HDL does not appear to be protective for major vascular events. HDL = high density lipoprotein cholesterol Michos ED. J Am Coll Cardiol. 2012;59(23): ; HPS2-THRIVE Collaborative Group. N Engl J Med 2014; 371: Lloyd- Jones D. N Engl J Med 2014; 371:
17 Risk of CHD by Triglyceride Level 3 The Framingham Heart Study 2.5 Relative 2 CHD Risk 1.5 Men N = 5127 Women CHD = coronary heart disease Triglyceride Level, mg/dl Castelli WP. Am J Cardiol. 1992;70:3H-9H.
18 ACCORD-LIPID: Primary Outcomes Possible Benefit Confined to the High Triglycerides/Low HDL-C Subgroup Major fatal or non-fatal CV events (%) Analysis of fenofibrate benefit in pre-specified high TG/low HDL subgroup vs. all others % RRR, adjusted P = Simva Simva + Fen Simva Simva + Feno High triglycerides ( 204 mg/dl) and low HDL ( 34 mg/dl) 17.6% (n=941) of entire cohort ACCORD Study Group, NEJM. 2010; 362: High TG/low HDL-C subgroup had 70% higher event rate No benefit for less than moderate dyslipidemia All others in entire cohort 82.4% (n=4548) of entire cohort CV = cardiovascular; Fen = fenofibrate; HDL-C = high-density lipoprotein cholesterol; Simva = simvastatin; TG = triglyceride


19 Algorithm for Managing Severe Hypertriglyceridemia (SH) Acute management SH +/- pancreatitis Dietary measures: NPO; I.V. fluids; Insulin, if diabetes Chronic management SH Dietary measures: Low carbohydrate, low-fat <20 g LC-FA/day, MCT, abstinence from alcohol If TG not at desirable level Add Rx-grade Omega-3 fatty acids Add fibrates to OM-3 fatty acids Add niacin to fibrates and OM-3 fatty acids Consider medium chain TG If poorly responsive, apheresis (plasmapheresis) until TG <1000 mg/dl When TGs are lowered to <500 mg/dl, secondary targets become non-hdl-c, LDL-C, LDL-P; begin statin therapy Modified from Ewald N, Kloer H-U. Clin Res Cardiol Suppl. 2012;7: HDL-C = high density lipoprotein cholesterol; I.V. = intravenous; LC-FA = long chain fatty acids LDL-C = low density lipoprotein cholesterol; LDL P = low density lipoprotein particles; MCT = medium-chain triglycerides; NPO = nothing by mouth; TG = triglyceride

 Add next agent from the above group, repeat If not at goal (2-3")
 Achievement of target blood pressure is critical Add beta-blocker or")

20 2013 AACE Blood Pressure Management Algorithm Hypertension ACEi or ARB Goal: Systolic ~130 mmhg Diastolic ~80 mmhg For initial blood pressure >150/100 ACEi Or ARB + Thiazide Calcium Channel Blocker Beta-blocker If not at goal (2-3 months) If not at goal (2-3 months) Add next agent from the above group, repeat If not at goal (2-3 months) Additional choices (alpha-blockers, central agents, vasodilators, spironolactone) Achievement of target blood pressure is critical Add beta-blocker or calcium channel blocker or thiazide diuretic Garber AJ, Chair, Task Force, AACE Comprehensive Diabetes Management Algorithm 2013 Consensus Statement, Endocrine Practice. 2013;19(suppl 2):1-48
21 Risk Reduction (%) Effect of Intensive BP Lowering on Risk of Micro- and Macrovascular Complications: UKPDS 0 Myocardial infarction Any diabetesrelated endpoint Diabetesrelated death Retinopathy Renal failure Stroke Vision deterioration Heart failure Benefits of 144/82 mm/hg vs 154/87 mm/hg UKPDS Group. UKPDS 38. BMJ. 1998;317:
22 Guideline Recommendations for Uncomplicated and Complicated Hypertension Type of hypertension BP goal (mmhg) Uncomplicated <140/90 Complicated Diabetes mellitus <130/80 Kidney disease <130/80* Other high risk (stroke, MI) <130/80 *Lower if proteinuria is >1 g/day. Chobanian et al. Hypertension. 2003;42: ; Torre JJ, et al. Endocr Pract. 2006;12: Handelsman Y, et al. Endocr Pract. 2011;17(suppl 2):1-53.; Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):
23 Beta-Blockers in Diabetic Patients: Post-MI 2024-patient study (340 had diabetes [DM] and 281 survived hospitalization for acute MI); of the 127 patients with diabetes taking -blockers, 80% received propranolol and 20% received other -blockers 100 No DM; -blockers 90 Survival (%) DM; -blockers No DM; No -blockers 80 DM; No -blockers Time (days) Kjekshus J et al. Eur Heart J. 1990;11:43-50.
24 Beta-Blocker Recommendations for T2DM Recommend the use of beta-blocker in type 2 diabetes patients with heart failure and/or history of myocardial infarction Beta-blockers may be used safely in patients using blood pressure control Early trials indicated that glucose metabolism may be adversely affected by some beta-blockers; however, newer agents such bisoprolol and carvedilol have not been shown to have this effect Beta-blockers may mask some signs and symptoms of hypoglycemia in patients with longstanding diabetes, particularly patients on insulin Kjekshus J et al. Eur Heart J. 1990;11:43-50; Erdmann E. Eur Heart J Suppl (2009) 11 (suppl A): A21-A25; Wai B, Kearney LG, Hare DL et al. Cardiovascular Diabetology 2012, 11:14
25 Glucose Control and CHD Events Ray KK, et al. Lancet. 2009;373:
 UKPDS T2DM, newly diagnosed (N=4209) 0.12 42% risk reduction P=0.02 1.0 15% risk reduction P=0.01 0.10 0.8 0.08 0.06 0.04 0.02 Randomized treatment Conventional Intensive 0.")
26 CV Outcome Cumulative incidence Proportion With MI Intensive Glycemic Control and Long-term Macrovascular Risk in Younger Patients With Shorter Duration of Disease DCCT T1DM, 5-6 years duration (N=1441) UKPDS T2DM, newly diagnosed (N=4209) % risk reduction P= % risk reduction P= Randomized treatment Conventional Intensive Randomized treatment Conventional Intensive Years No. at Risk Conventional Intensive Years CV, cardiovascular; DCCT, Diabetes Control and Complications Trial; MI, myocardial infarction; UKPDS, United Kingdom Prospective Diabetes Study. Nathan DM, et al. N Engl 26 J Med. 2005;353: Holman RR, et al. N Engl J Med. 2008;359:
27 The Prevalence of U.S. Adults with Diabetes Achieving A1C, Blood Pressure, and LDL-C Goals: : NHANES Percent (%) A1C<7.0% BP<130/80 LDL<100mg/dL All 3 at Goal Still a long way to go A1C = glycated hemoglobin; BP = blood pressure; LDL/LDL-C = low density lipoprotein cholesterol Casagrande SS, Fradkin JE, Saydah SH, Rust KF, Cowie CC. Diabetes Care 2013;36:
28 Treating the ABCs Reduces Diabetic Complications Strategy Complication Reduction of Complication Blood glucose control Myocardial infarction 16% 1 Blood pressure control Lipid control Cardiovascular disease Heart failure Stroke Diabetes-related deaths Coronary heart disease mortality Major coronary heart disease event Any atherosclerotic event Cerebrovascular disease event 51% 2 56% 3 44% 3 32% 3 35% 4 55% 5 37% 5 53% 4 1 UKPDS Study Group (UKPDS 33). Lancet. 1998;352: Grover SA, et al. Circulation. 2000;102: Hansson L, et al. Lancet. 1998;351: Pyŏrälä K, et al. Diabetes Care. 1997;20: UKPDS Study Group (UKPDS 38). BMJ. 1998;317:
29 ADA Recommendations for Aspirin Therapy in Diabetes Aspirin mg/day recommended as Secondary prevention in patients with diabetes and history of CVD Primary prevention for patients with diabetes and 10- year CVD risk >10% Do not use for primary prevention in patients with lower CVD risk because potential adverse effects (eg, bleeding) are likely to offset potential benefits Use clopidogrel 75 mg/day for those with CVD and documented aspirin allergy Combination therapy with aspirin and clopidogrel is reasonable for 1 year after ACS ADA. Diabetes Care.2011;34:S31. 29
30 Summary Major CV risk factors and CVD outcomes Therapeutic modalities available to clinicians to improve CV risk factors Implications of recent large trials on clinical decisions guiding choice and targets for blood pressure and lipid abnormalities Additional co-morbid/microvascular conditions seen in patients with T2DM Role of pharmacologic intervention in the treatment of type 2 diabetes
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes May 20, 2017 AACE Diabetes Day for Primary Care Physicians Jorge Plutzky, MD Director, Preventive Cardiology Cardiovascular Division
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes May 20, 2017 AACE Diabetes Day for Primary Care Physicians Jorge Plutzky, MD Director, Preventive Cardiology Cardiovascular Division
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
( Diabetes mellitus, DM ) ( Hyperlipidemia ) ( Cardiovascular disease, CVD )
 ( Hyperlipidemia ) ( Cardiovascular disease, CVD )") 005 6 69-74 40 mg/dl > 50 mg/dl) (00 mg/dl < 00 mg/dl(.6 mmol/l) 30-40% < 70 mg/dl 40 mg/dl 00 9 mg/dl fibric acid derivative niacin statin fibrate statin niacin ( ) ( Diabetes mellitus,
005 6 69-74 40 mg/dl > 50 mg/dl) (00 mg/dl < 00 mg/dl(.6 mmol/l) 30-40% < 70 mg/dl 40 mg/dl 00 9 mg/dl fibric acid derivative niacin statin fibrate statin niacin ( ) ( Diabetes mellitus,
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Welcome and Introduction
 Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Aggressive Lipid Management for Diabetes
 Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
Aggressive Lipid Management for Diabetes Practical Ways to Achieve Targets in Diabetes Care Keystone, CO July 16, 2011 Robert H. Eckel, M.D. Professor of Medicine Professor of Physiology and Biophysics
Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Macrovascular Management. What s next beyond standard treatment?
 Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
On May 2001, the Third Adult
 THE RISK OF DIABETES: CAN WE IMPACT CHD THROUGH THE ATP III CHOLESTEROL GUIDELINES? * Based on a presentation given by Steven M. Haffner, MD, MPH ABSTRACT Diabetes has been recognized among diabetologists
THE RISK OF DIABETES: CAN WE IMPACT CHD THROUGH THE ATP III CHOLESTEROL GUIDELINES? * Based on a presentation given by Steven M. Haffner, MD, MPH ABSTRACT Diabetes has been recognized among diabetologists
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Welcome! Mark May 14, Sat!
 Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
DYSLIPIDEMIA. Michael Brändle, Stefan Bilz
 DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review.
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Insulin resistance: targeting dyslipidemia beyond the LDL-cholesterol. Disclosures: Presentation outline
 Insulin resistance: targeting dyslipidemia beyond the LDL-cholesterol Rocky Mountain Metabolic Syndrome Symposium May 14 th 21 Mori Krantz MD FACC Associate Professor, University of Colorado Director of
Insulin resistance: targeting dyslipidemia beyond the LDL-cholesterol Rocky Mountain Metabolic Syndrome Symposium May 14 th 21 Mori Krantz MD FACC Associate Professor, University of Colorado Director of
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Management of Cardiovascular Disease in Diabetes
 Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities