CKD: An update on recent developments. Robert Lewis Wessex Kidney Centre
|
|
|
- Raymond Gilmore
- 5 years ago
- Views:
Transcription
1 CKD: An update on recent developments Robert Lewis Wessex Kidney Centre
 and calcitriol T2DM: Type 2 diabetes mellitus")
2 Anatomy and functions of the kidney Calyces Key functions of the kidney Renal artery Renal vein Ureter Cortex Renal pelvis Medulla Waste excretion Acid-base balance Salt/water homeostasis Blood pressure control Glycaemic control Gluconeogenesis Glucose absorption Insulin metabolism & excretion Secretion of hormones including erythropoietin (EPO) and calcitriol T2DM: Type 2 diabetes mellitus The kidneys and how they work. National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC). Available at Last accessed 12/02/2015

3

4 Financial impact of CKD The annual cost of CKD to the NHS in England was estimated at 1.45 billion in Represents 1.3% of all NHS spending that year 1 Equivalent to 1 in every 77 spent 2 There are thought to be around 1 million people in England who have undiagnosed CKD 2 Care for a patient on dialysis costs the NHS around 27,000 a year, while the cost of slowing down kidney deterioration is around 235 a year 3 CKD=chronic kidney disease. 1. NICE (2014) Available at: (accessed ); 2. NHS Choices (2012) Available at (accessed ); 3. Kerr M et al (2012) Nephrol Dial Transplant 27(Suppl 3): iii73 80
5 Targeted screening for CKD: diabetes hypertension acute kidney injury in last 2-3 years cardiovascular disease (ischaemic heart disease, chronic heart failure, peripheral vascular disease or cerebral vascular disease) structural renal tract disease, recurrent renal calculi or prostatic hypertrophy multisystem diseases with potential kidney involvement - for example, systemic lupus erythematosus family history of end-stage kidney disease (GFR category G5) or hereditary kidney disease opportunistic detection of haematuria.
6 NICE 2014: Diagnosis of CKD Two egfr estimations <60 ml/min/1.73 m 2 over a period not less than 90 days OR ACR >3 mg/mmol ACR=albumin:creatinine ratio; CKD=chronic kidney disease; egfr=estimated glomerular filtration rate. NICE (2014) Available at: (accessed )
7
8 GFR categories (ml/min/1.73 m 2 ), description and range Increasing risk Classification of CKD: NICE guidelines 2014 ACR categories (mg/mmol), description and range A1 (<3) Normal to mildly increased A2 (3 30) Moderately increased A3 (>30) Severely increased G1 ( 90) Normal and high G2 (60 89) Mild reduction related to normal range for a young adult G3a (45 59) Mild moderate reduction G3b (30 44) Moderate severe reduction G4 (15 29) Severe reduction G5 (<15) Kidney failure NB: ACR is an important indicator of cardiovascular risk and progression. ACR=albumin:creatinine ratio; CKD=chronic kidney disease; GFR=glomerular filtration rate. NICE (2014) Available at: (accessed ) Increasing risk
9 Percentage of subjects with CKD stage 3-5 (egfr<60mls/mim) by age and gender % 70 Male Female < >85 Age bands de Lusignan et al 2005
10 egfr<60mls/min in people over 75 years old Stage 4-5 Stage 3a Stage 3b J Am Med Dir Assoc Jan;11(1):33-41
11 When CKD category G3a A1 is open to question Poor validation of the egfr formula Very elderly 1 Children 1 Erroneously low egfr (i.e. function looks worse than it is) People with high BMI or muscle bulk 2 Dehydration 2 High protein intake 2 Trimethoprim 1 CKD=chronic kidney disease; egfr=estimated glomerular filtration rate. 1. Nankivell BJ (2001) Aust Prescr 24: 15 7; 2. British Medical Association, NHS Employers (2010) Available at: (accessed )
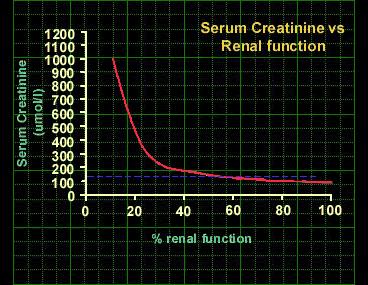
12 MDRD: A mathematical confection egfr* = 186 serum creatinine age (if black) (if female) *ml/min/1.73 m 2 egfr=estimated glomerular filtration rate; MDRD=Modification of Diet in Renal Disease. Levey AS et al (2003) Ann Intern Med 139:
13 Sample: people under the age of 75 with known renal impairment

14 Evidence of poorer outcomes in people over 75years with CKD only evident after egfr<45mls/min In older people, identification and management of CKD should prioritize the smaller numbers with more severe CKD.

15 BTS/Renal Association UK Guidelines for LRD Transplantation Age Acceptable GFR ml/min/1.73m2 <40y 86 50y 77 60y
16 Cardiovascular risk of CKD stratified by age stage 3A stage 3B stage 4 stage Adapted from Raymond et al NDT (2007) 22:
17 Can we improve the accuracy of egfr as a measure of risk? New formula: CKD EPI 1 New assay: cystatin C 2 CKD EPI =Chronic Kidney Disease Epidemiology Collaboration; egfr=estimated glomerular filtration rate. 1. Levey AS et al (2009) Ann Intern Med 150: ; 2. Shlipak MG et al (2013) N Engl J Med 369:
18 Cystatin C may be a useful alternative to creatinine for estimation of GFR when early CKD is suspected. Cystatin C to estimate GFR Creatinine to estimate GFR Produced by all nucleated cells 1,2 Produced by muscle cells 1,2 100% filtered at the glomerulus with no tubular secretion 2 Blood level independent of muscle mass or diet. Therefore unaffected by age, gender or race 2 Blood level is falsely raised in hypothyroidism and lowered in hyperthyroidism 3 100% filtered at the glomerulus with some tubular secretion 2 Blood level dependent on muscle mass. Therefore affected by age, gender and race. Also affected by meat content of diet 2 Unaffected by thyroid activity 3 Assay costs approximately Assay costs approximately CKD=chronic kidney disease; GFR=glomerular filtration rate. 1. Shiplak MG et al (2013) Am J Kidney Dis 62: ; 2. McMahon GM, Waikar SS (2013) Am J Kidney Dis 62: ; 3. Jayagopal V et al (2003) Clin Chem 49: 680 1; 4. NICE (2014) Available at: (accessed )
19 Cystatin C based egfr in the diagnosis of CKD At initial diagnosis to confirm or rule out CKD in people with: An egfr (estimated using serum creatinine) of ml/min/1.73 m 2, sustained for at least 90 days and: No albuminuria (ACR less than 3 mg/mmol) or other marker of kidney disease Do not diagnose CKD in people with: An egfr (estimated using serum creatinine) of ml/m An egfr (estimated using cystatin C) of more than 60 ml/min No other marker of kidney disease ACR=albumin:creatinine ratio; CKD=chronic kidney disease; egfr=estimated glomerular filtration rate. NICE (2014) Available at: (accessed )
20 Dipstick 1 Proteinuria Detects (predominately) albumin Becomes positive when protein >30 mg/dl Affected by urinary concentration/dilution ACR 2 Measures albumin Detects microalbuminuria (ACR between 3 30 mg/mmol) PCR 3 Measures total protein Correlates with 24 hour urinary protein Only correlates with risk above 45 mg/mmol ACR=albumin:creatinine ratio; PCR=protein:creatinine ratio. 1. BMJ Best Practice (2014) Available at: (accessed ); 2. NICE (2014) Available at: (accessed ); 3. National Collaborating Centre for Chronic Conditions (2008) Available at: (accessed )
21 Preferred test: ACR When: Recommended for initial detection of albuminuria and subsequent monitoring ACR >3 mg/mmol is abnormal in men and women How: Preferably early morning urine (not dipstick or 24 hour urine collection) If early morning sample not practical, send spot urine If ACR <3 mg/mmol, no need to obtain early morning sample. If ACR 3-70 mg/mmol, send MSU to exclude infection 2 and repeat ACR using a subsequent early morning sample 1 If the ACR is >70 mg/mmol, a repeat sample needed 1 :unequivocally abnormal and significant 3 samples required for diagnosis of nephropathy (within 3 months) Effect of exercise, hypertension ACR=albumin:creatinine ratio; MSU=mid-stream urine. 1. NICE (2014) Available at: (accessed ); 2. Based on speaker s experience
22 Urine testing: summary Do not use reagent strips to identify proteinuria (but required to detect haematuria). Significant proteinuria is present when ACR >3 mg/mmol in men and women The term microalbuminuria is obsolete EMU only necessary if ACR3-70mg/mmol ACR=albumin:creatinine ratio. NICE (2014) Available at: (accessed )
23 Define accelerated progression of CKD as: a sustained decrease in GFR of 25% or more and a change in GFR category within 12 months or a sustained decrease in GFR of 15 ml/min/1.73 m2 6 per year.
24 NICE 2014: Blood pressure control in CKD No diabetes or proteinuria Diabetes or ACR >70 mg/mmol <140/90 mmhg* <130/80 mmhg * Note: less stringent than QOF indicator of 140/85 mmhg. ACR=albumin:creatinine ratio; CKD=chronic kidney disease; QOF=quality and outcomes framework. NICE (2014) Available at: (accessed )


25 Mode of action of ACE inhibitors and ARBs ACE inhibitors and ARBs Glomerulosclerosis Intraglomerular hypertension RENAL FUNCTION Reduction in number of functioning glomeruli Increased blood flow to remaining nephrons ACE=angiotensin-converting-enzyme; ARB=angiotensin receptor blocker.
26 Subjects (%) Irbesartan diabetic nephropathy trial Irbesartan Amlodipine Control Time to doubling of serum creatinine RRR=37% P<0.001 P=NS RRR=33% P= Follow-up (months) NS=non-significant; RRR=unadjusted relative risk reduction. Lewis EJ et al (2001) N Engl J Med 345:
27 Indications for ACE inhibitors in CKD: Determined by level of proteinuria Diabetes and an ACR >3 mg/mmol Hypertension and an ACR >30 mg/mmol ACR >70 mg/mmol (irrespective of hypertension or cardiovascular disease) Check egfr 7 10 days after starting* <10% fall: safe to continue 10 25% fall: repeat 10 days later >25% fall: stop *Advice based upon speaker s experience and adapted from NICE (2014). ACE=angiotensin-converting-enzyme; ACR=albumin:creatinine ratio; CKD=chronic kidney disease; egfr=estimated glomerular filtration rate. NICE (2014) Available at: (accessed )
28 GFR ACE inhibitors and ARBs: Effect on GFR Slowly deteriorating CKD ACEi/ARB Long-term stabilisation in GFR (most likely in proteinuric patients) Acute reduction egfr expected and OK up to 25% Progressive fall in GFR, caused by renal artery stenosis or other cause of global reduction in renal perfusion Time ACE=angiotensin-converting-enzyme; ACEi=ACE inhibitor; ARB=angiotensin receptor blocker; CKD=chronic kidney disease; egfr=estimated glomerular filtration rate; GFR=glomerular filtration rate. Adapted from: NICE (2014) Available at: (accessed )
29 Care with those at increased risk of pre-renal acute kidney injury Especially if: Elderly ACE inhibitors: Cautions Pre-existing cardiac, renal disease Suspected renal vascular disease (PVD ± IHD, CVA) Check U+E and stop ACE inhibitor when acutely unwell ACE=angiotensin-converting enzyme; CVA=cerebrovascular accident; IHD=ischaemic heart disease; PVD=peripheral vascular disease; U+E=urea + electrolytes.
30 The causes of hypertension may be different in old people Reduced large arterial compliance (ISH) Atheroma Medial calcification Endothelial dysfunction ( NO) High incidence of CKD Decline in Na/K ATPase ( intracellular Ca, vasoconstriction) Reduced sodium excretion High coincidence of secondary HT Renovascular disease NSAIDs
31 Diagnosing hypertension in older people has pitfalls Pseudohypertension prevalence unknown (7-70%?) White coat hypertension More common in the elderly (prevalence 25%?) The risk-predictive value of ambulatory BP compared to office BP increases with age 1 Out-of-office BP monitoring Difference between office/home readings greater in the elderly than middle-aged 2 1. Staessen Brobie 2004
32 Hypertension looks different at different ages 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% < >80 systolic + diastolic isolated systolic isolated diastolic Aronow et al NEJN 2007
33 Old people handle medication differently Pharmacokinetics Lower liver volume and blood flow Body composition T ½ of lipophilic drugs increased Reduced renal clearance Changes in receptors at target organs
34 Older people are more susceptible to side effects of antihypertensive medication Renovascular disease: ACEi and ARBs Impaired tubular function: thiazides Hypokalaemia Hyponatraemia Cardiac conduction defects: β-blockers, CCBs Dysregulation of baroreflex-mediated reflexes (orthostatic hypotension)
35 The elderly are sailing close to the wind Absence of reserve capacity Dehydration falls, AKI Sepsis falls, CCF, AKI NSAIDs AKI, CCF Antihypertensive medication (diuretics, ACE-i) may inhibit corrective responses

36 What defines elderly Biological age? Comorbidities? How can management guidelines be tailored to the individual?
37 NICE: Acute Kidney Injury Flavour of the month
38 NCEPOD 2009 Only 50% of AKI care was rated good by the panel A fifth of post admission AKI was both predictable and avoidable
39 AKI is associated with poor outcomes Adjusted mortality increased 4 fold in hospital and extends beyond discharge Increased hospital length of stay Portsmouth: AKI/CKD v Controls LOS 12 days v 7 days (p=.002) Progression of CKD and increased incidence of ESRD.
40
41 Stage Serum Creatinine rise AKI Stage times baseline or 26.5 µmol/l increase AKI Stage times baseline AKI stage times baseline or Increase to 354 µmol/l or need for dialysis
42
43 Pathogenesis Risk Factors Old age CKD Diabetes Pre-existing cardiac and hepatic failure Vascular disease Chronic diarrhoeal diseases Usual medication ACE/ARB Diuretics NSAIDS Insults Acute sepsis (cytokine storm) Intravascular volume depletion (D&V, diuretics) Toxins Radiocontrast Gentamicin NSAIDS myoglobin
44 Objective Assessment Volume status Physical signs Serum albumin Fluid balance Urine output/fluid intake Weight? JVP Drug review Stop renovasoactive agents
45 Investigation Cause? Pre-renal Renal Post-renal Ultrasound Urine analysis
46 Management Fluid replacement (goal directed) Correction of acidosis Management of hyperkalaemia Dopamine? Furosemide? Referral if unresponsive to medical therapy
47 Learning points: AKI AKI is common and has serious implications for the patient AKI is preventable (forethought) Early management prevents morbidity Alert system in place throughout UK March 2015
The National Quality Standards for Chronic Kidney Disease
 The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care
 Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Summary of Recommendation Statements Kidney International Supplements (2013) 3, 5 14; doi: /kisup
 3, 5 14; doi: /kisup") http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales October 2017 Chronic kidney disease Chronic kidney disease (CKD) is a long-term irreversible deterioration in the function of the kidneys, often
Bulletin Independent prescribing information for NHS Wales October 2017 Chronic kidney disease Chronic kidney disease (CKD) is a long-term irreversible deterioration in the function of the kidneys, often
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
5/10/2014. Observation, control of blood pressure. Observation, control of blood pressure and risk factors.
 Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Overview The Kidneys Nicola Barlow Clinical Biochemistry Department City Hospital Renal physiology Renal pathophysiology Acute kidney injury Chronic kidney disease Assessing renal function GFR Proteinuria
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Managing Patients with CKD in Primary Care: A Shared Care Pathway. 5 th April 2018
 Managing Patients with CKD in Primary Care: A Shared Care Pathway 5 th April 2018 Learning Objectives 1) What health risks does CKD represent? 2) Why change how we manage CKD in NWL? 1) How do we improve
Managing Patients with CKD in Primary Care: A Shared Care Pathway 5 th April 2018 Learning Objectives 1) What health risks does CKD represent? 2) Why change how we manage CKD in NWL? 1) How do we improve
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Online clinical pathway for chronic kidney disease (CKD) in primary care. February 27, 2015 Dr. Kerry McBrien University of Calgary
 in primary care. February 27, 2015 Dr. Kerry McBrien University of Calgary") Online clinical pathway for chronic kidney disease (CKD) in primary care February 27, 2015 Dr. Kerry McBrien University of Calgary FACULTY/PRESENTER DISCLOSURE Faculty: Kerry McBrien Relationships with
Online clinical pathway for chronic kidney disease (CKD) in primary care February 27, 2015 Dr. Kerry McBrien University of Calgary FACULTY/PRESENTER DISCLOSURE Faculty: Kerry McBrien Relationships with
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
NORTHERN IRELAND GUIDELINES FOR MANAGEMENT OF CHRONIC KIDNEY DISEASE
 NORTHERN IRELAND GUIDELINES FOR MANAGEMENT OF CHRONIC KIDNEY DISEASE Practical points for use of estimated GFR + quality outcome framework indicators Developed by GAIN and the Northern Ireland Nephrology
NORTHERN IRELAND GUIDELINES FOR MANAGEMENT OF CHRONIC KIDNEY DISEASE Practical points for use of estimated GFR + quality outcome framework indicators Developed by GAIN and the Northern Ireland Nephrology
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Clinical guideline Published: 23 July 2014 nice.org.uk/guidance/cg182
 Chronic kidney disease in adults: assessment and management Clinical guideline Published: 23 July 2014 nice.org.uk/guidance/cg182 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Chronic kidney disease in adults: assessment and management Clinical guideline Published: 23 July 2014 nice.org.uk/guidance/cg182 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic kidney disease (CKD) (Southampton pathway)
 (Southampton pathway)") Background information Patient information Key messages for this pathway Definitions and abbreviations used in this pathway Classification of CKD Diagnosis of CKD Summary of referral criteria Screening
Background information Patient information Key messages for this pathway Definitions and abbreviations used in this pathway Classification of CKD Diagnosis of CKD Summary of referral criteria Screening
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS WHO SHOULD BE TESTED FOR CKD Offer testing for CKD using egfr, serum creatinine and urinary ACR to people with any of the following risk factors: diabetes hypertension acute
CHRONIC KIDNEY DISEASE DIAGSIS WHO SHOULD BE TESTED FOR CKD Offer testing for CKD using egfr, serum creatinine and urinary ACR to people with any of the following risk factors: diabetes hypertension acute
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM.
 The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The Kidney in Aging The the OF OF changes that occur in kidney with aging is THE MOST DRAMATIC ANY ORGAN SYSTEM. Age related charges in kidney structure and function At age 2 GFR at adult level. Reamins
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Creatinine & egfr A Clinical Perspective. Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC
 Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Supplement: Summary of Recommendation Statements CHAPTER 1: DEFINITION AND CLASSIFICATION OF CKD
 Supplement: Summary of Recommendation Statements CHAPTER 1: DEFINITION AND CLASSIFICATION OF CKD 1.1 DEFINITION OF CKD 1.1.1: CKD is defined as abnormalities of kidney structure or function, present for
Supplement: Summary of Recommendation Statements CHAPTER 1: DEFINITION AND CLASSIFICATION OF CKD 1.1 DEFINITION OF CKD 1.1.1: CKD is defined as abnormalities of kidney structure or function, present for
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine
 Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine Age and Kidney Weight renal weight and thickening of the vascular intima Platt et al. Gerentology 1999;45:243-253
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine Age and Kidney Weight renal weight and thickening of the vascular intima Platt et al. Gerentology 1999;45:243-253
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Chronic kidney disease screening and assessment
 Care map information Information resources for patients and carers Aboriginal and Torres Strait Islanders DEFINITION OF CKD egfr
Care map information Information resources for patients and carers Aboriginal and Torres Strait Islanders DEFINITION OF CKD egfr
Doncaster & Bassetlaw. AKI guidelines for primary care
 Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
A New Approach for Evaluating Renal Function and Predicting Risk. William McClellan, MD, MPH Emory University Atlanta
 A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th Introduction
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
Acute Kidney Injury (AKI) Undergraduate nurse education Year One Developed Summer 2017 Overview Basic A & P of: Urinary system Kidneys Followed by: Introduction to Acute Kidney Injury Urinary System The
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree
 and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree") Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
Nephrology - the study of the kidney. Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system
 Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
E.Ritz Heidelberg (Germany)
") Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease
 Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Hypertension management and renin-angiotensin-aldosterone system blockade in patients with diabetes, nephropathy and/or chronic kidney disease July 2017 Indranil Dasgupta DM FRCP, Debasish Banerjee MD
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation