Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
|
|
|
- Imogene Hicks
- 5 years ago
- Views:
Transcription

1 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
2 Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary care management

3

4 A Journal of the life of Charles Dickens In 1869 wrote a letter to W.H. Willis MD, mentioning difficulties speaking and moving the foot Jan new year s day at Gad s Hill suffering another attack of the foot trouble Jan 23 complains: something the matter with my right thumb and can t write plainly June 8th : writing Edwin Drood and suffers a stroke at Dinner.
5 Transient Ischaemic Attack (TIA) Concept of TIA gathered in 1950 s Neurologists e.g. Miller Fisher observed that stroke often followed transient neurological symptoms of the same arterial territory. Definition evolved: Transient focal neurological symptoms resulting from cerebral, retinal, or spinal ischaemia. Lasts < 24 hours. NOT USEFUL why?
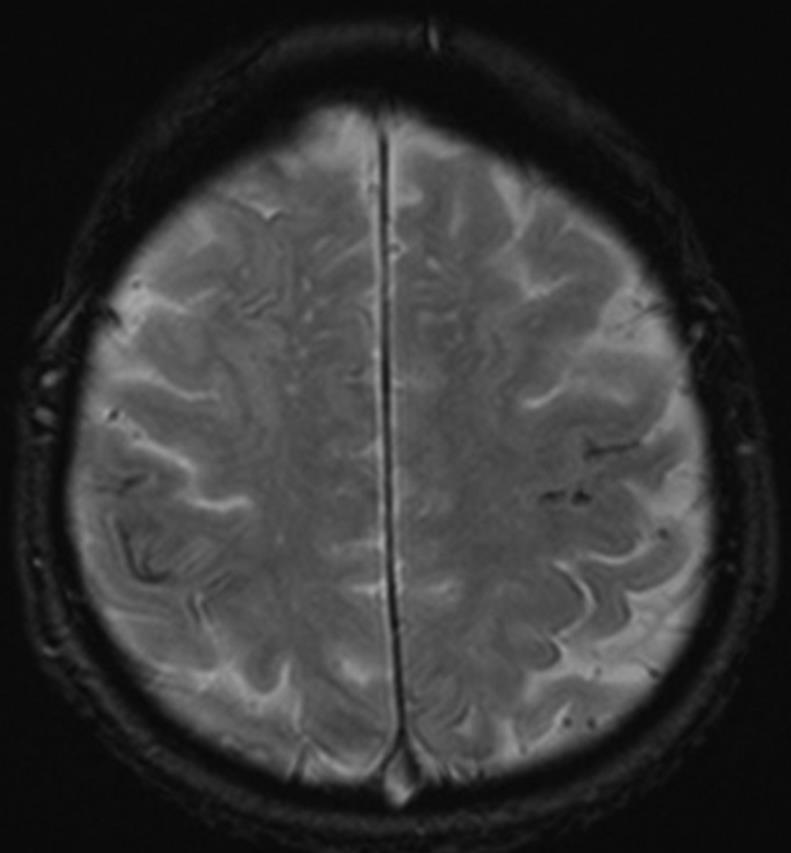
6 New definition TIA Vast majority of TIAs last less 1 hour. Up to 50% of TIAs are associated with infarction on diffusion weighted MRI. Acute ischaemic stroke requires urgent treatment within minutes let alone 24 hours. New tissue based AHA definition: A transient episode of neurological dysfunction caused by focal brain, spinal cord or retinal ischaemia, without acute infarction.
7 TIA Epidemiology 46,000 TIA s annually in the UK. ~ 480 TIA s treated annually in Sheffield. But, ~ 1300 TIA clinic referrals annually in Sheffield. Thus 60% clinic referrals turn out to be alternative diagnosis.
8 Oxfordshire Community Stroke Project Oxfordshire Community Stroke Project 512 Patients referred for suspected TIA 317 Others 195 (38%) with TIA 52 (10%) Migraine 33 (6%) Vertigo 48 (9%) Syncope 29 (6%) Epilepsy 46 (9%) Poss. TIA 17 (3%) TGA 45 (9%) Funny turn 47 (9%) Other OXVASC 2002
9 Diagnosing TIA Difficult symptoms resolved when acquiring history. No definitive test for TIA diagnosis remains clinical. Inter-observer agreement between stroke trained and nontrained poor.
10 Clinical features - History Age & demographics: TIA s are rare in young patients without vascular risk factors. Acute neurology in pregnant females unlikely TIA. Older age more likely TIA less likely mimic.
11 Clinical features - History Nature of symptoms: Positive: excess of neuronal discharge visual (flashing lights, zig-zags, lines, shapes), sensory (pain, paraesthesia), motor (limb jerking) Negative: loss of neuronal function loss of vision, hearing, sensation or power. TIA negative symptoms mostly arterial territory. Seizure & migraine positive symptoms particularly at the outset.
12 Clinical features - History Onset & progression: Abrupt onset of maximal symptoms. If multiple symptoms all generally occur together. Gradual offset over minutes. Migraine occurs over minutes to tens of minutes positive symptoms initially may be replaced by negative ones e.g. spreading paraesthesia followed by numbness; visual aura followed by field defect. Seizures progress over seconds usually one functional domain e.g. motor or sensory can be recurrent and stereotyped.
13 Clinical features - History Duration of symptoms: TIA s nearly always < 1 hr (mostly < 10 mins). Migrainous auras usually mins (can be few hours). Seizures usually < 5 mins. Syncope few seconds (unless remains upright). Episodes recurring over some years unlikely TIA.
14 Unlikely TIA Non-focal symptoms: LOC Dizziness Generalized weakness Mental confusion Loss of vision if associated with reduced LOC Sphincter incontinence

15 Headache and TIA Mild headache 1/6 TIA. Usually ipsilateral to affected carotid territory. More common in posterior TIA. Think about carotid or vertebral dissection. Bilateral headache TIA unlikely
16 Migraine Hemiplegic Migraine. Acephalgic Migraine. Opthalmoplegic Migraine. Basillar Migraine. Prolonged Aura. Status migrainosus. Gradual Onset ( > 5 mins) Positive symptoms. Symptom spread over several seconds to minutes. Gradual resolution - minutes to days. Headache not always. Recurrent Stereotyped attacks. Typically young.
17 Migraine
 OCP Smokers Account for 0.2-0.")
18 Migrainous Infarcts Classical Migraine vascular risk factor Migrainous infarction: Infarct during attack where aura lasts > 60 mins More prevalent in: Young women (<45 years) OCP Smokers Account for % Ischaemic stroke Most commonly posterior circulation
19 Seizure Generalised should be easier to identify but can be brief: Confusion, involuntary movements, incontinence. Negative motor symptoms are very rare as a sole manifestation of seizure. Complete speech arrest Seizure > TIA. Recurrent stereotyped events unlikely TIA.
20 Partial Seizures Common TIA mimic: Young or middle aged adults. Antecedent symptoms. Positive neurological symptoms. March of symptoms. Recurrent stereotypical attacks. +/- amnesia of event.
21 Syncope Transient loss of consciousness & postural tone associated with rapid recovery. Presyncopal symptoms: Faintness Dimming vision Muffling sounds Triggers: - Emotion, fear - Change in posture Pallor, sweating, nausea. TIA extremely unlikely with history of TLOC.
22 Acute vestibular syndrome Dizziness / giddiness what does this mean? True rotational vertigo vs. presyncope vs. unsteadiness Population-based study only 3% of emergency presentations for dizziness have TIA. Dix-Hallpike & Head-impulse tests are specific but not sensitive. In those with vascular risk factors difficult to determine. Kerber et al 2006
23 Posterior circulation TIA Unlikely if isolated: Unsteadiness / vertigo Dysarthria Diplopia Drop-attacks Usually at least 2 of these posterior circ. symptoms present in true ischaemia. Weakness Sensory loss confined to one part of face / limb
24 Other mimics TGA - > 50yrs vascular risk factors temporary loss of laying down new episodic memory procedural memory intact. Ask about features of seizures (lip-smacking, dystonic posturing). Tumours / SOL s stuttering onset over weeks. Functional younger inconsistent history / examination. Amyloid spells / haemorrhagic TIA difficult to differentiate.

25 Amyloid Spell
26 What next? Stroke risk? 20% strokes preceded by TIA % TIA s will stroke within next 5 years. 10% will stroke within next 3 months. 5% will stroke within next 2 days. How do we risk stratify? Rothwell & Warlow 2005, Gladstone et al 2004
27 Stroke risk stratification Clinical ABCD2 Imaging MRI DWI Carotid imaging
28 ABCD 2 score ABCD 2 2 days 7 days 6 8.1% 11.7% % 5.9% % 1.2% Score < 4 TIA clinic within 1 week Score 4 TIA clinic within 24 hrs Specialist review within 24 hrs
29 High risk TIA s AF Known carotid stenosis Crescendo TIA s On anticoagulation
30 Late presentation TIA Presentation > 1 week since symptoms generally treat as low risk.

31 EXPRESS Trial Rapid access TIA clinic (< 2 days) with diagnostics and treatment initiation vs. standard outpatient referral. Before and after study 1,278 patients.

32 Amarosis Fugax Eliasziw et al 2004
33 Emergency treatment Aspirin 300mg stat. Clopidogrel if aspirin intolerant same doses. If already on clopidogrel / prasugrel / ticagrelor continue until seen in TIA clinic. If on dual antiplatelets leave on these. If on warfarin: Therapeutic INR leave until specialist review. INR < mg aspirin.
34 Emergency treatment If on NOAC omit next dose until specialist review. Statin initiation. Don t worry too much about BP immediately await TIA clinic review unless very high (persistently > 200 mmhg SBP) admit.
35 TIA clinics Daily TIA clinic. Stroke specialist / neurologist assessment. Access to CT, MRI, carotid imaging on day of assessment.
36 Neuroimaging in TIA Excludes other causes e.g. SOL MRI and carotid imaging 90 day stroke rates: DWI negative 4.3% DWI positive 11% DWI positive & carotid stenosis 33%

37 Neuroimaging in TIA CT poor sensitivity. 50% TIA s are DWI positive on MRI scan depends on duration of symptoms:
38 Antiplatelets Clopidogrel 300mg and then 75mg daily thereafter. or Aspirin 75mg od and dipyridamole MR 200mg bd.

39 TIA and AF Offer anticoagulant with immediate effect: NOAC Treatment dose LMWH until warfarin therapeutic
40 Carotid Stenosis Symptomatic carotid stenosis of 50-99% - assessed and referred for intervention (CEA or stenting) to be performed within first 2 weeks.

41 Carotid stenosis NASCET & ECST Rothwell et al 2004
42 Secondary prevention BP (target < 130/80) Lipid management (chol < 4, LDL < 2) Diabetes management Smoking cessation / alcohol moderation Exercise management
43 Conclusion Correct diagnosis is key. Urgent investigation and vascular risk reduction required. Thank you any questions?
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Hyperacute Stroke Assessment. Dr Ali Ali Consultant Stroke and Geriatrics Sheffield Teaching Hospitals
 Hyperacute Stroke Assessment Dr Ali Ali Consultant Stroke and Geriatrics Sheffield Teaching Hospitals Objectives Importance of assessment Key aspects of the pathway Know where the problems are Enhancing
Hyperacute Stroke Assessment Dr Ali Ali Consultant Stroke and Geriatrics Sheffield Teaching Hospitals Objectives Importance of assessment Key aspects of the pathway Know where the problems are Enhancing
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
PAPER F National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
Suspected neurological conditions: clinical questions
 Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
Suspected neurological clinical questions For questions on signs and symptoms, the committee wanted to consider any studies that determine whether a certain sign or symptom accompanying a main presenting
MIGRAINE CLASSIFICATION
 MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
MIGRAINE CLASSIFICATION Nada Šternić At most, only 30% of migraineurs have classic aura The same patient may have migraine headache without aura, migraine headache with aura as well as migraine aura without
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Dr Jo-Anne Pon. Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch
 Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Dr Jo-Anne Pon Consultant Ophthalmologist and Oculoplastic Surgeon Southern Eye Specialists Christchurch 12:15-12:30 Visual Migraines to be Worried About Visual Migraines To Be Worried About Jo-Anne Pon
Referral Guideline for Patients with TIA
 DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Medicine Review Course Approach to Transient Amnesia
 Medicine Review Course Approach to Transient Amnesia 9 Sept 2012 Dr See Siew Ju Neurology NNI@SGH A Few Questions.. What did you have for breakfast on Friday? How many red lights did you stop at on your
Medicine Review Course Approach to Transient Amnesia 9 Sept 2012 Dr See Siew Ju Neurology NNI@SGH A Few Questions.. What did you have for breakfast on Friday? How many red lights did you stop at on your
International Pediatric Stroke Study (IPSS) Recovery and Recurrence Questionnaire
 Recovery and Recurrence Questionnaire") PhenX Measure: Functionality after Stroke (#820700) PhenX Protocol: Recovery and Recurrence Questionnaire (RRQ) - Pediatrics (#820702) Date of Interview/Examination (MM/DD/YYYY): International Pediatric
PhenX Measure: Functionality after Stroke (#820700) PhenX Protocol: Recovery and Recurrence Questionnaire (RRQ) - Pediatrics (#820702) Date of Interview/Examination (MM/DD/YYYY): International Pediatric
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Objectives. Amanda Diamond, MD
 Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Amanda Diamond, MD Objectives Recognize symptoms suggestive of seizure and what those clinical symptoms represent Understand classification of epilepsy and why this is important Identify the appropriate
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
Therapy for Acute Stroke. Systems of Care for TIA
 Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Stroke and transient ischaemic attack -
 Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
Pathophysiology. Central Nervous System (CNS) Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal
 Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal") Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Background. Background. Headache Examination. Headache History. Primary vs. Secondary Headaches. Headaches In Children: Why Worry?
 Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
All that blacks out is not syncope: a neurological view of transient loss of consciousness
 All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
Outline. Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call
 Street Medicine Outline Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call Terminology Physiology: The biological study of the functions of living organisms and their parts Pathology: the
Street Medicine Outline Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call Terminology Physiology: The biological study of the functions of living organisms and their parts Pathology: the
Supplementary Online Content
 Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Elements for a public summary
 VI.2 Elements for a public summary Part VI.2 Elements for a public summary is applicable for all products that are covered by this RMP, except from the important potential risk of Medication error with
VI.2 Elements for a public summary Part VI.2 Elements for a public summary is applicable for all products that are covered by this RMP, except from the important potential risk of Medication error with
Critical Review Form Therapy
 Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Fits, Faints and Funny Turns. Dr Aidan Neligan PhD MRCP Consultant Neurologist HUH and NHNN, Queen Square
 Fits, Faints and Funny Turns Dr Aidan Neligan PhD MRCP Consultant Neurologist HUH and NHNN, Queen Square 18-01-2016 Moya et al., 2009 What is referred to a First Seizure Clinic? Prospective study of 200
Fits, Faints and Funny Turns Dr Aidan Neligan PhD MRCP Consultant Neurologist HUH and NHNN, Queen Square 18-01-2016 Moya et al., 2009 What is referred to a First Seizure Clinic? Prospective study of 200
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
P1: OTA/XYZ P2: ABC c01 BLBK231-Ginsberg December 23, :43 Printer Name: Yet to Come. Part 1. The Neurological Approach COPYRIGHTED MATERIAL
 Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Part 1 The Neurological Approach COPYRIGHTED MATERIAL 1 2 Chapter 1 Neurological history-taking The diagnosis and management of diseases of the nervous system have been revolutionized in recent years by
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Epilepsy DOJ Lecture Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis
 Epilepsy DOJ Lecture - 2005 Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis Epilepsy SEIZURE: A temporary dysfunction of the brain resulting from a self-limited abnormal
Epilepsy DOJ Lecture - 2005 Masud Seyal, M.D., Ph.D. Department of Neurology University of California, Davis Epilepsy SEIZURE: A temporary dysfunction of the brain resulting from a self-limited abnormal
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation)
") what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
what is the permanent impact of loss of the vestibular sense? for balance, vision and spatial orientation) loss of speed - poor dynamic vision (daily life) - fear to fall and falls loss of automatisation
THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY?
 THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY? LOS 20th May 2008 Laurence Butler BA(hons); DO(hons); MSc/D.Ost My thanks go to: Barry Jacobs (slides on cervical rotation) Steve
THE CERVICAL SPINE: WHAT GUIDES CURRENT 'BEST PRACTICE' IN OSTEOPATHY? LOS 20th May 2008 Laurence Butler BA(hons); DO(hons); MSc/D.Ost My thanks go to: Barry Jacobs (slides on cervical rotation) Steve
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
Understanding Stroke
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
There are several types of epilepsy. Each of them have different causes, symptoms and treatment.
 1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA)
") NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Epilepsy: diagnosis and treatment. Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM
 Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
Epilepsy (and first seizure) on the acute take. Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff
 on the acute take. Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff") Epilepsy (and first seizure) on the acute take Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff Epilepsy (and first seizure) on the acute take First suspected seizure Acute symptomatic
Epilepsy (and first seizure) on the acute take Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff Epilepsy (and first seizure) on the acute take First suspected seizure Acute symptomatic
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Sheffield guidelines for the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017)
") Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Do Not Cite. Draft for Work Group Review.
 Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
The Psychiatrist s Guide to TIA and Stroke
 The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
Standard NICE (CG ) RCP (2016)
 RCP (2016)") Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Standard NICE (CG68 2008) RCP (2016) Stroke Unit Adults presenting at an A&E department with suspected stroke are admitted to a specialist stroke unit within 4 hours direct admission of patients with acute
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Valutazione iniziale e stratificazione del rischio
 Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Seizures explained. What is a seizure? Triggers for seizures
 Seizures explained What is a seizure? A seizure is a sign of a temporary disruption in the brain s electrical activity. Billions of brain cells pass messages to each other and these affect what we say
Seizures explained What is a seizure? A seizure is a sign of a temporary disruption in the brain s electrical activity. Billions of brain cells pass messages to each other and these affect what we say
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
CHAPTER 6 NERVOUS SYSTEM G00-G99. Presented by Jan Halloran
 CHAPTER 6 NERVOUS SYSTEM G00-G99 Presented by Jan Halloran 1 LEARNING OUTCOMES After studying this chapter you should be able to: Explain the difference between the central and peripheral nervous systems
CHAPTER 6 NERVOUS SYSTEM G00-G99 Presented by Jan Halloran 1 LEARNING OUTCOMES After studying this chapter you should be able to: Explain the difference between the central and peripheral nervous systems
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Pregabalin Aristo Version: RMP-Pregabalin0
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Epilepsy Epilepsy is a long-term condition affecting the brain and is characterised by recurring seizures (or fits). It is one
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Epilepsy Epilepsy is a long-term condition affecting the brain and is characterised by recurring seizures (or fits). It is one