TIA Transient Ischaemic Attack?
|
|
|
- Leona McBride
- 5 years ago
- Views:
Transcription
 Tal Anjum Consultant Stroke Physician, Morriston Hospital")
1 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians)
2 Qs. 1: 75, presented on Sunday with recurrent episodes (x 11) of right hand numbness and slurred speech over 2 weeks. The episodes are very similar in nature, each lasting 10 to 40 minutes with complete resolution. She is asymptomatic now. How would you manage her? 1. Admit, give Aspirin etc, refer for dopplers & urgent specialist review 2. Admit, brain imaging, Aspirin etc, urgent specialist review 3. Give Aspirin etc, discharge with urgent TIA clinic referral 4. Discharge without any antiplatelets, refer to TIA clinic 5. Admit, urgent brain imaging, review again to decide further Rx
3 Transient loss of function (TLOF) 1. Definition (and myths ) 2. Causes of a TLOF 3. Clinical presentation 4. Differential diagnoses/ mimics 5. Investigations 6. Management 7. Summary..
4 1. Definition Sudden onset of focal loss of neurological (cerebral or monocular) function, with symptoms lasting less than 24 hours and which, after adequate investigation, is presumed to be due to embolic or thrombotic vascular disease in an arterial territory WHO 1988
5 1. Definition Myths Myth - any neurological deficit lasting 24 hours or less is a TLOF Most TLOFs recover within 1 to 2 hours Symptoms hardly ever persist more than a few hours. Consider minor stroke / a mimic if they do
6 1. TLOF - Key Features Sudden onset (vs. Gradual onset in SOL/MS) Focal clinical deficits (vs. global deficits e.g. TLOC) Loss of function (vs. Positive symptoms in migraine / seizures) Symptoms related to arterial territory Identifiable (vascular) risk factors
7 1. Transient loss of function (TLOF) a practical definition Sudden onset Focal Neurological/monocular deficit due to an nontraumatic vascular event, Symptoms resolving within 1 to 2 hours
 Hypertension Diabetes Dyslipedemia Smoking Other vascular risk factors Clot migration from a distant source")
8 Picture from 2. Causes of TLOF Local clot formation (atherothrombotic) Hypertension Diabetes Dyslipedemia Smoking Other vascular risk factors Clot migration from a distant source (Embolic) Cardiac AF, Post MI / LV thrombus Endocarditis Large vessel disease Carotid /Vertebral artery Aortic arch disease
9 3. Clinical Features Carotid artery territory Unilateral weakness (face, arm, or leg) Unilateral numbness / paraesthesia Dysphasia Dysarthria Amaurosis fugax
10 3. Clinical Features Vertebro-basilar territory Hemiplegia / hemisensory disturbance Bilateral blindness or hemianopia Bilateral motor or sensory deficit Diplopia Vertigo Vomiting Dysarthria Dysphagia Ataxia
11 3. Clinical Features Physical signs None or trivial neurological signs CVS abnormalities e.g. AF, HTN Evidence of vascular disease (elsewhere)
12 3. Clinical Features What s not a TLOF Non-focal symptoms General weakness/numbness Syncope or incontinence Isolated symptoms e.g. Vertigo (labyrinthine) Slurred speech / dysphagia (neuro-muscular or structural) Double vision (ophthalmic disorders) Acute confusion Disorientation /impaired attention/ consciousness D/D: Isolated receptive dysphasia / visuo-spatial perception problem (? TIA)
13 Qs. 2: 56 brought to GP by wife. After 10k cycling (in summer) he could not remember cycling back or where things were in the house. He was repeating questions despite careful & repeated explanations by wife. Symptoms resolved within ~ 8 hours. Referred to stroke team as suspected TIA. Examination was unremarkable. What s the most likely diagnosis? 1. TIA affecting temporal lobe 2. Transient Global Amnesia 3. Transient Epileptic Amnesia 4. Brain tumor 5. Migrane
14 Migraine Focal seizures 4. Differentials / Mimics Structural brain disorders - SDH, AVM etc Malignant hypertension Hypoglycemia Severe anaemia Paroxysmal symptoms - MS, peripheral nerve lesions, labyrinthine disorders Somatisation
15 Diagnosing TLOF Depends ~ entirely on clinical history Implications of misdiagnosis Patients NHS Un-necessary Rx +/_ potential ADR s Primary condition Untreated Resource implications cost
16 5. Investigations Blood tests FBC, renal function, lipid profile ECG AF, cardiac ischaemia Carotid dopplers for anterior circulation TLOFs & Minor strokes only important to distinguish vascular territory on history
17 Yield in TLOF : 1% 5. Investigations Routine CT brain for TLOF? Use: Mainly to exclude structural lesions (SOL, SDH etc) Intracerebral haemorrhage does not cause TLOF Implications: Cost Radiation to pt
18 5. Neuro-imaging policy in TLOF Punch line People being considered for carotid endarterectomy (CEA) where it is uncertain whether the stroke is in the anterior or posterior No circulation Routine CT heads for TLOFs Unless People with TIA where haemorrhage needs to be excluded, for example long duration symptoms (MR better) or people on anticoagulants 1. Longer duration of symptoms Where alternative diagnosis (for example migraine, epilepsy or tumour) is being considered 2. Patient in AF (anticoagulation) Atypical features, persistent symptoms, headaches etc 3. Atypical symptoms NICE/RCP 2013
19 6. Medical Management Management of vascular risk factors Anti-platelet therapy Statins Anticoagulation (if in AF) Anti-hypertensives (ACEi+Thiazide diuretic) Advice regarding driving (DVLA) 1 month if 1 episode only 3 months if recurrent TIAs
20 6. Carotid Endarterectomy (CEA) Criteria for suitability for CEA Carotid TIA or stroke with good recovery 50-99% internal carotid stenosis ~ 5000 candidates in England & Wales (20 in a DGH) would prevent 500 strokes/year Morriston CEA/year
21 Risk of recurrent stroke during 90 days after TLOF (Express phase , phase ) Rothwell, Giles, Chandrateva, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007; 370:
22 Local services 1 step further Specialist TIA clinic runs on Weekdays only However Referrers (GP/A&E) are asked to initiate preventive treatment (anti-platelets, statins +/- BP Rx) Risk stratify (ABCD2) rapid referral for vascular imaging & TIA clinic
23 Prompt preventive treatment of TIA could reduce the need for a weekend TIA service QT Anjum, L Dacey, M Wani Stroke, Feb 2013;44AP386.pdf Planned service evaluation ( ) Retrospective analysis of TIA service database, clinic letters any recurrent presentation (s) Assess effects of preventive treatment started by referrers Recurrent neurovascular events Complications of early treatment
24 Summary Results Referrers started preventive Rx in 89% patients 12% of these patients had minor ADR s headaches, GI upset, myalgia, rash, bruising none required hospitalisation Recurrent TLOF/Stroke in the early treatment arm (0.7%) vs. Recurrent events in the non-treated group (25%) p <0.0001
25 Qs. 3: 59 - attends A&E on a Saturday after suddenly developing dysarthria, diploplia, numbness & pronounced weakness of right face & left hand which lasted ~2 hours. Past medical history: Hypertension, hyperlipidemia, claudication Current smoker (40 pack year history) She has stopped her medications (few months ago) Exam: BP 150/85, neurological and CV examination normal ECG shows AF what will you do? 1. Start secondary vascular prevention, smoking cessation advice, TIA referral, discharge home 2. CT head, anticoagulate 3. Admit for Rx and Carotid Dopplers 4. Combined option Combined option 2 + 3
26 Summary of Transient Loss of Function Good history identifies a TLOF 10% risk of stroke in the week after TLOF Urgent evaluation & early preventive treatment reduce recurrence after a TLOF by 80% at 90 days
27 Summary of Transient Loss of Function Early anticoagulation if AF Timely OP referral to stroke team Modification of vascular risk factors Hospital admission for TLOF exceptional circumstances ; Crescendo TLOFs (2 or more events in a week) Ongoing focal neurological symptoms TLOF symptoms on anticoagulation
28 Qs. 1: 75, presented on Sunday with recurrent episodes (x 11) of right hand numbness and slurred speech over 2 weeks. The episodes are very similar in nature, each lasting 10 to 40 minutes with complete resolution. She is asymptomatic now. How would you manage her? 1. Admit, give Aspirin etc, refer for dopplers & urgent specialist review 2. Admit, brain imaging, Aspirin etc, urgent specialist review 3. Give Aspirin etc, discharge with urgent TIA clinic referral 4. Discharge without any antiplatelets, refer to TIA clinic 5. Admit, urgent brain imaging, review again to decide further Rx
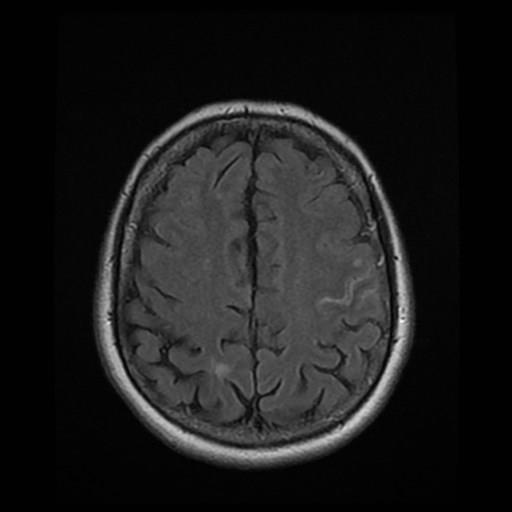

29 Images anonymised, patient consent obtained
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Referral Guideline for Patients with TIA
 DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
DERBYSHIRE COUNTY PCT & NHS DERBY CITY Clinical Effectiveness & Guidelines Group Referral Guideline for Patients with TIA Key Messages This is a revised guideline for patients referred to the TIA service
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Critical Review Form Therapy
 Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Stroke Mimics. Atlantic Canada Stroke Conference. Dr Warren Fieldus FRCP
 Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke Mimics Atlantic Canada Stroke Conference Dr Warren Fieldus FRCP No Conflicts of Interest the plan stroke or no stroke QEII Acute Stroke Protocol things to do before the CT common stroke mimics (25
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke and transient ischaemic attack -
 Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
The Psychiatrist s Guide to TIA and Stroke
 The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
The Psychiatrist s Guide to TIA and Stroke Dr Sam Limaye Consultant Stroke Physician, LTHT Key Learning Outcomes understand recent advances and current practice in the diagnosis, investigation, and management
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Reducing delays to outpatient assessment of strokes and TIAs
 Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Episode 117 TIA Update
 TIA Causes and Common Mimics Episode 117 TIA Update With Walter Himmel & David Dushenski Prepared by Shaun Mehta & Alex Hart, Nov 2018 Much has changed in recent years when it comes to TIA risk stratification,
TIA Causes and Common Mimics Episode 117 TIA Update With Walter Himmel & David Dushenski Prepared by Shaun Mehta & Alex Hart, Nov 2018 Much has changed in recent years when it comes to TIA risk stratification,
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
PAPER F National Collaborating Centre for Chronic Conditions at the Royal College of Physicians
 6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
6.3 Early carotid imaging in acute stroke or TIA Evidence Tables IMAG4: Which patients with suspected stroke/tia should be referred for urgent carotid imaging? Reference Ahmed AS, Foley E, Brannigan AE
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Hyperandrogenism and polycystic ovary syndrome are clear casual factors (trends) which result in hirsuitism and acne.
 which result in hirsuitism and acne.") VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Indication: Treatment of moderate to severe acne related to androgen-sensitivity (with or without seborrhoea) and/or hirsutism,
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Indication: Treatment of moderate to severe acne related to androgen-sensitivity (with or without seborrhoea) and/or hirsutism,
Outline. Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call
 Street Medicine Outline Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call Terminology Physiology: The biological study of the functions of living organisms and their parts Pathology: the
Street Medicine Outline Chest Pain/Heart Attack Stroke Fits + fainting Making a 999 Call Terminology Physiology: The biological study of the functions of living organisms and their parts Pathology: the
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Patient with Daily Headache NTERNATIONAL CLASSIFICATION HEADACHE DISORDERS. R. Allan Purdy, MD, FRCPC,FACP. Professor of Medicine (Neurology)
") Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly
Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Supplementary Online Content
 Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Carotid Artery Dissection Causing an Isolated Hypoglossal. Nerve Palsy
 Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.96550035 Volume 2, Issue 5 Case Report Carotid Artery Dissection Causing an Isolated Hypoglossal Muzzammil Ali*, Yatin Sardana Nerve Palsy
Archives of Clinical and Medical Case Reports doi: 10.26502/acmcr.96550035 Volume 2, Issue 5 Case Report Carotid Artery Dissection Causing an Isolated Hypoglossal Muzzammil Ali*, Yatin Sardana Nerve Palsy
Asthma J45.20 Mild, uncomplicated J45.21 Mild, with (acute) exacerbation J45.22 Mild, with status asthmaticus
 exacerbation J45.22 Mild, with status asthmaticus") A Fib & Flutter I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillation I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter Asthma J45.20 Mild, uncomplicated J45.21 Mild, with
A Fib & Flutter I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillation I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter Asthma J45.20 Mild, uncomplicated J45.21 Mild, with
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA)
") NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
NEW ZEALAND GUIDELINE FOR THE ASSESSMENT AND MANAGEMENT OF PEOPLE WITH RECENT TRANSIENT ISCHAEMIC ATTACK (TIA) Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Rapid Access Clinics for Transient Loss of Consciousness
 Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Vertebrobasilar Insufficiency
 Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
If you have any of these symptoms or see them in someone else, call 911! Treatment can be more effective if given quickly. Every minute counts!
 Sudden numbness or weakness of face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking,
Sudden numbness or weakness of face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking,
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
All that blacks out is not syncope: a neurological view of transient loss of consciousness
 All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
All that blacks out is not syncope: a neurological view of transient loss of consciousness Dr Simon Taggart Consultant Clinical Neurophysiologist. JCUH, Middlesbrough. Misdiagnosis of Blackouts Sutula
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1:
 Clinical Case 1:") ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1: to your office at 2 pm for a feeling of weakness and numbness
ESM 1. Survey questionnaire sent to French GPs. Correct answers are in bold. Part 2: Clinical cases: (Good answer are in bold) Clinical Case 1: to your office at 2 pm for a feeling of weakness and numbness
Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report
 Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report BY JIRI J. VITEK, M.D., JAMES H. HALSEY, JR., M.D., AND HOLT A. McDOWELL, M.D. Abstract: Occlusion of All Four
Occlusion of All Four Extracranial Vessels With Minimal Clinical Symptomatology. Case Report BY JIRI J. VITEK, M.D., JAMES H. HALSEY, JR., M.D., AND HOLT A. McDOWELL, M.D. Abstract: Occlusion of All Four
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Strokes , The Patient Education Institute, Inc. hp Last reviewed: 11/11/2017 1
 Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Using the Neuro Exam to Diagnose Mimics
 Using the Neuro Exam to Diagnose Mimics Jennifer Simpson, MD Neurohospitalist Vascular Neurologist None 2 Review the differential diagnosis for stroke Identify patients physical examination findings that
Using the Neuro Exam to Diagnose Mimics Jennifer Simpson, MD Neurohospitalist Vascular Neurologist None 2 Review the differential diagnosis for stroke Identify patients physical examination findings that
Epilepsy (and first seizure) on the acute take. Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff
 on the acute take. Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff") Epilepsy (and first seizure) on the acute take Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff Epilepsy (and first seizure) on the acute take First suspected seizure Acute symptomatic
Epilepsy (and first seizure) on the acute take Phil Smith Consultant Neurologist University Hospital of Wales, Cardiff Epilepsy (and first seizure) on the acute take First suspected seizure Acute symptomatic
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
Prevention of stroke in primary health care
 Module 3.4 Prevention of stroke in primary health care I ca... sp.. What s inside Introduction Learning objectives Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.4 Prevention of stroke in primary health care I ca... sp.. What s inside Introduction Learning objectives Topics covered Competency Teaching and learning activities Background information Introduction
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.