Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
|
|
|
- Carmel May
- 5 years ago
- Views:
Transcription
1 STROKE Anne Kinnear Lead Pharmacist NHS Lothian
2 Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal working practice.
3 Objectives Describe the disease, identify risk factors and signs and symptoms associated with Stroke. Define the current therapeutic management of acute Stroke and secondary prevention measures. Identify pharmaceutical care issues and respond to symptoms in patient scenarios and identify appropriate management solutions. Explore how to implement the principles of a pharmaceutical care needs assessment tool in practice.
4 Stroke Third commonest cause of death in Scotland 15,000 stroke patients in Scotland annually One of leading causes of disability in adults

5 Time is Brain

6 Stroke 2 million neurones per minute

7 How do you know if someone is having a stroke?

8 What is FAST? F acial weakness - can the person smile? Has their mouth or eye drooped? A rm weakness - can the person raise both arms? S peech problems - can the person speak clearly and understand what you say? T est all 3
9 Stroke WHO Definition A neurological deficit (usually loss of function) caused by reduction in blood supply to the brain. This is usually because a blood vessel bursts or is blocked by a clot. This affects the supply of oxygen and nutrients, causing damage to the brain tissue.
10 Chest Heart and Stroke Definition A stroke is a brain attack. It happens when the blood supply to the brain is disrupted. Most strokes occur when a blood clot blocks the flow of blood to the brain. Some strokes are caused by bleeding in or around the brain from a burst blood vessel.
11 Stroke Transient Ischaemic Attack (TIA) a stroke which resolves within 24 hours (10% risk of stroke within 7 days) Minor Stroke a stroke resulting in persisting symptoms but not causing significant disability Major Stroke a stroke resulting in persistent deficit
")
12 Diagnosis Computed Tomography scan (CT scan) `Immediate`


13 Diagnosis stroke type STROKE Cerebral infarct CT scan Cerebral haemorrhage
14 Stroke
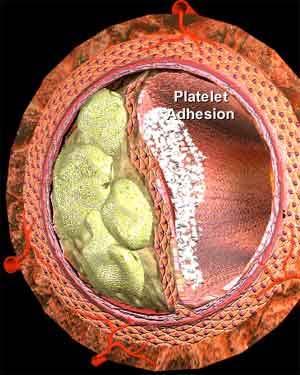
15 Atherosclerotic thrombosis

16 Stroke 1 - Anterior cerebral artery 2 - Anterior communicating artery 3 - Internal carotid artery 4 - Posterior communicating artery 5 - Middle cerebral artery 6 - Posterior cerebral artery 7 - Superior cerebellar artery 8 - Basilar artery 9 - Anterior inferior cerebellar artery
17

18 Cerebrum intellect, speech, emotion, sensory, movement Cerebellum balance, co-ordination Brain stem respiration, heart rate, blood pressure, wakefulness Cerebrum - left hemisphere speech and language
19 Risk factors Risk Factors For Stroke: Treatable Major Diabetes Hypertension Smoking Lifestyle Diet Cholesterol Heart disease, esp. atrial fibrillation Transient ischaemic attacks Less Well Documented Excessive alcohol intake / drug abuse Acute infection
 Family history of stroke")
20 Risk factors Risk Factors for Stroke That Cannot Be Changed Increased age Being male Race (e.g., African- Americans) Family history of stroke

21 Evidence Base for Treatment ACTIVE PROGRESS CHARISMA SPARCL ESPRIT MATCH PROFESS RE-LY
22 Acute Secondary Prevention
23 Acute treatment Thrombolysis Antiplatelets Blood pressure Hydration Oxygen Blood glucose Temperature
24 Thrombolysis Lyses clot by digesting fibrinogen Intravenous recombinant tissue plasminogen activator (tpa - Alteplase) 0.9mg/kg after test dose Within 4.5 hours (6hrs if IST-3 clinical trial) Reduces death and disability at 90 days 2% incidence of symptomatic haemorrhage at 24 hrs 8% incidence of symptomatic haemorrhage at 7 days
25 Antiplatelets Aspirin 300mg within 48 hours continued for 14 days or until discharge from hospital reduces 14 day mortality and morbidity No evidence for: Anticoagulants Combinations of antiplatelets or antiplatelets with anticoagulants Neuroprotectants
26 Blood pressure - not actively managed in acute phase Hydration IV Sodium Chloride 0.9% is preferred to glucose 5% Blood glucose - treat if blood glucose is >11mmol/L Oxygen - supplemental Oxygen if saturation <95% Temperature prescribe antipyretics
27 Secondary Prevention Treatment
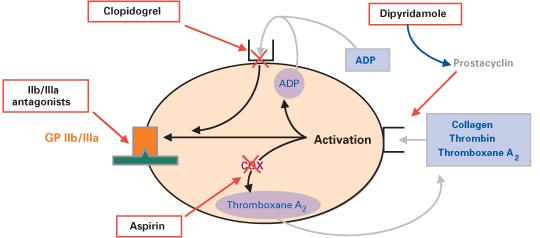
28 Antiplatelets

29 Antiplatelets Evidence Cochrane Reviews Dipyridamole MR Clopidogrel vs Aspirin Randomised Clinical Trials MATCH Aspirin + Clopidogrel vs Clopidogrel CHARISMA Aspirin + Clopidogrel vs Aspirin ESPRIT Aspirin + Dipyridamole MR vs either alone PROFESS Aspirin + Dipyridamole MR vs Clopidogrel
30 Antiplatelets Aspirin and Dipyridamole MR in combination significantly reduces risk of vascular events compared to aspirin alone (approx 25% risk reduction) without an increase in bleeding The combination of Aspirin and Clopidogrel is no more effective than either alone is associated with an increase in moderate/life threatening bleeding only 25% patients in studies had a history of previous stroke used in acute coronary syndrome (NSTEMI) or carotid stenosis
31 Antiplatelets The combination of Aspirin and Dipyridamole MR vs Clopidogrel showed no difference in efficacy
32 Antiplatelets Recommendations Clopidogrel 75mg daily OR Aspirin 75mg daily and Dipyridamole 200mg MR twice daily should be prescribed after ischaemic stroke for secondary prevention of vascular events OR aspirin alone if dipyridamole or clopidogrel intolerance (headache 26% withdrawal ESPRIT trial) - or if carotid stenosis 70% or unstable angina The combination of aspirin and clopidogrel is not recommended for prevention of ischaemic stroke or TIA

33 Statins Evidence 2 x Systematic reviews ( pts) Randomised Clinical Trial SPARCL (4700 pts) Statins significantly reduce relative risk of ischaemic stroke by 21% but stroke death is not reduced Effect occurs without an increase in haemorrhagic stroke Statins reduce coronary events and all cause mortality Effect occurs irrespective of baseline cholesterol level (proportional to LDL lowering)
34 Statins Recommendations A statin should be prescribed to patients who have had an ischaemic stroke irrespective of cholesterol level Which statin? Simvastatin 40mg high risk coronary event Atorvastatin 80mg TIA / ischaemic stroke Should not be used in patients with a prior history of intracerebral haemorrhage

35 Anticoagulants Non-cardioembolic ischaemic stroke Evidence Systematic review Anticoagulant vs antiplatelet Randomised clinical trial ESPRIT Anticoagulants no more effective than aspirin No difference in all cause mortality between antiplatelets and low or medium anticoagulation Higher mortality and major bleeding at intensive anticoagulation Recommendation Anticoagulation not recommended
36 Anticoagulants Atrial fibrillation and ischaemic stroke Evidence ROCKET-AF trial RE-LY trial Warfarin MORE effective for prevention of all vascular events and recurrent stroke No significant increase in intracranial bleed Not within 2 weeks Recommendation Warfarin should be offered with target INR of OR Dabigatran or Rivaroxaban (oral direct thrombin inhibitors) may become alternatives to warfarin
37 Anticoagulants Atrial fibrillation and ischaemic stroke Evidence RE LY trial (NEJM 2009) Warfarin versus Dabigatran in AF with primary outcome of stroke Recommendation Equal efficacy for warfarin and dabigatran with no worse safety profile for the dabigatran

38 Antihypertensives Evidence Well established link between BP reduction and stroke primary prevention Systematic review (7 trials) Randomised Clinical Trial - PROGRESS Perindopril/Indapamide Lowering BP reduced recurrent stroke and major vascular events No effect on vascular or all cause mortality Reduction in stroke related to difference in systolic BP between groups
39 Antihypertensives Recommendation BP should be assessed in all patients and therapy with an ACE inhibitor and thiazide diuretic should be considered regardless of BP Target blood pressure is <140/85 diabetics <130/80 mmhg

40 Summary Secondary Prevention of Ischaemic Stroke Aspirin 75mg + Dipyridamole 200mg twice daily (or Clopidogrel 75mg if ACS) Simvastatin 40mg / Atorvastatin 80mg Thiazide diuretic ACE inhibitor If in atrial fibrillation, warfarin/rivaroxaban/dabigatran should replace antiplatelets
41 Pharmacist Role Public health, education and information Pharmaceutical care Research Multidisciplinary team membership
42 Public Health, education and information Awareness and promotion of: Public Health campaigns CHSS campaigns and resources Risk factors action to take Stroke Identification FAST test Lifestyle advice smoking, weight loss/diet, vitamins
43 Pharmacist Role Public health, education and information Pharmaceutical care Research Multidisciplinary team membership
44 Pharmaceutical Care Transfer of patient information primary/secondary care interface - continuity of care - reduction of medication errors/discrepancies Identification and resolution of pharmaceutical care issues - level and type of resultant disability
45 Modified Rankin Score (mrs) Disability Score Score Symptoms 0 No symptoms 1 No significant disabling symptoms 2 Slight disability 3 Moderate disability 4 Moderate/severe disability 5 Severe disability 6 Dead
46 Disability Dysphasia Aphasia Dysphagia Aphagia Hemiparesis Hemiplegic Hemianopia Speech Swallow Weakness Paralysis Visual difficulties

47 Pharmaceutical Care Issues Speech Comprehension Communication/counselling carers Swallow Ability to take medicines aspiration risk and liquids formulations bioavailability eg phenytoin NG and PEG tube feeding
48 Stroke Weakness or paralysis Ability to operate devices inhalers, insulin Ability to open containers Visual problems Ability to read instructions labels, leaflets, charts
49 Pharmacist Role Public health, education and information Pharmaceutical care Research Multidisciplinary team membership
50 Research Practice development project MSc Strathclyde University Standardised pharmaceutical care plan validation Validation of care issues for transfer needs assessment tool Pharmacist Research Fellow Design and validate transfer document for stroke
51 Research Audit of prescribing adherence to stroke guidelines and design and evaluation of a pharmaceutical care model Prospective evaluation of prescribing in acute stroke unit patients against guidelines and development of a pharmaceutical care plan Retrospective evaluation of prescribing in the same patients following discharge to primary care and design of documentation to facilitate information transfer between secondary and primary care
52 Research Primary Care - Results adherence 75% (hospital 79% 94%) lower for quality indicators not included in GMS contract lower for communication criteria Primary Care - Conclusions Improvement areas for prescribing use of warfarin in atrial fibrillation achievement of clinical target blood pressure and glycaemic control to audit and clinical standards

53 Pharmacist Role Public health, education and information Pharmaceutical care Research Multidisciplinary team membership


54 Multidisciplinary team membership SIGN Scottish Intercollegiate Network Managed Clinical Network for Stroke (MCN) National Advisory Group for Stroke Stroke Unit Multidisciplinary Team
55 Stroke Key Messages Time is brain Think FAST Brain attack dial 999

56 Useful Contacts
CONCISE GUIDE National Clinical Guidelines for Stroke 2nd Edition
 CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
CONCISE GUIDE 2004 National for Stroke 2nd Edition This concise guide summarises the recommendations, graded according to the evidence, from the National 2nd edition. As critical aspects of care are not
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Pharmaceutical care of stroke patients Course information
 Pharmaceutical care of stroke patients Course information Contents of pack Your pack contains: Pharmaceutical care of stroke patients Course information Pharmaceutical care of stroke patients Course activities
Pharmaceutical care of stroke patients Course information Contents of pack Your pack contains: Pharmaceutical care of stroke patients Course information Pharmaceutical care of stroke patients Course activities
Stroke secondary prevention. Gill Cluckie Stroke Nurse Consultant St. George s Hospital
 Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Stroke secondary prevention Gill Cluckie Stroke Nurse Consultant St. George s Hospital Stroke recurrence The risk of recurrent stroke is greatest after first stroke 2 3% of survivors of a first stroke
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Pharmaceutical care of stroke patients Course information
 Pharmaceutical care of stroke patients Course information Contents of pack Your pack contains: Pharmaceutical care of stroke patients Course information Pharmaceutical care of stroke patients Course activities
Pharmaceutical care of stroke patients Course information Contents of pack Your pack contains: Pharmaceutical care of stroke patients Course information Pharmaceutical care of stroke patients Course activities
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Stroke Advice. What is a Stroke. What is a Stroke 1
 Stroke Advice 2 What is a Stroke www.nichs.org.uk What is a Stroke www.nichs.org.uk 1 What is a Stroke? Every two hours someone in Northern Ireland has a stroke, that s about 4,000 strokes a year. A stroke
Stroke Advice 2 What is a Stroke www.nichs.org.uk What is a Stroke www.nichs.org.uk 1 What is a Stroke? Every two hours someone in Northern Ireland has a stroke, that s about 4,000 strokes a year. A stroke
Medicine for Managers. BSc MB BS BDS FDSRCSEng MRCS LRCP DRCOG MHSM FRSM. Stroke Revisited
 nhsmanagers.net Briefing 3 March 2017 Medicine for Managers Dr Paul Lambden BSc MB BS BDS FDSRCSEng MRCS LRCP DRCOG MHSM FRSM Stroke Revisited A stroke is a rapidly developing loss of brain functions which
nhsmanagers.net Briefing 3 March 2017 Medicine for Managers Dr Paul Lambden BSc MB BS BDS FDSRCSEng MRCS LRCP DRCOG MHSM FRSM Stroke Revisited A stroke is a rapidly developing loss of brain functions which
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide
 User Guide") New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
New Zealand Guideline for the Assessment and Management of Transient Ischaemic Attack (TIA) User Guide Acknowledgements The generous voluntary contribution of time and expertise by writers, consumers and
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
This booklet has been published by CREST (the Clinical Resource Efficiency Support Team).
.") This booklet has been published by CREST (the Clinical Resource Efficiency Support Team). CREST is a small committee of health care professionals established under the auspices of the Central Medical Advisory
This booklet has been published by CREST (the Clinical Resource Efficiency Support Team). CREST is a small committee of health care professionals established under the auspices of the Central Medical Advisory
Apixaban for stroke prevention in atrial fibrillation. August 2010
 Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Management of Acute Confusional State in Older People
 Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Management of Acute Confusional State in Older People BACKGROUND Acute confusional state or delirium occurs in 15-20% of all admissions to hospital. It is more likely to occur on a background of pre existing
Strokes , The Patient Education Institute, Inc. hp Last reviewed: 11/11/2017 1
 Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Clinical Guidelines for Stroke Management 2017 Summary Nursing
 Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Dementia is an overall term for a set of symptoms that is caused by disorders affecting the brain.
 Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
Vascular Dementia Vascular Dementia Other Dementias This information sheet provides an overview of a type of dementia known as vascular dementia. In this information sheet you will find: An overview of
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
North Wales Cardiac Network Guidelines on oral antiplatelet therapy in cardiovascular disease
 Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Guideline Stroke and transient ischaemic attack in over 16s: diagnosis and initial management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Stroke and transient ischaemic attack in over s: diagnosis and initial management Draft for consultation, November 0 This guideline covers interventions
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
HEART HEALTH WEEK 2 SUPPLEMENT. A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS. Fatty deposits can narrow and harden the artery
 WEEK 2 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS FIGURE 1 Atherosclerosis is an inflammatory process where cholesterol is deposited in the wall of arteries and
WEEK 2 SUPPLEMENT HEART HEALTH A Beginner s Guide to Cardiovascular Disease ATHEROSCLEROSIS FIGURE 1 Atherosclerosis is an inflammatory process where cholesterol is deposited in the wall of arteries and
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Transient Ischaemic Attack (TIA) Patient Handbook
 Patient Handbook") Transient Ischaemic Attack (TIA) Patient Handbook Contents Introduction 3 About my handbook 3 My details 4 Information about transient 6 ischaemic attack (TIA) What is transient ischaemic attack (TIA)
Transient Ischaemic Attack (TIA) Patient Handbook Contents Introduction 3 About my handbook 3 My details 4 Information about transient 6 ischaemic attack (TIA) What is transient ischaemic attack (TIA)
Variables in Riksstroke - TIA
 Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Variables in Riksstroke - TIA The TIA registration started 2010 for patients treated in hospital and 2015 it was 67 of 72 hospitals are registrating TIA On the www.riksstroke.org/forms/ you find the Riksstroke
Transient ischaemic attack (TIA)
") Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Transient ischaemic attack (TIA) A transient ischaemic attack or TIA is similar to a stroke, but the symptoms do not last as long. However, it should
Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Transient ischaemic attack (TIA) A transient ischaemic attack or TIA is similar to a stroke, but the symptoms do not last as long. However, it should
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
GWTG Post-Discharge Follow-up Form
 Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Stroke and transient ischaemic attack -
 Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
Stroke and transient ischaemic attack Stroke and transient ischaemic attack - cerebrovascular accident unspecified G66) I60-I64, G45 (Clinical term: Stroke and Presenting complaints Usually sudden on-set
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Understanding transient ischaemic attack
 chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
chemistanddruggist.co.uk/update UPDATE Module 1679 PREMIUM CPD CONTENT FOR 1 per week Buy UPDATEPLUS for 52+VAT Visit chemistanddruggist.co.uk/update-plus for full details This module covers: Causes, symptoms
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Prevention of stroke in primary health care
 Module 3.4 Prevention of stroke in primary health care I ca... sp.. What s inside Introduction Learning objectives Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.4 Prevention of stroke in primary health care I ca... sp.. What s inside Introduction Learning objectives Topics covered Competency Teaching and learning activities Background information Introduction
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Coronary artery disease and as anticoagulant (inhibiting the clotting of the blood) in patients undergoing surgery to treat blockages
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Coronary artery disease and as anticoagulant (inhibiting the clotting of the blood) in patients undergoing surgery to treat blockages
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Steps Against Recurrent Stroke (STARS)
") Steps Against Recurrent Stroke (STARS) Take steps against recurrent stroke by making the necessary changes in your life. Your Guide to Ischemic Stroke What happened to me? You had a stroke. The stroke
Steps Against Recurrent Stroke (STARS) Take steps against recurrent stroke by making the necessary changes in your life. Your Guide to Ischemic Stroke What happened to me? You had a stroke. The stroke
NORTH MISSISSIPPI MEDICAL CENTER MEDICAL CENTER. Stroke: Are you at risk? A guide to stroke risk factors & resources at ACUTE STROKE UNIT
 North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
STROKE INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE General practice Indicators for the NICE menu Indicator area: Pulse rhythm assessment for AF Indicator: NM146 Date: June 2017 Introduction There is evidence
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Restart or stop antithrombotics after intracerebral haemorrhage (ICH)?
?") Restart or stop antithrombotics after intracerebral haemorrhage (ICH)? Rustam Al-Shahi Salman professor of clinical neurology & honorary consultant neurologist www.rush.ed.ac.uk @BleedingStroke /bleedingstroke
Restart or stop antithrombotics after intracerebral haemorrhage (ICH)? Rustam Al-Shahi Salman professor of clinical neurology & honorary consultant neurologist www.rush.ed.ac.uk @BleedingStroke /bleedingstroke
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Stroke and TIA. Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne
 Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke and TIA Stephen Davis Melbourne Brain Centre Department of Neurology, Royal Melbourne Hospital University of Melbourne Global burden of stroke 20 million strokes each year 2 nd leading cause of
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Sheffield guidelines for the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017)
") Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
Sheffield guidelines f the use of antiplatelets in the prevention and treatment of cardiovascular disease (October 2017) Approved by Sheffield Area Prescribing Committee and Sheffield Teaching Hospitals
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Medications for Treating Stroke
 Medications for Treating Stroke Subject Expert Sonny Kupniewski, PharmD, BCPS Swedish Medical Center Englewood, CO 2 Objectives Medications used to prevent stroke Prevention of strokes in patients with
Medications for Treating Stroke Subject Expert Sonny Kupniewski, PharmD, BCPS Swedish Medical Center Englewood, CO 2 Objectives Medications used to prevent stroke Prevention of strokes in patients with
WHAT IS A STROKE? What causes a stroke? What disabilities can result from a stroke?
 Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Know Stroke Stroke is the third leading cause of death in the United States and a leading cause of serious, long-term disability in adults. About 600,000 new strokes are reported in the U.S. each year.
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Retrospective Study on the Safety and Efficacy of Clopidogrel in the Treatment of Acute Cerebral Infarction
 International Journal of Neurologic Physical Therapy 2018; 4(1): 24-28 http://www.sciencepublishinggroup.com/j/ijnpt doi: 10.11648/j.ijnpt.20180401.14 ISSN: 2575-176X (Print); ISSN: 2575-1778 (Online)
International Journal of Neurologic Physical Therapy 2018; 4(1): 24-28 http://www.sciencepublishinggroup.com/j/ijnpt doi: 10.11648/j.ijnpt.20180401.14 ISSN: 2575-176X (Print); ISSN: 2575-1778 (Online)
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and