Carotid endarterectomy as complex intraoperative monitoring
|
|
|
- Tamsin Johnston
- 5 years ago
- Views:
Transcription

1 Carotid endarterectomy as complex intraoperative monitoring Dr. Cristina Tudor 1, Dr. Ramona Jemna 1, Dr. Horia Muresian 2, Conf. Dr. Elena Copaciu 1 1 Clinica Anestezie-Terapie Intensiva, Spitalul Universitar de Urgenta Bucuresti 2 Clinica Chirurgie Cardio-Vasculara, Spitalul Universitar de Urgenta Bucuresti


2 History of Carotid Disease Sir William Richard Gowers (British neurologist) First to link stroke with extracranial vascular disease in 1875 The first surgical intervention to relieve atherosclerotic obstruction of the carotid arteries was successfully performed by Dr. Michael DeBakey in 1953 for the first time, at the Methodist Hospital in Houston Dr. Egas Moni, portuguese neurologist and the developer of cerebral angiography (Nobel Prize in 1949)
, accounted for nearly 50% of all deaths.")
3 STROKE In 2010, the first two leading causes of death, heart disease (597,689 deaths) and cancer (574,743), accounted for nearly 50% of all deaths. The fourth as the cause of death was stroke

4

5 Incidence of the Various Causes of Stroke Atheroembolic 44% Subarachnoid hemorrhage 3% Atrial fibrillation 11% STROKE Intracranial hemorrhage 13% Other cardiac emboli 10% Small vessel 21%
6 Evaluation of carotid artery stenosis Carotid doppler ultrasonography Transcranial doppler Computed tomographic angiography Magnetic resonance angiography (MRA) Carotid angiography (the gold standard)
7 Treatment Options Carotid Endarterectomy (CEA) Medical Management Carotid Artery Stenting (CAS)

8 Medical Management Treatment of Hypertension Cessation of Tobacco Smoking Control of Hyperlipidemia Management of Diabetes Mellitus Antithrombotic Therapy
9 Facts 33% of TIA patients will suffer a stroke within 5 years, 17% within 1 year With 75% asymptomatic stenosis, 22% of patients will have an ischemic cerebrovascular event at 2 years CEA reduces the risk of any stroke from 25% to 10% at two years in patients with symptomatic stenosis of 70% (NASCET) CEA reduces the risk of any stroke or death from 11% to 5% at five years in patients with asymptomatic stenosis of 60% (ACAS) Large series of CAS have shown that stenting can be performed with an acceptable complication rate Stenting equivalent to CEA?
10 Studies NASCET North American Symptomatic Carotid Endarterectomy Trial (50 centers in US and Canada) - Stratified patients according to the degree of stenosis NASCET Patients with 70% stenosis had durable benefit at eight years. Veterans Affairs Trial, Asymptomatic Carotid Stenosis Veterans Administration Study - Randomized to optimal medical treatment alone vs. optimal medical treatment plus carotid endarterectomy ACAS, Asymptomatic Carotid Artery Study Prospective randomized trial - medical vs. carotid endarterectomy CAVATAS, Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study - no difference in the major risks of endovascular treatment compared with carotid surgery CARESS, CEA vs. CAS with embolic protection SAPPHIRE, Stenting and Angioplasty with Protection for Patients at High Risk for Endarterectomy (SAPPHIRE) trial SAPPHIRE, no difference in long-term outcome
11 Studies EVA-3S, Endarterectomy vs. Angioplasty in Patients with Symptomatic Severe carotid Stenosis - the excess of primary outcome events after stenting was considered large enough for the safety committee to recommend stopping the trial SPACE, Stent-Supported Percutaneous Angioplasty of the Carotid Artery vs. Endarterectomy (SPACE) collaborative group - failed to prove non-inferiority of CAS vs CEA CREST - Carotid Revascularization Endarterectomy Versus Stenting Trial day stroke/death rate higher with age 80 years 12.1% in patients 80 years 3.2% in patients < 80 years Peri-procedural rate of stroke and death was significantly higher in CAS versus CEA for symptomatic patients (6.0% versus 3.2%) but not for asymptomatic patients (2.5% versus 1.4%) Peri-procedural rate of MI was lower after CAS versus CEA for symptomatic patients (1.0% versus 2.3%) and for asymptomatic patients (1.2% versus 2.2%), however, this was not statistically significant.


12 CREST 2010 Study results???

13 Consensus Guidelines 2011

14 Consensus Guidelines 2011
15 Consensus Guidelines 2011
16 SVS Guidelines 2011




17 Carotid Endarterectomy Surgical removal of the inner layer of the carotid artery when narrowed by atheromatous intimal plaques
18 The perioperative mortality ranges from <0.5 to 3% Cardiac complications (myocardial infarction) Stroke is the second most common cause of mortality Stroke rates range from < 0.25 to 3% Causes of perioperative stroke: embolic, ischemic, hyperemic Nerve injury Vagus nerve, recurrent laryngeal nerve, facial nerve, hypoglossal nerve, glossopharyngeal nerve Bleeding resulting in neck hematoma Infection Complications Restenosis which occurs in up to 20% of patients

19 General Anesthesia versus Regional/Local Anesthesia

20 General Anesthesia versus Regional/Local Anesthesia
21 General Anesthesia Does not prevent hemodynamic response of manipulation of the carotid sinus (severe vagal response) Due to comorbidities (i.e. CAD, MI) it s important to avoid large BP swings especially upon intubation and emergence Maintenance of normocarbia Quick emergence Important to quickly assess neurological function
22 Cervical Plexus Block Deep Cervical Plexus Block Palpate the mastoid process behind the ear Draw a line at the posterior border of the sternocleidomastoid muscle connecting the tip of the mastoid process and the Chassaignac tubercle (i.e. transverse process of C6) 3 separate injections: at 2 cm below mastoid process there is the transverse process of C2; at 2 cm below C2 is C3 and another 2 cm below C3 is C4 22 G needle x3 advanced perpendicular to the skin and slightly caudal until contacting the transverse process (depth about 1.5 to 3 cm) Inject 3 to 4 ml of solution Complications Intravascular injection (Vertebral artery, Carotid artery, Internal jugular, External jugular) Intrathecal injection (Epidural / Subarachnoid anesthetic) Paralysis of the ipsilateral diaphragm (Partial phrenic nerve block) Laryngeal block causing hoarseness, coughing and dysphagia
23

24 Cervical Plexus Block Superficial Cervical Plexus Block Anesthetize C2 to C4 branches Midpoint of the posterior border of the sternocleidomastoid muscle at the intersection with the internal jugular vein 5ml local anesthetic injected subcutaneously posterior and immediately deep to SCM. Redirect needle superiorly and inferiorly along the border of the SCM and inject 5ml at each site. Aspirate frequently and with each redirection to detect intravascular injection.
25 CBF Cerebral Blood Flow Cell death 10mls/100gms/min Cell membranes become dysfunctional 15-20mls/100gms/min EEG flat 15-20mls/100gms/min Evoked Potentials change 20mls/100gms/min Loss of function (awake patient) 25mls/100gms/min Ischaemia 54mls/100gms/m (average grey > white) Normothermic persons with a normal brain and a normal
26 Cerebral Monitoring Why is it important? Decreased cerebral blood flow determines / predicts the need for carotid shunt that may improve cerebral oxygen delivery During carotid endarterectomy, the ischemic risk is correlated with the dependency between the cerebral circulation, the ipsilateral internal carotid artery, the cerebrovascular reserve of the contralateral cerebral hemisphere, as well as the presence and functioning of Willis polygon Why not shunt everyone? Potential displacement of atheromatous debris, introduction of air embolism or thrombosis of shunt Increases surgical time Presence of shunt makes surgical field less than optimal There are still 2 moments of low cerebral blood flow: placement and removal of the carotid shunt 80-85% of patients tolerate well cross clamping of carotid artery, without requiring carotidian shunt

27


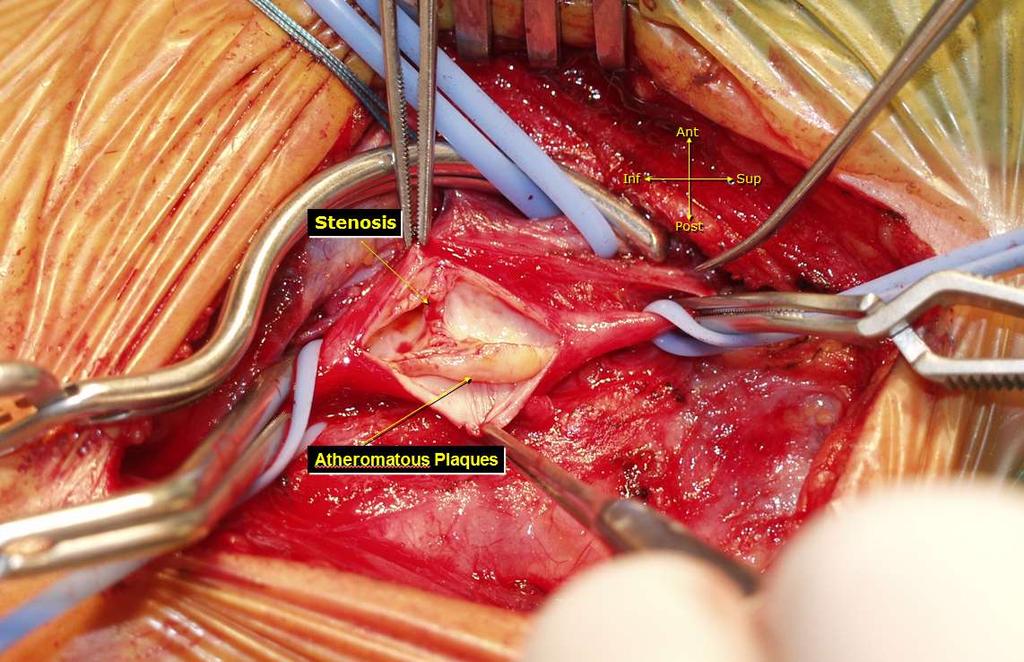
28 Digastric XII ECA ICA CCA OPENING of the CAROTID BIFURCATION NO SHUNT PRE-OCCLUSIVE STENOSIS, DIAPHRAGM-LIKE
29 Cerebral Monitoring Awake patient with locoregional anesthesia Electroencephalography Processed Electroencephalography (Bispectral Index) Somatosensory Evoked Potentials Transcranial Doppler Ultrasound Carotid stump pressure Jugular Oxygen Saturation Conjunctival Oxygen Tension (pcj O2) Cerebral Blood Flow Measurement with ¹³³Xe Near Infrared Spectroscopy Cerebral Oximetry

30 Awake patient - gold standard Assessment of grip strength of the contralateral hand and responsive to verbal commands Disadvantages low degree of patient comfort during surgery sometimes it can convert to general anesthesia Neurological assessment is made early after surgery and throughout the ongoing surgical intervention especially during carotid clamping Indicators of the need for shunt placement or of the shunt malfunction: Agitation, confusion Drowsiness, Seizures, Muscle weakness in the extremities.
31 Electroencephalography Indirect method for determining the cerebral blood flow Limited sensitivity and specificity (respectively 69% and 89% in the study by Evans and respectively 73% and 92% in the study by Stoughton) EEG needs to be interpreted by neurologists, can have delays of 150 before detecting ischemic phenomena - occurrence of cerebral ischemia is indicated by delta waves or disorganised rhythm EEG is influenced by diathermy, general anesthesia agents, PaCO2, hypotension and previous ischemic phenomena Reflects ischemic impairments in the most superficial layer of cerebral cortex Laman et al (2005) clarified which EEG parameters are able to indicate the need for installing shunt for anesthesia with isoflurane, SEF 90% is the best single parameter in order establish whether shunt is necessary or not and the 4 best derivations are F3- Cz, P4-Cz, C4-Cz and F7-Cz. propofol sedation the best single parameter is the relative delta power and its 4 best derivation are F8-Cz, T4-Cz, C4-Cz and F4-Cz.


32 Process EEG BIS, Entropy Bispectral Index / Cerebral Entropy Under general anesthesia, a suddenly modification of these scores after carotid clamping may be suggestive of cerebral ischemia Monitors only frontal lobes supplied by anterior communicating artery and can not estimate blood flow in the middle cerebral artery Is not a specific or sensitive method for detecting cerebral ischemia especially in patients with loco-regional anesthesia
33 Somatosensory Evoked Potentials Sensitivity on 60% and a specificity on 100% Exploring subcortical part of the brain but explores a more limited cortical territory than EEG Intraoperative strokes which occur outside the middle cerebral artery sometimes cannot be detected by SSEP Less reliable on patients with previous neurological deficit The parameter suggested by Haupt et al and subscribed by Rowed which best relates with the neurological outcome after CEA is a reduction of 50% of P25 width.
34 Transcranial Doppler Ultrasound Modality for measuring the ipsilateral mean middle cerebral artery velocity (VMCAi) during carotid endarterectomy Continuous and non-invasive measurement of cerebral blood flow - changes in velocity are proportional to cerebral blood flow changes based on the assumption that the vessel diameter (middle cerebral artery) and blood viscosity remain constant At carotid clamping is a initial decrease of the VCMAi followed by partial recovery in the next 15 seconds, the recovery that occurs due to brain self-regulation. A greater than 40% reduction of VMCAi determine the need for shunt placement.
35 Transcranial Doppler Ultrasound Benefits: Allows the detection of embolic phenomena Allows the detection of haemodynamic phenomena of hypo- or hyperperfusion and micro-embolisation phenomena Identify the occurrence of the postoperative hyperperfusion syndrome with very good use for the immediate postoperative phase Disadvantages Doppler signal is difficult to maintain during surgery At 10% of patients skull conformation prevents transmission of ultrasound

36 Carotid Artery Stump pressure Gives an estimate of collateral circulation above the crossclamp Carotid stump pressure tries to predict need for temporary shunt placement > 50 mmhg adequate collateral circulation < 40 mmhg need for temporary shunt placement PaCO2, body temperature and anesthetic agents influence vascular resistances Method used with caution in patients with preexisting ipsilateral stroke where there is a poor correlation between adequate perfusion pressure and cerebral ischemia

37 Jugular Oxygen Saturation (SjO2) Very low sensitivity and specificity because venous blood may originate from different brain regions
38 Conjunctival Oxygen Tension (pcj O2) Correlation between conjuctival oxygen tension and cortical oxygen tension Is not a specific or sensitive method for detecting cerebral ischemia

39 Cerebral Blood Flow Measurement with ¹³³Xe Three main limitations Difficult to use routinely in the operating room It has discontinuous feature The inability of detecting the areas with low or absent flow because the detect or can only see the perfused tissue areas
40 From Pulse Oximetry to Cerebral Oximetry Oxygen Saturation SO2= Oxy-Hemoglobin / (Total Hemoglobin) X100% Both are based on Beer-Lambert s Law that describes light absorption Pulse Oximetry: Two wavelengths. Using light loss (Systole Diastole) to calculate only signals due to pulsation of arterial blood to derive arterial O2 saturation. Cerebral Oximetry: Looking into entire nonpulsating field to derive tissue O2 saturation. It requires precise light sources and more wavelengths to account for light lost from elements in addition to Oxy- and Deoxy- Hemoglobin. Cerebral oxygen saturation is biased toward venous oxygen saturation because on average, cerebral blood flow is com-posed of 75% venous and 25% arterial blood
41 Transcranial Cerebral Oximetry ARTERIES Pulse Oximetry SpO2 or SaO2: Arterial Oxygen Saturation Normal range: % TISSUE (Arterioles, capillaries, venules) Cerebral Oximetry ro2: Regional Tissue Oxygen Saturation Normal Range: 60-80% VEINS SjvO2: Jugular Venous Oxygen Saturation Normal Range: 50-70%
 from ischemic changes of ro2 during carotid clamping.")

42 Transcranial Cerebral Oximetry Two sensors placed bilaterally on forehead - differentiates changes of non-ischemic source of rso2 (low blood pressure that causes global hypoperfusion) from ischemic changes of ro2 during carotid clamping. Light from light source penetrates the scalp and the skull to reach the gray matter in the brain Closer detector collects reflected light from extracerebral tissue only Further detector collects reflected light from entire path. Patented algorithm solves the hemoglobin concentration while minimizing influence from extracerebral tissue.

43 Transcranial Cerebral Oximetry INVOS measure the regional hemoglobin oxygen saturation of blood in the brain of an individual The sign of low cerebral blood flow is the decrease of rso2 > 20% compared to the baseline value and not the decrease of rso2 from a set value (e.g. rso2 <60) Useful also in postoperative monitoring - decrease of rso2 postoperatively immediately after carotid endarterectomy can demonstrate early carotid artery reocclusion
44

45


46 University Emergency Hospital Bucharest Cardiovascular Department Locoregional Anesthesia - Cervical Plexus Block Monitorizare intraoperatorie clinica + INVOS


47 INVOS monitor with awake patient Carotid endarterectomy incision

48

49
50

51

52
53

54 ATHEROMATOUS PLAQUES AFTER THE EXCISION
55 DATA Total Without shunt With shunt General anesthesia Cervical block plexus Total Percent 89% 11% 28,90% 71,10%
56 Complications (number) DATA Complications (percent) Locoregional anesthesia complications Death % ,05% ,80% ,10% ,80% ,30% % 1 0 Total Percent 3,80% 0,90% 1,04%
57 Carotid Endarterectomy complications: Hemorrhagic Stroke 5 patients Ischemic Stroke 5 patients Transient ischemic attack 1 patient Cardiac complication 3 patients Neck hematoma 4 patients Shunt related injuries 2 patients (carotid disection and embolic stroke) Nerve Injury (hypoglossal nerve) 2 patients Cervical Plexus Block complications: Seizures 3 patients Apnea 1 patient
58 Conclusions Cerebral monitoring system used in carotid endarterectomy must detect early and exact appearance of cerebral ischemia No single monitoring method provides 100% sensitivity and 100% specificity compared with awake patient monitoring Don t forget the baseline Using two types of monitoring decreases the rate of false positives and fals negatives results.

59 An experienced surgeon and an experienced anesthesist
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA
 Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side
 Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Controversies in Carotid Endarterectomy
 Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
The contribution of the external carotid artery to cerebral perfusion in carotid disease
 The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Carotid endarterectomy
 British Journal of Anaesthesia 99 (1): 119 31 (2007) doi:10.1093/bja/aem137 Advance Access publication June 6, 2007 Carotid endarterectomy S. J. Howell* Academic Unit of Anaesthesia, The General Infirmary
British Journal of Anaesthesia 99 (1): 119 31 (2007) doi:10.1093/bja/aem137 Advance Access publication June 6, 2007 Carotid endarterectomy S. J. Howell* Academic Unit of Anaesthesia, The General Infirmary
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY
 GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
Surgical Procedures for. Symptomatic Post-CAS Carotid. Restenosis: Experiences and. Mid-Term Outcomes. Lefeng Qu M.D., Ph.D. Professor of Surgery
 Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng
Surgical Procedures for Symptomatic Post-CAS Carotid Restenosis: Experiences and Mid-Term Outcomes Lefeng Qu M.D., Ph.D. Professor of Surgery Department of Vascular and Endovascular Surgery, Changzheng
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
On behalf of the education Committee of the SNACC
 Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
Neuro Quiz 36 Cerebral Oximetry Shobana Rajan M.D, Assistant Professor Anesthesiology Cleveland Clinic Quiz Team; Suneeta Gollapudy M.D, Angele Marie Theard M.D, Verghese Cherian M.D On behalf of the education
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Measure #344: Rate of Carotid Artery Stenting (CAS) for Asymptomatic Patients, Without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Effective Clinical
Measure #344: Rate of Carotid Artery Stenting (CAS) for Asymptomatic Patients, Without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Effective Clinical
Subclavian and Vertebral Artery Angioplasty - Vertebro-basilar Insufficiency: Clinical Aspects and Diagnosis
 HOSPITAL CHRONICLES 2008, 3(3): 136 140 ORIGINAL ARTICLE Subclavian and Vertebral Artery Angioplasty - Vertebro-basilar Insufficiency: Clinical Aspects and Diagnosis Antonios Polydorou, MD Hemodynamic
HOSPITAL CHRONICLES 2008, 3(3): 136 140 ORIGINAL ARTICLE Subclavian and Vertebral Artery Angioplasty - Vertebro-basilar Insufficiency: Clinical Aspects and Diagnosis Antonios Polydorou, MD Hemodynamic
CAROTID STENTING A 2009 UPDATE. Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital
 CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS
 TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
Oximeters. Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan
 Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Oxygen transport in blood Hemoglobin Oxygen O Deoxygen +O O Oximeters Arterial saturation
Oximeters Hsiao-Lung Chan, Ph.D. Dept Electrical Engineering Chang Gung University, Taiwan chanhl@mail.cgu.edu.tw Oxygen transport in blood Hemoglobin Oxygen O Deoxygen +O O Oximeters Arterial saturation
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Carotid artery disease: stenting vs endarterectomy
 British Journal of Anaesthesia 105 (S1): i34 i49 (2010) doi:10.1093/bja/aeq319 NEUROSCIENCES AND NEUROANAESTHESIA Carotid artery disease: stenting vs endarterectomy K. M. Erickson* and D. J. Cole Mayo
British Journal of Anaesthesia 105 (S1): i34 i49 (2010) doi:10.1093/bja/aeq319 NEUROSCIENCES AND NEUROANAESTHESIA Carotid artery disease: stenting vs endarterectomy K. M. Erickson* and D. J. Cole Mayo
Cerebral hyperperfusion syndrome after carotid angioplasty
 case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
CERVICAL PLEXUS BLOCK FOR CAROTID ENDARTERECTOMY FOLLOWED BY GENERAL ANESTHESIA FOR ABDOMINAL AORTIC SURGERY
 CERVICAL PLEXUS BLOCK FOR CAROTID ENDARTERECTOMY FOLLOWED BY GENERAL ANESTHESIA FOR ABDOMINAL AORTIC SURGERY - A Case Report - ALEXANDRE YAZIGI *, FADIA HADDAD *, SAMIA MADI-JEBARA *, GEMMA HAYECK * AND
CERVICAL PLEXUS BLOCK FOR CAROTID ENDARTERECTOMY FOLLOWED BY GENERAL ANESTHESIA FOR ABDOMINAL AORTIC SURGERY - A Case Report - ALEXANDRE YAZIGI *, FADIA HADDAD *, SAMIA MADI-JEBARA *, GEMMA HAYECK * AND
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
 Case Reports in Vascular Medicine Volume 2013, Article ID 207602, 4 pages http://dx.doi.org/10.1155/2013/207602 Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
Case Reports in Vascular Medicine Volume 2013, Article ID 207602, 4 pages http://dx.doi.org/10.1155/2013/207602 Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
Carotid Endarterectomy: A Concise Review for the Surgical PA
 Carotid Endarterectomy: A Concise Review for the Surgical PA Every year, more than 795,000 Americans experience a stroke, 87% of which are ischemic strokes caused by a blockage of blood flow to the brain.
Carotid Endarterectomy: A Concise Review for the Surgical PA Every year, more than 795,000 Americans experience a stroke, 87% of which are ischemic strokes caused by a blockage of blood flow to the brain.
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Index. average stress 146. see ACIS
 Index ACIS (autonomous catheter insertion system) 156, 237 39, 241 49 acute stroke treatment 59, 69, 71 anatomical model 88 aneurismal clipping treatment 106, 110 aneurysm 2 3, 26, 47 50, 52 55, 67 68,
Index ACIS (autonomous catheter insertion system) 156, 237 39, 241 49 acute stroke treatment 59, 69, 71 anatomical model 88 aneurismal clipping treatment 106, 110 aneurysm 2 3, 26, 47 50, 52 55, 67 68,
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards
 Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
CLINICAL TIMELINE EVA-3S CREST ICSS SPACE SAPPHIRE
 Normal Risk Symptomatic Patients: Ongoing Debate CAS vs CEA John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center University of California, Davis CLINICAL TIMELINE Randomized
Normal Risk Symptomatic Patients: Ongoing Debate CAS vs CEA John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center University of California, Davis CLINICAL TIMELINE Randomized
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography
 Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Carotid Artery Stenting Today: A Few Updating Remarks
 Carotid Artery Stenting Today: A Few Updating Remarks Camilo R. Gomez, MD, MBA Director, Alabama Neurological Institute Birmingham, Alabama Disclaimer & Warning Company Pharmaceutical BMS-Sanofi-Aventis
Carotid Artery Stenting Today: A Few Updating Remarks Camilo R. Gomez, MD, MBA Director, Alabama Neurological Institute Birmingham, Alabama Disclaimer & Warning Company Pharmaceutical BMS-Sanofi-Aventis
Surgical treatment and perioperative management of intracranial aneurysms in Chinese patients with ischemic cerebrovascular diseases: a case series
 Zheng and Wu BMC Neurology (2018) 18:142 https://doi.org/10.1186/s12883-018-1147-8 RESEARCH ARTICLE Open Access Surgical treatment and perioperative management of intracranial aneurysms in Chinese patients
Zheng and Wu BMC Neurology (2018) 18:142 https://doi.org/10.1186/s12883-018-1147-8 RESEARCH ARTICLE Open Access Surgical treatment and perioperative management of intracranial aneurysms in Chinese patients
Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy
 13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
Carotid Ultrasound: Improving Ultrasound
 Carotid Ultrasound: Improving Ultrasound Edward I. Bluth, M.D., F.A.C.R. Chairman Emeritus, Department of Radiology, Ochsner Clinic Foundation, New Orleans, Louisiana Professor, Ochsner Clinical School,
Carotid Ultrasound: Improving Ultrasound Edward I. Bluth, M.D., F.A.C.R. Chairman Emeritus, Department of Radiology, Ochsner Clinic Foundation, New Orleans, Louisiana Professor, Ochsner Clinical School,
Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm.
 Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Glossary of Terms Abdominal Exam: The examination of the abdomen used by physicians to detect an abdominal aortic aneurysm. Angiogram: A diagnostic test requiring the insertion of a catheter into an artery
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Fast-track CEA: a 3-year experience
 Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
History of revascularization
 History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
History of revascularization Author (year) Kredel, 1942 Woringer& Kunlin, 1963 Donaghy& Yasargil, 1968 Loughheed 1971 Kikuchini & Karasawa1973 Karasawa, 1977 Story, 1978 Sundt, 1982 EC/IC bypass study
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Clinical outcomes after carotid endarterectomy: comparison of the use of regional and general anesthetics
 J Neurosurg 92:291 296, 2000 Clinical outcomes after carotid endarterectomy: comparison of the use of regional and general anesthetics ACHILLES K. PAPAVASILIOU, M.D., HULDA B. MAGNADOTTIR, M.D., TAMAS
J Neurosurg 92:291 296, 2000 Clinical outcomes after carotid endarterectomy: comparison of the use of regional and general anesthetics ACHILLES K. PAPAVASILIOU, M.D., HULDA B. MAGNADOTTIR, M.D., TAMAS
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
THE incidence of stroke after noncardiac surgery
 Lack of Association between Carotid Artery Stenosis and Stroke or Myocardial Injury after Noncardiac Surgery in High-risk Patients ABSTRACT Background: Whether carotid artery stenosis predicts stroke after
Lack of Association between Carotid Artery Stenosis and Stroke or Myocardial Injury after Noncardiac Surgery in High-risk Patients ABSTRACT Background: Whether carotid artery stenosis predicts stroke after
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH
 ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
Disclosures. Set up audience participation. Test question. Outline. Neuromonitoring What and When? IP for monitoring technology licensed to Medtronic
 Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Unit #3: Dry Lab A. David A. Morton, Ph.D.
 Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
DESCRIPTION: Percent of asymptomatic patients undergoing CEA who are discharged to home no later than post-operative day #2
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Carotid Stenting and Surgery in 2016 in Russia
 Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia
Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Preoperative assessment of a patient for carotid endarterectomy
 Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers
 The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Approach to the Patient with Carotid Artery Disease
 Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Carotid Artery Disease How the Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient
 Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner