Carotid Ultrasound: Improving Ultrasound
|
|
|
- Andrea Horn
- 6 years ago
- Views:
Transcription



1 Carotid Ultrasound: Improving Ultrasound Edward I. Bluth, M.D., F.A.C.R. Chairman Emeritus, Department of Radiology, Ochsner Clinic Foundation, New Orleans, Louisiana Professor, Ochsner Clinical School, The University of Queensland School of Medicine
2 DUPLEX EVALUATION OF CAROTID ARTERIES 1. Plaque Characterization 2. Evaluation for FlowLimiting Stenosis

3 PATHOLOGIC TYPES OF PLAQUE Fibrous Plaque With Hemorrhage
4 Classification Schemes Type 1 Type 2 Matalanis Echolucent & Lusby Gray-Weale Bluth Kelly Heterogeneous Type 3 Type 4 Echogenic Homogeneous
5 PATHOLOGIC TYPES OF PLAQUE Fibrous Plaque Homogeneous With Hemorrhage Heterogeneous

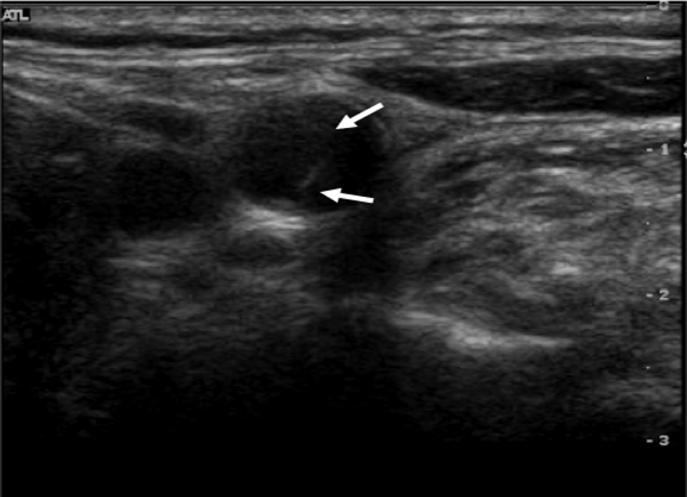
6 Homogeneous Plaque Uniform Low level echoes Smooth surface Corresponds to fibrous collagenous plaque < 50% sonolucent


7 Homogeneous Type 4


8 Homogeneous Type 3


9 Heterogeneous Plaque Focal sonolucent areas > 50% sonolucent Smooth or irregular surfaces


10 Heterogeneous Type 1
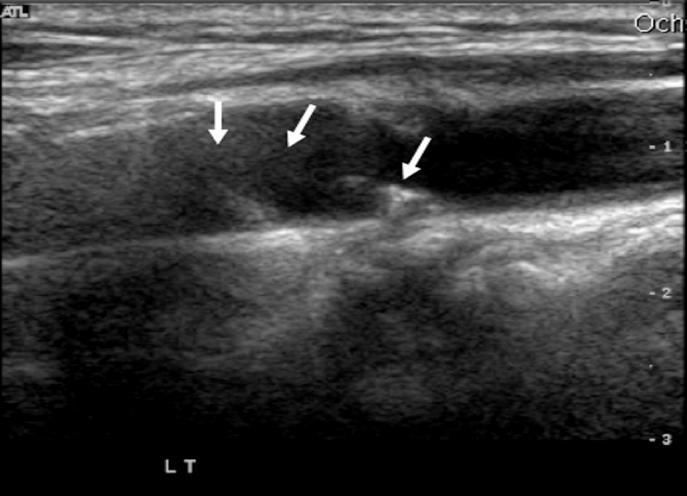
11 Heterogeneous Type 1
12 SIGNIFICANCE OF PLAQUE CLASSIFICATION The incidence of CT infarction increased with degree of echolucency from 10.5% - 66%. Seen in both symptomatic and asymptomatic patients with a stenosis greater than 50%. Nicolaides, JEMU 1996; 17:404
 extending from the adventitia through the media and into thickened intima.")
13 VULNERABLE PLAQUE Nonatherosclerotic Coronary Vessel Elaborate Atherosclerotic Microvascular Network Intraplaque Hemorrhage Studies involving injection of silicone polymer into atherosclerotic human coronary arteries demonstrated on elaborate microvascular network (the vasa vasorum) extending from the adventitia through the media and into thickened intima. Nonatherosclerotic vessels rarely had vasa vasorum. Kolodgie et al, NEJM 2003;349:
14 Origin of Intraplaque Hemorrhage Nonatherosclerotic Coronary Vessel Elaborate Atherosclerotic Microvascular Network Intraplaque Hemorrhage Intraplaque hemorrhage is believed to arise from the disruption of thin-walled microvessels (vasa vasorum) that are lined by discontinuous endothelium without supporting smooth-muscle cells Kolodgie et al, NEJM 2003;349:

15 PATHOLOGIC TYPES OF PLAQUE Fibrous Plaque Homogeneous, Stable With Hemorrhage Heterogeneous, Vulnerable
16 HINTS TO EFFECTIVELY CHARACTERIZE PLAQUE Plaque must be characterized with grayscale only, not with color or power.
17 HINTS TO EFFECTIVELY CHARACTERIZE PLAQUE Plaque must be characterized with grayscale only, not with color or power. Homogeneous plaque is most common (80-85%).
18 HINTS TO EFFECTIVELY CHARACTERIZE PLAQUE Plaque must be characterized with grayscale only, not with color or power. Homogeneous plaque is most common (8085%). Need to evaluate plaque in both transverse and sagittal planes.
19 Transverse view of heterogeneous plaque C' C' Sagittal view of heterogeneous plaque falsely appearing as homogeneous D' D' Sagittal view of heterogeneous plaque
20 Transverse view of homogeneous plaque C D C Sagittal view of heterogeneous plaque D Sagittal view of heterogeneous plaque falsely appearing as homogeneous
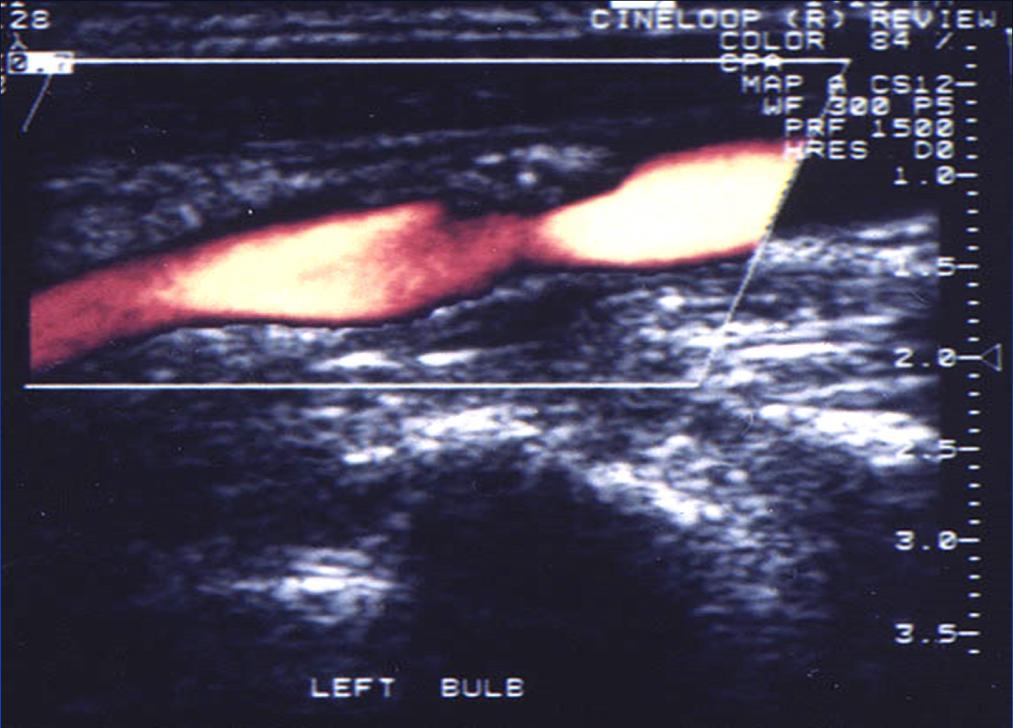
21 DUPLEX EVALUATION OF CAROTID ARTERIES 1. Plaque Characterization 2. Evaluation for FlowLimiting Stenosis
22 Obtain Velocity Measurements ICA CCA


23 Obtain Velocity Measurements ICA CCA
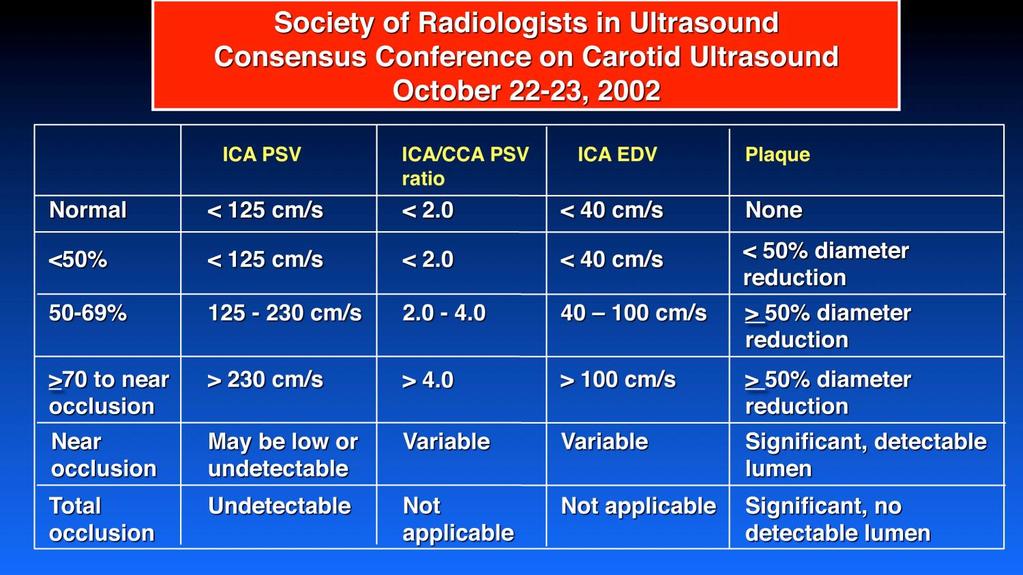
24 LEFT Peak Systole ICA 444 Peak Systole CCA 79 Systolic Ratio 5.62 Plaque Homogeneous Vertebral Forward flow ICA PSV End Diastole ICA End Diastole CCA Diastolic Ratio Normal < 125 cm/s ICA/CCA PSV ICA EDV ratio < 2.0 < 40 cm/s <50% < 125 cm/s < 2.0 < 40 cm/s 50-69% cm/s cm/s >70 to near occlusion Near occlusion Total occlusion > 230 cm/s > 4.0 > 100 cm/s May be low or undetectable Undetectable Variable Variable Not applicable Not applicable Plaque < 50% diameter reduction > 50% diameter reduction > 50% diameter reduction Significant, detectable lumen Significant, no detectable lumen None
25 Velocity Parameters for Carotid Stenosis % Stenosis > 60% > 70% > 80% Peak Systolic End Systolic Diastolic Velocity Diastolic Velocity Ratio Velocity Ratio Reference (cm/sec) Velocity (VICA/VCCA) (VICA/VCCA) Bluth et al > 130 Carpenter et al > 170 Moneta et al > 260 Filinger et al > 200 Jackson et al > 245 Moneta et al > 325 Carpenter et al > 210 Neale et al > 270 Hunink et al > 230 Bluth et al > 250 > 40 > 40 > 70 > 65 > 110 > 100 VICA = peak velocity at point of maximum stenosis in internal carotid artery VICA = peak velocity in unobstructed common carotid artery > 1.8 > 2.0 > 3.5 > 3.3 > 4.0 > 3.0 > 3.7 > 2.4 > 2.4 > 5.5

26 ICA ECA Measurement Methodology ECST = B - A x 100 B NASCAT = 1 - A x 100 C ACAS CCA

27 Criteria Comparison ICA ECA ECST = 66% CCA NASCET = 0% ACAS = 0%
28
29
30
31 Which velocity values are correct?
32
33 COMMON PITFALLS Mistaking ICA for ECA or ECA for ICA Improper plaque characterization Confusion over carotid grading criteria and which table or cut-off value to use Measuring CCA velocities at incorrect location Relying on systolic velocity parameters only Forgetting to integrate all information (internal consistency) In patients with arrhythmias, measuring velocities of compensatory beat
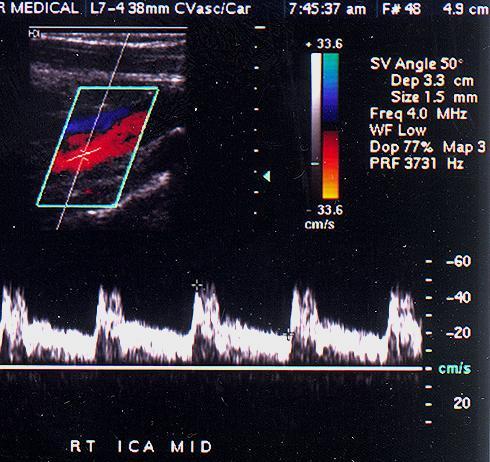
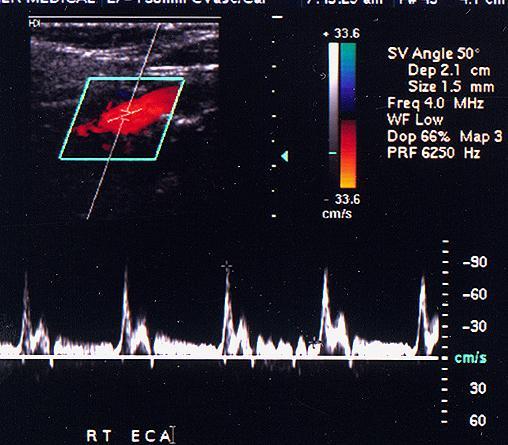
34 Differences in Internal Carotid Artery and External Carotid Artery ICA ECA Size Larger Smaller Location Posterior/lateral Anterior/medial Branches No Yes Waveform Low resistance High resistance Temporal tap No pulsations Pulsations
35
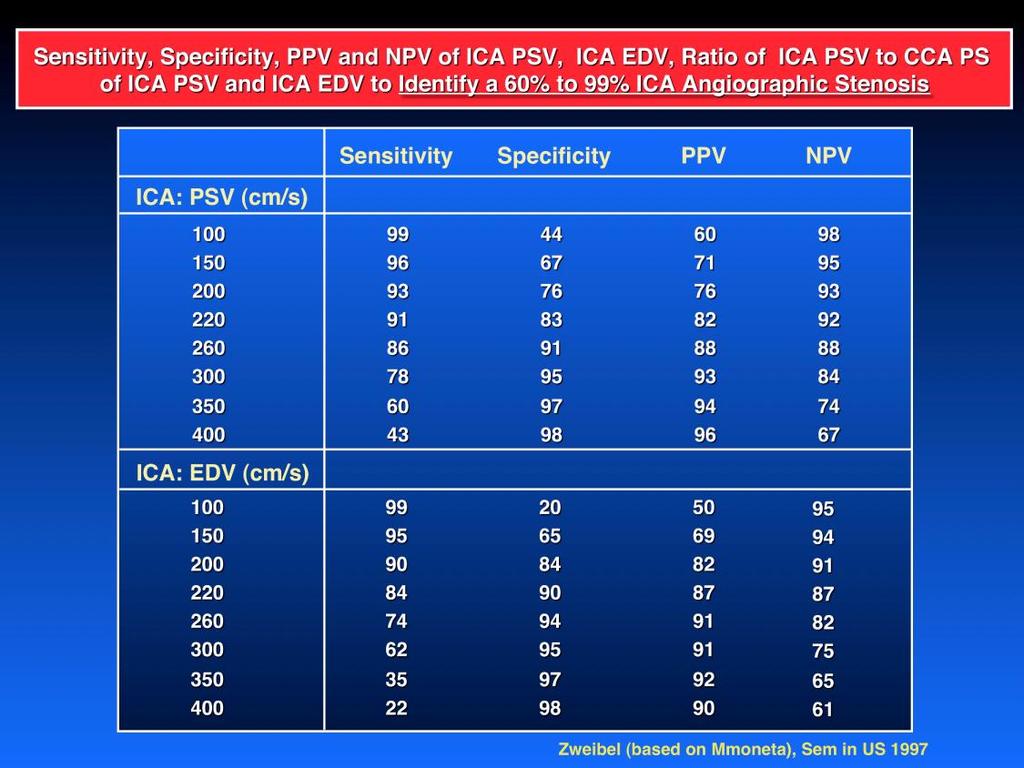
36 COMMON PITFALLS Mistaking ICA for ECA or ECA for ICA Improper plaque characterization Confusion over carotid grading criteria and which table or cut-off value to use Measuring CCA velocities at incorrect location Relying on systolic velocity parameters only Forgetting to integrate all information (internal consistency) In patients with arrhythmias, measuring velocities of compensatory beat Missing high grade stenosis with normal velocity

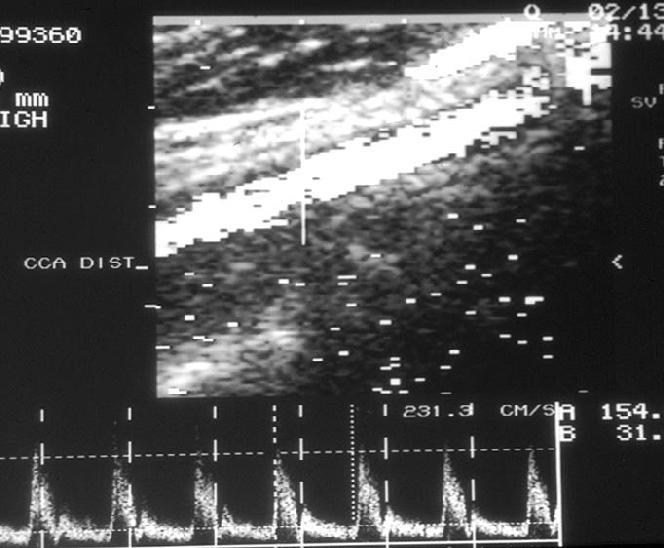
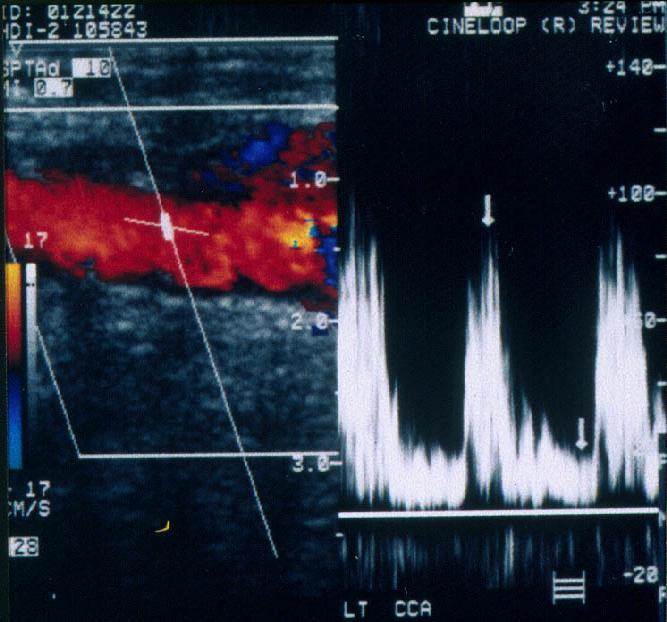
37 ICA: PSV 166 cm/sec EDV 79 cm/sec Stenosis: 50-69%??

38 CCA: ICA: PSV 166 cm/sec EDV 79 cm/sec CCA: PSV 96 cm/sec EDV 36 cm/sec Ratios: SVR 1.7 DVR 2.2 Stenosis = < 50% PATIENT IS HYPERTENSIVE


39 Normal Velocities Peak Systole ICA Peak Systole CCA End Diastole ICA End Diastole CCA 23 8
40 ABNORMAL RATIOS Peak Systole ICA 67 End Diastole ICA 23 Peak Systole CCA 23 End Diastole CCA 8 Systolic Ratio 2.91 (Diastolic Ratio Stenosis 50 69% Poor Cardiac Output Cardiomyopathy 2.88)
41 COMMON PITFALLS Mistaking ICA for ECA or ECA for ICA Improper plaque characterization Confusion over carotid grading criteria and which table or cut-off value to use Measuring CCA velocities at incorrect location Relying on systolic velocity parameters only Forgetting to integrate all information (internal consistency) In patients with arrhythmias, measuring velocities of compensatory beat Missing high grade stenosis with normal velocity
42
43 COMMON PITFALLS Mistaking ICA for ECA or ECA for ICA Improper plaque characterization Confusion over carotid grading criteria and which table or cut-off value to use Measuring CCA velocities at incorrect location Relying on systolic velocity parameters only Forgetting to integrate all information (internal consistency) In patients with arrhythmias, measuring velocities of compensatory beat Missing high grade stenosis with normal velocity
44
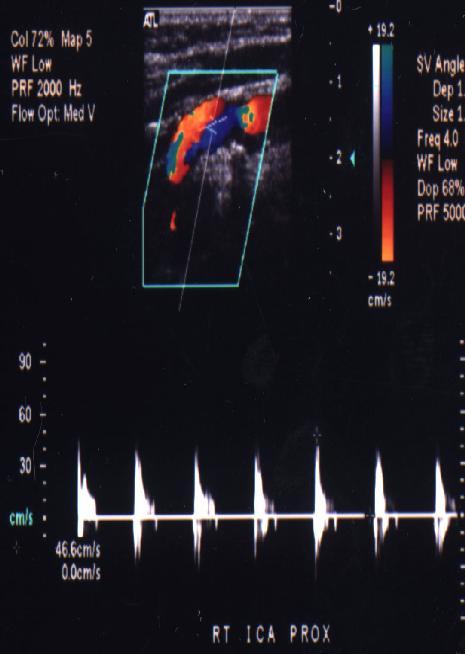
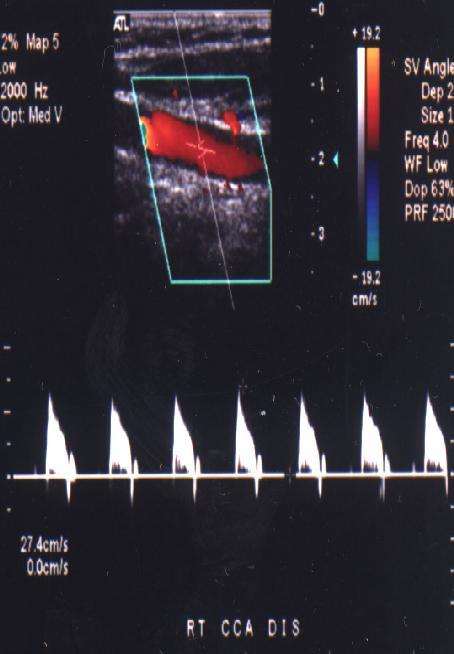
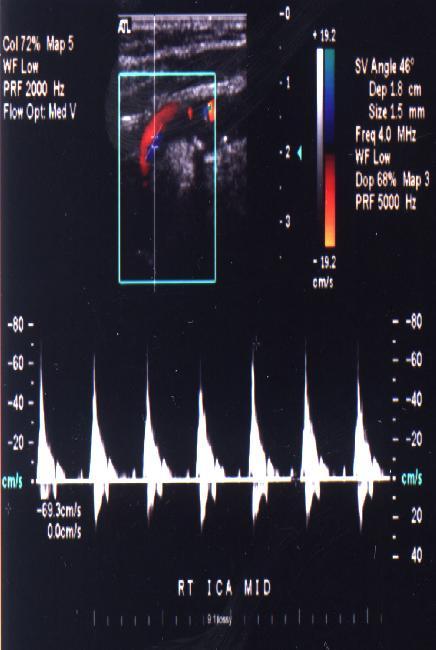
45 Rt ICA 69/0 Rt CCA 27/0 SVR 2.6
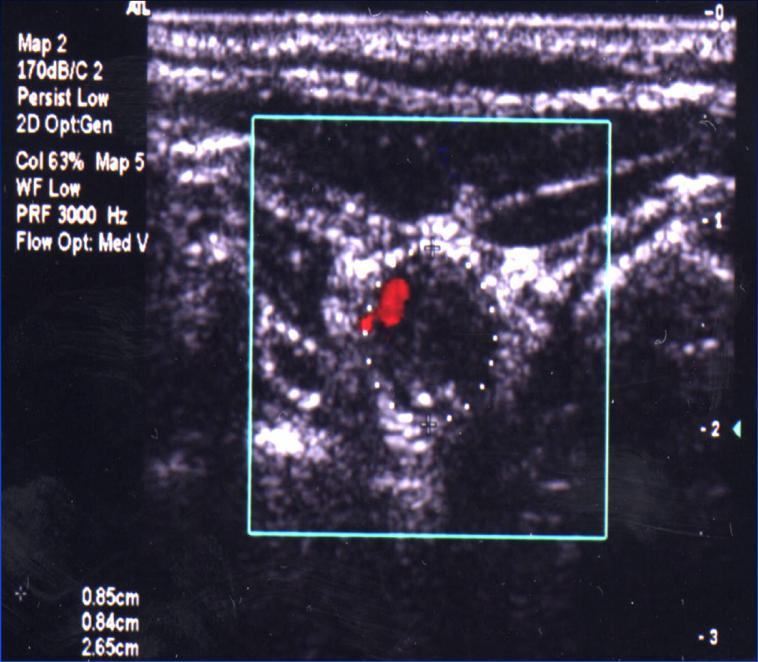
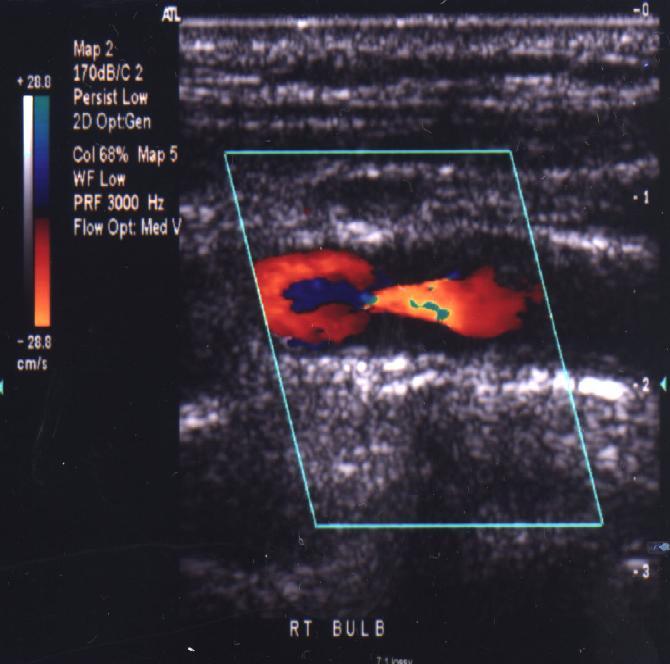
46 RT BULB
 (ml/min) and (cm/sec) THE EFFECT OF STENOSIS ON BLOOD FLOW 36 From Spencer &")
47 500 Velocity Volume Flow Fo = 3 MHZ = 60 Vessel Dia. = 5 mm Percent Stenosis Doppler Frequency (KHz) (ml/min) and (cm/sec) THE EFFECT OF STENOSIS ON BLOOD FLOW 36 From Spencer & Reid, Cerebrovascular Evaluation with Doppler Ultrasound. 1981
48 COMMON PITFALLS (continued) Incorrect angle position Inconsistent angle-cursor adjustment Ignoring symmetry of CCA Ignoring dampening of CCA Ignoring dampening of ICA Contralateral stenosis causing an ipsilateral velocity elevation Occlusion versus tight stenosis Unusual velocity measurements with post-op venous grafts


49 Incorrect Angle PSV = 61 cm/sec Angle = 60 PSV = 132 cm/sec Angle = 70
50 COMMON PITFALLS (continued) Incorrect angle position Inconsistent angle-cursor adjustment Ignoring symmetry of CCA Ignoring dampening of CCA Ignoring dampening of ICA Contralateral stenosis causing an ipsilateral velocity elevation Occlusion versus tight stenosis Unusual velocity measurements with post-op venous grafts

51 Dampening of CCA


52 Elevated Velocities PSV = 563 cm/sec, EDV = 325 cm/sec

53 Asymmetry of the CCA
54 Normal Velocity Measurements in ICA

55 Normal Velocities: Tardus Parvus

56 Innominate Stenosis
57 RECOMMENDATIONS FOR FOLLOW-UP RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT RECOMMENDATIONS FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT BASEDFORON ULTRASOUND ASSESSMENT ASYMPTOMATIC 1-39%** (1-50%)*** SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE HETEROGENEOUS PLAQUE 3 months 2 Then 6 months Then yearly 2-5 years depending the degree of plaque and other risk factors 1-3 years depending the degree of plaque Then yearly and other risk factors Medical therapy* Refer for evaluation for other sources such as cardioembolic disease or neurovascular sources of symptoms 3 months 2 6 months 2 Then every 6 months Then yearly until converted to homogeneous or degree of stenosis increases 3 months 2 ASYMPTOMATIC Then 6 months HETEROGENEOUS PLAQUE 1-39%** (1-50%)*** 3 months 2 Then 6 months Then yearly 3 months 2 Yearly Then every 6Medical months Medical Rx* Rx* until converted to HOMOGENEOUS PLAQUE HOMOGENEOUS PLAQUE SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE 2-5 years depending 3 months 2 the degree of plaque Then 6 months and other risk factors Then yearly Medical therapy* 1-3 years depending the degree of plaque and other risk factors 40-59%** Refer for evaluation homogeneous or for other sources degree of stenosis increases such as cardioembolic 60-79%** Refer to vascular 6-month follow-up 2 Refer to vascular Refer to vascular (50-70%)*** specialist** for stability, then specialist ** specialist** disease or annually (Alternatively, if no (Alternatively, if no neurovascular intervention, followintervention, followup every 3 months to up every 3 months to sources of assess stability) assess stability) 80-99%** Refer to vascular specialist** symptoms (>70%)*** *Medical Rx includes antiplatelet Rx, statin Rx, smoking good blood pressure control %** 3 months 2 cessation, andyearly 3 months 2 6 months 2 **Bluth et al. Criteria ***SRU Criteria Then every 6 months Then every 6 months Then yearly **Vascular specialist could be a vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on the skill set of providers given area. Treatment. converted to untilin anyconverted to recommended by these specialists could be endovascular until stent, endarterectomy, or intensive Medical Rx homogeneous or homogeneous or degree of stenosis degree of stenosis increases increases %** (50-70%)*** Refer to vascular specialist** 6-month follow-up 2 Refer to vascular for stability, then specialist ** Refer to vascular specialist** 1
58 RECOMMENDATIONS FOR FOLLOW-UP ASYMPTOMATIC SYMPTOMATIC BASED ON ULTRASOUND ASSESSMENT RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT HETEROGENEOUS FOR HOMOGENEOUS HETEROGENEOUS HOMOGENEOUS RECOMMENDATIONS FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT PLAQUE 1-39%** (1-50%)*** 1-39%** (1-50%)*** 40-59%** 60-79%** 40-59%** (50-70%)*** 80-99%** (>70%)*** PLAQUE PLAQUE PLAQUE 3 months years depending 3 months years depending Then 6 months the degree of plaque Then 6 months the degree of plaque ASYMPTOMATIC SYMPTOMATIC Then yearly and other risk factors Then yearly and other risk factors HETEROGENEOUS HOMOGENEOUS HETEROGENEOUS HOMOGENEOUS Medical Rx* Medical therapy* Refer for evaluation PLAQUE PLAQUE PLAQUE for other sources PLAQUE such2as 3 months years depending 3 months 1-3 years depending cardioembolic Then 6 months the degree of plaque Then 6 months the degree of plaque disease or Then yearly and other risk factors Then yearly and other risk factors neurovascular Medicalsources therapy* Refer for evaluation of symptoms for other sources 3 months 2 Yearly 3 months 2 6 months 2 such as Then every 6 months Then every 6 months Then yearly cardioembolic until converted to until converted to disease or homogeneous or homogeneous or degree of stenosis degree of stenosis neurovascular increases increases sources of Refer to vascular 6-month follow-up 2 Refer to vascular Refer to vascular 3 months 2 for stability,yearly 3 months 2 specialist** then specialist ** specialist** Medical Rx* every 6 months annually Then every Medical Rx* Then 6 months (Alternatively, if no Medical Rx* (Alternatively, if no converted to until converted to until intervention, follow intervention, follow homogeneous homogeneous or up every 3 months to or up every 3 months to degree of stenosis degree of stenosis assess stability) assess stability) Refer to vascular specialist** increases increases symptoms 6 months 2 Then yearly *Medical Rx includes antiplatelet Rx, smoking6-month cessationfollow-up, and good blood pressure control %** ReferRx, to statin vascular 2 Refer to vascular Refer to vascular **Bluth et al. Criteria45 (50-70%)*** specialist** for stability, then specialist ** specialist** 122 ***SRU Criteria annually Medical Rx* **Vascular specialist could bemedical a vascularrx* surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on the skill set of(alternatively, providers in any given specialists could be endovascular Treatment Rx* recommended by these. if no area. Medical (Alternatively, if no stent, endarterectomy, or intensive Medical Rx intervention, followup every 3 months to assess stability) 80-99%** (>70%)*** intervention, followup every 3 months to assess stability) Refer to vascular specialist** *Medical Rx includes antiplatelet Rx, statin Rx, smoking cessation, and good blood pressure control. **Bluth et al. Criteria45 ***SRU Criteria122 **Vascular specialist could be a vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon,
59 RECOMMENDATIONS FOR FOLLOW-UP BASED ON ULTRASOUND ASSESSMENT RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT ASYMPTOMATIC 1-39%** (1-50%)*** SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE 3 months 2 Then 6 months Then yearly 2-5 years depending the degree of plaque and other risk factors 3 months 2 Then 6 months Then yearly Medical therapy* 1-3 years depending the degree of plaque and other risk factors Refer for evaluation for other sources such as cardioembolic disease or neurovascular sources of symptoms 6 months 2 Then yearly RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT ASYMPTOMATIC 1-39%** (1-50%)*** 40-59%** 40-59%** SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE HETEROGENEOUS PLAQUE 3 months 2 Then 6 months Then yearly 2-5 years depending the degree of plaque and other risk factors 3 months 2 Then 6 months Then yearly Medical therapy* HOMOGENEOUS PLAQUE 1-3 years depending the degree of plaque and other risk factors Refer for evaluation for other sources such as 3 months 2 Yearly cardioembolic disease orrx* Then every 6 months Medical neurovascular until converted to sources of symptoms homogeneous or 3 months 2 Yearly 3 months 2 6 months 2 degree of stenosis Then every 6 months Then every 6 months Then yearly until converted to increases until converted to homogeneous or homogeneous or degree of stenosis degree of stenosis increases increases Refer to vascular 6-month follow-up 3 months 2 Then every 6 months until converted to homogeneous or degree of stenosis increases 60-79%** 2 Refer to vascular 60-79%** Refer to vascular 6-month follow-up 2 Refer to vascular Refer to vascular (50-70%)*** specialist** for stability, then specialist ** (50-70%)*** specialist** for stability, then specialist ** specialist** annually Medical Rx* annually (Alternatively, if no (Alternatively, if no no (Alternatively, if no intervention, follow-(alternatively, if intervention, followup every 3 months to up every-3 months to intervention, follow intervention, follow assess stability) assess stability) up every months to up every 3 months to 80-99%** Refer3 to vascular specialist** (>70%)*** assess stability) assess stability) 80-99%** *Medical Rx includes antiplatelet Rx, statin Rx, smoking cessation, and good blood pressure control. Refer to vascular specialist** **Bluth et al. Criteria45 (>70%)*** ***SRU Criteria122 Refer to vascular specialist** **Vascular specialist could be a vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on the skill set of providers in any given area. Treatment recommended by these specialists could be endovascular. *Medical Rxorincludes Rx, statin Rx, smoking cessation, and good blood pressure control. stent, endarterectomy, intensive Medicalantiplatelet Rx **Bluth et al. Criteria ***SRU Criteria **Vascular specialist could be a vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on the skill set of providers in any given area. Treatment recommended by these specialists could be endovascular. stent, endarterectomy, or intensive Medical Rx 1
60 RECOMMENDATIONS FOR FOLLOW-UP BASED ON ULTRASOUND ASSESSMENT RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT ASYMPTOMATIC 1-39%** (1-50%)*** SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE 3 months 2 Then 6 months Then yearly 2-5 years depending the degree of plaque and other risk factors 3 months 2 Then 6 months Then yearly Medical therapy* 1-3 years depending the degree of plaque and other risk factors Refer for evaluation for other sources such as cardioembolic disease or neurovascular sources of symptoms 6 months 2 Then yearly RECOMMENDATIONS FOR FOLLOW -UP BASED ON ULTRASOUND ASSESSMENT ASYMPTOMATIC 1-39%** (1-50%)*** 40-59%** 40-59%** SYMPTOMATIC HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE HETEROGENEOUS PLAQUE HOMOGENEOUS PLAQUE 3 months 2 Then 6 months Then yearly 2-5 years depending the degree of plaque and other risk factors 3 months 2 Then 6 months Then yearly Medical therapy* 1-3 years depending the degree of plaque and other risk factors Refer for evaluation for other sources such Rx*as cardioembolic disease or neurovascular sources of symptoms 6 months 2 Then yearly 3 months 2 Yearly Then every 6 months Medical until converted to homogeneous or degree of stenosis 3 months 2 Yearly 3 months 2 increases Then every 6 months Then every 6 months until converted to until converted to 3 months 2 Then every 6 months until converted to homogeneous or degree of stenosis increases or homogeneous or 60-79%** homogeneous follow-up 2 Refer to vascular degree of stenosisrefer to vascular degree of 6-month stenosis increases increases for stability, then (50-70%)*** specialist** specialist ** annually 60-79%** Refer to vascular 6-month follow-up 2 Refer to vascular Refer to vascular (Alternatively, Rx* (Alternatively, if no (50-70%)*** specialist** for stability, then if no specialist Medical ** specialist** annually Medical Rx* intervention, follow intervention, follow (Alternatively, if no if no up every 3 months(alternatively, to up every 3 months to intervention, followintervention, followup every 3 monthsassess to stability) up every 3 months to assess stability) assess stability) 80-99%** assess stability) Refer to vascular specialist** 80-99%** Refer to vascular specialist** (>70%)*** (>70%)*** *Medical Rx includes antiplatelet Rx, statin Rx, smoking cessation, and good blood pressure control. 45 *Medical Rx includes antiplatelet Rx, statin Rx, smoking cessation, and **Bluth et al. Criteria 45 ***SRU Criteria122 **Bluth et al. Criteria **Vascular specialist could be a 122 vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on thecriteria skill set of providers in any given area. Treatment recommended by these specialists could be endovascular ***SRU. stent, endarterectomy, or intensive Medical Rx Refer to vascular specialist** good blood pressure control. **Vascular specialist could be a vascular surgeon, interventional cardiologist, or interventional neuroradiologist or neurosurgeon, depending on the skill set of providers in any given area. Treatment recommended by these specialists could be endovascular. stent, endarterectomy, or intensive Medical Rx 1
61 Summary 1. The carotid evaluation study involves plaque characterization and stenosis grading 2. Either heterogeneous/homogeneous or the 1-4 International Classification System should be used 3. Careful attention must be directed to technique, similar to the attention needed to evaluate flow limiting stenosis

62 PLAQUE CONCLUSIONS Heterogeneous plaque histologically correlates with intraplaque hemorrhage. Heterogeneous plaque appears to be an unstable plaque The presence of significant stenosis and heterogeneous plaque appear to be independent risk factors.
63 CONCLUSION The key factor to identifying heterogeneous plaque is a focal sonolucent area greater than 50% of the plaque volume. Examination of the plaque must be made in both the sagittal and transverse planes.
64 Summary 4. Duplex US is an accurate method to assess flowlimiting stenosis 5. The SRU consensus group has recommended a new table, but if you have a tested verified system in your laboratory, you can continue to use it. 6. Integrate all anatomic and physiologic (hemodynamic) date to make an accurate interpretation and to insure internal consistency.
65 Summary 7. By careful attention to detail, you can avoid pitfalls and improve accuracy in duplex carotid interpretation
Disclosure Statement:
 Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL
 GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012
 Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Carotid Artery Doppler
 Carotid Artery Doppler Patient Position supine or semisupine head slightly hyper extended rotated 45 away from the side being examined. Higher frequency linear transducers (7 MHz) Vessels should be imaged
Carotid Artery Doppler Patient Position supine or semisupine head slightly hyper extended rotated 45 away from the side being examined. Higher frequency linear transducers (7 MHz) Vessels should be imaged
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Carotid US: More than just a chart on the wall
 Carotid US: More than just a chart on the wall Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section Medical
Carotid US: More than just a chart on the wall Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section Medical
Categorical Course: Update of Doppler US 8 : 00 8 : 20
 159 Categorical Course: Update of Doppler US 8 : 00 8 : 20 160 161 Table 1.Comparison of Recommended Values from Data in the Published Literature* S t u d y Lesion PSV E D V VICA/VCCA S e v e r i t y (
159 Categorical Course: Update of Doppler US 8 : 00 8 : 20 160 161 Table 1.Comparison of Recommended Values from Data in the Published Literature* S t u d y Lesion PSV E D V VICA/VCCA S e v e r i t y (
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
(Department of Radiology, Beylikdüzü State Hospital, İstanbul, Turkey) Corresponding Author: Dr. Mete Özdikici
 Corresponding Author: Dr. Mete Özdikici") Quest Journals Journal of Medical and Dental Science Research Volume 5~ Issue 6 (2018) pp: 61-65 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Quantitative Measurements
Quest Journals Journal of Medical and Dental Science Research Volume 5~ Issue 6 (2018) pp: 61-65 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Quantitative Measurements
Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease
 Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease Jan M. Sloves RVT, RCS, FASE Technical Director New York Cardiovascular Associates Disclosures
Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease Jan M. Sloves RVT, RCS, FASE Technical Director New York Cardiovascular Associates Disclosures
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards
 Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Quality ID #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care
: Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care") Quality ID #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Neurovascular Ultrasound Course
 Neurovascular Ultrasound Course William M. McKinney (6/6/30-10/24/03) Father of Neurosonology Founder, Neurosonology Course, WFUSM Welcome to Winston-Salem, NC, Wake Forest School of Medicine, and the
Neurovascular Ultrasound Course William M. McKinney (6/6/30-10/24/03) Father of Neurosonology Founder, Neurosonology Course, WFUSM Welcome to Winston-Salem, NC, Wake Forest School of Medicine, and the
Pitfalls in the evaluation of carotid artery stenosis. Serge Kownator «Centre Cardiologique et Vasculaire» Thionville, Fr
 Pitfalls in the evaluation of carotid artery stenosis Serge Kownator «Centre Cardiologique et Vasculaire» Thionville, Fr Disclosure Statement of Financial Interest I currently have, or have had over the
Pitfalls in the evaluation of carotid artery stenosis Serge Kownator «Centre Cardiologique et Vasculaire» Thionville, Fr Disclosure Statement of Financial Interest I currently have, or have had over the
Non-invasive Imaging of Carotid Artery Atherosclerosis
 Non-invasive Imaging of Carotid Artery Atherosclerosis 최연현 성균관의대삼성서울병원영상의학과 Noninvasive Techniques US with Doppler CT MRI Ultrasonography Techniques of Carotid US US Anatomy (ICA vs ECA) Gray scale and
Non-invasive Imaging of Carotid Artery Atherosclerosis 최연현 성균관의대삼성서울병원영상의학과 Noninvasive Techniques US with Doppler CT MRI Ultrasonography Techniques of Carotid US US Anatomy (ICA vs ECA) Gray scale and
Measure #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care
: Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care") Measure #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
Measure #195 (NQF 0507): Radiology: Stenosis Measurement in Carotid Imaging Reports National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
No financial or commercial relationships to disclose
 Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Vascular Portfolio: Carotid Reflection. Paige Fabre
 Vascular Portfolio: Carotid Reflection Paige Fabre 13654584 14 Carotid Reflection For this portfolio I produced three pieces of work; a case study, a PowerPoint of study protocol and a poster of stenosis
Vascular Portfolio: Carotid Reflection Paige Fabre 13654584 14 Carotid Reflection For this portfolio I produced three pieces of work; a case study, a PowerPoint of study protocol and a poster of stenosis
Sonographic Characterization of Carotid Plaque: Detection of Hemorrhage
 311 Sonographic Characterization of Carotid Plaque: Detection of Hemorrhage E. I. Bluth' D.Kai C. R. B. Merritt' M. Sullivan' G. Farr2 N. L. Mills 3 M. Foreman' K. Sloan' M. Schlater' J. Stewart 3 By careful
311 Sonographic Characterization of Carotid Plaque: Detection of Hemorrhage E. I. Bluth' D.Kai C. R. B. Merritt' M. Sullivan' G. Farr2 N. L. Mills 3 M. Foreman' K. Sloan' M. Schlater' J. Stewart 3 By careful
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions. No Disclosures. Prevalence >70% Asymptomatic ICA Stenosis*
 How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Screening for asymptomatic internal artery stenosis: Duplex criteria for discriminating 60% to 99% stenosis
 Screening for asymptomatic internal artery stenosis: Duplex criteria for discriminating 60% to 99% stenosis carotid Gregory L. Moneta, MD, James M. Edwards, MD, George Papanicolaou, MD, Thomas Hatsukami,
Screening for asymptomatic internal artery stenosis: Duplex criteria for discriminating 60% to 99% stenosis carotid Gregory L. Moneta, MD, James M. Edwards, MD, George Papanicolaou, MD, Thomas Hatsukami,
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC
 CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Lezione 3 Tronchi Sovraortici
 CORSO DI CERTIFICAZIONE DI COMPETENZA in ECOGRAFIA VASCOLARE GENERALE Lezione 3 Tronchi Sovraortici Settore formazione 2007-2009: Direttore: Paolo G. Pino Marco Campana, Antonella Moreo, Fausto Rigo, Ketty
CORSO DI CERTIFICAZIONE DI COMPETENZA in ECOGRAFIA VASCOLARE GENERALE Lezione 3 Tronchi Sovraortici Settore formazione 2007-2009: Direttore: Paolo G. Pino Marco Campana, Antonella Moreo, Fausto Rigo, Ketty
Carotid intima media thickness as an usefull tool in predicting cerebrovaskular events
 Carotid intima media thickness as an usefull tool in predicting cerebrovaskular events Poster No.: C-0005 Congress: ECR 2015 Type: Authors: Keywords: DOI: Scientific Exhibit A. Rahimic - Catic; Sarajevo/BA
Carotid intima media thickness as an usefull tool in predicting cerebrovaskular events Poster No.: C-0005 Congress: ECR 2015 Type: Authors: Keywords: DOI: Scientific Exhibit A. Rahimic - Catic; Sarajevo/BA
What effects will proximal or distal disease have on an waveform?
 Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography
 Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
Evaluation of Carotid Vessels and Vertebral Artery in Stroke Patients with Color Doppler Ultrasound and MR Angiography Dr. Pramod Shaha 1, Dr. Vinay Raj R 2, Dr. (Brig) K. Sahoo 3 Abstract: Aim & Objectives:
Morphological duplex ultrasound criteria how to assess and report echolucency, inhomogeneity and ulceration
 Morphological duplex ultrasound criteria how to assess and report echolucency, inhomogeneity and ulceration Prof. Daniel Staub, Angiology, University Hospital Basel, Switzerland daniel.staub@usb.ch Disclosure
Morphological duplex ultrasound criteria how to assess and report echolucency, inhomogeneity and ulceration Prof. Daniel Staub, Angiology, University Hospital Basel, Switzerland daniel.staub@usb.ch Disclosure
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Imaging. Dr Andrew Farrall. Consultant Neuroradiologist
 20121123 SSCA http://www.neuroimage.co.uk/network Andrew Farrall Carotid Imaging Dr Andrew Farrall Consultant Neuroradiologist SFC Brain Imaging Research Centre (www.sbirc.ed.ac.uk), SINAPSE Collaboration
20121123 SSCA http://www.neuroimage.co.uk/network Andrew Farrall Carotid Imaging Dr Andrew Farrall Consultant Neuroradiologist SFC Brain Imaging Research Centre (www.sbirc.ed.ac.uk), SINAPSE Collaboration
Critical appraisal of the Carotid Duplex Consensus criteria in the diagnosis of carotid artery stenosis
 From the Society for Vascular Surgery Critical appraisal of the Carotid Duplex Consensus criteria in the diagnosis of carotid artery stenosis Ali F. AbuRahma, MD, a Mohit Srivastava, MD, a Patrick A. Stone,
From the Society for Vascular Surgery Critical appraisal of the Carotid Duplex Consensus criteria in the diagnosis of carotid artery stenosis Ali F. AbuRahma, MD, a Mohit Srivastava, MD, a Patrick A. Stone,
Duplex Criteria for Determination of 50% or Greater Carotid Stenosis
 Article Duplex Criteria for Determination of 50% or Greater Carotid Stenosis David G. Neschis, MD, Frank J. Lexa, MD, Julia T. Davis, RN, RVT, Jeffrey P. Carpenter, MD, RVT Recently the North American
Article Duplex Criteria for Determination of 50% or Greater Carotid Stenosis David G. Neschis, MD, Frank J. Lexa, MD, Julia T. Davis, RN, RVT, Jeffrey P. Carpenter, MD, RVT Recently the North American
Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical
 Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical School Boston, Massachusetts Disclosures I do not have
Carotid Duplex: Beyond Stenosis Ido Weinberg, MD Vascular Medicine Massachusetts General Hospital Assistant Professor of Medicine Harvard Medical School Boston, Massachusetts Disclosures I do not have
Carotid arterial ultrasound scan imaging: A direct approach to stenosis measurement
 Carotid arterial ultrasound scan imaging: A direct approach to stenosis measurement Hugh G. Beebe, MD, Sergio X. Salles-Cunha, PhD, Robert P. Scissons, RVT, Steven M. Dosick, MD, Ralph C. Whalen, MD, Steven
Carotid arterial ultrasound scan imaging: A direct approach to stenosis measurement Hugh G. Beebe, MD, Sergio X. Salles-Cunha, PhD, Robert P. Scissons, RVT, Steven M. Dosick, MD, Ralph C. Whalen, MD, Steven
Pathology of Coronary Artery Disease
 Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Fibromuscular Dysplasia. Miranda Forrest Baker College
 Fibromuscular Dysplasia Miranda Forrest Baker College Overview Case Study Patient Information Exam Images Findings FMD Types Signs and Symptoms Treatment Case Study Patient Information Female 57 years
Fibromuscular Dysplasia Miranda Forrest Baker College Overview Case Study Patient Information Exam Images Findings FMD Types Signs and Symptoms Treatment Case Study Patient Information Female 57 years
For the ICSS Investigators. 7 th Munich Vascular Conference Munich, 7 December 2017
 Restenosis and its impact on recurrent stroke risks after CAS and CEA for symptomatic carotid stenosis results from the International Carotid Stenting Study Leo H Bonati, John Gregson, Joanna Dobson, Dominick
Restenosis and its impact on recurrent stroke risks after CAS and CEA for symptomatic carotid stenosis results from the International Carotid Stenting Study Leo H Bonati, John Gregson, Joanna Dobson, Dominick
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Radial Artery Assessment for Coronary Artery Bypass
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Radial Artery Assessment for Coronary Artery Bypass This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Radial Artery Assessment for Coronary Artery Bypass This Guideline was prepared by the Professional Guidelines Subcommittee of the Society for Vascular
COLOUR DOPPLER EVALUATION OF DEGREE OF STENOSIS AND PLAQUE MORPHOLOGY IN EXTRACRANIAL CAROTID ARTERIES IN PATIENTS OF STROKE
 wjpmr, 2019, 5(1), 122-128 SJIF Impact Factor: 4.639 Hassan et al. Research Article WORLD JOURNAL OF PHARMACEUTICAL AND MEDICAL RESEARCH ISSN 2455-3301 www.wjpmr.com WJPMR COLOUR DOPPLER EVALUATION OF
wjpmr, 2019, 5(1), 122-128 SJIF Impact Factor: 4.639 Hassan et al. Research Article WORLD JOURNAL OF PHARMACEUTICAL AND MEDICAL RESEARCH ISSN 2455-3301 www.wjpmr.com WJPMR COLOUR DOPPLER EVALUATION OF
Duplex Carotid Sonography Peak Systolic Velocity in Quantifying Internal Carotid Artery Stenosis
 Duplex Carotid Sonography Peak Systolic Velocity in Quantifying Internal Carotid Artery Stenosis Cynthia E Withers, MD", Barbara B Gosink, MD", Alison M Keightley, MD", Giovanna Casola, MD", Arthur A Lee,
Duplex Carotid Sonography Peak Systolic Velocity in Quantifying Internal Carotid Artery Stenosis Cynthia E Withers, MD", Barbara B Gosink, MD", Alison M Keightley, MD", Giovanna Casola, MD", Arthur A Lee,
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Vascular Sonography Examination
 Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES
 Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES No financial or commercial relationships to disclose Carotid artery disease: Stroke is one of the most serious causes of mortality and morbidity
Carotid Imaging IT S ABOUT MORE THAN JUST OBTAINING THE IMAGES No financial or commercial relationships to disclose Carotid artery disease: Stroke is one of the most serious causes of mortality and morbidity
Proposed duplex velocity criteria for carotid restenosis following carotid endarterectomy with patch closure
 From the Southern Association for Vascular Surgery Proposed duplex velocity criteria for carotid restenosis following carotid endarterectomy with patch closure Ali F. AbuRahma, MD, a Patrick Stone, MD,
From the Southern Association for Vascular Surgery Proposed duplex velocity criteria for carotid restenosis following carotid endarterectomy with patch closure Ali F. AbuRahma, MD, a Patrick Stone, MD,
Detection of carotid plaque neovascularization with Superb Micro-Vascular Imaging
 Detection of carotid plaque neovascularization with Superb Micro-Vascular Imaging Yong Qiang Professor Ultrasonic Department, Beijing An-Zhen Hospital, Capital Medical University, China 1. Background Conventional
Detection of carotid plaque neovascularization with Superb Micro-Vascular Imaging Yong Qiang Professor Ultrasonic Department, Beijing An-Zhen Hospital, Capital Medical University, China 1. Background Conventional
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
STRUCTURED EDUCATION REQUIREMENTS IMPLEMENTATION DATE: JULY 1, 2016
 STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Color Doppler Imaging Evaluation of Proximal Vertebral Artery Stenosis
 Vascular and Interventional Radiology Original Research Hua et al. Color Doppler Imaging of Proximal Vertebral Artery Stenosis Vascular and Interventional Radiology Original Research Yang Hua 1 Xiu-Feng
Vascular and Interventional Radiology Original Research Hua et al. Color Doppler Imaging of Proximal Vertebral Artery Stenosis Vascular and Interventional Radiology Original Research Yang Hua 1 Xiu-Feng
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report
 P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
Three-Dimensional Color Doppler Sonography in Carotid Artery Stenosis
 AJNR Am J Neuroradiol 24:1294 1299, August 2003 Three-Dimensional Color Doppler Sonography in Carotid Artery Stenosis Robert A. Bucek, Markus Reiter, Albert Dirisamer, Markus Haumer, Angelika Fritz, Erich
AJNR Am J Neuroradiol 24:1294 1299, August 2003 Three-Dimensional Color Doppler Sonography in Carotid Artery Stenosis Robert A. Bucek, Markus Reiter, Albert Dirisamer, Markus Haumer, Angelika Fritz, Erich
8/20/18. The Doppler Effect. Objectives. What is the Doppler Effect. Doppler principles. Spectral Waveform. Image recognition. Vascular Ultrasound
 Vascular Ultrasound: Physics and Haemodynamics Objectives Doppler principles Spectral Waveform Key factors Haemodynamics: Stenosis Waveforms Image recognition Vascular Ultrasound: A flawed paradigm What
Vascular Ultrasound: Physics and Haemodynamics Objectives Doppler principles Spectral Waveform Key factors Haemodynamics: Stenosis Waveforms Image recognition Vascular Ultrasound: A flawed paradigm What
Image Formation (10) 2 Evaluation and Selection of Representative Images (10)
 2 Evaluation and Selection of Representative Images (10)") STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Antegrade and retrograde flow of carotid
 Antegrade and retrograde flow of carotid The ECA waveform is high resistance and may have retrograde flow in diastole.. They should always demonstrate antegrade flow (toward the brain) and be. external
Antegrade and retrograde flow of carotid The ECA waveform is high resistance and may have retrograde flow in diastole.. They should always demonstrate antegrade flow (toward the brain) and be. external
Merwyn Fernandes, B Keerthiraj, Ajith R Mahale, Ashwini Kumar, Anees Dudekula
 Original Article Evaluation of carotid arteries in stroke patients using color Doppler sonography: A prospective study conducted in a tertiary care hospital in South India Merwyn Fernandes, B Keerthiraj,
Original Article Evaluation of carotid arteries in stroke patients using color Doppler sonography: A prospective study conducted in a tertiary care hospital in South India Merwyn Fernandes, B Keerthiraj,
Duplex Doppler Sonography of the Carotid Artery: False-Positive Results in an Artery Contralateral to an Artery with Marked Stenosis
 049 Duplex Doppler Sonography of the Carotid Artery: False-Positive Results in an Artery Contralateral to an Artery with Marked Stenosis William W. Beckett, Jr. Patricia C. Davis James C. Hoffman, Jr.
049 Duplex Doppler Sonography of the Carotid Artery: False-Positive Results in an Artery Contralateral to an Artery with Marked Stenosis William W. Beckett, Jr. Patricia C. Davis James C. Hoffman, Jr.
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Stroke prevention in asymptomatic carotid stenosis. ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ
 Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Vascular Ultrasound: Current state, current needs, future directions
 Vascular Ultrasound: Current state, current needs, future directions Laurence Needleman, MD Thomas Jefferson University Hospitals Sidney Kimmel Medical College of Thomas Jefferson University Disclosures
Vascular Ultrasound: Current state, current needs, future directions Laurence Needleman, MD Thomas Jefferson University Hospitals Sidney Kimmel Medical College of Thomas Jefferson University Disclosures
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!!
 PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!! Prof Piotr Pieniazek MD PhD Jagiellonian University Institute of Cardiology, John Paul II Hospital Krakow, Poland
PrOspective multicenter study of carotid artery stenting Usinng mer Stent OCEANUS study!!! Prof Piotr Pieniazek MD PhD Jagiellonian University Institute of Cardiology, John Paul II Hospital Krakow, Poland
Carotid Stenosis (carotid artery disease)
") 1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
Duplex US of the External Carotid Artery
 Acta Radiologica ISSN: 0284-1851 (Print) 1600-0455 (Online) Journal homepage: https://www.tandfonline.com/loi/iard20 Duplex US of the External Carotid Artery M. J. Päivänsalo, T. M. J. Siniluoto, T. A.
Acta Radiologica ISSN: 0284-1851 (Print) 1600-0455 (Online) Journal homepage: https://www.tandfonline.com/loi/iard20 Duplex US of the External Carotid Artery M. J. Päivänsalo, T. M. J. Siniluoto, T. A.
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Goals. Access flow and renal artery stenosis evaluation by Doppler ultrasound. Reimbursement. WHY use of Doppler Ultrasound
 Access flow and renal artery stenosis evaluation by Doppler ultrasound Adina Voiculescu, MD Interventional Nephrology Brigham and Women s Hospital Boston Instructor at Harvard Medical School Understand
Access flow and renal artery stenosis evaluation by Doppler ultrasound Adina Voiculescu, MD Interventional Nephrology Brigham and Women s Hospital Boston Instructor at Harvard Medical School Understand
Transducer Selection. Renal Artery Duplex Exam. Renal Scan. Renal Scan Echogenicity. How to Perform an Optimal Renal Artery Doppler Examination
 How to Perform an Optimal Renal Artery Doppler Examination Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging
How to Perform an Optimal Renal Artery Doppler Examination Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging
頸動脈の超音波検査 頸動脈エコーの原理 患者情報の収集 検査時の患者の体位 超音波装置の条件設定 特集 : 脈管疾患診断における非侵襲的画像診断 : 進歩と現状. J Jpn Coll Angiol :
 Online publication January 22, 2010 総 説 特集 : 脈管疾患診断における非侵襲的画像診断 : 進歩と現状 頸動脈の超音波検査 要旨 : J Jpn Coll Angiol 2009 49: 453 458 Key words: brain infarction, transient ischemic attack, amaurosis fugax, intima
Online publication January 22, 2010 総 説 特集 : 脈管疾患診断における非侵襲的画像診断 : 進歩と現状 頸動脈の超音波検査 要旨 : J Jpn Coll Angiol 2009 49: 453 458 Key words: brain infarction, transient ischemic attack, amaurosis fugax, intima
TO CATCH A THIEF: IMAGING OF SUBCLAVIAN STEAL
 October 2013 TO CATCH A THIEF: IMAGING OF SUBCLAVIAN STEAL Sumir Pandit, Harvard Medical School, Year III 1 AGENDA Introduction to our patient A.B. Anatomy review of aorta and branches CT imaging of our
October 2013 TO CATCH A THIEF: IMAGING OF SUBCLAVIAN STEAL Sumir Pandit, Harvard Medical School, Year III 1 AGENDA Introduction to our patient A.B. Anatomy review of aorta and branches CT imaging of our
What Do We Know? Disclosure Statement: 3/11/2015. Deep abdominal imaging
 Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
THE incidence of stroke after noncardiac surgery
 Lack of Association between Carotid Artery Stenosis and Stroke or Myocardial Injury after Noncardiac Surgery in High-risk Patients ABSTRACT Background: Whether carotid artery stenosis predicts stroke after
Lack of Association between Carotid Artery Stenosis and Stroke or Myocardial Injury after Noncardiac Surgery in High-risk Patients ABSTRACT Background: Whether carotid artery stenosis predicts stroke after
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Carotid Ddisease, Carotid IMT and Risk of Stroke
 Carotid Ddisease, Carotid IMT and Risk of Stroke TATJANA RUNDEK, MD PhD Professor of Neurology, Epidemiology and Public Health Director, Clinical translational Division Department of Neurology, Miller
Carotid Ddisease, Carotid IMT and Risk of Stroke TATJANA RUNDEK, MD PhD Professor of Neurology, Epidemiology and Public Health Director, Clinical translational Division Department of Neurology, Miller
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Visceral Vascular Ultrasound. Joel Thompson, MD, MPH Borg & Ide Imaging
 Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging Objectives: Review major abdominal vascular structures Identify normal peak systolic velocity (PSV) for major abdominal arteries.
Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging Objectives: Review major abdominal vascular structures Identify normal peak systolic velocity (PSV) for major abdominal arteries.
The carotid atheromatous plaque: a multi-disciplinary approach towards optimal management of symptomatic and asymptomatic subjects
 The carotid atheromatous plaque: a multi-disciplinary approach towards optimal management of symptomatic and asymptomatic subjects Spyretta Golemati, PhD Lecturer in Biomedical Engineering, Medical School,
The carotid atheromatous plaque: a multi-disciplinary approach towards optimal management of symptomatic and asymptomatic subjects Spyretta Golemati, PhD Lecturer in Biomedical Engineering, Medical School,
CEREBRAL ISCHAEMIA AND STROKE; ROLE OF CAROTID DOPPLER
 The Professional Medical Journal DOI: 10.1797/TPMJ/17.4001 ORIGINAL PROF-4001 CEREBRAL ISCHAEMIA AND STROKE; ROLE OF CAROTID DOPPLER 1. MBBS, DIP Radiology Radiologist 2. MBBS, FCPS (Med), FACP Medical
The Professional Medical Journal DOI: 10.1797/TPMJ/17.4001 ORIGINAL PROF-4001 CEREBRAL ISCHAEMIA AND STROKE; ROLE OF CAROTID DOPPLER 1. MBBS, DIP Radiology Radiologist 2. MBBS, FCPS (Med), FACP Medical
Hemodynamics in the Stenosed Carotid Bifurcation with Plaque Ulceration
 Western University Scholarship@Western Electronic Thesis and Dissertation Repository March 2011 Hemodynamics in the Stenosed Carotid Bifurcation with Plaque Ulceration Emily Y. Wong The University of Western
Western University Scholarship@Western Electronic Thesis and Dissertation Repository March 2011 Hemodynamics in the Stenosed Carotid Bifurcation with Plaque Ulceration Emily Y. Wong The University of Western
Carotid artery occlusion: Positive predictive value of duplex sonography compared with arteriography
 Carotid artery occlusion: Positive predictive value of duplex sonography compared with arteriography Jonathan D. Kirsch, MD, Louis R. Wagner, MD, E. Meredith James, MD, J. William Charboneau, MD, Douglas
Carotid artery occlusion: Positive predictive value of duplex sonography compared with arteriography Jonathan D. Kirsch, MD, Louis R. Wagner, MD, E. Meredith James, MD, J. William Charboneau, MD, Douglas
ASDIN 7th Annual Scientific Meeting DISCLOSURES TECHNICAL CONSIDERATIONS TECHNICAL CONSIDERATIONS UTILITY OF ULTRASOUND IN EVALUATING ACCESS
 DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
OCT. molecular imaging J Jpn Coll Angiol, 2008, 48: molecular imaging MRI positron-emission tomography PET IMT
 48 6 CT MRI PET OCT molecular imaging J Jpn Coll Angiol, 2008, 48: 456 461 atherosclerosis, imaging gold standard computed tomography CT magnetic resonance imaging MRI CT B intima media thickness IMT B
48 6 CT MRI PET OCT molecular imaging J Jpn Coll Angiol, 2008, 48: 456 461 atherosclerosis, imaging gold standard computed tomography CT magnetic resonance imaging MRI CT B intima media thickness IMT B
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Author Query: 1. Please provide yellow arrow in figure as you mentioned in the legend (caption). Peripheral Vascular Ultrasound
. Peripheral Vascular Ultrasound") uthor Query: 1. Please provide yellow arrow in figure 33.16 as you mentioned in the legend (caption). CHPTER 33 Peripheral Vascular Ultrasound Ricardo enenstein, Muhamed Saric Snapshot ¾Ultrasound Diagnosis
uthor Query: 1. Please provide yellow arrow in figure 33.16 as you mentioned in the legend (caption). CHPTER 33 Peripheral Vascular Ultrasound Ricardo enenstein, Muhamed Saric Snapshot ¾Ultrasound Diagnosis
Carotid Stenting and Surgery in 2016 in Russia
 Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia
Carotid Stenting and Surgery in 2016 in Russia Novosibirsk research institute of circulation pathology named by Meshalkin, Novosibirsk, Russia Starodubtsev V., Karpenko A., Ignatenko P. Annually in Russia