At the conclusion of this activity, participants will be able to: 1. Classify different etiologies of ischemic stroke
|
|
|
- Lambert Hopkins
- 5 years ago
- Views:
Transcription
1 Alan Dobson MD
2 At the conclusion of this activity, participants will be able to: 1. Classify different etiologies of ischemic stroke 2. Identify different approaches for recanalization for ischemic stroke 3. Recognize signs and symptoms of ischemic stroke and common missed stroke syndrome and stroke mimics

3 I Have No Conflicts of Interest to Disclose
4 Term refers the sudden onset of symptoms from the Stroke of God s Hand Stroke is a sudden onset of neurological signs and symptoms from either focal cerebral ischemia or hemorrhage (older term apoplexy) By definition symptoms need to last for 24 hours. If symptoms are less and no damage to CNS found this is referred to as a Transient Ischemic Attack(TIA)

5 600,000 ischemic strokes and 100,000 hemorrhagic strokes per year in the US Leading cause of permanent disability in adults and 3 rd leading cause of death

6
 in the Stroke")
7 Stroke distribution correlates with other vascular risk factors (DM, Obesity, Hypertension) in the Stroke Belt

8 Transient and sudden neurological dysfunction best explained by focal CNS ischemia without permanent damage lasting less then 24 hours Most TIAs are approx minutes. Symptoms lasting more than a couple hours are likely due to a small stroke Risk for stroke can be calculated by using ABCD2-higest in first 90 days

9
10 Diagnosis of TIA is all in a detailed history of symptoms and signs Anterior circulation (Carotid) Ipsilateral Amaurosis Fugax Contralateral sensory or motor dysfunction Aphasia or hemianopsia(can also be posterior circulation) Posterior Circulation (Vertebral) Ipsilateral face contralateral body(crossed findings) Two or more of the following vertigo, diplopia, dysphagia, dysarthria, ataxia- Symptoms not acceptable as evidence of TIA Syncope, dizziness, confusion, or isolated - vertigo, diplopia, dysarthria, ataxia, or amnesia
11 Embolism 32% Lacunes 18.5% Hypertensive hemorrhage 15.5% Atherosclerotic thrombosis 12% Indeterminate 9.5% Other 8% Ruptured aneurysms and vascular malformation 4.5% Data from Boston City Hospital Autopsy study 1949 C.M. Fisher R.D. Adams

12 Cerebrovascular disorders mechanism/etiology
 Paradoxical emboli (from the venous system due to")
13 Usually present as sudden onset of symptoms Artery to artery emboli from atheromas or dissection, most commonly emboli can arise from the aorta and carotid for anterior circulation, or aorta, subclavian or vertebral system for posterior circulation strokes Cardiogenic- (Atrial fibrillation, Valves, Endocarditis Mural Thrombus, Myxoma) Paradoxical emboli (from the venous system due to right to left shunting)-pfo Air and fat emboli from trauma or IVs
14 Atherosclerotic plaques causing atherothrombotic occlusion of large vessels Can have slower symptom onset and more waxing and waning then embolic events Most common locations are areas of turbulent flow such as: Origin of internal carotid artery-amenable to CEA Cavernous Carotid artery-not amenable to CEA Vertebral artery at the junction with basilar artery Proximal middle cerebral artery Posterior cerebral artery Anterior cerebral artery Microhyalinosis causing gradual thrombosis of small angiographic invisible penetrating arteries causes lacunar strokes Most common locations for lacunar strokes- Basil ganglia, Pons, Cerebellum, deep white matter of the hemispheres-are these the white matter changes seen in older hypertensive patients?

15 Mitochondrial disorders such as MELAS can cause cell death from cellular level energy failure Prolonged seizures can cause cell death from glutamate induced excitotoxicity Anoxia, carbon monoxide poisoning, severe hypoglycemia and other metabolic problems Migraines usually with aura and can cause stroke-focal vasospasm?
16 Sinus Thrombosis (Thrombosis of cerebral venous outflow PRES(Posterior Reversible encephalopathy Syndrome) Cerebral Vasoconstriction
17 Occlusion of the dural venous sinus (superior sagittal, internal cerebral veins, transverse/sigmoid) accounts for approx.. 1% of all strokes and commonly missed and treatable Can present with headaches, papilledema, 6 th nerve palsy, increased ICP or focal neurological deficits Can produce venous infarctions or intracranial hemorrhages from venous congestion frequently bilateral Can occasionally be seen on CT by looking for increased density of the sinuses. Best found on MRI or dedicated MRV Treatment is with anticoagulation or rarely intrasinus intervention (TPA, mechanical clot extraction) More common after dehydration, hypercoagable disorders and in the peripartum period

18
 Can also occur with pregnancy as well as in")
19 Syndrome of loss of normal autoregulatory control of cerebral blood flow. Believed to affect the posterior circulation preferentially Classic history is rapid change in BP causing confusion and vision problems(cortical blindness) Can also occur with pregnancy as well as in patients treated with VEGF inhibitors MRI can show edema and in severe cases irreversible infarction (restricted diffusion) Treatment is controlling blood pressure and symptoms usually resolve within two weeks but could persist if infarction occurs


20 34 y/o female with amnesia and blindness with preeclampsia and methamphetamine use 56 y/o male treated with Avastin for CLL with confusion and vision problems
21 Best described in patient with aneurysmal Subarachnoid hemorrhage Patients develops spasms of cerebral vasculature causing focal ischemia In aneurysmal subarachnoid patients treated with hypervolemia, hypernatremia and hypertension as well as Calcium channel Nimodipine or catheter intervention Can also occur in the peripartium period, migraine patients, and patients exposed to vasoactive compounds (SSRI, SNRI, nicotine, triptans, etc.) Cerebral vasospasm usually resolves within two months

 Marked")

22 MRI shows Left Posterior inferior Cerebellar Artery Stroke(PICA) Marked narrowing of vertebral arteries and basilar arteries
23 Todds paralysis after focal seizure (transient cerebral dysfunction after seizure) Migraine can cause a variety of focal neurological deficits (vision, parasthesia, hemiplegia, confusion, aphasia) Conversion reaction *Cervical spine problems (may be unilateral early on but should spare cranial nerves) Metabolic derangements (glucose, hepatic, uremia, hypercapnia, periodic paralysis) Worsening of old stroke symptoms with infection Peripheral vertigo Masses such as tumors or intracranial abscess
24 Named after Robert Todd Irish Neurologist in 1849 Is due to persistent focal cerebral dysfunction (hemiparesis, hemanopsia, aphasia etc.)usually more common after a focal motor seizures. History of LOC and rhythmic movements can be helpful in detecting Todd's Paralysis Usually resolves within 36 hours
25 Patient can have focal neurological deficits before, after or without onset of headaches Most common deficits are scotomas, confusion or parsthesia that begin in hands or lips and progress in somatotopic fashion. However any neurological deficits can be a result of migraine History of recurrent stereotyped episodes with negative MRIs should raise suspicion for Migraines Neurological deficits believed to be due to spreading cortical depression and careful history might reveal symptoms spread in somotopic fashion
26 Usually hereditary disorder characterized by recurrent episodes of transient hemiplegia Caused by a variety of genetic channelopathies of sodium channel genes that can also have progressive neurological symptoms (episodic ataxia, Spinocerbellar ataxia type 6, etc.) Best characterized gene are CACNA1A, ATP1A2, SCN1A which genetic testing is available Sometimes responds to verapamil or acetazolamide
27 Can be due to structural lesions (disk, abscess, tumor), vascular disease (Stroke, AVMs, Dural AV fistula) or inflammation (transverse myelitis, infections) Key physical exam finding are sensory and myotomal level with sparing of cranial nerves. Can be asymmetric symptoms. Depending on chronicity might have upper motor nerve finding of hyperreflexia and Babinski



28
29 Salvaging viable brain tissue with therapies such as thrormobolysis and revascularization in acute period (IV TPA and intra-arterial therapy) Avoidance of post stroke complications (Cerebral Edema, DVT, Aspiration Pneumonia) Evaluation for rehabilitation Secondary Stroke prevention Addressing stroke risk factors

30 Every minute 2 million neurons die in a MCA stroke TPA Treatment within the first 90 minutes of onset increased the odds of an excellent outcome by 2.6-fold In the 91- to 180-minute window by 1.6-fold In the 181- to 270-minute window by 1.3 fold Every 10 minutes in which therapy is delayed, one fewer of each hundred treated patients benefits.
31
32 Approved based on NINDS trial in 1995 Of 100 patients treated within the first 3 hours, 32 had a better outcome as a result and 3 had a worse outcome compared to placebo Number needed to treat for minimal or no disability at follow up compared to placebo was 8 ECASS hour window had about ½ benefit with a similar number needed to harm


33 IV TPA has been FDA approved since 1996 for up to 3 hours after last time patient seen well ECASS III showed benefit in select patient up to 4.5 hours While it can be given up to 4.5 hours, patients who receive TPA sooner generally have lower bleeding risk and greater chances of recovery Intra-arterial therapy is available at UNM 24/7 and generally can be used up to 6-24 hours in patients with large vessel occlusion (Internal Carotid, Basilar artery, Middle Cerebral Artery)
34 Oral anticoagulant use Major surgery or serious trauma in previous 14 days Administration of heparin within 48 hrs and an elevated PTT at Presentation or upper limits of normal Pregnancy Age less then 18? Stroke or intracranial surgery in last 3 months
35 IV TPA has poor recanalization rates for large vessel disease Multiple randomized trial have shown clear benefit compared to IV TPA alone Mechanical embolectomy in general double the chance of independent living (modified Rankin less then 3 compared to IV TPA Is now considered standard of care for large vessel strokes NIH scale greater then 8 can help predict patients with large vessel occlusion




36
37 Improved rates of recanualization compared to older devices Allows immediate restoration of blood flow to ischemic tissue

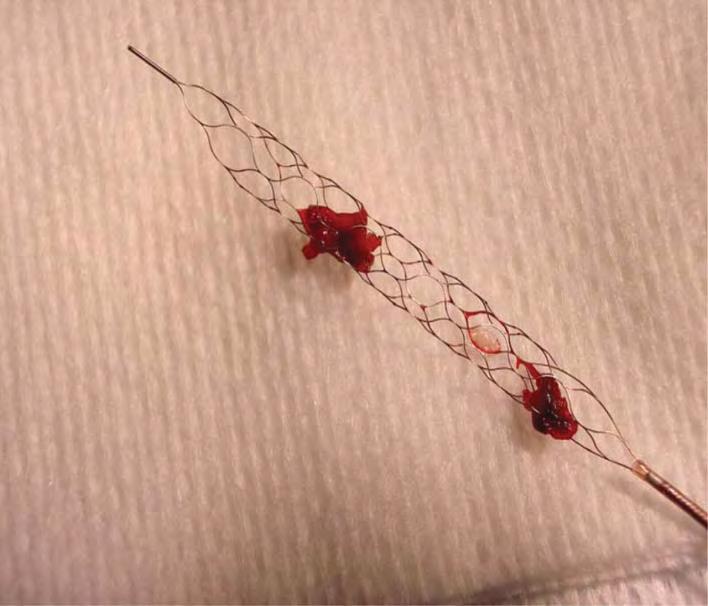
38 Solitaire Trevo
39 M R CLEAN First large trial in 2016 which showed clear benefit of mechanical revascularization over TPA for symptoms less then 6 hours DAWN trial-preliminary data shows benefit up to 24 hours out in select patient with large Bessel occlusion After 20 years finally catching up to the cardiology data for catheter therapy
40 Aspiration Pneumonia is common after stroke due to a variety of issues Decreased Level of Consciousness Weakness of oral and pharyngeal musculature Weak cough All stroke patients need to have dysphagia screen performed before POs given and have the swallowing function monitored. If any doubt have patient made NPO until seen by speech therapy
41 Why even get an MRI I know my patient has a Stroke MRI can help clarify if symptoms are from a stroke or one of the mimics Localization to know which vascular territory (the 60% carotid stenosis is asymptomatic if stroke is in the occipital lobe unless patient has a fetal PCA) Size and location of infract can help determine etiology- lacunar stroke from microvascular disease or bilateral embolic stroke from aorta or heart Size and location can help determine prognosis and other associated symptoms: memory problems from hippocampal damage or executive problems from frontal or parietal lobe
42 CT most commonly and easily available tool. However, it is associated with radiation exposure. In addition early strokes, small strokes and posterior fossa strokes can be missed MRI(without contrast) is best study as it can show almost all ischemic strokes (small brain stem strokes can still be missed). MRI also visualizing intracranial vessels by viewing the normal flow voids Acute Strokes less then 14 days usually show as areas of restricted diffusion on Diffusion weighted Imaging sequence (DWI) and ADC map


43
44 Can help detect patient with internal carotid narrowing >50% that might benefit from carotid endarterectomy Can be useful in finding dissection which is usually treated with anticoagulation Aortic dissection and hematomas can present with stroke as first symptoms Rare disorders like fibromuscular dysplasia and moyamoya, cerebral vasospasm might be detected by vascular imaging
45 Usually dramatic presentations-not the stroke patients try to sleep off High NIH Stroke scale (greater then 10) If not recognized and treated 80% of patients can not live independently Left MCA -Global aphasia, Right sided hemiplegia Right MCA-Neglect, gaze deviation left hemiplegia Basilar-Cranial nerve findings, ataxia, obtundation
46 Right hemiplegia Global Aphasia Right hemianopia Left gaze Preference Right hemianopia No response to pain on right
47 No Aphasia but some dysarthria Left hemiplegia Profound Right gaze preference Profound Neglect (frequently will deny any problems) I m OK despite severe neurological deficits No response to pain on left

48


49 DENSE MCA SIGN COMPLETED INFARCT
50 One basilar artery formed by confluence of the two vertebral arteries Common symptoms include Bilateral weakness and sensory loss Crossed finding (Cranial nerve on one side, weakness or sensory loss on contralateral side) Diplopia and vision loss (hemianopia, cortical blindness) Ataxia Severe dysarthria but not aphasia Lethargy with progression to coma and posturing Symptoms can progress over days and if left untreated is 99% fatal

51

52
53 Sudden onset of hemiplegia is rarely missed by many stroke cause no focal weakness Wallenberg or lateral medullary infarct-sudden onset of dysphagia Wernicke aphasia-sudden onset of receptive aphasia with fluent speech Cerebellar hemispheric strokes-sudden onset of vertigo nausea and vomiting
54 Adolf Wallenberg German neurologist described in early 20 th century this common brain stem stroke syndrome No weakness but has the following: Ipsilateral facial numbness(cn V) Ipsilateral ataxia, nystagmus and vertigo (cerebellar tracts and vestibular nuclei) Ipsilateral paralyzed palate (CN X ) Contralateral decreased pain and temperature but intact light touch vibration (spinothalamic track) Hiccups (medullary hiccup center), Horner's (descending symphatic fibers) Frequently missed as thought to be GI, however, sudden onset as well as Horner's, facial numbness and loss of pain and temperature key findings Dysphagia can be debilitating and almost half require G tube


55 Infarction of lateral medulla in distribution of Posterior Inferior Cerebellar Artery (PICA) Frequently associated with vertebral artery disease
56 Usually present with sudden onset of vertigo, intractable nausea and ataxia Ataxia might be subtle but can usually be picked up by gait exam, dysmetria with finger to nose and finger chase. Would have low threshold for MRI in patient with sudden vertigo, nausea and intractable vomiting
57 Wernicke aphasia, fluent aphasia, receptive aphasia-usually parietal temporal lobe region mostly embolic in nature No weakness but has impaired comprehension and fluent but frequently paraphasic speech(semantic errors, neologisms Carefully examination might show a hemi or quandratopsia Frequently misdiagnosed as confused or psychotic Key features are that the symptoms occurred suddenly and patient can follow non verbal commands (pantomime) with good attention
58 A problem of language not of cognition In isolation is a frequently missed stroke symptom Often patients are labeled confused or psychiatric diagnosis considered Need to determine if difficulty with speech is from dysarthria, confusion or a true language problem

59
60 Also know as Wernicke, Sensory, fluent or posterior aphasia Presents with fluent speech but nonsensical. Occasional stock phrases can be clear (yes, no thank you, profanity) Does not follow verbal commands but can follow nonverbal communications (gestures) Need to check visual fields as can be associated with hemianopia or quandratopsia given proximity to optic radiations

61
62 Also know as Broca, Motor, anterior or nonfluent aphasia Presents with decreased spontaneous speech and intact comprehension May be able to repeat (transcortical motor aphasia) typically patients are not able to write May be associated with facial droop or tongue deviation given proximity to motor strip Slow stuttering speech is almost never due to ischemic stroke

63


64 Hypertension is the largest modifiable stroke risk factor Hyperlipidemia should be treated Diabetes is major stroke risk factor Untreated sleep apnea should also be treated Antiplatelet should be given to decrease risk for ischemic stroke and treat comorbid cardiac conditions
65 Up to 20% of patient without a clear cause of stroke(cryptogenic) are believed to have occult afib Detection of atrial fibrillation in a patient with stroke markedly change management Paroxysmal atrial fibrillation can be difficult to detect and average length of cardiac monitoring for detection of atrial fibrillation is 4 months
 In patient with large vessel")
66 The largest modifiable stroke risk factor All patient with ischemic stroke should be treated for uncontrolled hypertension ACE inhibitors and ARB with diuretics are usually first line therapy Permissive hypertension up to 220/120 is allowed for the first several days to allow perfusion of viable tissue at risk for infraction (ie, Penumbra of the stroke) In patient with large vessel occlusion (carotid, vertebral) might benefit from longer period of HTN

 might warrant prophylactic hemi-craniectomy to prevent further damage and life threating")
67 Cytotoxic edema from cell death can cause significant mass effect and damage normal brain tissue by herniation and secondary ischemia in large ischemic strokes Usually peaks at 3-5 days after an ischemic stroke Cytotoxic edema does not respond to corticosteroids but may respond to osmotic agents (mannitol and 3% saline)-would avoid hypotonic fluids(d5 1/2NS) Large middle cerebral artery infarcts in young patient or posterior fossa strokes (cerebellum) might warrant prophylactic hemi-craniectomy to prevent further damage and life threating herniation


68
69 DVT Seizures Pneumonia Spasticity-usually develops several months after damage to corticospinal tract Can be treated with baclofen, tizandine, splinting, ROM and Botox. Thalamic pain syndrome-painful parasthesia that develop after damage to thalamus-treated with neuropathic pain meds (TCA, gabapentin, etc.)
70 Discharged on Antithrombotic VTE Prophylaxis Stroke Education Discharged on lipid lowering Medication if LDL greater then 100 Ischemic Stroke-Assessed for Rehabilitation Patients with afib discharged on anticoagulant Patient who present within 2 hours evaluated for Thrombolysis Door to needle time less than 60 minutes Dysphagia screen done before any POs given (including ASA) NIH stroke scale done in first 24 hours
71 USES Standardized scoring system for patients with ischemic stroke Good interrater reliability All patient will have NIH stroke scale on admission and during hospitalization Allows objective determination of severity of stroke Points given for weakness, aphasia, ataxia, neglect, cognition, vision, sensory changes etc MORE POINTS LARGER DEFICITS 0= no stroke 1-4= minor stroke 5-15= moderate stroke 15-20= moderate/severe stroke 21-42= severe stroke Training available from American Heart Association
72 Patients with aneurysmal subarachnoid hemorrhage (patients do better when treated at aneurysm center) Patients with significant intraventricular hemorrhage Patients needing intra-arterial therapy Patients that might need decompressive craniectomy -patients with large posterior fossa stroke (cerebellum) or large MCA strokes in younger patients
73 Evaulate patient and obtain time last seen well (not when the symptoms where discovered) Order labs(cbc, Chem, PT, PTT, CBG, and non contrast head CT, page rad tech) Contact neurology via dedicated stroke pager Review TPA contraindication and CT + labs Consider CTA head and neck for large strokes
74 All patients with acute ischemic stroke should be evaluated for TPA if presents within 4.5 hours Patients with clinical suspicion for large vessel occlusion should be evaluated for IA therapy Patients should be screened for causes of stroke, receive education and secondary prevention (Hypertension, Hyperlipidemia, DM, Afib etc) Appropriate rehab and follow up needed
75
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
TIA Transient Ischaemic Attack?
 TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
TIA Transient Ischaemic Attack? OR Transient loss of function (TLOF) Tal Anjum Consultant Stroke Physician, Morriston Hospital Training & education lead, WASP (Welsh Association of Stroke Physicians) Qs.
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology
 Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Definition of Stroke. Non modifiable Risk Factors. Modifiable Risk Factors. Modifiable Risk Factors cont.. STROKE Rehabilitation 3/28/2013
 Definition of Stroke STROKE Rehabilitation Sudden focal neurological deficit secondary to occlusion or rupture of blood vessels supplying the brain. TIA (transient ischemic attack)= stroke symptoms that
Definition of Stroke STROKE Rehabilitation Sudden focal neurological deficit secondary to occlusion or rupture of blood vessels supplying the brain. TIA (transient ischemic attack)= stroke symptoms that
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Disorders of language and speech. Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology
 Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al.
 ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
11/2/2016. Stroke. Carl F. McComas, M.D. November 3, Disclosures. None (of any kind)
") Stroke Carl F. McComas, M.D. November 3, 2016 None (of any kind) Disclosures 1 HYPERTENSION Stroke The seat of apoplexy seems to be within the same portion of the of the brain.... Both affects, the imagination,
Stroke Carl F. McComas, M.D. November 3, 2016 None (of any kind) Disclosures 1 HYPERTENSION Stroke The seat of apoplexy seems to be within the same portion of the of the brain.... Both affects, the imagination,
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning