IDPH EMS Region Five. Stroke Education
|
|
|
- Joleen Harvey
- 5 years ago
- Views:
Transcription


1 IDPH EMS Region Five Stroke Education

2 Time is Brain!!!!!

3 Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed. Strokes should be treated emergently. During a stroke, up to 2 million brain cells die every minute. For every hour a stroke continues, up to 200 million nerve cells die and the brain ages 4 years. Intravenous tpa (Activase / alteplase) should be given within 180 minutes of the onset of ischemic stroke, so do not delay transport and minimize scene time. It is recommended to limit scene time to 10 minutes. TIME IS BRAIN!
4 Cerebrovascular Accident (CVA) Pathophysiology Thrombosis (brain itself) Embolus (head, neck or heart) Hemorrhage (within brain) Ischemia (systemic blood flow)
5 Predisposing Factors: Modifiable Hypertension Cigarette smoking Diabetes Mellitus Heart disease Hyperlipidemia Cardiovascular disease Chronic atrial fibrillation Sickle cell disease Polycythemia Hypercoagulability Birth control pill use Cocaine use

6 Predisposing Factors: Unmodifiable Age Gender Race Prior stroke Heredity
7 CVA Mechanisms


8 CVA Origin Thrombus Embolus Aneurysm Arrhythmia Hypovolemia
9 Ischemic Stroke Blood vessel occlusion Thrombosis Embolism Plaque fragments from carotids Chronic atrial fibrillation Fat particles IV substance abuse particulates Systemic hypoperfusion Pump failure Hypovolemia
10 Ischemic Stroke Syndromes Transient Ischemic Attack (TIA) Neurological deficits that resolve in 24 hours or less (most in 30 minutes) Commonly result from carotid artery disease Same symptoms as CVA Often warning sign of impeding CVA 5% risk of stroke per year
11 Ischemic Stroke Syndromes Dominant Hemisphere Infarction Contralateral weakness, numbness Contralateral blurring of vision of half the visual field in both eyes Difficulty pronouncing words (dysarthria) Difficulty speaking or understanding speech (dysphasia or aphasia)
12 Ischemic Stroke Syndromes Nondominant Hemisphere Infarction Contralateral weakness, numbness Contralateral visual field cut Neglect of contralateral extremities Dysarthria Usually NOT dysphasic or aphasic

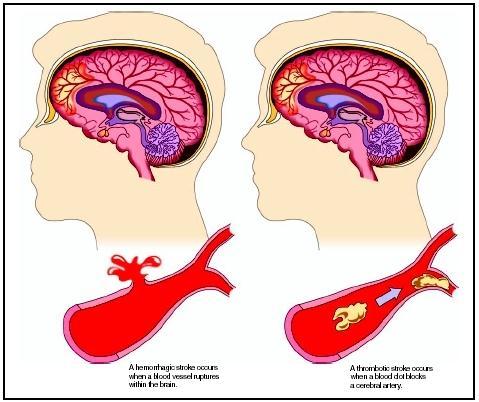
13 Hemorrhagic Stroke
14 Hemorrhagic Stroke Syndromes Intracerebral Hemorrhage Headache, nausea, vomiting precede deficits Patients commonly have decreased LOC with extreme hypertension Contralateral hemiplegia, hemianesthesia Possible aphasia, extremity neglect depending on hemisphere involved
15 Grade I Grade II Grade III Hemorrhagic Stroke Syndromes Subarachnoid Hemorrhage Asymptomatic or mild headache and mild nuchal rigidity Moderate to severe headache, nuchal rigidity, cranial nerve dysfunction but no other deficits Drowsiness, confusion, mild focal deficits Grade IV Grade V Stupor, moderate to severe hemiparesis, possibly early decerebrate rigidity, vegetative response Deep coma, decerebrate rigidity, moribund appearance
16 CVA Presentation Brain can show injury in only three ways: Decreased LOC Seizures Localizing signs Hemiparesis or hemiplegia Dysphasia (Receptive or expressive) Visual disturbances Gait disturbances Inappropriate affect Bizarre behavior Incontinence
. One new onset positive sign on the CSS indicates a 72% probability of stroke.")
17 Cincinnati Stroke Scale To facilitate accuracy in diagnosing stroke and to expedite transport, a rapid neurological examination tool is recommended. The most common prehospital exam used is the Cincinnati Stroke Scale (CSS). One new onset positive sign on the CSS indicates a 72% probability of stroke. Three new onset positive signs on the CSS indicates a greater than 85% probability of stroke.

18

19 Cincinnati Stroke Scale: Facial Droop (ask the patient to show their teeth or smile) Normal Both sides of the face move equally/symmetrically. Abnormal One side of the face does not move as well as the other.
. Normal Both arms move the same. Abnormal One arm turns over, drifts down compared to the other arm, or is flaccid.")
20 Cincinnati Stroke Scale: Arm Drift (ask the patient to close their eyes and hold both arms out straight with palms up for 10 seconds). Normal Both arms move the same. Abnormal One arm turns over, drifts down compared to the other arm, or is flaccid.

21 Cincinnati Stroke Scale: Speech (ask the patient to say, You can t teach an old dog new tricks ) Normal The patient says the phrase correctly with no slurring/slowing of words. Abnormal The patient slurs words, uses the wrong words or is unable to speak.

22 Cincinnati Stroke Scale: Time (ask the patient/witness when the symptoms started) Time of Onset: the time symptoms actually begin. Last Known Well Time: the last time the patient was known to be without symptoms (asymptomatic).

23 CRITICAL THINKING ELEMENTS: CRITICAL THINKING ELEMENTS: EMS personnel should ask family members or bystanders the stroke symptom onset time if the patient is unable to provide that information. Consider transporting a witness or obtaining witness contact information. Maintain the head/neck in neutral alignment. Elevate the head of the cot 30 degrees if the systolic BP is >100mmHg (this will facilitate venous drainage and help reduce ICP). Be alert for airway problems (swallowing difficulty, vomiting/aspiration) Bradycardia may be present in a suspected stroke patient due to increased ICP. DO NOT give Atropine if the patient s BP is normal or elevated. Spinal immobilization should be provided if the patient sustained a fall or other trauma. Monitor and maintain the patient s airway. 87% of strokes are ischemic and should be considered for tpa, while 13% of strokes are hemorrhagic.
24 Assessment Signs & Symptoms Ischemic S&S usually of slower onset Hemiparesis or hemiplegia Numbness or decreased sensation of face or unilateral Altered LOC or coma Convulsions Visual disturbances Slurred or inappropriate speech Headache or dizziness

25 Assessment Signs & Symptoms Cerebral Embolus with rapid onset Emboli from valvular HD or Afib rapid onset Often with an identifiable cause (e.g. Afib, Valvular heart disease, recent long bone fracture)
26 Assessment Signs & Symptoms Cerebral hemorrhage associated with rapid onset high mortality rate Often with severe HA ( Worst headache ever ) N/V Rapid decrease in LOC or seizure Coma, Cushing s and Herniation
27 Assessment Past Medical History Associated Altered LOC or Seizure? Onset/Precipitating factors? Initial symptoms and progression? Dizziness, Severe HA, N/V Previous CVA or TIA? Previous neurological deficits? Concomitant illnesses? Sickle Cell Disease Atrial fibrillation Risk factors for stroke & thrombus formation? BCP, Smoking HTN, CVD
28 Assessment Physical Exam Mental Status & Behavior Extremity Motor & Sensory Gait Pupils & Vision Cincinnati Prehospital Stroke Scale Evidence of Cushing s Syndrome (Reflex)or Herniation Blood glucose level
29 CVA Management Basic Objective Improve cerebral blood flow and oxygenation
30 Airway CVA Management If no gag reflex, intubate Otherwise, position to ensure drainage of secretions Suction as needed Breathing Oxygen via NRB Ventilate with BVM and O 2 if rate or tidal volume inadequate
31 CVA Management Circulation Check blood glucose level Hypoglycemia may mimic CVA Treat hypoglycemia with D50W Establish IV Access Draw blood samples TKO avoid solutions with glucose (Hypertonic) Monitor ECG 10% of CVAs are associated with cardiac event 12 Lead ECG if suspected ischemia
32 CVA Management Do not assume patient cannot understand because they cannot talk Position appropriately: If hypertensive, semireclined (head slightly elevated) If normotensive, on affected side If hypotensive, supine
33 CVA Management Increased Blood pressure treated ONLY if strongly suggestive of ischemic stroke If systolic >220 or diastolic >120 consider gradual blood pressure reduction Labetalol Nitropaste Nitroprusside Controlled reduction Return to pre-cva levels, NOT to normal
34 CVA Management Thrombolytic agents Consider for all patients with ischemic CVA presenting within 3 hours of onset Early recognition of ischemic stroke and administration of thrombolytics can prevent/limit loss of neurologic function Requires CT scan!!!
35 CVA Management Think like AMI of the Brain Time is Muscle.. Time is Brain Therapy Mainstays Oxygenation/Ventilation IV Access Rapid assessment & differential Treat associated conditions (hypoglycemia, hypoxia, hypotension) Rapid Transport to appropriate facility CT Scan & Thrombolytics vs. CT Scan & Neurosurgery
 a hospital that is")
 or")
 as")
36 Definitions Primary Stroke Center (PSC) a hospital that is currently certified by The Joint Commission (TJC) or Healthcare Facilities Accreditation Program (HFAP) as a Primary Stroke Center.

37 Definitions Emergent Stroke Ready Hospital (ESRH) a hospital which provides emergency care with a commitment to Stroke with recognition by Illinois Department of Public Health that has the following capabilities: CT availability with in-house technician availability 24/7/365 Lab availability 24/7/365 Ability to rapidly evaluate an acute stroke patient to identify patients who would benefit from thrombolytic administration Ability and willingness to administer thrombolytic agents to eligible acute Stroke patients Accepts all patients regardless of bed availability

38 Definitions Non-Stroke Hospital No recognized organized treatment for acute stroke.

 and head positioned midline.")
39 INTERHOSPITAL TRANSPORT GUIDELINES FOR CONFIRMED STROKE PATIENTS TPA (Activase / alteplase) Transfers Patients with a tpa infusion in progress must be accompanied by a Registered Nurse. Patients that have completed a tpa infusion must be transported by an ILS/ALS ambulance. It is preferred to complete tpa before transferring patient. Hemorrhagic Transfers Keep head of cot elevated at least 30 degrees (if stable) and head positioned midline. Vital Signs and Neuro checks every 15 minutes Notify Medical Control immediately of SBP > 180 mmhg DBP > 105 mmhg Deterioration in level of consciousness Bleeding at any location Severe headache

40 Time is Brain!!!!!!!
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
CBT/OTEP 442 Stroke. Seattle-King County EMS. Print version of EMS Online Course
 Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4693 January 2009 (rev. 4/1/09)
Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4693 January 2009 (rev. 4/1/09)
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Chapter 15. Neurologic Emergencies
 Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
Chapter 15 Neurologic Emergencies Introduction (1 of 4) Stroke is the third leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More men than
EMS Stroke Care in the Fox Valley
 EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Memorandum. Peoria Area EMS System Agencies & Providers. From: Peoria Area EMS System Office. Date: February 24, 2016
 Memorandum To: Peoria Area EMS System Agencies & Providers From: Peoria Area EMS System Office Date: February 24, 2016 Re: Glucagon Administration for BLS Agencies As discussed at the EMS Quarterly Update,
Memorandum To: Peoria Area EMS System Agencies & Providers From: Peoria Area EMS System Office Date: February 24, 2016 Re: Glucagon Administration for BLS Agencies As discussed at the EMS Quarterly Update,
Neurological Emergencies. Aaron J. Katz, AEMT-P, CIC
 Neurological Emergencies Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 1 Stroke ( CVA ) CerebroVascular Accident Brain Attack Brain damage caused by a blockage of blood to a specific area of the brain
Neurological Emergencies Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 1 Stroke ( CVA ) CerebroVascular Accident Brain Attack Brain damage caused by a blockage of blood to a specific area of the brain
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Chapter 18. Objectives. Objectives 01/09/2013. Altered Mental Status, Stroke, and Headache
 Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital
 Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital Objectives Describe the A & P of the nervous system Outline pathophysiological changes in the nervous system that may alter
Stroke: Every Minute Counts! Primary Stroke Center, Ingalls Memorial Hospital Objectives Describe the A & P of the nervous system Outline pathophysiological changes in the nervous system that may alter
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Most hypertensive: headache, vomiting, seizures, changes in mental status, fever, changes EKG
 Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Wk 2. Management of Clients with Stroke 1. Stroke neurologic changes by interruption in blood supply to brain 1) Etiology Ischemia: thrombosis or embolism thrombotic strokes > embolic strokes (1) Thrombosis
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
STROKE TRAINING FOR EMS PROFESSIONALS
 1 STROKE TRAINING FOR EMS PROFESSIONALS COURSE OBJECTIVES About Stroke Stroke Policy Recommendations Stroke Protocols and Stroke Hospital Care Stroke Assessment Tools Pre-Notification Stroke Treatment
1 STROKE TRAINING FOR EMS PROFESSIONALS COURSE OBJECTIVES About Stroke Stroke Policy Recommendations Stroke Protocols and Stroke Hospital Care Stroke Assessment Tools Pre-Notification Stroke Treatment
Various Stroke and Symptoms and Causes
 Various Stroke and Symptoms and Causes ShinJung Park Daegu Dongho high School, Korea G12 [Abstract] Stroke is one of the most common leading causes of death. In America, it is the 5 th leading cause of
Various Stroke and Symptoms and Causes ShinJung Park Daegu Dongho high School, Korea G12 [Abstract] Stroke is one of the most common leading causes of death. In America, it is the 5 th leading cause of
Medical Emergencies. Emergency Medical Response
 Medical Emergencies Lesson 23: Medical Emergencies You Are the Emergency Medical Responder You are the emergency medical responder (EMR) responding to a scene on a downtown street involving a male who
Medical Emergencies Lesson 23: Medical Emergencies You Are the Emergency Medical Responder You are the emergency medical responder (EMR) responding to a scene on a downtown street involving a male who
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
STROKE INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
STROKE INTRODUCTION Stroke is the medical term for a specific type of neurological event that causes damage to the brain. There are two types of stroke, but both types of stroke cause the same type of
CBT442-EMT12-Neurologic Emergencies
 Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2012 CBT442-EMT12-Neurologic
Seattle-King County EMS Seattle-King County Emergency Medical Services Division Public Health - Seattle/King County 401 5 th Avenue, Suite 1200 Seattle, WA 98104 (206) 296-4863 January 2012 CBT442-EMT12-Neurologic
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Management Of Medical Emergencies
 Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
Management Of Medical Emergencies U.S. Aging Population 35 million people (12%) 65 years or older Number will increase by nearly 75% by year 2030 The number of people more than 85 years old will approach
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Pathophysiology. Central Nervous System (CNS) Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal
 Peripheral Nervous System (PNS) Consists of. Consists of brain/spinal") Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Neurological Emergencies Pathophysiology Central Nervous System (CNS) Consists of brain/spinal cord Peripheral Nervous System (PNS) Consists of everything else Afferent (sensory) Efferent (motor) Autonomic
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
E X P L A I N I N G STROKE
 EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
EXPLAINING STROKE Introduction Explaining Stroke is a practical step-by-step booklet that explains how a stroke happens, different types of stroke and how to prevent a stroke. Many people think a stroke
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
NORTH MISSISSIPPI MEDICAL CENTER MEDICAL CENTER. Stroke: Are you at risk? A guide to stroke risk factors & resources at ACUTE STROKE UNIT
 North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
North Mississippi Medical Center Acute Stroke Unit 830 South Gloster Street Tupelo, MS 38801 (662) 377-3000 or 1-800-THE DESK (1-800-843-3375) www.nmhs.net Stroke: Are you at risk? A guide to stroke risk
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Cardiovascular Diseases and Diabetes
 Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
REGIONAL STROKE TRIAGE PLAN
 REGIONAL STROKE TRIAGE PLAN Rappahannock EMS Council 435 Hunter Street Fredericksburg, VA 22401 Phone: (540) 373-0249 Fax: (540) 373-0249 E-mail: rems@vaems.org www.remscouncil.org Board of Directors Approved:
REGIONAL STROKE TRIAGE PLAN Rappahannock EMS Council 435 Hunter Street Fredericksburg, VA 22401 Phone: (540) 373-0249 Fax: (540) 373-0249 E-mail: rems@vaems.org www.remscouncil.org Board of Directors Approved:
It s Not All One Sided. James Smith, MD (Smitty)
") It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
It s Not All One Sided James Smith, MD (Smitty) Disclosures Chair, NE State EMS Board Medical Director, Emergency Services, GPH Medical Director, GPH LifeNet, NPFD, Maxwell, Tryon, Chase County, NP Rec
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Depress consciousness by destroying or encroaching upon the substance of the brain Examples: Brain tumor ( ) disease Intracranial Parasites Trauma
 disease Intracranial Parasites Trauma") 1 Chapter 29 Neurology 2 Pathophysiology CNS Disorders: Alterations in mental status in the sign of central nervous system disorder Alterations may range from a loss in the thought process to totally unconscious
1 Chapter 29 Neurology 2 Pathophysiology CNS Disorders: Alterations in mental status in the sign of central nervous system disorder Alterations may range from a loss in the thought process to totally unconscious
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke. Objectives: After you take this class, you will be able to:
 Stroke Objectives: After you take this class, you will be able to: 1. Describe the signs of a stroke and how a stroke happens. 2. Discuss stroke risk factors. 3. Detail the care and rehabilitation of a
Stroke Objectives: After you take this class, you will be able to: 1. Describe the signs of a stroke and how a stroke happens. 2. Discuss stroke risk factors. 3. Detail the care and rehabilitation of a
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
CEREBROVASCULAR ACCIDENT (CVA)
") Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP5-002 Approval Date: 12/01/2017 Effective Date: 12/01/2017 Revision Due Date: 12/01/2018 CEREBROVASCULAR ACCIDENT (CVA) PURPOSE
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Understanding Stroke
 MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
MINTO PREVENTION & REHABILITATION CENTRE CENTRE DE PREVENTION ET DE READAPTATION MINTO Understanding Stroke About This Kit Stroke is the fourth leading cause of death in Canada after heart disease and
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
11/2/2016. The Acute Phase of Cerebrovascular Accident. L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV
 The Acute Phase of Cerebrovascular Accident L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV 1 Faculty Disclosure Information 1. SPEAKER: L. Michael Peterson, D.O.
The Acute Phase of Cerebrovascular Accident L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV 1 Faculty Disclosure Information 1. SPEAKER: L. Michael Peterson, D.O.
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Strokes , The Patient Education Institute, Inc. hp Last reviewed: 11/11/2017 1
 Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
Strokes Introduction A stroke or a brain attack is a very serious condition that can result in death and significant disability. This disease is ranked as the third leading cause of death in the United
1 of :55
 1 of 7 30-05-2012 23:55 SECTIONS CHAPTERS Brain, Spinal Cord, and Nerve Disorders Stroke (CVA) An ischemic stroke is death of an area of brain tissue (cerebral infarction) resulting from an inadequate
1 of 7 30-05-2012 23:55 SECTIONS CHAPTERS Brain, Spinal Cord, and Nerve Disorders Stroke (CVA) An ischemic stroke is death of an area of brain tissue (cerebral infarction) resulting from an inadequate
It s All in Your Head: Neuro Assessment for Non- Neuro Folks
 It s All in Your Head: Neuro Assessment for Non- Neuro Folks Causes for Neuro Changes Stroke Head Injury Tumors Increased ICP Drugs Anoxia Altered Blood Glucose Toxins Alcohol Meningitis Poor Circulation
It s All in Your Head: Neuro Assessment for Non- Neuro Folks Causes for Neuro Changes Stroke Head Injury Tumors Increased ICP Drugs Anoxia Altered Blood Glucose Toxins Alcohol Meningitis Poor Circulation
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Your Risk for Stroke and How to Be Prepared
 Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
Your Risk for Stroke and How to Be Prepared TABLE OF CONTENTS 01 / 02 / 03 / 04 / 06 / 07 / 08 / 09 / 14 / Stroke Education Stroke: The No. 5 Cause Of Death In The U.S. Is Stroke Preventable? Stroke Risk
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy