Lesson. The most important aspect in the assessment of headache is a careful history
|
|
|
- Donna Richards
- 5 years ago
- Views:
Transcription
1 Lesson The most important aspect in the assessment of headache is a careful history

2 Investigation of? SAH
3 Summary A CT scan within 12 hours of presentation is 98% sensitive for SAH CSF >12 hours with spectrophotometric detection of bilirubin is 96% sensitive for a SAH. Visual analysis of CSF is not acceptable
4 CSF spectrophotometry Confirmed SAH evident by CT also had a confirmed bilirubin peak on spectrophotometry 100% of cases, 12 hours to two weeks 70% after 3weeks 40% after 4 weeks
5 CT scans positive for SAH 98% within 12 hours 95% within 24 hours 73% on day three
6 71 patients with thunderclap headache and negative CT and CSF examinations were followed up for a mean of 3.3 years. None of these patients had a subarachnoid haemorrhage during the follow up period Wijdicks EFM, Kerkhoff H, Van Gijn. Long term follow up of 71 patients with thunderclap headache mimicking subarachnoid hemorrhage. Lancet 1988;ii:68 70
7
8 1 67 year old nurse awoke two weeks prior with a constant right parietal headache unrelieved by simple analgesia -8/10 day1 Still continue in her work as a Nurse day Eased after 24 hours remained persistent Fluctuating severity from 2 to 6/10 with slight nausea Worse for bouncing on a trampoline and with other Valsalva manoeuvres.
9 Two days after onset she had developed a number of episodes which she thought she could smell gas, associated with feeling shaky and weak lasting for seconds Had hit her head two weeks prior running into a netball hoop. Associated with bilateral periorbital black eyes.
10 PH of 2monthly migraine with a visual aura for 30 minutes and subsequent global nonthrobbing headache with nausea. Effectively treated with Paracetamol. Current headache different to normal migraine headache. PH hypertension.
11 On examination, longstanding reduced hearing left ear. Air conduction greater than bone conduction. Weber referred to the left. Remaining examination normal.?diagnosis and what do you want to do
12 in rysm
13
14 Clinical Pointers Headache was new onset, different character to previous headache. Worse with Valsalva manoeuvre Associated symptoms - suggesting focal seizures. Headache was not apparently of sudden onset. It did not cause waking from sleep, but was consistent with intracranial mass.
15 2 A 36 year old Maori women complained of headache and dizziness while refereeing touch rugby but was still able to run on for a period before suddenly collapsing to the ground with a severe headache and loss of consciousness for about 5 minutes. There were episodes of body stiffening.
16 Repeated neurological examination over 3 days was normal though there were episodes of apparently severe headache associated with thrashing around during which she remained responsive.
17 What diagnosis/diagnoses would you consider important? What investigation(s) would you consider important?
18 Days 1-2 CT scan - normal CSF 800 RBC in the first bottle 194 RBC in the 3rd bottle. Xanthochromia -ve EEG - normal
19 Day 10 MRI 10 days after the ictus - normal Repeat CSF 10 days after the ictus 92 lymphocytes, 51 RBC. Protein 0.71 Normal CSF glucose.
20 Day 14 Patient collapsed with sudden headache with dysconjugate eye movements and developed a locked in state with the only means of communication being vertical eye movement. Horizontal VOR was absent; bilateral facial palsies, a depressed corneal reflex, quadraparesis and bilateral extensor plantars.
21 Because of her previously inflammatory CSF she was treated for meningitis though a repeat CSF was normal. The patient deteriorated with a depressed level of consciousness with a CT head scan showing acute hydrocephalus improving with an intraventricular drain.
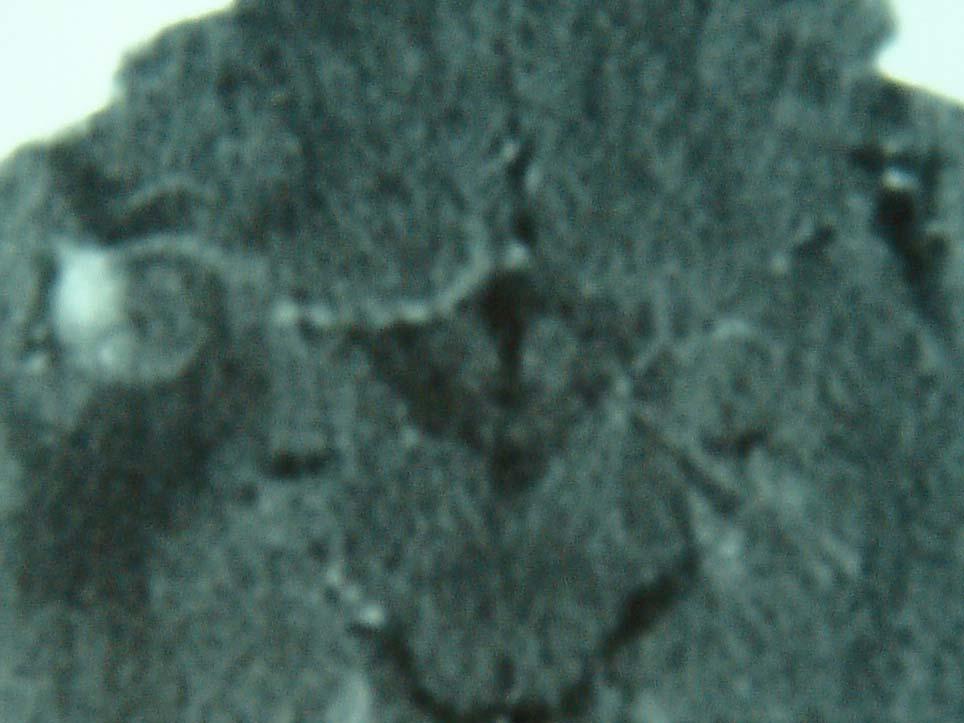
22 Repeat MRI showed an abnormal cerebellar hemisphere.

23 T2 MRI Infarct of Cerebellar Hemisphere
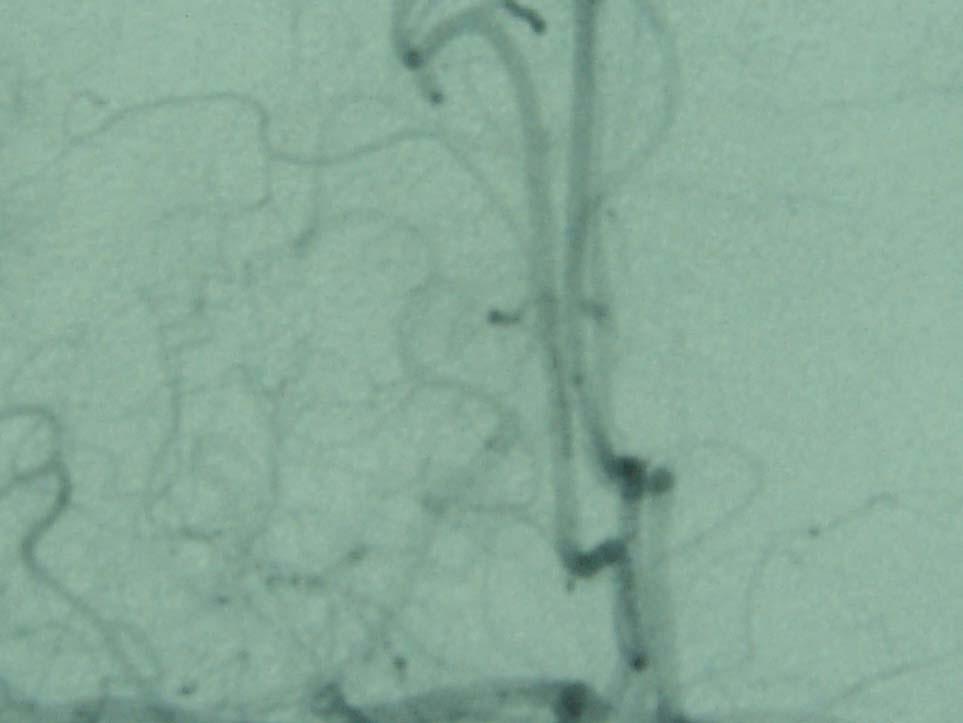
24 What investigation would you have liked to do on the day of her presentation?

25 Poorly filling basilar

26 Dissection of vertebral vessel wall
27 Lessons The essence is in the history An inflammatory CSF may represent infection inflammation malignancy blood Neck stiffness may be absent in up to 16% of known subarachnoid haemorrhages - even when examined by experts (J Edmeads 1995)
28 Dissection The mode of onset of headache is instantaneous and severe in about 13% of cases. Unless accompanied by stroke or SAH, CT and lumbar puncture may be unrevealing MR angiography is fast becoming the imaging modality of choice in demonstrating the arterial dissection
29 A 24 year old woman has the sudden onset of a severe hemicranial headache while sitting on a bus. The headache reached its maximal intensity at onset and persisted as a constant headache for the next 2 weeks. There was associated dizziness and intermittent vomiting occurring every second day? 3
30 Neurological examination was normal. What is your differential diagnosis Does the history warrant any investigations?
31 Head CT scan was normal. A CSF performed to look for xanthochromia from a possiible subarachnoid bleed showed 200 WBC, predominantly lymphocytes with a mildly raised protein and a normal glucose. Xanthochromia -ve
32 An EEG was abnormal with bilateral increase in slow wave activity. The patient was well and to try and seek further information as to the cause of her clinical condition an MRI with Gadolinium was performed. This was normal.
33 The patient had an episode of dysphasia on the 2nd hospital day? Want to do
34 The patient was treated for herpes simplex encephalitis and for TB. Three days later a polymerase chain reaction for HSV encephalitis was positive. TB treatment was discontinued
35
36 4 A 22 year old pregnant woman at 25 weeks gestation developed throbbing occipital headaches with exacebation by postural change. What is your diagnosis?
37 Two days later she was diagnosed as having an intrauterine death. Half an hour following this diagnosis, one hand went out in front of her and there was shaking of the fingers with heavy breathing. She bit her tongue.
38 A few days later a generalised seizure occurred Subsequent episodes of generalised limb shaking, of a different character to the initial event, were associated with preserved consciousness
39 On day 10 the patient complained of difficulty moving her left hand side. Her blood pressure had been elevated post delivery to levels of 180/120 requiring a Nitroprusside drip in coronary care.
40 O/E mixture of functional and organic signs. Swollen optic discs Left leg pyramidal signs
41 What is the diagnosis now?
42 Puerperal sagittal sinus thrombosis
43 What investigation is needed to confirm this?
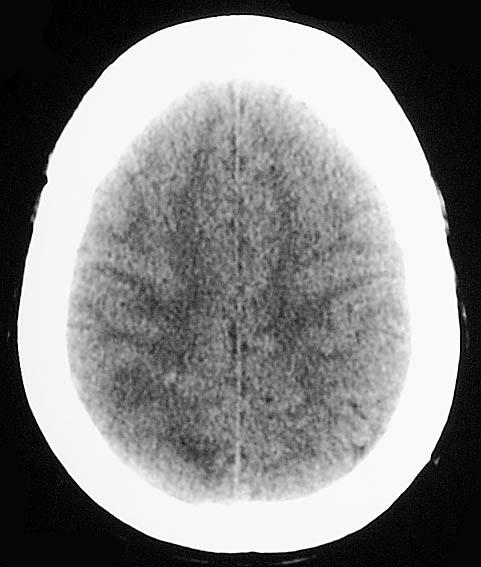
44 Normal CT

45 Filling defect

46 Absent venous filling
47 CT may be normal. MRI / MRA is the investigation of choice. MRI may be normal < 5 days or > 30 days and an angiogram may be needed Repeat MRI at 3 months to ensure that the CVT has resolved as in some patients the CVT may persist and could give a false diagnosis in subsequent pregnancies.
48 What treatment is indicated and why?
49 Rx Heparin in all cases - even if associated with venous haemorrhage. Thrombolysis not used by this group but advocated if Rx fails. Give low molecular weight heparin at time of further pregnancy to prevent recurrence. Anticonvulsants stopped after 6/12.
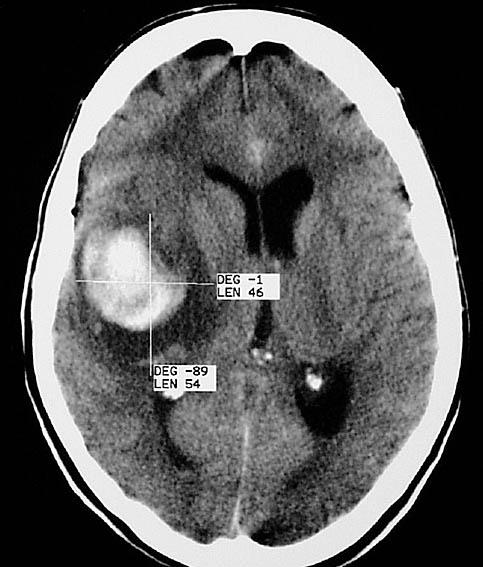
50 Differential pueperal related SST headache: Boussay France Can present with migraine with or without aura. Menstrual migraine may improve in pregnancy and often recurr post partum. Can be thunderclap with blood in CSF simulating an aneurysmal bleed (10%). May simulate low pressure post epidural headache with improvement on lying down. However, improvement is not as dramatic as occurs with true low pressure headache.
51 CVST The CSF pressure should always be measured as high intracranial pressure may be an important clue to the presence of CVST where about 25% of CT scans will be negative.
52 CSVT - onset is usually subacute over several days, Thunderclap headache may be the presenting feature in up to 10% CT is interpreted as normal in about 25% of patients with CVST.
53 Eclampsia can occur up to 2 wks post delivery and cause headaches and seizures. Pituitary necrosis may cause sudden severe headache and mimic SAH
54 5 53 year old woman, PH Bipolar Depression Sudden onset of headache with shooting pains to her shoulders and hips, lasting for 10 mins. Simultaneously hit by a grey light Subsequent vomiting O/E CNS NAD ECG sinus Bradycardia 38/min, Inverted T waves V2-V6 and 1st degree heart block
55 Day 2 dehydration 2nd to vomiting but complaining of headache and restless Patient concerned that she was unwell and attributed this to withdrawal from smoking and requested to see a social worker Day 3 febrile Day 4 Incontinent overnight Day 5 cognitive deterioration. L hand weakness
56 What investigation would you like to do?

57
58 CT scan Haemorraghic infarction of right temporal parietal region. CSF 54 WBC 74 RBC, Protein 0.56, glucose CSF/serum : 2.5/6.0
59 Neurologist did not find any neck stiffness Patient was confused with bilateral grasp reflexes with spasticity and bilateral upgoing plantars
60 What possible diagnoses would you consider in light of the CSF?
61 Considered - cortical venous sinus thrombosis, vasculitis with haemorraghic infarct Day 7 Positive sciatic nerve stretch test, spiking fevers, depressed level of consciousness. Day 15 Rapid deterioration.
62
63 Progressive cerebral oedema and death What abnormality do you expect to find at postmortem?
64 Ruptured berry aneurysm of the right middle cerebral artery, containing thrombus with extensive intracerebral and subarachnoid haemorraghe
65 An inflammatroy response can be seen in the CSF from subarachnoid blood. The presentation was complex with sidetracking symptoms but there was a history of sudden onset headache with radiation to the spine, consistent with subarachnoid bleeding. The history is the most important item. Without an accurate history and correct intepretation the direction of investigation is random and inappropriate.
66 An increased opening pressure may also help distinguish between a traumatic lumbar puncture and a subarachnoid haemorrhage. NB 20% of lumbar punctures are traumatic
67 Where the CSF or clinical findings are difficult to interpret or the index of suspicion is unusually high (family or personal history of subarachnoid haemorrhage), MRA is an appropriate procedure for detecting a saccular aneurysm in most patients.
68 Thunderclap headaches with normal neurological examinations can be the presenting feature of cerebral venous sinus thrombosis pituitary apoplexy, cervicocephalic arterial disection, acute hypertensive crisis -pheochromcytoma spontaneous intracranial hypotension orgasmic headache - may often evade detection by CT and lumbar puncture.
69
70 Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study BMJ 2011;343:d4277 doi: /bmj.d4277
71 100% sensitivity and specificity in 121 patients with SAH but criticisms: LPs only done in ½ Spectrophotometric analysis of CSF not done No strong evidence to demonstrate the superiority of xanthochromia by spectrophotometer versus visual detection of xanthochromia?? CT sensitivity drops too 85% after 8hrs AE physicians and radiology trainees misinterpreted scan in 4 subjects 2% of patients were lost to follow-up at six months.
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Neurology on the MAU. Geraint Fuller
 Neurology on the MAU Geraint Fuller Conflicts of Interest Clinical neurologist No drug company links Past President of Association of British Neurologists Co-Editor of Practical Neurology Receive Royalties
Neurology on the MAU Geraint Fuller Conflicts of Interest Clinical neurologist No drug company links Past President of Association of British Neurologists Co-Editor of Practical Neurology Receive Royalties
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Acute neurology. CME Acute Medicine. Headache. Intracranial haemorrhage
 Acute neurology Table 1. Causes to consider in emergency presentation of headache. Headache type Causes Susan E Tomlinson BMed FRACP(Australia), Clinical Research Fellow, Department of Molecular Neuroscience,
Acute neurology Table 1. Causes to consider in emergency presentation of headache. Headache type Causes Susan E Tomlinson BMed FRACP(Australia), Clinical Research Fellow, Department of Molecular Neuroscience,
Secondary Headaches: A Strategic Approach. Emerg Med 40(4):18, 2008
:18, 2008") Secondary Headaches: A Strategic Approach Emerg Med 40(4):18, 2008 Headaches are common complaints in the emergency department, but the causes of secondary headaches are often misdiagnosed. The authors
Secondary Headaches: A Strategic Approach Emerg Med 40(4):18, 2008 Headaches are common complaints in the emergency department, but the causes of secondary headaches are often misdiagnosed. The authors
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Pregnancy and Neurological Disorders
 Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Pregnancy and Neurological Disorders Myles Connor NHS Borders and University of Edinburgh, United Kingdom Outline Why is it important? Specific conditions Eclampsia Cerebrovascular disease Epilepsy Idiopathic
Stroke Mimics. Paul Guyler
 Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Stroke Mimics Paul Guyler Consultant Stroke Physician at Southend University Hospital Clinical Lead for Acute Stroke Essex Cardiac and Stroke Network Aims Why worry? Stroke Recognition Tools History, Examination
Pause for thought. Dr Jane Anderson Consultant Neurologist
 Pause for thought Dr Jane Anderson Consultant Neurologist Which is the top cause of years lived with disability worldwide? 1. COPD 2. Low Back pain 3. Diabetes 4. Migraine with medication overuse headache
Pause for thought Dr Jane Anderson Consultant Neurologist Which is the top cause of years lived with disability worldwide? 1. COPD 2. Low Back pain 3. Diabetes 4. Migraine with medication overuse headache
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Symptoms of a brain tumour in adults
 Symptoms of a brain tumour in adults A tumour is an abnormal growth caused by cells dividing in an uncontrolled manner. Approximately 9,300 people are diagnosed with a primary brain tumour each year. (Primary
Symptoms of a brain tumour in adults A tumour is an abnormal growth caused by cells dividing in an uncontrolled manner. Approximately 9,300 people are diagnosed with a primary brain tumour each year. (Primary
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Neurologic Examination
 John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
There are several types of epilepsy. Each of them have different causes, symptoms and treatment.
 1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
1 EPILEPSY Epilepsy is a group of neurological diseases where the nerve cell activity in the brain is disrupted, causing seizures of unusual sensations, behavior and sometimes loss of consciousness. Epileptic
Neuroimaging in Pregnancy
 Neuroimaging in Pregnancy January 18, 2014 Sarasota, FL Joshua P. Klein, M.D., Ph.D. Departments of Neurology and Radiology Brigham and Women s Hospital and Harvard Medical School American Society of Neuroimaging
Neuroimaging in Pregnancy January 18, 2014 Sarasota, FL Joshua P. Klein, M.D., Ph.D. Departments of Neurology and Radiology Brigham and Women s Hospital and Harvard Medical School American Society of Neuroimaging
Background. Background. Headache Examination. Headache History. Primary vs. Secondary Headaches. Headaches In Children: Why Worry?
 Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH. Matt Greer February 10 th, 2015
 TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Subarachnoid Hemorrhage as a Complication of Cerebral Venous Thrombosis
 Mitali Madhusmita et al CASE REPORT 10.5005/jp-journals-10036-1183 Subarachnoid Hemorrhage as a Complication of Cerebral Venous Thrombosis 1 Mitali Madhusmita, 2 Archana Bhate, 3 Anannya Mukherji ABSTRACT
Mitali Madhusmita et al CASE REPORT 10.5005/jp-journals-10036-1183 Subarachnoid Hemorrhage as a Complication of Cerebral Venous Thrombosis 1 Mitali Madhusmita, 2 Archana Bhate, 3 Anannya Mukherji ABSTRACT
Department of Radiology University of California San Diego. MR Angiography. Techniques & Applications. John R. Hesselink, M.D.
 Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Department of Radiology University of California San Diego MR Angiography Techniques & Applications John R. Hesselink, M.D. Vascular Imaging Arterial flow void Flow enhancement Gadolinium enhancement Vascular
Syncope and Seizure Questionnaire
 Syncope and Seizure Questionnaire World College of Neurology 2/79 Wheatley Drive Bull Creek WA 6149 T 08 93320488 F 08 93329988 Copyright 2011. All rights reserved. Patient Name: MAIN PROBLEM I am here
Syncope and Seizure Questionnaire World College of Neurology 2/79 Wheatley Drive Bull Creek WA 6149 T 08 93320488 F 08 93329988 Copyright 2011. All rights reserved. Patient Name: MAIN PROBLEM I am here
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
The Neurologic Examination. John W. Engstrom, M.D. University of California San Francisco School of Medicine
 The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Intracranial hypotension secondary to spinal CSF leak: diagnosis
 Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
Intracranial hypotension secondary to spinal CSF leak: diagnosis Spinal cerebrospinal fluid (CSF) leak is an important and underdiagnosed cause of new onset headache that is treatable. Cerebrospinal fluid
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
Evaluating an Apparent Unprovoked First Seizure in Adults
 Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
PREVALENCE BY HEADACHE TYPE
 CLINICAL CLUES AND CLINICAL RULES: PRIMARY VS SECONDARY HEADACHE * Based on a presentation by David W. Dodick, MD ABSTRACT Headache is a common condition, accounting for many specialist office visits annually.
CLINICAL CLUES AND CLINICAL RULES: PRIMARY VS SECONDARY HEADACHE * Based on a presentation by David W. Dodick, MD ABSTRACT Headache is a common condition, accounting for many specialist office visits annually.
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
PAEDIATRIC ACUTE CARE GUIDELINE. Headache. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level
 Residents: Pediatric residents at the PL1, PL2, PL3 level") Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level Prerequisites: Any prior pediatric rotations and experience Primary Goals for this
Subspecialty Rotation: Child Neurology at SUNY (KCHC and UHB) Residents: Pediatric residents at the PL1, PL2, PL3 level Prerequisites: Any prior pediatric rotations and experience Primary Goals for this
About one fifth of the patients seen by a general neurologist in the UK will present with
 Correspondence to: Dr Richard Davenport, Department of Clinical Neurosciences, Western General Hospital, Crewe Road, Edinburgh EH4 2XU, UK; rjd@skull.dcn.ed.ac.uk ACUTE HEADACHE IN THE EMERGENCY DEPARTMENT
Correspondence to: Dr Richard Davenport, Department of Clinical Neurosciences, Western General Hospital, Crewe Road, Edinburgh EH4 2XU, UK; rjd@skull.dcn.ed.ac.uk ACUTE HEADACHE IN THE EMERGENCY DEPARTMENT
Headache Syndrome. Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL
 Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage
 Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
e) None of the above e) None of the above
 None of the above e) None of the above") Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Analysis of Characteristics in Patients with Non-Hemorrhagic Reversible Cerebral Vasoconstriction syndrome NH-RCVS
 Analysis of Characteristics in Patients with Non-Hemorrhagic Reversible Cerebral Vasoconstriction syndrome NH-RCVS Owais Mufti, MBBS Aaron McMurtray, MD, PhD and Bijal K. Mehta, MD, MPH, MA Department
Analysis of Characteristics in Patients with Non-Hemorrhagic Reversible Cerebral Vasoconstriction syndrome NH-RCVS Owais Mufti, MBBS Aaron McMurtray, MD, PhD and Bijal K. Mehta, MD, MPH, MA Department
Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE
 Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE Jeffrey J. Perry, MD, MSc1; Ian G. Stiell, MD, MSc1; Marco L. A. Sivilotti, MD, MSc5,6; Michael J. Bullard, MD11; Corinne
Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE Jeffrey J. Perry, MD, MSc1; Ian G. Stiell, MD, MSc1; Marco L. A. Sivilotti, MD, MSc5,6; Michael J. Bullard, MD11; Corinne
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Stroke mimics. Case 1. Acute cases. History. 43 year old healthy male Shortly after awakening developed:
 Stroke mimics Acute cases Gothenburg 21. may 2007 History Case 1 43 year old healthy male Shortly after awakening developed: Left-sided lower facial weakness Left-sided arm paralysis and weakness in leg
Stroke mimics Acute cases Gothenburg 21. may 2007 History Case 1 43 year old healthy male Shortly after awakening developed: Left-sided lower facial weakness Left-sided arm paralysis and weakness in leg
Initial Patient Health Assessment Form
 Initial Patient Health Assessment Form General Information: Patient Name:, Date: / /20 Patient s Address:. City:, State:, Zip Code: Home Phone #: - -, Work Phone #: - -, Cell #: - - E-mail address:, Date
Initial Patient Health Assessment Form General Information: Patient Name:, Date: / /20 Patient s Address:. City:, State:, Zip Code: Home Phone #: - -, Work Phone #: - -, Cell #: - - E-mail address:, Date
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Section la. Migraine and other headache syndromes. Migraine. Other headache syndromes G44
 Section la Migraine and other headache syndromes Overview of categories dealing with migraine, other headache syndromes, and neuralgia of cranial nerves, in accordance with the ICD-NA, second edition G43
Section la Migraine and other headache syndromes Overview of categories dealing with migraine, other headache syndromes, and neuralgia of cranial nerves, in accordance with the ICD-NA, second edition G43
Neurology Topics. Ian Rosemergy
 Neurology Topics Ian Rosemergy Plan An unusual presentation of a not so unusual problem Some seizure cases 49 year old female Patient 1 Hit on back and neck by swinging car door o Severe neck and shoulder
Neurology Topics Ian Rosemergy Plan An unusual presentation of a not so unusual problem Some seizure cases 49 year old female Patient 1 Hit on back and neck by swinging car door o Severe neck and shoulder
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
Sinus and Cerebral Vein Thrombosis
 Sinus and Cerebral Vein Thrombosis A Summary Sinus and cerebral vein clots are uncommon. They can lead to severe headaches, confusion, and stroke-like symptoms. They may lead to bleeding into the surrounding
Sinus and Cerebral Vein Thrombosis A Summary Sinus and cerebral vein clots are uncommon. They can lead to severe headaches, confusion, and stroke-like symptoms. They may lead to bleeding into the surrounding
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Recommendations. for Care of Adults with Epilepsy. Seeking the best treatment from the right doctor at the right time!
 Recommendations for Care of Adults with Epilepsy Seeking the best treatment from the right doctor at the right time! Contents This booklet is to help adults and their caregivers know when it is appropriate
Recommendations for Care of Adults with Epilepsy Seeking the best treatment from the right doctor at the right time! Contents This booklet is to help adults and their caregivers know when it is appropriate
Advanced Concept of Nursing- II
 In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- VIII Advance Nursing Management Of neurovascular Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- VIII Advance Nursing Management Of neurovascular Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
Central nervous system
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Provider Led Entity. CDI Quality Institute PLE Headache AUC 09/04/2018
 Provider Led Entity CDI Quality Institute PLE Headache AUC 09/04/2018 Appropriateness of advanced imaging procedures* in patients with headache and the following clinical presentations: *including MRI
Provider Led Entity CDI Quality Institute PLE Headache AUC 09/04/2018 Appropriateness of advanced imaging procedures* in patients with headache and the following clinical presentations: *including MRI
Subarachnoid Haemorrhage and Thunderclap Headache. Tom Heaps Consultant Acute Physician
 Subarachnoid Haemorrhage and Thunderclap Headache Tom Heaps Consultant Acute Physician Lesson Outline Clinical Case Why is this topic important? Thunderclap Headache (TCH): definition SAH: diagnosis, management
Subarachnoid Haemorrhage and Thunderclap Headache Tom Heaps Consultant Acute Physician Lesson Outline Clinical Case Why is this topic important? Thunderclap Headache (TCH): definition SAH: diagnosis, management
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Unit #3: Dry Lab A. David A. Morton, Ph.D.
 Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
Cerebrovascular diseases-2
 Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Cerebrovascular diseases-2 Primary angiitis of CNS - Other causes of infarction i. Hypercoagulable states ii. Drug-abuse such as amphetamine, heroin and cocain Note - The venous side of the circulation
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Risk Management in an Office Setting: Who are we sending home?
 Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance