Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
|
|
|
- Barrie Lambert
- 5 years ago
- Views:
Transcription
1 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
2 Speaker Disclosures Funding Sources: The National Institute of Health/National Institute of Neurological Disorders and Stroke (K23-NS073806) University of Pittsburgh Foundation Grant Site PI for Newton II clinical trial (Edge Therapeutics Inc.)
3 A Familiar Story 46 woman, healthy except for high blood pressure and tobacco use. Suddenly collapses with a severe headache and shaking movements. She is intubated in the field by EMS and brought to the ED. Exam: obtunded, brain stem reflexes intact, grimaces only to deep sternal rub, minimal withdraw to noxious stimuli in limbs.




4 Another Familiar Story > 30,000 cases/year in the US alone. 25% mortality. 80% SAH occur in people ages Over 50% of these patient survive in long term severe disability.
5
6
7 What do we do now?
8 Overview of Talk Basics of Aneurysmal SAH Hyper-acute Management Delayed Vasospasm & Ischemic Injuries Systemic Complications
9 Typical Presentations Worse Headache of Life : 80% ~20% describe sentinel headache Often associated with nausea/vomiting, stiff neck, loss of consciousness, or focal neurological deficits. Seizures: 20% Can induce cardiac arrhythmia and patients can present in cardiac arrest. Mis-diagnosis rate ~12% from recent data. Mis-diagnosis is associated with 4-fold increase risk for death or severe disability at 1 year.
10 SAH Diagnosis Non-contrast head CT: % sensitivity in the first 12 hrs after SAH, decreasing to 93% at 24 hrs and 57-85% by 6 days post SAH. Diagnostic lumbar puncture should be performed in patients with negative CT and high clinical suspicion of SAH. CSF profile also changes at different time points after SAH: from abundant RBC to xanthrochromia, to bilirubin in CSF. Emerging MRI technology (GRE, susceptibility, FLAIR) improves sensitivity for SAH, especially delayed presentation.

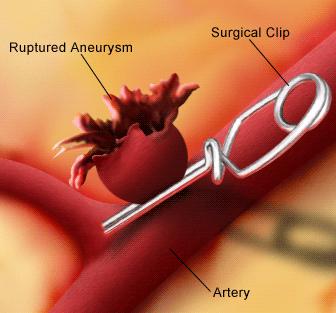
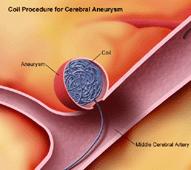
11 Aneurysm Basics


12 Typical Locations


13 Typical Locations
14 Basics of Aneurysmal SAH: Clinical Grades




15 Basics of Aneurysmal SAH: Radiologic Groups Fisher 1 No blood. Fisher 3 Localized clots, thickness >= 1mm. Fisher 2 Diffuse SAH, thickness < 1mm. Fisher 4 SAH with intraparenchymal or intraventricular clots.
16 Overview of Talk Basics of Aneurysmal SAH Hyper-acute Management Delayed Vasospasm & Ischemic Injuries Systemic Complications
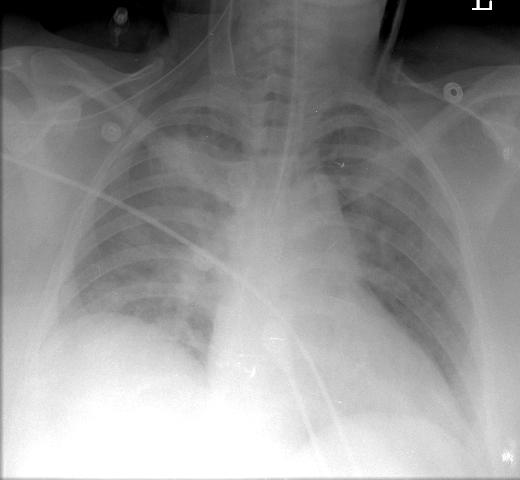
17 Hyper-acute Management: How Does SAH Kill? cardiac arrhythmia sudden ICP elevation Hydrocephalus Aneurysm re-rupture Voodoo heart Neurogenic pulmonary edema Delayed vasospasm and stroke
18 Hyper-acute Management 1: Treat Acute Hydrocephalus Hydrocephalus is a clinical diagnosis! Acute hydrocephalus is high on the differential for ALL SAH patients with impaired mental status. Casting of 4 th ventricle and/or cerebral aqueduct is high risk radiographic finding. Emergent external ventricular drain (EVD) placement SAVES LIVES. Many recommend keeping EVD clamped and only open it prn ICP > 20, before you the aneurysm is fixed.


19 EVD Temporal-horn dilatation Casting of cerebral aqueduct
20 Hyper-acute Management 2: Prevent Aneurysm Re-rupture Re-rupture is associated with 70% case-fatality rate. Re-rupture risk is maximal on day 1 post rupture (4%). Each additional day confers 1-2% bleeding risk in first 4 weeks post aneurysm rupture. Prevention methods (controversial) include: Strict BP control (SBP less than 140), bed rest, avoid overdraining CSF, and...




21 Hyper-acute Management 3: FIX THE ANEURYSM ASAP Pre-op aneurysm re-rupture rate: 0-3 days: 5.7% 4-6 days: 9.4% 7-10 days: 12.7% days: 13.9% days: 21.5% Kassell NF et al, J Neurosurg 1990; 73:18-36
22 Hyper-acute Management 3: International Subarachnoid Aneurysm Trial Clip vs. coil in anterior circulation aneurysms Cumulative mortality Cumulative re-bleeding risk Molyneux A et al, Lancet 2005; 366:809-17
23 Overview of Talk Basics of Aneurysmal SAH Hyper-acute Management Delayed Vasospasm & Ischemic Injuries Systemic Complications

 fever, cerebral salt wasting.")
24 Unique Time-line in SAH and Vasospasm DAY 0 => aneurysm rupture DAY 0-1 => fix aneurysm DAY 0-4 => patient improves DAY 5-6 => some patients develop neurological dysfunction DAY 7-14 => visible vasospasm (VSP) fever, cerebral salt wasting. DAY => VSP resolution
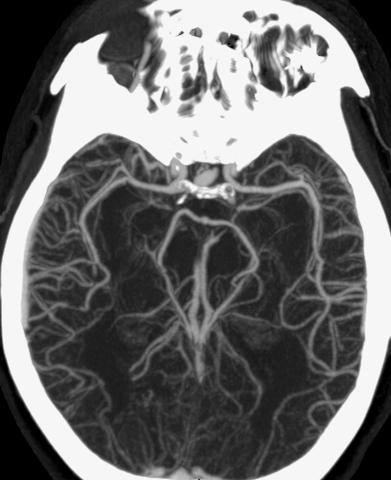
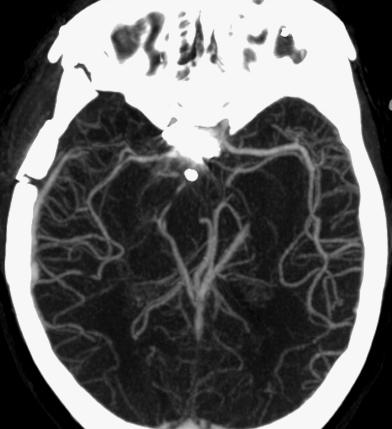
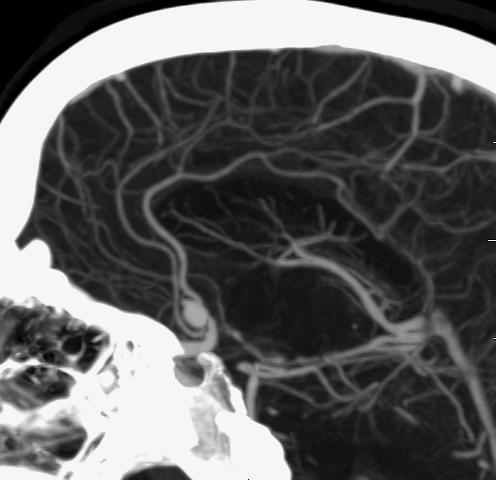
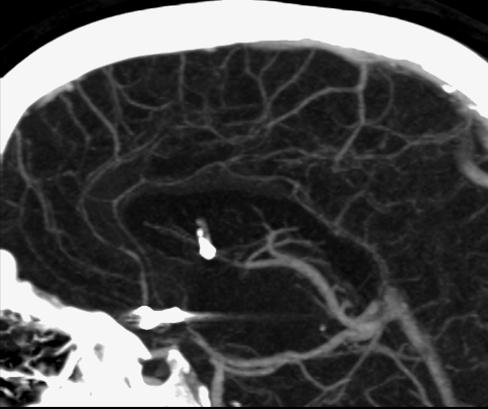
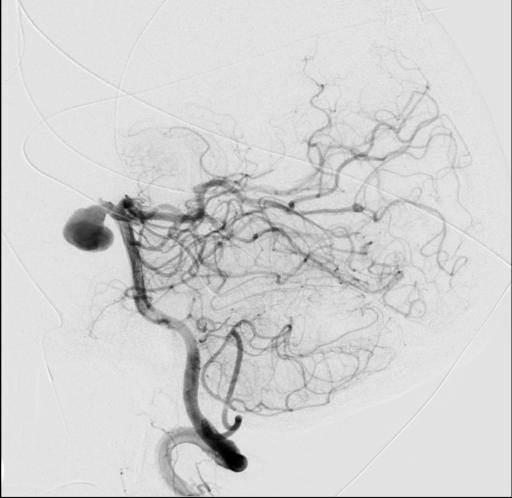
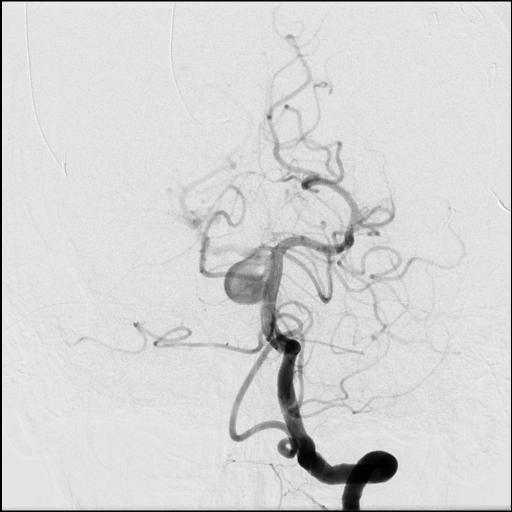
25 Angiographic Vasospasm Post SAH Day 0 Post SAH Day #7
26 Delayed Vasospasm: Impact 50% surviving SAH patients have angiographic VSP, and 32% have clinical, symptomatic VSP. Of those with symptomatic VSP, 15-20% suffer further stroke, severe disability, or die from VSP. 50% of SAH/VSP survivors suffer significant morbidity. Development of clinically symptomatic VSP requires urgent treatment. In this disease, excellent neurocritical care support changes outcome
27 Delayed Vasospasm: ICU Management Hypovolemia and hypotension are associated with poor outcome in SAH and should be avoided. Hemodynamic augmentation and induce hypertension may reverse neurologic deterioration in patients with symptomatic vasospasm. There is no evidence that prophylactic use of hemodynamic augmentation improves outcome.
28 Intra-arterial Therapy IA Vasodilator Injection: Treatment of choice in acute symptomatic VSP Ca channel antagonist: nicardipine, verapamil Phosphodiesterase III inhibitor: milrinone Often causes transient ICP elevation and hypotension May need repeat treatments for persistent vasospasm. Balloon angioplasty Durable effects compared with IA injection Only available for proximal segment VSP Rare but serious complication of artery rupture


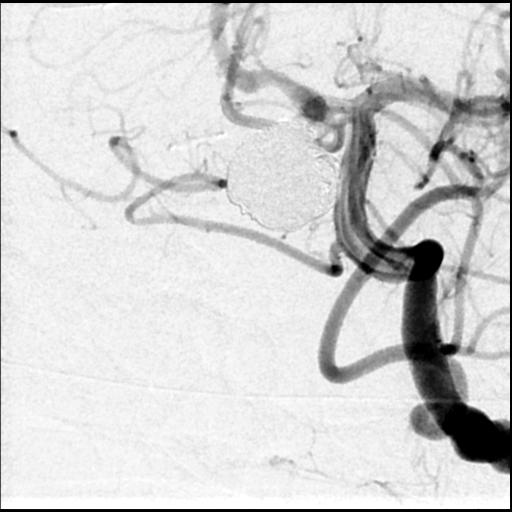
29 IA Vasodilator Injection Pre Post
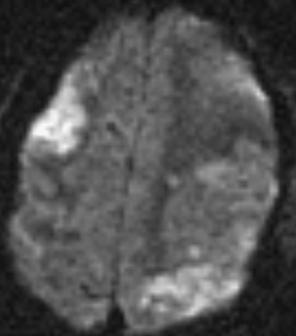
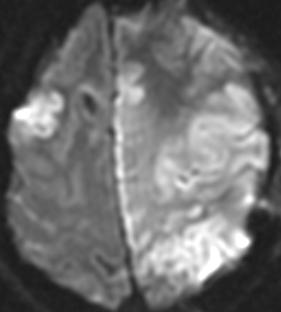
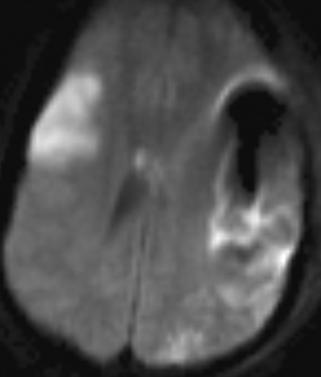
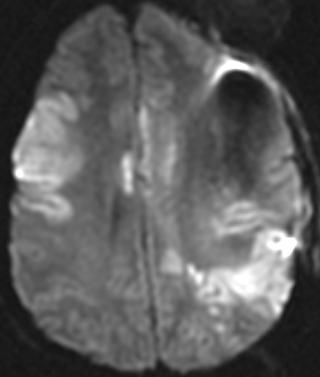
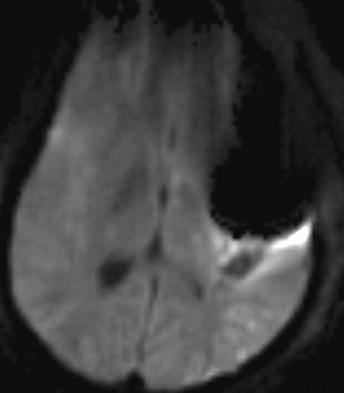
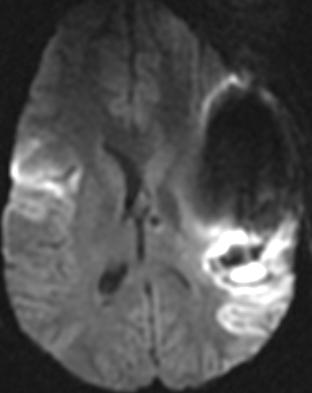
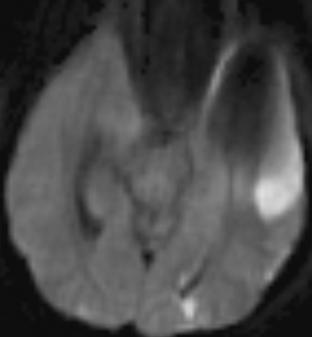
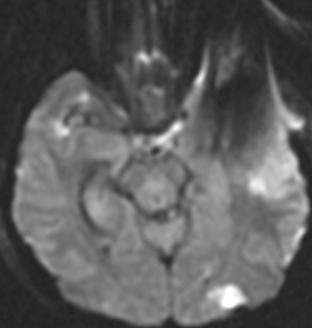
30 Delayed Vasospasm: Ischemic Infarcts Post SAH day 5 Post SAH day 8 Post SAH day 5 Post SAH day 8
31 Overview of Talk Basics of Aneurysmal SAH Hyper-acute Management Delayed Vasospasm & Ischemic Injuries Systemic Complications
32 Neurogenic Stunned Myocardium % SAH have ECG changes (QTc prolongation, repolarization abnormalities) not associated with poor outcome % SAH have cardiac troponin elevation. Troponin release is associated with poor clinical grade, cerebral edema, intraventricular blood. Approximately 20% of SAH patients develop LV systolic dysfunction, cardiogenic shock, & cardiogenic pulmonary edema. Cardiac dysfunction is usually reversible. Naidech A et al, Circulation 2005;112:



33 Broken Heart Syndrome? NSM, Takotsubo cardiomyopathy, & voodoo heart : There is confusion of terms in literature and practice. Pathology: subendocardial contraction band necrosis. Thought to result from excessive release of nor-epineprhine Typically not associated with coronary artery disease. Apical ballooning is often not seen in SAH patients with LV dysfunction and cardiogenic shock. Bybee KA et al, Ann Intern Med 2004; 141:
34 Cerebral Salt Wasting vs. SIADH Hyponatremia occurs in up to 30% patients. Difficult to distinguish between CSW and SIADH because we must maintain strict euvolemia at all times. Hypouricemia and increased FeUA more consistent with CSW. CSW in SAH is associated with elevated BNP. Fludrocortisone shown to be effective for hypona in SAH. Berendes E et al, Lancet 1997: 349: ; Wijdicks EFM et al, CLin Neurol Neurosurg 1988; 90:
35 In Summary SAH is a serious but treatable condition if diagnosed correctly and treated timely. SAH presents with a constellation of severe neurologic and systemic symptoms. SAH treatment requires correct initial diagnosis, prompt alleviation of hydrocephalus, aneurysm obliteration, and critical care support through delayed vasospasm. Successful SAH treatment requires a collaborative team including emergency medicine, neurosurgery, interventional neuroradiology, and neurocritical care specialists.
36 Thank you
37 SAH Mimics Thunder-clap headaches in migrainers Sudden cardiac arrest Cocaine use Call-Fleming Syndrome Vasculitis of cerebral vessels Eclampsia/Post-partum angiopathy
38 Delayed Vasospasm: Diagnostic Tools 1. Transcranial Doppler Ultrasound Monitoring Useful as a surveillance tool (daily monitoring with pre-vsp baseline velocities known). Sensitivity and specificity best for MCA spasm, and is operator dependent. May only detect large vessel spasm Lindergaard ratio: distinguish between VSP and hyperremia.


39 Transcranial Doppler Ultrasound Pro: non-invasive you can do this everyday; no contrast load. Con: neither sufficiently sensitive nor specific requires confirmatory studies.
40 Delayed Vasospasm: Diagnostic Tools 2. CT Angiography +/- CT Perfusion: Pro: non-invasive, anatomic study that can visualize mid size cerebral vessels. Con: not yet validated (though new data are promising); contrast load. 3. Conventional 4-vessel Cerebral Angiography: Pro: Gold-standard diagnostic tool; allows direct intervention if VSP is seen. Con: Invasive; complications include stroke, vessel dissection, hematoma.
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Takotsubo Cardiomyopathy: Pathophysiology and Assessment
 Takotsubo Cardiomyopathy: Pathophysiology and Assessment Roberto M Lang, MD Tako-Tsubo Cardiomyopathy Broken Heart Syndrome Apical Balooning 1. Sato H, Tateishi H, Uchida T, et al. Takotsubo type cardiomyopathy
Takotsubo Cardiomyopathy: Pathophysiology and Assessment Roberto M Lang, MD Tako-Tsubo Cardiomyopathy Broken Heart Syndrome Apical Balooning 1. Sato H, Tateishi H, Uchida T, et al. Takotsubo type cardiomyopathy
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Case Report Inverted (Reverse) Takotsubo Cardiomyopathy following Cerebellar Hemorrhage
 Takotsubo Cardiomyopathy following Cerebellar Hemorrhage") Case Reports in Cardiology, Article ID 781926, 4 pages http://dx.doi.org/10.1155/2014/781926 Case Report Inverted (Reverse) Takotsubo Cardiomyopathy following Cerebellar Hemorrhage Sophie Piérard, 1 Marco
Case Reports in Cardiology, Article ID 781926, 4 pages http://dx.doi.org/10.1155/2014/781926 Case Report Inverted (Reverse) Takotsubo Cardiomyopathy following Cerebellar Hemorrhage Sophie Piérard, 1 Marco
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
This quiz is being published on behalf of the Education Committee of the SNACC.
 Shobana Rajan, M.D. Assistant professor Anesthesiology, Cleveland Clinic, Cleveland, Ohio Quiz Team; Suneeta Gollapudy M.D, Verghese Cherian M.D This quiz is being published on behalf of the Education
Shobana Rajan, M.D. Assistant professor Anesthesiology, Cleveland Clinic, Cleveland, Ohio Quiz Team; Suneeta Gollapudy M.D, Verghese Cherian M.D This quiz is being published on behalf of the Education
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
NEUROCARDIOLOGY NEUROCARDIOLOGY
 NEUROCARDIOLOGY JON BRILLMAN, M.D CHAIRMAN EMERITUS, DEPARTMENT OF NEUROLOGY ALLEGHENY GENERAL HOSPITAL PROFESSOR OF NEUROLOGY DREXEL UNIVERSITY COLLEGE OF MEDICINE, ALLEGHENY CAMPUS 1 SUD SUDDEN DEATH
NEUROCARDIOLOGY JON BRILLMAN, M.D CHAIRMAN EMERITUS, DEPARTMENT OF NEUROLOGY ALLEGHENY GENERAL HOSPITAL PROFESSOR OF NEUROLOGY DREXEL UNIVERSITY COLLEGE OF MEDICINE, ALLEGHENY CAMPUS 1 SUD SUDDEN DEATH
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Treatment of Acute Hydrocephalus After Subarachnoid Hemorrhage With Serial Lumbar Puncture
 19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Clinical manifestations, diagnosis and medical management of
 Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Takotsubo cardiomyopathy. Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida
 Takotsubo cardiomyopathy Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida 79 year old woman, pre chemo echo for esophageal cancer Post chemo, dehydration,
Takotsubo cardiomyopathy Joseph L. Blackshear, MD Professor of Medicine Mayo Clinic College of Medicine Mayo Clinic Florida 79 year old woman, pre chemo echo for esophageal cancer Post chemo, dehydration,
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Case report: Intra-procedural aneurysm rupture during endovascular treatment causing immediate, transient angiographic vasospasm Zoe Zhang, MD
 Case report: Intra-procedural aneurysm rupture during endovascular treatment causing immediate, transient angiographic vasospasm Zoe Zhang, MD, Farhan Siddiq, MD, Wondwossen G Tekle, MD, Ameer E Hassan,
Case report: Intra-procedural aneurysm rupture during endovascular treatment causing immediate, transient angiographic vasospasm Zoe Zhang, MD, Farhan Siddiq, MD, Wondwossen G Tekle, MD, Ameer E Hassan,
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Imaging of Coronary Artery Disease: II
 Acta Radiológica Portuguesa, Vol.XIX, nº 74, pág. 45-51, Abr.-Jun., 2007 Imaging of Coronary Artery Disease: II Jean Jeudy University of Maryland School of Medicine Department of Diagnostic Radiology Armed
Acta Radiológica Portuguesa, Vol.XIX, nº 74, pág. 45-51, Abr.-Jun., 2007 Imaging of Coronary Artery Disease: II Jean Jeudy University of Maryland School of Medicine Department of Diagnostic Radiology Armed
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC
 Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Paul Gigante HMS IV Gillian Lieberman, MD. Sept Mr. T s T s Headache. Paul Gigante,, Harvard Medical School Year IV Gillian Lieberman, MD
 Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage
 Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage Hubert Lee A thesis submitted to the Faculty of Graduate and Postdoctoral Studies in partial fulfillment of the requirements
Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage Hubert Lee A thesis submitted to the Faculty of Graduate and Postdoctoral Studies in partial fulfillment of the requirements
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage
 Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Myocardial Infarction
 Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Ruptured Cerebral Aneurysm of the Anterior Circulation
 Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Treatment of Unruptured Vertebral Artery Dissecting Aneurysms
 33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
33 Treatment of Unruptured Vertebral Artery Dissecting Aneurysms Isao NAITO, M.D., Shin TAKATAMA, M.D., Naoko MIYAMOTO, M.D., Hidetoshi SHIMAGUCHI, M.D., and Tomoyuki IWAI, M.D. Department of Neurosurgery,
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Subarachnoid Hemorrhage & Vasospasm basic level
 Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Subarachnoid Haemorrhage
 2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
Takotsubo Cardiomyopathy
 Advances in Heart Disease 2008 Takotsubo Cardiomyopathy Mary O. Gray, MD, FAHA, FACC Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training Faculty Divisions
Advances in Heart Disease 2008 Takotsubo Cardiomyopathy Mary O. Gray, MD, FAHA, FACC Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training Faculty Divisions
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive