Children with Single Ventricle Physiology: The Possibilities
|
|
|
- Ronald Blankenship
- 5 years ago
- Views:
Transcription

1 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center at Houston (UTHealth) Medical School
2 Single Ventricle Physiology Definition A cardiac defect in which there is only one functioning ventricle The single ventricle may be a morphological right or left ventricle, or indeterminate May be due to underdeveloped chamber, valve, or outflow tract There may be two good-sized ventricles where the inflow and/or outflow tracts cannot be separated
3 Single Ventricle Physiology Diagnoses Tricuspid atresia Pulmonary atresia with intact septum HLHS Unbalanced AVSD D-TGA w/ HV L-TGA w/ HV Heterotaxy Ebstein s anomaly Double inlet LV DORV AVC with TGA
4 Normal Circulation
5 Normal Circulation
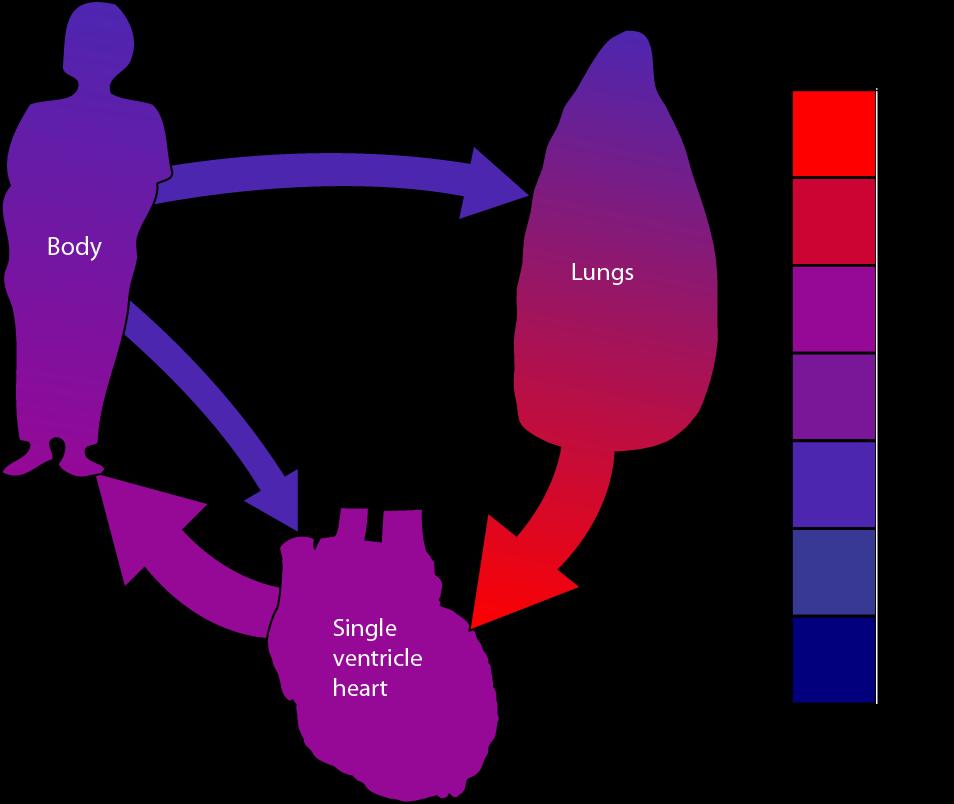
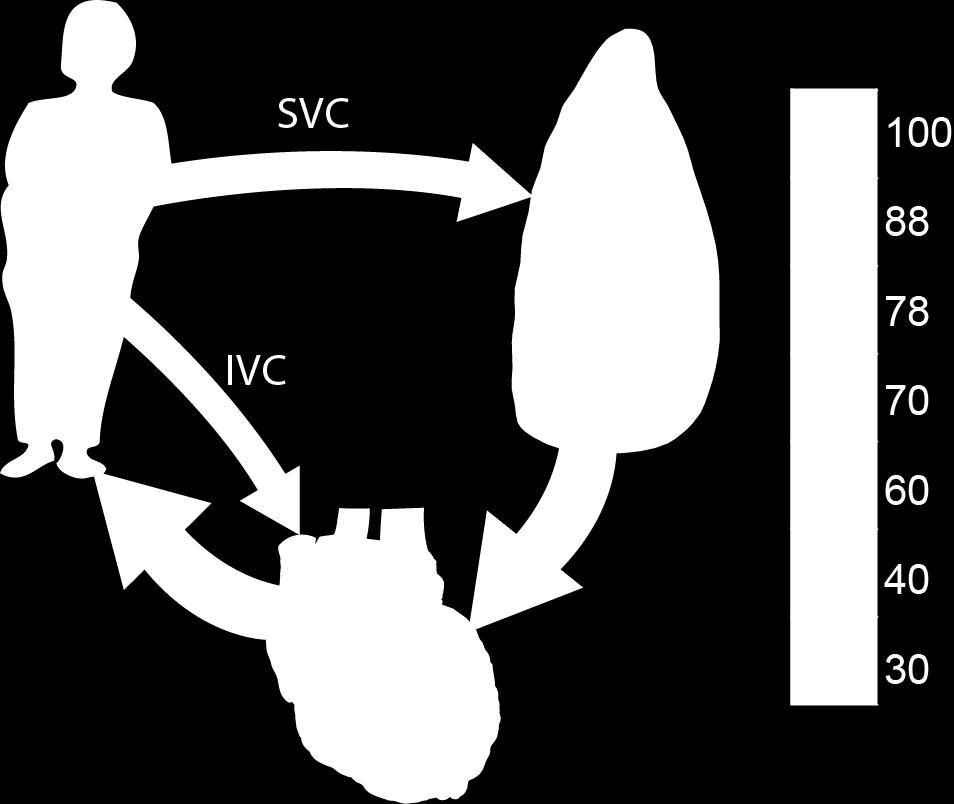
6 Single Ventricle Circulation
7 Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Single Ventricle Physiology Possibilities at Birth Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed
8 Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Single Ventricle Physiology Possibilities at Birth Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed
9 Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed Single Ventricle Physiology Possibilities at Birth
10 Single Ventricle Physiology Possibilities at Birth Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed
11 Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Single Ventricle Physiology Possibilities at Birth Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed
12 Principles of SVP Pulmonary Resistance < Systemic Resistance Ideal Qp:Qs 1 Single Ventricle Physiology Possibilities at Birth Pulmonary stenosis necessary to achieve ideal Qp:Qs There is no balanced systemic obstruction The pulmonary outflow and systemic outflow cannot both be obstructed
13 Single Ventricle Physiology Possibilities at Birth Unobstructed systemic blood flow Appropriately balanced Pulmonary stenosis No Surgery Insufficient PBF (Severe PS or atresia) BT Shunt Excessive PBF (unobstructed PA) PA Band Obstructed systemic blood flow Complex Neonatal Surgery (Norwood)

14 Unobstructed systemic blood flow Appropriately balanced Pulmonary stenosis No Surgery Single Ventricle Physiology Possibilities at Birth
15 Unobstructed systemic blood flow Unobstructed pulmonary blood flow Excessive PBF Single Ventricle Physiology Possibilities at Birth
 PA Band Single Ventricle Physiology Possibilities at")
16 Unobstructed systemic blood flow Excessive PBF (unobstructed PA) PA Band Single Ventricle Physiology Possibilities at Birth
17 Unobstructed systemic blood flow Insufficient PBF (Severe PS or atresia) Single Ventricle Physiology Possibilities at Birth
18 Unobstructed systemic blood flow Insufficient PBF (Severe PS or atresia) Systemic-Pulmonary Artery Shunt Shunt Single Ventricle Physiology Possibilities at Birth
19 Single Ventricle Physiology Possibilities at Birth Obstructed systemic blood flow Implies unobstructed flow to the lungs Make Qs arrow smaller
20 Obstructed systemic blood flow Complex Neonatal Surgery (DKS, Norwood) Single Ventricle Physiology Possibilities at Birth
21 Obstructed systemic blood flow Complex Neonatal Surgery (DKS, Norwood) Single Ventricle Physiology Possibilities at Birth
22 Surgical Treatment Single ventricle physiology Unobstructed flow to the body Moderately obstructed blood flow to the body No surgery as a newborn

23 Bored Surgeon
24 Surgical Treatment Single ventricle physiology Unobstructed flow to the body Severely obstructed blood flow to the lungs Systemic-pulmonary artery shunt (BT shunt) Usually performed without cardiopulmonary bypass Operative mortality: 5%
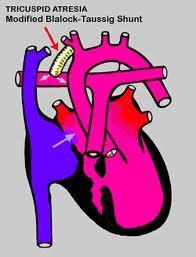
25 Blalock-Taussig Shunt
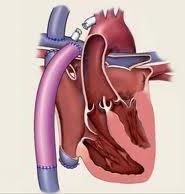
26 Surgical Treatment Single ventricle physiology Unobstructed flow to the body Unobstructed flow to the lungs Surgery: Pulmonary artery band (PA Band) Almost always without cardiopulmonary bypass Operative Mortality: 5%

27 Pulmonary Artery Band
28 Surgical Treatment Obstructed blood flow to the body Blood flow to the lungs always unobstructed These are the complex procedures Re-route the pulmonary outflow to the aorta Add back pulmonary blood flow (e.g., BT shunt) Always require CPB; often circulatory arrest Norwood or Damus-Kaye-Stansel Operative mortality: 15%

29 Norwood Procedure
30 Single Ventricle Physiology WHAT HAPPENS NEXT
31 Single Ventricle Physiology SPA Shunt: Disadvantages Arterial blood not fully saturated Difficult to precisely control amount of pulmonary blood flow Inherent volume overload Doomed for failure
32 Single Ventricle Physiology Solution: Fontan Procedure Total cavopulmonary anastomosis Allows the pulmonary and systemic circuits to be in series Patients are fully oxygenated Volume overload on the ventricle is removed
33 Fontan Procedure
34 Fontan
35 Superior Cavopulmonay Anastomosis

36 Staged Fontan
37 Single Ventricle Physiology Staged Approach Stage I: neonatal physiology Small percentage won t need surgery BT Shunt or PA Band if pulm blood flow or 5% operative risk Norwood needed if aortic obstruction present 15% risk procedures Stage II: Glenn (sup. cavopulmonary shunt) Six months of age Stage III: total cavopulmonary anastomosis (Fontan) 2-3 years of age
38 Children with Single Ventricle Physiology OUTCOMES
39 Outcomes in Pediatric Cardiac Surgery Risk adjustment methods Basic outcome statistics
40 Risk Adjustment Methods Mortality to hospital discharge is the current metric for judging program outcomes 30 day mortality not appropriate 30 day mortality not benchmarked Raw mortality not sufficient as programs have different profiles of case complexity
41 Risk Adjustment Methods RACHS-1 is first method created All subsequent methods relatively similar 79 identified procedures were divided into 5 groups (by experts) Originally 6 groups (one group too small)
42 RACHS-1 Level 1 (Simple) Level 2 (Straightforwar d) Level 3 (Moderately Complex) Level 4 (Complex) Level 5-6 PDA Ligation VSD Closure Complete AVC ASO + VSD Norwood ASD closure TOF Repair Fontan Truncus Damus-Kaye- Stansel CoA Repair (>30 days) Partial AV Canal Arterial Switch PAPVR Glenn Valve Replacements TAPVR (>30 days) BT Shunts and PA Bands TAPVR (<30 days) Interrupted Aortic Arch Hypoplastic Arch Repair Truncus-IAA (Level 5)
43 Other Risk Adjustment Methods Aristotle 130 operations each with its own score Grouped into 4 Levels STS-EACTS Very similar to RACHS-1, except data has redefined which operations are grouped State of Texas (AHRQ) Privileged methodogy 6 risk levels (like RACHS-1) with some non-cardiac comorbidities
44 Important Insight All primarily use PROCEDURE to stratify risk Few use any patient related variables None use any cardiac co-morbidities: A 6-hour old child with a single ventricle and highly obstructed TAPVR undergoes emergent TAPVR repair A 2 week-old with unobstructed TAPVR undergoes semi-elective repair THEY CARRY THE SAME RISK PROFILE; THEY HAD THE SAME PROCEDURE STS Data is Voluntarily Submitted
45 Bottom Line Data is useful for screening programs which are outliers Wide variability in accuracy Not good for distinguishing between good programs
46 Outcomes: Sources Source Society of Thoracic Surgeons Comprehensive US Database STS-EACTS Combined US- European Database Single Ventricle Trial Prospective trial with focused population (HLHS) First Author NA O Brien Ohye Journal/ Reference Note Complete and well analyzed Not readily available Data is voluntarily submitted How most programs are judged NA JTCVS 2009; 138(5): 1139 Varied centers, so difficult to interpret results Fairly complete list of mortality (by lesion) published N Engl J Med 2010;362: Prospectively collected data on a uniform lesion Very well analyzed Describes natural history of HLHS
47 STS ,000 operations submitted 24,000 analyzed in 20,000 patients Discharge mortality: 3.2% Discharge mortality by age group: Neonates (0-30 days): 9.1% Infants (1 month 1 year): 2.8% Children (1-18 years): 1.1% Adults (>18 years): 2.7%
48 STS 2010 Mortality for Key Procedures Norwood: 15% Not just Classic HLHS TAPVR: 9.6% Obstructed and unobstructed Interrupted Aortic Arch: 5.6% Systemic-Pulmonary Artery Shunt: 4.7% Arterial Switch: 2.0% Arterial Switch + VSD: 4.0% Arterial Switch + Arch Repair: 11.5%
49 STS 2010 Mortality for Key Procedures Complete AV Canal: 2.9% Tetralogy of Fallot: 0.9% (no RV-PA conduit) PA Band: 6.7% Ross: 1.1% Ross-Konno: 13.6%
50 Combined European + STS Overall: 4.3% ( ) Coarctation repair: 2.5% Arterial switch: 4.8% ASO + aortic arch repair: 11% Aortic arch repair: 7.9% TOF repair: 2% Complete AV Canal: 4.6% Truncus: 14.3% Norwood: 23.7%
51 Single Ventricle Trial (HLHS) Death or Transplantation (12 months): 31.3% Time to initial extubation: 5.25 days Average ICU stay: 14 days Incidence of ECMO: 10% Incidence of CPR: 16% Excludes patients with any major extracardiac abnormality affect the likelihood of survival(?) Cohort did include patients <2.5 kg
52 Summary Newborns with single ventricle physiology can be grouped into 4 treatment categories Simplifies initial explanation to families Pediatric cardiac surgery still carries a significant operative mortality Neonatal pediatric cardiac surgery exceptionally high risk Mortality for neonatal cardiac surgery: 9-10%

53
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database. Carlos M.
 Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database Carlos M. Mery, MD, MPH Assistant Professor, and Pediatrics Congenital Heart Texas
Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database Carlos M. Mery, MD, MPH Assistant Professor, and Pediatrics Congenital Heart Texas
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin. Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong
 Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Leitlinien. Hypoplastisches Linksherzsyndrom. Hypoplastic left heart syndrome (HLHS)
") 1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
Down Syndrome Medical Interest Group Friday, 12 June Cardiac Surgery in patients with Down Syndrome
 Down Syndrome Medical Interest Group Friday, 12 June 2015 Cardiac Surgery in patients with Down Syndrome Mr. Attilio Lotto, FRCS CTh Congenital Cardiac Surgeon Cardiac surgery in patients with Down syndrome
Down Syndrome Medical Interest Group Friday, 12 June 2015 Cardiac Surgery in patients with Down Syndrome Mr. Attilio Lotto, FRCS CTh Congenital Cardiac Surgeon Cardiac surgery in patients with Down syndrome
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
5/22/2013. Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4
 Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4 1 National Library of Medicine, NIH, Bethesda, MD, USA, 2 Centers for Disease Control and Prevention,
Alan Zuckerman 1, Swapna Abhyankar 1, Tiffany Colarusso 2, Richard Olney 2, Kristin Burns 3, Marci Sontag 4 1 National Library of Medicine, NIH, Bethesda, MD, USA, 2 Centers for Disease Control and Prevention,
Surgical Treatment for Double Outlet Right Ventricle. Masakazu Nakao Consultant, Paediatric Cardiothoracic Surgery
 for Double Outlet Right Ventricle Masakazu Nakao Consultant, Paediatric Cardiothoracic Surgery 1 History Intraventricular tunnel (Kawashima) First repair of Taussig-Bing anomaly (Kirklin) Taussig-Bing
for Double Outlet Right Ventricle Masakazu Nakao Consultant, Paediatric Cardiothoracic Surgery 1 History Intraventricular tunnel (Kawashima) First repair of Taussig-Bing anomaly (Kirklin) Taussig-Bing
Preoperative Echocardiographic Assessment of Uni-ventricular Repair
 Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT
 LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
LEFT VENTRICULAR OUTFLOW OBSTRUCTION WITH A VSD: OPTIONS FOR SURGICAL MANAGEMENT 10-13 March 2017 Ritz Carlton, Riyadh, Saudi Arabia Zohair AlHalees, MD Consultant, Cardiac Surgery Heart Centre LEFT VENTRICULAR
4a.i. 4a.ii. Form 12: Pre Transplant Status Report. Height and Weight. Status.
 PHTS - Form : Pre Transplant Report Page of 5 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Pre Transplant Report Print this Form t Started Was
PHTS - Form : Pre Transplant Report Page of 5 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form : Pre Transplant Report Print this Form t Started Was
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Perioperative Management of DORV Case
 Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Fundamentals of Congenital heart surgery in the adult
 Fundamentals of Congenital heart surgery in the adult Hospital Nacional A Posadas Hospital Universitario Austral Christian Kreutzer, MD AATS Cardiovscular Symposium, Sao Paulo December, 2017 STS CHSD Procedures
Fundamentals of Congenital heart surgery in the adult Hospital Nacional A Posadas Hospital Universitario Austral Christian Kreutzer, MD AATS Cardiovscular Symposium, Sao Paulo December, 2017 STS CHSD Procedures
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Surgical Procedures. Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder
 PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
NASCI 2012 Segmental Analysis
 NASCI 2012 Segmental Analysis Frandics Chan, M.D., Ph.D. Stanford University Medical Center Lucile Packard Department Children s of Radiology Hospital Menagerie of Congenital Cardiac Lesions 1. Absent
NASCI 2012 Segmental Analysis Frandics Chan, M.D., Ph.D. Stanford University Medical Center Lucile Packard Department Children s of Radiology Hospital Menagerie of Congenital Cardiac Lesions 1. Absent
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Tetralogy of Fallot (TOF) repair, Ventriculotomy Coarctation repair, Other
 repair, Ventriculotomy Coarctation repair, Other") Tier 1 Surgery Form Date of Surgery DD/MM/YYYY Primary Cardiac Procedure Select the patient's primary surgical procedure. If the patient has multiple operating room visits, these should be reported on
Tier 1 Surgery Form Date of Surgery DD/MM/YYYY Primary Cardiac Procedure Select the patient's primary surgical procedure. If the patient has multiple operating room visits, these should be reported on
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
NIH Public Access Author Manuscript World J Pediatr Congenit Heart Surg. Author manuscript; available in PMC 2015 April 01.
 NIH Public Access Author Manuscript Published in final edited form as: World J Pediatr Congenit Heart Surg. 2014 April ; 5(2): 272 282. doi:10.1177/2150135113519455. Linking the Congenital Heart Surgery
NIH Public Access Author Manuscript Published in final edited form as: World J Pediatr Congenit Heart Surg. 2014 April ; 5(2): 272 282. doi:10.1177/2150135113519455. Linking the Congenital Heart Surgery
The Arterial Switch Operation for Transposition of the Great Arteries
 The Arterial Switch Operation for Transposition of the Great Arteries Jan M. Quaegebeur, M.D., Ph.D. A Journey of 60 Years Transposition of the Great Arteries First description: M. BAILLIE The morbid anatomy
The Arterial Switch Operation for Transposition of the Great Arteries Jan M. Quaegebeur, M.D., Ph.D. A Journey of 60 Years Transposition of the Great Arteries First description: M. BAILLIE The morbid anatomy
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Management of a Patient after the Bidirectional Glenn
 Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Dear Parent/Guardian,
 Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Double outlet right ventricle: navigation of surgeon to chose best treatment strategy
 Double outlet right ventricle: navigation of surgeon to chose best treatment strategy Jan Marek Great Ormond Street Hospital & Institute of Cardiovascular Sciences, University College London Double outlet
Double outlet right ventricle: navigation of surgeon to chose best treatment strategy Jan Marek Great Ormond Street Hospital & Institute of Cardiovascular Sciences, University College London Double outlet
The Double Switch Using Bidirectional Glenn and Hemi-Mustard. Frank Hanley
 The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Accuracy of the Fetal Echocardiogram in Double-outlet Right Ventricle
 Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Validation of Relative Value Scale for Congenital Heart Operations
 Validation of Relative Value Scale for Congenital Heart Operations Kathy J. Jenkins, MD, Kimberlee Gauvreau, ScD, Jane W. Newburger, MD, Ludmila B. Kyn, MA, Lisa I. Iezzoni, MD, and John E. Mayer, MD Departments
Validation of Relative Value Scale for Congenital Heart Operations Kathy J. Jenkins, MD, Kimberlee Gauvreau, ScD, Jane W. Newburger, MD, Ludmila B. Kyn, MA, Lisa I. Iezzoni, MD, and John E. Mayer, MD Departments
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
ISUOG Basic Training. Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA. Basic training. Editable text here
 ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center
 Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs)
") Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs) Manny Gaziano, MD, FACOG obimages.net obimages.net@gmail.com Acknowledgements: Krista Wald, RDMS, sonographer,
Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs) Manny Gaziano, MD, FACOG obimages.net obimages.net@gmail.com Acknowledgements: Krista Wald, RDMS, sonographer,
The modified natural history of congenital heart disease
 The modified natural history of congenital heart disease Matthias Greutmann, MD Adult Congenital Heart Disease Program University Hospital Zurich, Switzerland matthias.greutmann@usz.ch Are we ready for
The modified natural history of congenital heart disease Matthias Greutmann, MD Adult Congenital Heart Disease Program University Hospital Zurich, Switzerland matthias.greutmann@usz.ch Are we ready for
What Can the Database Tell Us About Reoperation?
 AATS/STS Congenital Heart Disease Postgraduate Symposium May 5, 2013 What Can the Database Tell Us About Reoperation? Jeffrey P. Jacobs, M.D. All Children s Hospital Johns Hopkins Medicine The Congenital
AATS/STS Congenital Heart Disease Postgraduate Symposium May 5, 2013 What Can the Database Tell Us About Reoperation? Jeffrey P. Jacobs, M.D. All Children s Hospital Johns Hopkins Medicine The Congenital
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
"Giancarlo Rastelli Lecture"
 "Giancarlo Rastelli Lecture" Surgical treatment of Malpositions of the Great Arteries Pascal Vouhé Giancarlo Rastelli (1933 1970) Cliquez pour modifier les styles du texte du masque Deuxième niveau Troisième
"Giancarlo Rastelli Lecture" Surgical treatment of Malpositions of the Great Arteries Pascal Vouhé Giancarlo Rastelli (1933 1970) Cliquez pour modifier les styles du texte du masque Deuxième niveau Troisième
Outflow Tracts Anomalies
 Diagnosis of Outflow Tract Anomalies in the Fetus General Framing D.Paladini Fetal Medicine & Surgery Unit Gasllini Children s Hospital - Genoa dariopaladini@ospedale-gaslini.ge.it Outflow Tracts Anomalies
Diagnosis of Outflow Tract Anomalies in the Fetus General Framing D.Paladini Fetal Medicine & Surgery Unit Gasllini Children s Hospital - Genoa dariopaladini@ospedale-gaslini.ge.it Outflow Tracts Anomalies
Damus-Kaye-Stanzel vs Bulboventricular Foramen resection
 Damus-Kaye-Stanzel vs Bulboventricular Foramen resection Emile Bacha, MD Director, Pediatric Cardiac Surgery Morgan Stanley Children s Hospital of New York-Presbyterian Columbia University Medical Center
Damus-Kaye-Stanzel vs Bulboventricular Foramen resection Emile Bacha, MD Director, Pediatric Cardiac Surgery Morgan Stanley Children s Hospital of New York-Presbyterian Columbia University Medical Center
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
An Analysis of Results for the Norwood. Operation at Evelina London Children s Hospital (ELCH)
") An Analysis of Results for the Norwood Operation at Evelina London Children s Hospital (ELCH) 2012-2015 1 Introduction This report addresses the concerns raised by the 2012-2015 National Congenital Heart
An Analysis of Results for the Norwood Operation at Evelina London Children s Hospital (ELCH) 2012-2015 1 Introduction This report addresses the concerns raised by the 2012-2015 National Congenital Heart
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 2013
 Fall Work Weekend Nov. 2013") Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 03 Work Weekend Objectives General overview of cohort Generate feasible research question based on current data Early
Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 03 Work Weekend Objectives General overview of cohort Generate feasible research question based on current data Early
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Appendix A.2: Tier 2 Surgical Procedure Terms and Definitions
 Appendix A.2: Tier 2 Surgical Procedure Terms and Definitions Tier 2 surgeries Anomalous Systemic Venous Connection Anomalous Systemic Venous Connection Repair Repair includes a range of surgical approaches,
Appendix A.2: Tier 2 Surgical Procedure Terms and Definitions Tier 2 surgeries Anomalous Systemic Venous Connection Anomalous Systemic Venous Connection Repair Repair includes a range of surgical approaches,
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Trends in 30-day mortality rate and case mix for paediatric cardiac surgery in the UK between 2000 and 2010
 To cite: Brown KL, Crowe S, Franklin R, et al. Trends in 30-day mortality rate and case mix for paediatric cardiac surgery in the UK between 2000 and 2010. Open Heart 2015;2:e000157. doi:10.1136/openhrt-2014-000157
To cite: Brown KL, Crowe S, Franklin R, et al. Trends in 30-day mortality rate and case mix for paediatric cardiac surgery in the UK between 2000 and 2010. Open Heart 2015;2:e000157. doi:10.1136/openhrt-2014-000157
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
FUNCTIONALLY SINGLE VENTRICLE
 MORPHOLOGICAL DETERMINANTS VI TRAN EuroEcho, Budapest, 7 th December 2011 DECLARATION OF CONFLICT OF INTEREST: I have nothing to declare What is the functionally single ventricle? The heart that is incapable
MORPHOLOGICAL DETERMINANTS VI TRAN EuroEcho, Budapest, 7 th December 2011 DECLARATION OF CONFLICT OF INTEREST: I have nothing to declare What is the functionally single ventricle? The heart that is incapable
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 2013
 Fall Work Weekend Nov. 2013") Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 03 Work Weekend Objectives General overview of cohort Generate feasible research question based on current data Early
Critical Left Ventricular Outflow Tract Obstruction (LVOTO) Fall Work Weekend Nov. 03 Work Weekend Objectives General overview of cohort Generate feasible research question based on current data Early
Neonatal Single Ventricle Heart Disease Recognition, Management, Counseling
 Neonatal Single Ventricle Heart Disease Recognition, Management, Counseling Christopher J. Petit MD Assistant Professor, Pediatric Cardiology Director, Single Ventricle Program Baylor College of Medicine,
Neonatal Single Ventricle Heart Disease Recognition, Management, Counseling Christopher J. Petit MD Assistant Professor, Pediatric Cardiology Director, Single Ventricle Program Baylor College of Medicine,
Cardiac CT in Infants with Congenital heart disease Sunrise Session. LaDonna Malone, MD May 17, 2018
 Cardiac CT in Infants with Congenital heart disease Sunrise Session LaDonna Malone, MD May 17, 2018 None Disclosures Objectives Describe cardiac CT techniques used in infants with congenital heart disease.
Cardiac CT in Infants with Congenital heart disease Sunrise Session LaDonna Malone, MD May 17, 2018 None Disclosures Objectives Describe cardiac CT techniques used in infants with congenital heart disease.
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Upon completion of this presentation, the participant will be able to:
 B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
Hemodynamic assessment after palliative surgery
 THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Surgical Interventions for Congenital Heart Disease
 Chapter 46 Surgical Interventions for Congenital Heart Disease Alden M. Parsons, G. William Henry, and Michael R. Mill Our understanding of the complexities of congenital heart disease, a deviation from
Chapter 46 Surgical Interventions for Congenital Heart Disease Alden M. Parsons, G. William Henry, and Michael R. Mill Our understanding of the complexities of congenital heart disease, a deviation from
The Aristotle Comprehensive Complexity Score Predicts Mortality and Morbidity After Congenital Heart Surgery
 ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
World Database for Pediatric and Congenital Heart Surgery Appendix A: Surgical Procedure Terms and Definitions
 World Database for Pediatric and Congenital Heart Surgery Appendix A: Surgical Procedure Terms and Definitions All surgeries are Tier 2 surgeries unless otherwise noted. Anomalous Systemic Venous Connection
World Database for Pediatric and Congenital Heart Surgery Appendix A: Surgical Procedure Terms and Definitions All surgeries are Tier 2 surgeries unless otherwise noted. Anomalous Systemic Venous Connection
Management of complex CHD in adults
 Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
Management of complex CHD in adults Victor Tsang Society of Thoracic Surgeons of Thailand 2016 The impact of infant cardiac surgery Over 90 % of infants born with CHD will reach adulthood By 2010, adults
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Multimodality Imaging of Septal Defects
 Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Epidemiology of congenital heart diseases
 Epidemiology of congenital heart diseases Damien Bonnet Unité médico-chirurgicale de Cardiologie Congénitale et Pédiatrique Hôpital Universitaire Necker Enfants malades APHP, Université Paris Descartes,
Epidemiology of congenital heart diseases Damien Bonnet Unité médico-chirurgicale de Cardiologie Congénitale et Pédiatrique Hôpital Universitaire Necker Enfants malades APHP, Université Paris Descartes,