Multimodality Imaging of Septal Defects
|
|
|
- Ursula Floyd
- 5 years ago
- Views:
Transcription

1 Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide Children s Hospital The Ohio State University No relevant financial disclosure
2 Outline (Learning Objectives) Describe the different types of septal defects Isolated ASD and VSD Septal defects in complex congenital heart defects Review of available modalities to image septal defects Echocardiogram, CT and MRI Determine when to use each modality Example of cases to show added value of different modalities

3 Background: Septal Defects Atrial Septal Defects (ASD) 7-10% of all congenital defects 100/100,000 live births Frequently associated with complex CHD ASD shunt crucial in: Hypoplastic left heart syndrome D-transposition of the great arteries Tricuspid atresia Total anomalous pulmonary venous return
4 Background: Septal Defects Ventricular Septal Defects (VSD) 20% of all congenital defects 5-50/1,000 live births Frequently associated with complex CHD Most common lesion in chromosomal anomalies >95% of VSDs do not have associated chromosomal anomaly



5 Background: Imaging Modalities Images of the heart will be obtained to evaluate structure and function
6 Background: Imaging Modalities Echocardiography Cardiac Magnetic Resonance Imaging Cardiac CT Angiography
 3-Dimension (3D TTE or TEE) Workhorse of most")
7 Background: Imaging Modalities Echocardiography Transthoracic (TTE) Transesophageal (TEE) 3-Dimension (3D TTE or TEE) Workhorse of most imaging lab


8 Background: Echocardiography Advantages Readily available Can be done quickly Great first line tool Doppler assessment* Disadvantages Difficult windows Extra cardiac vessels can be difficult to visualize Not able to measure flow or saturation accurately



9 Background: Cardiac MRI Advantages Accurate measurements Anatomy, function, chamber, flow Tissue characterization and other newer techniques Disadvantages IV placement for scar and angiography May take longer study - improving Have to lay still Not as readily available-changing
10 Background: Cardiac MRI CMR - is not just one test, it is many tests rolled into one modality (one stop shop) Similar to CT angiography but without radiation exposure Similar to echocardiogram but without acoustic window limitations Cardiac MRI is a one stop shop




11 Background: Cardiac MRI ICMR T2 mapping for edema T1 Diffuse Fibrosis Extracellular volume (ECV) extracellular matrix expansion T2 Relaxometry - O2 Sat For inflammation For Scar assessment Myocardial Tissue Characteristic Perfusion Cardiac MRI Flow Studies Stress Test Tagged Imaging Function Pericardium Masses MRA
12 Background: CMR vs CTA Cardiac MRI comprehensive diagnostic test But there are times when we should consider a CT instead: Risk of heating up Risk of movement Interruption of device function Artifacts from device, stents or coils Sedation issues/risk Horwood t al, Europace, 2016, Russo et al, Circ 2014, Langman et al, Pacing Clin Electrophy 2011, Langman et al, JMRI 2011, Higgins et al, Pacing Clin Electrophy 2014, mrisafety.com,
13 Han et al, JCCT, 2013 Background: CTA When to use CT Angiography over Cardiac MRI? The need for speed CTA takes 0.35 to 0.5 seconds MRA seconds per dynamic CT has better spatial resolution (0.5 mm) Avoid or minimize sedation Basis: in some patients initiation of anesthesia adds significant risk (Williams Syndrome, pulmonary hypertension, unstable patients)
14 Cases Scenarios and Best Modality? Isolated secundum ASD in pediatrics Dilated right heart in older patients (? ASD) Other ASDs (superior sinus venosus ASD) ASD associated with complex CHD (non-heterotaxy) Complete Atrioventricular canal Hypoplastic left heart syndrome Isolated perimembranous VSD in pediatricsvsd frequently associated with complex CHD Unusually position large muscular VSD TOF/PA VSD with multiple aortopulmonary collateral vessels (MAPCAs) Double outlet right ventricle (DORV) A case of post-operative blue
15 Best Modality? 3 year male with isolated large secundum ASD with right sided enlargement ECHO only modality needed? Basis Echocardiogram has no risk and can be performed without sedation Define ASD size, rims and chamber sizes CT Angiography: limited to no value in this setting even with low dose new generation multi-detector scanners Cardiac MRI limited use in this situation at this time Issues including need for sedation (may change with faster sequences and bundling of patient) Additional value of Qp/Qs does not alter management


16 ECHO Best Modality: Isolated ASD 3 year male with murmur and fix split S2. Echo below with isolated large secundum ASD with right sided enlargement



17 ECHO Best Modality: Isolated ASD 3D Echo not vital but can help visualize septum in 3D space
18 Best Modality? 50 y/o male with murmur since childhood and RVH on ECG. ECHO only modality needed? Basis Echocardiogram has no risk but in larger patients the acoustic windows is limited Can we define ASD size, rims and chamber sizes? Identify other causes of right sided chamber enlargement? CT Angiography: limited to no value in this setting even with low dose new generation multi-detector scanners lack ability to show physiologic data Cardiac MRI Augment Echo finding with no risk if echo limited Confirm right chamber enlargement Additional value of Qp/Qs does can alter management Additional causes of right chamber enlargement can alter management



19 Best Modality? ECHO Enough? 50 y/o male murmur since childhood. Initial echo: possible drop out in atrial septum with some color jet noted with right heart enlargement Possible small ASD poor imaging windows

 Surgical repair of PAPVR only ASD left open (very small")
20 ECHO + CMR Best Modality 50 y/o male murmur since childhood. CMR: confirmed small ASD but found partial anomalous venous return of the LUPV and lingula with RVEDVi 118 ml/m2 and Qp/Qs of 1.7 to 1 (mostly from PAPVR) Surgical repair of PAPVR only ASD left open (very small shunt) CMR better delineate disease in this setting altered management

21 Best Modality? Superior Sinus Venosus ASD? 37 y/o with SOB and fatigue with history of murmur. Initial echo: drop out in superior atrial septum with some color jet noted with right heart enlargement.


22 CMR Best Modality: Beyond isolated ASD 37 y/o with SOB and fatigue with history of murmur. CMR: confirmed superior sinus ASD with RUPV, RMPV and likely part of RLPV with RVEDVi 129 ml/m2 and Qp/Qs of 1.8 to 1 Surgical repair ASD and PAPVR CMR better delineate disease in this setting CT adds no additional value with risk of radiation exposure

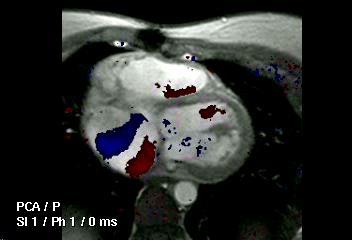
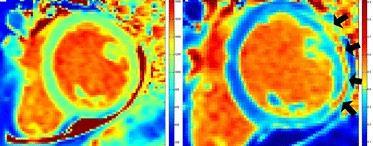
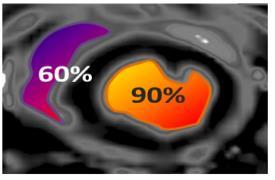
23 The Added Value of Cardiac MR Velocity Mapping for Flow Quantification In setting of septal defect use to assess Qp/Qs Augments anatomic, functional and volumetric data




")
24 The Added Value of Cardiac MR Quantification of volume and function Velocity Mapping for Flow Quantification: Qp/QS In setting of septal defect (example of ASD) MPA flow (Qp) and Aortic flow (Qs)
25 ASD frequently associated with complex CHD (non-heterotaxy) Complete atrioventricular canal defect ASD shunt crucial in: Best Modality? Hypoplastic left heart syndrome (obligate left to right shunt) D-transposition of the great arteries (mixing) Tricuspid atresia (obligate right to left shunt) Total anomalous pulmonary venous return (obligate right to left shunt) Atrial shunt must be non-restrictive
26 Best Modality? ASD in Complex CHD 1 week day old with Trisomy 21 with CAVC 2 day old with hypoplastic left heart syndrome ECHO only modality needed? Basis Echocardiogram has no risk and can be performed without sedation Define intra- and extracardiac anatomy well in most instances CT Angiography: limited to no value in this setting even with low dose new generation multi-detector scanners Cardiac MRI limited use in this situation at this time Issues including need for sedation with complex long scan time Additional value of Qp/Qs does not alter management Exception: associated with heterotaxy syndrome

 Spectrum of AV canal")


27 ECHO is Best Modality: ASD with CAVC ASD in setting of atrioventricular canal defect (AVC) Spectrum of AV canal defect from complete AVC or isolated primum ASD with or without cleft MV Echo is the best modality (no benefit of CT or CMR in my cases)






28 ECHO is Best Modality: ASD in HLHS ASD shunt crucial in: Hypoplastic left heart syndrome (obligate left to right shunt) Atrial restriction requires emergent balloon septostomy and/or stent Atrial restriction associated with high mortality Echo is the best modality (no benefit of CT or CMR in many cases, exception would be complex CHD with heterotaxy)
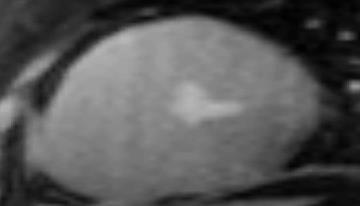
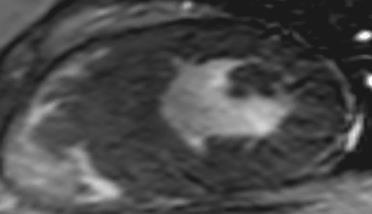
29 Best Modality? 3 month old with isolated large ventricular septal defect with increase work of breathing ECHO only modality needed? Basis Echocardiogram has no risk and can be performed with or withoout sedation Define intra- and extracardiac anatomy well in most instances CT Angiography: Need outweighs benefit CT for 3D modeling and printing can be performed without sedation and low dose (1 msev) Cardiac MRI limited use in this situation at this time



30 ECHO Best Modality: Isolated VSD 3 month old with large perimembranous VSD with inlet extension Repaired at 6 months with no complications No added value of CT or Cardiac MRI (risk outweighs benefit)
31 Best Modality? 3 month old with large unusually position apical muscular VSD (felt not to be a straight forward surgical candidate) ECHO only modality needed? Basis Echocardiogram has no risk and can be performed without sedation Define intra- and extracardiac anatomy well but challenging for 3D modeling and road mapping CT Angiography: Need outweighs benefit CT for 3D modeling and printing can be performed without sedation and low dose (1 msev) Cardiac MRI limited use in this situation at this time Compared to CT (need for sedation and low spatial resolution) results in risks outweighing benefit



32 ECHO Best Modality? 3 month old with isolated large unusually position apical muscular VSD Felt not to be a straight forward surgical candidate Rare occasion CT can complement echo for 3D printing and modeling

 Added value of CTA: 3D dataset")


33 ECHO + CTA Best Modality 3 month old with large unusually position apical muscular VSD (felt not to be a straight forward surgical candidate) Added value of CTA: 3D dataset for virtual assessment, 3D printing for device selection, post-device assessment on model and implantation Trans-atrial approach by modeling with prediction of small residual defect
34 Best Modality? VSD in Complex CHD VSD frequently associated with complex CHD Pulmonary atresia VSD with multiple aortopulmonary collateral vessels (MAPCAs) ECHO only modality needed? Basis Echocardiogram has no risk and can be performed without sedation Challenging to define extracardiac anatomy in MAPCAs CT Angiography: Need outweighs benefit CT for to define collaterals and can potentially delay cardiac catheterizatio can be performed without sedation and low dose (1 msev) Cardiac MRI limited use in this situation at this time Compared to CT (need for sedation and low spatial resolution) results in risks outweighing benefit





35 ECHO + CTA = Best Modality 1 day with Tetralogy of Fallot with near pulmonary atresia with MAPCAs Echocardiogram: Define intracardiac anatomy very well Non-sedated CT Angiography augmented Echo with road-mapping of the MAPCA Allows cardiac catheterization to be delayed until closer to surgical date
36 Best Modality? VSD in Complex CHD VSD frequently associated with complex CHD Double outlet right ventricle (defining relationship of VSD to aorta) ECHO only modality needed? Basis Echocardiogram has no risk and can be performed without sedation Challenging to define relationship of VSD to Aorta in some cases CT Angiography: Need outweighs benefit CT for 3D modeling and printing can be performed without sedation and low dose (1 msev) Cardiac MRI limited use in this situation at this time Compared to CT (need for sedation and low spatial resolution) results in risks outweighing benefit






37 ECHO + CTA = Best Modality Double outlet right ventricle inlet VSD with concern of AV chords affecting VSD to Aortic baffle Echocardiogram: Define intracardiac anatomy well but challenging to roadmap VSD to Aorta Non-sedated CT with low dose radiation performed for virtual and 3D modeling to determine that VSD can be baffle to the aorta Underwent biventricular repair with a Nikaidoh procedure with reconstruction of his right ventricular outflow tract (16 mm Contegra valved conduit)
38 Added Value of CT Angiography VSD frequently associated with complex CHD Pulmonary atresia VSD with multiple aortopulmonary collateral vessels (MAPCAs) Double outlet right ventricle (DORV) Echocardiogram is still first line tool CMR and CT augments echocardiogram Extracardiac vasculature with roadmapping of the MAPCAs. CT preference over Cardiac MRI with use of low dose radiation and no sedation (anatomy over physiology)
39 Best Modality? Post-Operative Blues 27 year old with history of ASD repair with desaturation on exercise testing ECHO only modality needed? Basis Echocardiogram has no risk should be first line Challenging in adults, agitated saline study (must understand defect) CT Angiography: limited to no value in this setting lack ability to show physiologic data Cardiac MRI Augment Echo finding if echo limited or questions remain Confirm any echo finding Additional value of Qp/Qs does can alter management Improve ability to assess challenging problems can alter management


40 Best Modality? 27 year old with history of ASD repair with desaturation on exercise testing ECHO: Structurally normal heart with left heart enlargement Intravenous injection of agitated saline contrast with no shunt. Further testing needed?





41 CMR = Best Modality 27 year old with history of ASD repair with desaturation on exercise testing Cardiac MRI: Sinus venosus defect and PAPVR s/p repair with no residual ASD but inferior vena cava baffle to left atrium (pt had inferior sinus venosus ASD with PAPVR)
42 The Added Value of Cardiac MR First issue: agitated saline contrast was performed on upper extremity. Given history of inferior ASD and cyanosis a LLE IV should have been placed Added value of CMR: Anatomically confirmed the surgical mis-hap and demonstrated the issues needed Alter management course Patient underwent surgical correction Patient feels great and has no desaturation with exercise
43 Multimodality Imaging of Septal Defects What is the best modality? ECHO, CT and Cardiac MRI are complementary tests Depends on what you are looking for Echo should always be first line tool Add CT or Cardiac MRI when Echo has limitations Difficult windows Extra cardiac vessels that are not well visualized When your questions have not been answered
44 Multimodality Imaging of Septal Defects What is the best modality? Use low risk test first Avoid radiation if possible In children balance risk benefit of radiation against sedation Determine what your goal is: Intracardiac anatomy: Echo is best Extra-cardiac anatomy: CT is best Anatomy and detail physiology: Cardiac MR is best
45


46 Thank you! Questions?
47 Background: CMR vs CTA CT Scan Radiation exposure: 2-10 msv = 3-5 yr back ground radiation Cost $ Time seconds MRI None - MRI does not emit ionizing radiation Cost $ Time = minutes to hours Application: vascular, bone Application: vascular and soft and lungs tissue Better spatial resolution Better temporal resolution Scan in systole HR >90, diastole MRA is collected over many heart HR < 90 or whole cardiac cycle beats and average of systole and diastole
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience
 Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience Ximing Wang, M.D., Zhaoping Cheng, M.D., Dawei Wu, M.D., Lebin
Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience Ximing Wang, M.D., Zhaoping Cheng, M.D., Dawei Wu, M.D., Lebin
Cardiology Fellowship Manual. Goals & Objectives -Cardiac Imaging- 1 P a g e
 Cardiology Fellowship Manual Goals & Objectives -Cardiac Imaging- 1 P a g e UNIV. OF NEBRASKA CHILDREN S HOSPITAL & MEDICAL CENTER DIVISION OF CARDIOLOGY FELLOWSHIP PROGRAM CARDIAC IMAGING ROTATION GOALS
Cardiology Fellowship Manual Goals & Objectives -Cardiac Imaging- 1 P a g e UNIV. OF NEBRASKA CHILDREN S HOSPITAL & MEDICAL CENTER DIVISION OF CARDIOLOGY FELLOWSHIP PROGRAM CARDIAC IMAGING ROTATION GOALS
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult: A Diagnostic Imaging Challenge
 Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia
 Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΜΕΣΟΚΟΛΠΙΚΗ ΕΠΙΚΟΙΝΩΝΙΑ ΖΑΧΑΡΑΚΗ ΑΓΓΕΛΙΚΗ ΚΑΡΔΙΟΛΟΓΟΣ ΗΡΑΚΛΕΙΟ - ΚΡΗΤΗ European Accreditation in TTE, TEE and CHD Echocardiography NOTHING TO DECLARE ATRIAL SEPTAL DEFECT TYPES SECUNDUM
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Anatomy of Atrioventricular Septal Defect (AVSD)
") Surgical challenges in atrio-ventricular septal defect in grown-up congenital heart disease Anatomy of Atrioventricular Septal Defect (AVSD) S. Yen Ho Professor of Cardiac Morphology Royal Brompton and
Surgical challenges in atrio-ventricular septal defect in grown-up congenital heart disease Anatomy of Atrioventricular Septal Defect (AVSD) S. Yen Ho Professor of Cardiac Morphology Royal Brompton and
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Simple Congenital Heart Lesions
 Journal of Cardiovascular Magnetic Resonance (2006) 8, 619 631 Copyright c 2006 Taylor & Francis Group, LLC ISSN: 1097-6647 print / 1532-429X online DOI: 10.1080/10976640600721510 CONGENITAL HEART DISEASE
Journal of Cardiovascular Magnetic Resonance (2006) 8, 619 631 Copyright c 2006 Taylor & Francis Group, LLC ISSN: 1097-6647 print / 1532-429X online DOI: 10.1080/10976640600721510 CONGENITAL HEART DISEASE
DGPK guideline: PAPVC
 DGPK guideline: PAPVC Partial anomalous pulmonary venous connection (PAPVC) Harald Bertram, Hannover Oliver Dewald, Bonn Angelika Lindinger, Kaiserslautern & Trier DGPK guideline committee No disclosures
DGPK guideline: PAPVC Partial anomalous pulmonary venous connection (PAPVC) Harald Bertram, Hannover Oliver Dewald, Bonn Angelika Lindinger, Kaiserslautern & Trier DGPK guideline committee No disclosures
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Atrial Septal Defect Closure. Stephen Brecker Director, Cardiac Catheterisation Labs
 Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Stephen Brecker Director, Cardiac Catheterisation Labs ADVANCED ANGIOPLASTY Incorporating The Left Main 5 Plus Course Conflicts of Interest The following companies have supported educational courses held
Cardiovascular MRI of Adult Congenital Heart Disease
 Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Perioperative Management of DORV Case
 Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Assessing Cardiac Anatomy With Digital Subtraction Angiography
 485 JACC Vol. 5, No. I Assessing Cardiac Anatomy With Digital Subtraction Angiography DOUGLAS S., MD, FACC Cleveland, Ohio The use of intravenous digital subtraction angiography in the assessment of patients
485 JACC Vol. 5, No. I Assessing Cardiac Anatomy With Digital Subtraction Angiography DOUGLAS S., MD, FACC Cleveland, Ohio The use of intravenous digital subtraction angiography in the assessment of patients
PULMONARY VENOLOBAR SYNDROME. Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital.
 PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Echocardiography in the Adult with Congenital Heart Disease
 1 1 Echocardiography in the Adult with Congenital Heart Disease Julie A. Kovach Indications for Echocardiography in the Evaluation of the Adult with Congenital Heart Disease........ 279 Indications and
1 1 Echocardiography in the Adult with Congenital Heart Disease Julie A. Kovach Indications for Echocardiography in the Evaluation of the Adult with Congenital Heart Disease........ 279 Indications and
Recent technical advances and increasing experience
 Pediatric Open Heart Operations Without Diagnostic Cardiac Catheterization Jean-Pierre Pfammatter, MD, Pascal A. Berdat, MD, Thierry P. Carrel, MD, and Franco P. Stocker, MD Division of Pediatric Cardiology,
Pediatric Open Heart Operations Without Diagnostic Cardiac Catheterization Jean-Pierre Pfammatter, MD, Pascal A. Berdat, MD, Thierry P. Carrel, MD, and Franco P. Stocker, MD Division of Pediatric Cardiology,
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
DISCLOSURE OBJECTIVES PULMONARY VEIN STENOSIS DIAGNOSTIC TOOLS. Echo with Doppler Catheterization with angiography CT angiography MRI
 1 2 ND INTERNATIONAL CONFERENCE: NEONATAL AND CHILDHOOD PULMONARY VASCULAR DISEASE, MARCH 13-14, 2009, SAN FRANCISCO, USA PATHOPHYSIOLOGY OF PULMONARY VEIN FLOW: IMAGING NORMAL AND ABNORMAL PULMONARY VEIN
1 2 ND INTERNATIONAL CONFERENCE: NEONATAL AND CHILDHOOD PULMONARY VASCULAR DISEASE, MARCH 13-14, 2009, SAN FRANCISCO, USA PATHOPHYSIOLOGY OF PULMONARY VEIN FLOW: IMAGING NORMAL AND ABNORMAL PULMONARY VEIN
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
The role of intraoperative TOE in congenital cardiac surgery
 The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Imaging of the Heart Todd Tessendorf MD FACC
 Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Spectrum of Findings of Sinus Venosus Atrial Septal Defect: CT and MR Findings
 Spectrum of Findings of Sinus Venosus Atrial Septal Defect: CT and MR Findings Poster No.: P-0026 Congress: ESCR 2015 Type: Scientific Poster Authors: J. M. Madrid, P. J. Mergo, P. Bartolomé, J. Phelan,
Spectrum of Findings of Sinus Venosus Atrial Septal Defect: CT and MR Findings Poster No.: P-0026 Congress: ESCR 2015 Type: Scientific Poster Authors: J. M. Madrid, P. J. Mergo, P. Bartolomé, J. Phelan,
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
UPDATE FETAL ECHO REVIEW
 UPDATE 1 FETAL ECHO REVIEW Study Alert for RDCS Candidates D A V I E S P U B L I S H I N G I N C. Fetal Echo Review Study Alert U P D A T E D A U G U S T 1, 2 0 1 2 Nikki Stahl, RT(R)(M)(CT), RDMS, RVT
UPDATE 1 FETAL ECHO REVIEW Study Alert for RDCS Candidates D A V I E S P U B L I S H I N G I N C. Fetal Echo Review Study Alert U P D A T E D A U G U S T 1, 2 0 1 2 Nikki Stahl, RT(R)(M)(CT), RDMS, RVT
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
2018 Guideline for the Management of Adults with Congenital Heart Disease
 2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE. Krishna Kumar SevenHills Hospital, Mumbai, India
 INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
INTEGRATING ECHOCARDIOGRAPHY WITH CATHETER INTERVENTIONS FOR CONGENITAL HEART DISEASE Krishna Kumar SevenHills Hospital, Mumbai, India Why talk about it? What is the big deal? Are we not stating the obvious?
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Surgical Management Of TAPVR. Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital
 Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
General Cardiovascular Magnetic Resonance Imaging
 2 General Cardiovascular Magnetic Resonance Imaging 19 Peter G. Danias, Cardiovascular MRI: 150 Multiple-Choice Questions and Answers Humana Press 2008 20 Cardiovascular MRI: 150 Multiple-Choice Questions
2 General Cardiovascular Magnetic Resonance Imaging 19 Peter G. Danias, Cardiovascular MRI: 150 Multiple-Choice Questions and Answers Humana Press 2008 20 Cardiovascular MRI: 150 Multiple-Choice Questions
September 28-30, 2018
 September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
The Adolescent and Adult Congenital Heart Disease Program
 The Adolescent and Adult Congenital Heart Disease Program The Heart Center at Nationwide Children s Hospital & The Ohio State University D- Transposition of the Great Vessels D- transposition of the great
The Adolescent and Adult Congenital Heart Disease Program The Heart Center at Nationwide Children s Hospital & The Ohio State University D- Transposition of the Great Vessels D- transposition of the great
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5
 DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
2D/3D in Evaluation of Atrial Septum
 2D/3D in Evaluation of Atrial Septum Roberto M Lang, MD OSTIUM SECUNDUM ASD: 2D AND 3D TNSESOPHAGEAL ECHO 1 Biplane views 90 0 3D Acquisi on Acquire 3D volume Lang RM et al. JASE 2012;25:3 46. Right atrial
2D/3D in Evaluation of Atrial Septum Roberto M Lang, MD OSTIUM SECUNDUM ASD: 2D AND 3D TNSESOPHAGEAL ECHO 1 Biplane views 90 0 3D Acquisi on Acquire 3D volume Lang RM et al. JASE 2012;25:3 46. Right atrial
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Segmental Analysis. Gautam K. Singh, M.D. Washington University School of Medicine St. Louis
 Segmental Analysis Gautam K. Singh, M.D. Washington University School of Medicine St. Louis Segmental Analysis Segmental Analysis: From Veins to Ventricles Segmental Approach to Evaluation of Congenital
Segmental Analysis Gautam K. Singh, M.D. Washington University School of Medicine St. Louis Segmental Analysis Segmental Analysis: From Veins to Ventricles Segmental Approach to Evaluation of Congenital
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Cardiac CT Techniques in Neonates (and infants)
") Cardiac CT Techniques in Neonates (and infants) Siddharth P. Jadhav, MD Director, Body CT and MRI Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Disclosures None Objectives
Cardiac CT Techniques in Neonates (and infants) Siddharth P. Jadhav, MD Director, Body CT and MRI Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Disclosures None Objectives
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
For Personal Use. Copyright HMP 2013
 12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
Fetal Tetralogy of Fallot
 36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
36 Fetal Tetralogy of Fallot E.D. Bespalova, R.M. Gasanova, O.A.Pitirimova National Scientific and Practical Center of Cardiovascular Surgery, Moscow Elena D. Bespalova, MD Professor, Director Rena M,
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
Implantation of Cardioverter Defibrillator After Percutaneous Closure of Atrial Septal Defect
 The Ochsner Journal 10:27 31, 2010 f Academic Division of Ochsner Clinic Foundation Implantation of Cardioverter Defibrillator After Percutaneous Closure of Atrial Septal Defect Anas Bitar, MD, Maria Malaya
The Ochsner Journal 10:27 31, 2010 f Academic Division of Ochsner Clinic Foundation Implantation of Cardioverter Defibrillator After Percutaneous Closure of Atrial Septal Defect Anas Bitar, MD, Maria Malaya
Echocardiography in Congenital Heart Disease
 Chapter 44 Echocardiography in Congenital Heart Disease John L. Cotton and G. William Henry Multiple-plane cardiac imaging by echocardiography can noninvasively define the anatomy of the heart and the
Chapter 44 Echocardiography in Congenital Heart Disease John L. Cotton and G. William Henry Multiple-plane cardiac imaging by echocardiography can noninvasively define the anatomy of the heart and the
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man