INVESTIGATIONAL TREATMENTS FOR SEPSIS AN OVERVIEW
|
|
|
- Hubert Hall
- 5 years ago
- Views:
Transcription

1 INVESTIGATIONAL TREATMENTS FOR SEPSIS AN OVERVIEW
2 THE GLOBAL BURDEN OF SEPSIS Mortality rate estimated to be 30-50% Rates estimated to be as high as 80% in developing nations One third to one half of all hospital deaths are related to sepsis Post Sepsis Syndrome: Survivors have significant long term physical, psychological, and cognitive disabilities 63% will be re-hospitalized within 1 year 1/3rd will die within the first year 24 billion spent annually in the US $325 million spent annually in Canada 45.1% of sepsis patients in Canada require ICU
3 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
4 SEPSIS: DEFINITION Life-threatening organ dysfunction caused by a dysregulated host response to an infection Three elements: Infection, Host response, Organ dysfunction Shaped by host, and pathogen factors Inflammatory mediators, clotting, anti-inflammatory mediators Characteristics can change over time Septic shock is considered a subset of sepsis Patients in which underlying circulatory, cellular, and metabolic abnormalities are profound enough to substantially increase mortality Lactate greater than 2 mmol/l and hypotension requiring vasopressors
5 SCREENING TOOLS Sequential Organ Failure Assessment score (SOFA) and Multiple Organ Dysfunction Syndrome score (MODS) Measure severity of organ dysfunction Describes how a patients status changes over time Acute Physiology and Chronic Health Evaluation II score (APACHE II score) Measure severity of disease in patients admitted to ICU Describes morbidity and can be used to predict mortality Simplified Acute Physiology Score II (SAPS II) Measure severity of disease in patients admitted to ICU Predicts mortality
6 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions

7
8 INFLAMMATION AND CLOTTING Both an integral part of a normal immune response Immune system and coagulation system are evolutionarily linked Activate, and interact with each other Clotting restricts the spread of infection Inflammation increases blood flow to the site of infection (vasodilation), and allows for leakage of fluid from the blood vessels into damaged/infected tissue (vascular permeability) During a normal immune response, these processes are highly regulated and balanced to maintain localized effects and homeostasis Pro and anti-inflammatory mediators Coagulants and anticoagulants In Sepsis, there is a dysregulation of the normal immune response

9 Inflammation and coagulation
10 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
11 UNCOMPLICATED INFECTION VS SEPSIS The exact reason why uncomplicated infections turn in to sepsis is unknown, but likely multifactorial Pathogen factors: toxin production (exotoxins), bacterial structure (endotoxin) Host factors: age, gender, susceptibility to infection, genetic susceptibility, site of infection, etc. Pneumonia is the most common source accounting for 50% of cases Organisms involved in sepsis have changed over time In many cases an organism cannot be identified on cultures
12 SEPSIS AND ORGAN DYSFUNCTION Caused by direct cellular injury or impairment of tissue oxygenation Impaired tissue oxygenation Macrovascular causes: vasodilation results in hypotension and less oxygenated blood getting to organs Microvascular causes: imbalance in coagulation pathways results in clot formation in the microvasculature Direct cellular injury Nitric oxide released by endothelium can result in free radical production Anaerobic metabolism results in less ATP formation Critical point is reached where energy production doesn t meet demand Cell Death Lactate associated with anaerobic metabolism
13 SEPSIS: GENERAL APPROACH TO TREATMENT Time = Life For each hour therapy is delayed mortality increases 8% Source control Drain abscess, remove infected hardware, etc. Broad spectrum antibiotics Narrow regimen as cultures return Supportive care Fluids and Inotropes Ventilation Continuous Renal Replacement Therapy (CRRT)
14 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
15 ANTICOAGULATION Sepsis represents a pro-coagulant state with profound deficiencies in circulating endogenous anticoagulants Clots formed in the microvasculature can contribute to organ failure Certain anticoagulants have been shown to have anti-inflammatory properties Eg. Heparin neutralizes endotoxin, and inhibits TNF-alpha (increases protein binding)
16 ACTIVATED PROTEIN C One of the first agents that showed a mortality benefit in patients with septic shock (2001) Activated protein C (drotecogin alpha, APC) In its activated form, Protein C has antithrombotic, pro-fibrinolytic, and anti-inflammatory properties In sepsis, protein C levels are depleted, and conversion to activated form is impaired PROWESS study (2001)- consistent mortality benefit, regardless of age, sex, site of infection, severity of illness, etc. Subsequent studies failed to reproduce results, and showed an increase risk of bleeding APC voluntarily withdrawn from market by manufacturer in 2011
17 ACTIVATED PROTEIN C: NEW BEGINNINGS? SCARLET-2 a phase 3, randomized, double blind, placebo controlled study Still in approval process. Hope to start enrolling patients early 2019, and complete trial by 2022 Will study mortality benefits of ART-123 (Thrombomodulin alpha) vs placebo in septic shock Thrombomodulin is a cofactor in the process of converting protein C to its activated form Previous trials have compared ART-123 vs Heparin for Disseminated Intravascular Coagulopathy (DIC) Statistically significant increase in resolution of DIC
18 HEPARIN Early Intravenous Unfractionated Heparin and Mortality in Septic Shock Published 2008 Retrospective study on adult patients admitted for septic shock to Winnipeg ICU s between During this time period total patients were admitted Of these 2912 met 1991 criteria for septic shock Patients were further excluded if they died within 48 hours, received heparin > 48 hours after admission, or had mixed shock states (cardiogenic, hemorrhagic, obstructive, etc) Final study cohort was 2326 patients 1604 did not receive therapeutic heparin Control 722 received therapeutic heparin Intervention
19
20 HEPARIN Baseline characteristics: Treatment group: lower APACHE II scores, older, more likely to have COPD, CHF, diabetes Control group: higher APACHE II scores, higher incidence of liver failure, neutropenia, and lower platelet counts Propensity matching was performed to attempt to eliminate baseline bias between the two groups Suitable matches were found for 695(96%) of treatment group
21
22 HEPARIN Baseline characteristics: Treatment group: lower APACHE II scores, older, more likely to have COPD, CHF, diabetes Control group: higher APACHE II scores, higher incidence of liver failure, neutropenia, and lower platelet counts Propensity matching was performed to attempt to eliminate baseline bias between the two groups Suitable matches were found for 695(96%) of treatment group Primary outcome was 28 day mortality Reduction in mortality treatment group (40.1%) vs control (44.2%) Hazard ratio 0.85, 95% CI: P: 0.05 For patients with the highest APACHE II scores absolute reduction in mortality of 13% Hazard raio 0.70, 95% CI: , P: 0.01
23 HEPARIN Secondary outcomes Statistically significant reduction in vasopressor requirements, and were more likely to be liberated from mechanical ventilation, but median length of hospital stay was longer Safety: no significant difference in rate of GI bleed, CNS bleed, or need for transfusions Conclusions: Early administration of therapeutic doses of heparin may be associated with reduced mortality over 28 days. Reduction in mortality is more pronounced with increasing severity of illness
24 HEPARIN: HETRASE TRIAL Unfractionated Heparin for Treatment of Sepsis: A Randomized Clinical Trial HETRASE Trial Published in 2009 Single center, randomized, double blind, placebo control study with 319 patients Intervention Unfractionated heparin infusion at 500 units/hr for 7 days Control Placebo infusion Primary outcomes: Length of hospital stay (discharged alive) Change from baseline Multiple Organ Dysfunction (MOD) score
25 HEPARIN: HETRASE TRIAL Inclusion Criteria Adult patients coming in to ER Main reason for admission was suspected or confirmed infection Exclusion Criteria Pregnancy Increased risk of bleeding Requirement for anticoagulation Transplantation > 24 hours of admission to the hospital No significant differences between treatment and control groups at baseline
26
27 HEPARIN: HETRASE TRIAL Primary outcomes Median length of stay was 12.5 days for treatment group, and 12 days for placebo No statistically significant difference Hazard ratio 1.04, 95% CI: No statistical difference in decline in MOD score Secondary outcomes 28 day mortality: no statistically significant difference Safety 2 episodes of minor bleeding in each group 1 episode of serious bleeding (GI bleed)
28
29 HEPARIN Difference between retrospective Winnipeg study and HETRASE Dose used: Treatment dose vs. 500 Units/hr HETRASE patients had less severe illness Lower APACHE II score, younger, 50% had no comorbidities Future/Current study: Heparin Anticoagulation to Improve Outcomes in Septic Shock: HALO study Multi center, randomized, open label study (phase 2) IV heparin infusion at 18 units/kg/hr vs. Control of standard DVT prophylaxis Will include patients with a high severity of illness Primary outcome: Number of vasopressor free days Secondary outcome: 90 day mortality, ICU mortality Hopes to be completed by 2020
30 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
31 STEROIDS IN SEPSIS The use of steroids in sepsis has several theoretical benefits Increase transcription of anti-inflammatory cytokines Decrease transcription of pro-inflammatory cytokines Inhibit platelets Inhibit Nitric Oxide Enhances vasculatures responsiveness to vasopressors However, the evidence supporting the use of steroids in sepsis is controversial Studies dating as far back as the 1960 s Wide range of results (significant improved outcome vs. potential harm) Steroid use has fallen in and out of favour as a result
32 STEROIDS IN SEPSIS: HISTORY Early trials done in the 1960 s-1970 s Used large doses of methylprednisolone (30mg/kg) or dexamethasone (3mg/kg) Bolus dose at time of diagnosis. Could be repeated in 4 hours Mortality rates 10.4% in steroid groups vs 38.4% in placebo group Based on this evidence, high dose methylpred administered at the onset of septic shock became standard practice High dose methylpred revisited in the 1980 s (various trials) No difference in mortality/higher mortality seen in steroid groups Potential adverse effects and higher rate of secondary infections High dose steroid use fell out of practice
33 STEROIDS IN SEPSIS: HISTORY Series of trials in the 1990 s Used hydrocortisone instead of methylpred Much smaller doses ( mg/day of hydrocortisone) Showed quicker reversal of shock, potentially showed improvement in mortality Small studies (40 patients) that prompted larger studies in the 2000 s Annane trial (French trial) in 2002 Multicenter, double-blind, placebo controlled trial with 300 patients Treatment arm: hydrocortisone 50mg IV q6h + Fludrocortisone 50 mcg po daily for 7 days
34
35 STEROIDS IN SEPSIS: HISTORY Annane trial ctd. All patients given ACTH stim test, classified as either having adequate or inadequate adrenal reserve (non responders) Adequate adrenal reserve: change in cortisol > 248 nmol/l Non-responders: change in cortisol <248 nmol/l No mortality difference noted 28 day mortality (53% v 63%), ICU mortality (58% vs 70%), and hospital mortality (61% vs 72%), and duration of shock all lower in non responders receiving hydrocortisone No difference in mortality at 1 year No difference in adverse effects Conclusion: Low dose corticosteroids reduced mortality rates in patients with evidence of relative adrenal insufficiency (non responders in ACTH stim test)
36 STEROIDS IN SEPSIS: HISTORY CORTICUS trial 2008 Multicenter, randomized, double-blinded, placebo controlled study with 499 patients Underpowered: only 499 out of the intended 800 Treatment arm: Hydrocortisone 50mg IV q6h for 5 days, then tapered off over 6 days (11 days total) No statistical difference in 28 day mortality ACTH stim test done on all patients No statistical difference even for ACTH non-responders CORTICUS vs French trial French trial had patients that were more sick French trial enrolled patients within the first 8 hours of diagnosis, vs 72 hours in CORTICUS missed window of opportunity?

37
38 STEROIDS: ADRENAL TRIAL Adjunctive Glucocorticoid Therapy in Patients With Septic ShockADRENAL trial Published in March of 2018 Multicenter, randomized, double-blind, placebo controlled trial with 3658 patients 3800 patients enrolled, 142 (3.7%) withdrew/lost to follow up Primary outcome was 90 day mortality with an intention-to-treat analysis Intervention Hydrocortisone 200mg/day administered as a continuous infusion for 7 days or until ICU discharge Control Placebo infusion No statistical difference in baseline characteristics of control group and treatment group

39
40 STEROIDS: ADRENAL TRIAL Inclusion Criteria Age 18 years Mechanical ventilation Strong clinical suspicion of infection 2 SIRS criteria Continuous vasopressor for SBP 90mmHG or MAP 60mmHG for 4 hours Exclusion Criteria Met all inclusion criteria >24 hours ago Corticosteroid use for other indication Treatment with Etomidate or Amphotericin B Death deemed inevitable or imminent, or death from underlying disease likely within 90 days Cerebral malaria or strongloides infection
41 ADRENAL: RESULTS Primary outcome: no statistical difference in 90 day mortality (OR: 0.95, CI: , p = 0.50) Six subgroups were also analyzed: 1. admission type (surgical vs medical), 2. Site of sepsis (pulmonary vs non pulmonary) 3. Sex 4. Duration of shock before enrollment 5. APACHE II score 6. Dose of vasopressors No significant differences in mortality between subgroups
42 ADRENAL: RESULTS Primary outcome: no statistical difference in 90 day mortality (OR: 0.95, CI: , p = 0.50) Six subgroups were also analyzed: 1. admission type (surgical vs medical), 2. Site of sepsis (pulmonary vs non pulmonary) 3. Sex 4. Duration of shock before enrollment 5. APACHE II score 6. Dose of vasopressors No significant differences in mortality between subgroups Secondary outcomes: Treatment group had faster reversal of shock, time to initial extubation, and discharge from ICU No significant difference in rate of shock recurrence, total time alive off ventilator, and hospital discharge Treatment group needed fewer blood transfusions
43 ADRENAL: RESULTS Secondary outcomes: No statistical difference between groups in 28 day mortality, need for renal replacement therapy, and incidence of new-onset bacteremia/fungemia Adverse events: Significantly greater in treatment group (1.1% vs 0.3%) Hyperglycemia 6 vs 3, Hypernatremia 3 vs 0, Encephalopathy 3 vs 0 Serious adverse events 4 events in treatment group: 2 myopathy, 1 Ischemic bowel, 1 Circulatory shock 2 events in placebo group: 1 bleeding, 1 wound dehiscence
44
45 ADRENAL CONCLUSIONS Among patients with septic shock undergoing mechanical ventilation, a continuous infusion of hydrocortisone did not result in lower 90-day mortality than placebo Criticisms: Antibiotic therapy was recorded but appropriateness based on culture results was not Infusion vs intermittent dosing of hydrocortisone Some patients received open label steroids (7.4% and 8.8%) Clinician reported adverse events Didn t monitor for secondary infections other than bacteremia/fungemia Did not check for long term neuromuscular weakness
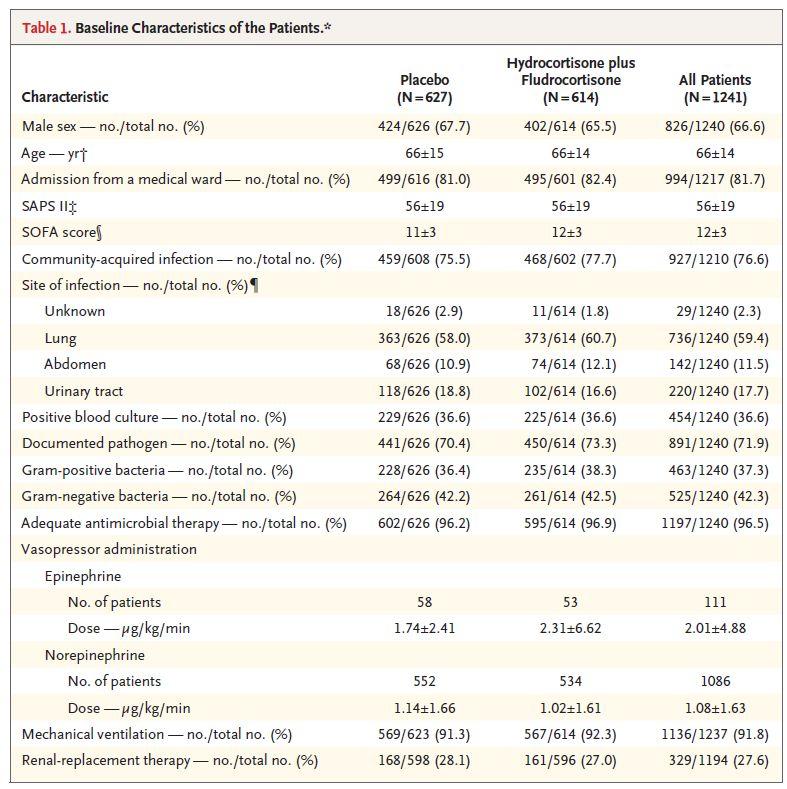
46 APROCCHSS TRIAL Hydrocortisone Plus Fludrocortisone for Adults With Septic Shock APROCCHSS TRIAL (French 2, Annane 2) Published March of 2018 Multicentre, randomized, double-blinded, placebo controlled study 1241 patients enrolled Intervention/Control Originally, study was designed to have 4 parallel groups to evaluate benefits/risks of steroids and APC given alone or in combination via 2 by 2 factorial design Steroids + APC Steroids + Placebo APC + Placebo Placebo + Placebo
47 APROCCHSS TRIAL Intervention/Control APC was withdrawn from the market during the trial Subsequent analysis was performed to show no interaction between APC and other treatment elements Use of APC was suspended and groups were combined Intervention Infusion 1: Hydrocortisone 50 mg IV q6h x 7 days Infusion 2: Placebo or APC Enteral: Fludrocortisone 50 mcg daily x 7 days Control Infusion 1: Placebo Infusion 2: Placebo or APC Enteral: Placebo Primary outcome was 90 day mortality with an intention to treat analysis
48 APROCCHSS TRIAL No statistical differences in baseline criteria between groups Inclusion criteria Admitted to ICU for < 7 days Indisputable or probable septic shock <24 hours Presence of clinically or microbiologically documented infection Sofa Score of 3-4 for 2 organ systems for 6 consecutive hours Vasopressor therapy for 6 hours Exclusion criteria Septic shock > 24 hours High risk of bleeding (eg. Recent surgery) Pregnancy or lactation Previous treatment with corticosteroids Underling conditions that could affect short-term survival Known hypersensitivity to activated drotrecogin alfa (APC)
49
50 APROCCHSS: RESULTS Primary outcome: Statistically significant reduction in 90 day mortality with intervention Intervention 43% vs Control 49.1% Relative Risk: 0.88, 95% CI: , p: 0.03 Absolute Risk Reduction: 6.1% CI: 0.6% %, p: 0.03 NNT: 17 Secondary outcomes: Statistically significant reduction with intervention for: mortality at ICU/hospital discharge, mortality at 180 days, vasopressor free days, organ failure free days, weaning from vent and vasopressors at 28 days No statistical difference: 28 day mortality, safety outcomes/incidence of serious adverse events

51
52 APROCCHSS: CONCLUSIONS In critically ill patients with septic shock, the addition of hydrocortisone and fludrocortisone compared to placebo was associated with a significant improvement in mortality at 90 days. Criticisms Fragility Index = 3 No survival benefit at 28 days, but benefit at 90 days Withdrawal of APC Underpowered Used old sepsis guidelines to guide treatment
53 APROCCHSS VS. ADRENAL Patients in the APROCCHSS (French 2) trial were more ill at time of enrollment Higher vasopressor requirements and higher SAPS II scores ADRENAL trial used continuous infusion of hydrocortisone APROCHSS trial used Fludrocortisone APROCHSS trial had fewer surgical patients More pneumonia related sepsis rather than intraabdominal sepsis in ADRENAL Benefit of steroids depending on cause/source of infection?
54 STEROIDS: WHAT HAVE WE LEARNED? High dose steroids are likely not beneficial and potentially harmful Low dose steroids result in faster resolution of shock and liberation from mechanical ventilation does this even matter? Weak evidence to suggest benefit of steroids in patients who have a non surgical source of infection Weak evidence to suggest benefit of steroids in patients with septic shock who have a high severity of illness (high mortality risk) Surviving Sepsis Guidelines Avoid steroids in the absence of shock Avoid steroids if fluids/vasopressors can restore hemodynamic stability Hydrocortisone 200 mg/day if this is unachievable Kitchen Sink scenarios Acknowledges low quality of evidence to support this practice
55 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
56 VITAMIN C: A CURE FOR SEPSIS? Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock Published February of 2017 (Marik Trial) Theory: Vitamin C acts as an anti-oxidant, and down regulates the production of pro-inflammatory mediators. Prevents free radical related organ damage Acts synergistically with steroids on the anti-inflammatory cascade Thiamine helps prevent oxalate crystallization, a by-product of high dose Vitamin C (can lead to renal failure) Critically ill patients are often deficient in vitamin C and thiamine
57 VITAMIN C: A CURE FOR SEPSIS? Single center, unblinded, retrospective before-after study, with historical controls (Eastern Virginia Medical School ICU) 47 patients in treatment arm compared to 47 historical controls Intervention Vitamin C 1.5 g IV q6h for 4 days or ICU discharge Dosage devoid of any complications or side effects Thiamine 200 mg IV q12h for 4 days Hydrocortisone 50 mg IV q6h for 7 days or ICU discharge, followed by 3 day taper Control Standard sepsis treatment Of note, 60% of historical controls had received hydrocortisone as part of standard treatment
58 VITAMIN C: A CURE FOR SEPSIS? Primary outcome: hospital survival Inclusion criteria Consecutive patients admitted to Eastern Virginia Medical School Critical Care Unit Primary diagnosis of severe sepsis or septic shock Procalcitonin level 2 ng/ml Exclusion criteria <18 years of age Pregnant Patients with limitations of care No statistical differences between treatment group and controls

59
60 VITAMIN C: RESULTS Primary outcome: Statistically significant decrease in hospital mortality in treatment group 8.5% (4 of 47) vs 40.4% (19 of 47) Odds ratio of 0.13, 95% CI: , p: Per the Authors: Of the 4 patients that did pass away, they all died from underlying disease and NOT sepsis Advanced dementia, heart failure, sarcoidosis, COPD All survived ICU care Secondary outcomes: Treatment group had significantly lower duration of vasopressor therapy, and requirement for renal replacement therapy Treatment group had greater improvement in SOFA score, and procalcitonin clearance in the first 72 hours
61
62 VITAMIN C Conclusion: The early use of IV vitamin C with corticosteroids and thiamine may prove to be effective in preventing progressive organ dysfunction, and reducing mortality of patients with severe sepsis and septic shock Criticisms Potential bias: Single centre study, historical controls, unblinded Treatment and Control period not concurrent and not during same season (Late winter-summer vs Fall-early winter) Small Sample size 60%Control group received part of treatment (steroids) Multiple interventions used A hypothesis generating study at best with further need for RCTs
63 VITAMIN C Study in Korea using Marik protocol (2018) Single center, unblinded, retrospective before-after study, with historical controls Patients admitted to ICU with community acquired pneumonia (treatment = 53 patients, control = 46) No statistical difference in mortality between groups Propensity matching was performed to help eliminate bias from baseline group characteristics 17% (6 of 36) mortality in treatment group vs 39% (14 of 36) mortality in propensity matched historical controls OR 0.31, 95% CI , p = 0.04 No statistical difference in change in SOFA score Majority of the same criticisms apply as to the original Marik trial
64 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
65 OTHER THERAPIES BEING INVESTIGATED Beta-blockade Patients with sepsis often remain tachycardic can result in myocardial damage, inefficient pump Tachycardia associated with mortality Esmolol has been shown to increase survival, while not influencing hemodynamics Cytokine and endotoxin inactivation or removal Hemoperfusion through adsorptive materials eg. Polymixin B fiber column Plasma exchange IVIG Inhibition of innate immune system Eg. Eritoran, TLR-4 antagonist Statins
66 FAILED TREATMENT APPROACHES Inhibition of innate immune system TLR-4 (PRR) antagonist TAK-242 Anti-endotoxin antibody HA-1A TNF-alpha antibody, IL-1 receptor antagonists Preventing Organ Failure Nitric oxide inhibitors prevent vasodilation and free radical production N-acetylcysteine antioxidant Therapeutic Hypothermia Ibuprofen Activated protein C
67 OUTLINE Review Definition of Sepsis Immune System Sepsis Pathophysiology Anticoagulation Steroids: The Great Debate Vitamin C: A Cure for Sepsis? Other Therapies Being Investigated Failed Treatment Approaches Example Case/Questions
68 EXAMPLE CASE Patient L.S. is a 75 year old African American male with a past medical history of ESRD requiring renal transplant, diabetes, and hypertension. He presents to the ER with a 3 day history of productive cough, fever, chills, and shortness of breath. L.S. is diagnosed with community acquired pneumonia and admitted. What are some L.S. s risk factors for having an uncomplicated CAP turn in to sepsis? Mr. Worst Case Scenario Age, gender, ethnicity, comorbidities, immune suppression, pneumonia as admission diagnosis.
69 EXAMPLE CASE L.S. quickly deteriorates on the medical ward. He becomes anuric, hypotensive, and needs to be intubated for extreme SOB and falling O2 sats. L.S. is taken to the ICU with an updated diagnosis of septic shock. In ICU his blood pressure is stabilized after several fluid bolus and a low dose of norepinephrine infusion. The ICU physician asks your opinion on starting this patient on stress dose steroids for sepsis. How do you respond? Steroids not appropriate at this time as patient is hemodynamically stable with use of fluid bolus and vasopressors.
70 EXAMPLE CASE L.S. course in the ICU takes a dramatic turn for the worse. Despite maximal doses of multiple vasopressors, L.S. s blood pressure continues to plummet. The topic of steroids is raised again. How do you respond? Steroids would not be unreasonable, based on hypotension refractory to vasopressors. (Weak evidence) The ICU physician also recently read an article about using high dose Vitamin C in sepsis. Would it be appropriate to start L.S. on the Marik protocol? Evidence based answer: no, not enough quality evidence to support its use Anecdotal answer:..
71 THE END THANK YOU!
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Top Sepsis Studies
 A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes
 Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes Matt Anderson, MD USD SSOM, Clinical Assistant Professor Regional Health, Critical Care Medicine mjanderson972@gmail.com Disclosure(s)
Updates in Critical Care Sepsis, Fluids, Epi and Long-Term Outcomes Matt Anderson, MD USD SSOM, Clinical Assistant Professor Regional Health, Critical Care Medicine mjanderson972@gmail.com Disclosure(s)
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA
 DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Novel Sepsis Therapies
 RSEM-GSA 17 Novel Sepsis Therapies Khaled Ahmed Alghamdi, MD, ABEM, FACEP, FAAEM Consultant Emergency Medicine Deputy program director Medical Director of Emergency Medical Services King Faisal Specialist
RSEM-GSA 17 Novel Sepsis Therapies Khaled Ahmed Alghamdi, MD, ABEM, FACEP, FAAEM Consultant Emergency Medicine Deputy program director Medical Director of Emergency Medical Services King Faisal Specialist
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital.
 Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital. Aryan J. Rahbar, University Medical Center of Southern Nevada Marina Rabinovich, Emory
Outcomes after administration of drotrecogin alfa in patients with severe sepsis at an urban safety net hospital. Aryan J. Rahbar, University Medical Center of Southern Nevada Marina Rabinovich, Emory
BLOOD COAGULATION AND INFLAMMATION IN SEPSIS. A NEW CHALLENGE. Antonio Artigas Critical Center Sabadell Hospital Autonomous University of Barcelona
 BLOOD COAGULATION AND INFLAMMATION IN SEPSIS. A NEW THINKING AND THERAPEUTIC CHALLENGE Antonio Artigas Critical Center Sabadell Hospital Autonomous University of Barcelona SEVERE SEPSIS PATHOPHYSIOLOGY
BLOOD COAGULATION AND INFLAMMATION IN SEPSIS. A NEW THINKING AND THERAPEUTIC CHALLENGE Antonio Artigas Critical Center Sabadell Hospital Autonomous University of Barcelona SEVERE SEPSIS PATHOPHYSIOLOGY
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Drug intervention trials in sepsis Armand R.J. Girbes
 Drug intervention trials in sepsis Armand R.J. Girbes Professor in Intensive Care Medicine Clinical Pharmacologist VU medical center Amsterdam, NL Sepsis - definition Sepsis Epidemiology 50-95 cases per
Drug intervention trials in sepsis Armand R.J. Girbes Professor in Intensive Care Medicine Clinical Pharmacologist VU medical center Amsterdam, NL Sepsis - definition Sepsis Epidemiology 50-95 cases per
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
New approaches to the treatment of sepsis
 Clin Chest Med 24 (2003) 521 548 New approaches to the treatment of sepsis James M. O Brien, Jr, MD*, Edward Abraham, MD Division of Pulmonary Sciences and Critical Care Medicine, University of Colorado
Clin Chest Med 24 (2003) 521 548 New approaches to the treatment of sepsis James M. O Brien, Jr, MD*, Edward Abraham, MD Division of Pulmonary Sciences and Critical Care Medicine, University of Colorado
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Sepsis Pathophysiology
 Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Sepsis Pathophysiology How Kids Differ From Adults Steve Standage Pediatric Critical Care Medicine Seattle Children's Hospital University of Washington School of Medicine Disclosures & Preamble No agenda,
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis. Deborah Cook
 Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Endothelium as a part of septic Multiple Organ Dysfunction Syndrome (MODS)-is endocan an answer?
-is endocan an answer?") Endothelium as a part of septic Multiple Organ Dysfunction Syndrome (MODS)-is endocan an answer? Małgorzata Lipinska-Gediga Department of Anaesthesiology and Intensive Therapy Medical University Wroclaw,
Endothelium as a part of septic Multiple Organ Dysfunction Syndrome (MODS)-is endocan an answer? Małgorzata Lipinska-Gediga Department of Anaesthesiology and Intensive Therapy Medical University Wroclaw,
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Text-based Document. Implications of the Sepsis-3 Definition on Nursing Research and Practice. Authors Peach, Brian C. Downloaded 5-Jul :03:48
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Usefulness of Sepsis Biomarkers. Dr Vineya Rai Department of Anesthesiology University of Malaya
 The Usefulness of Sepsis Biomarkers Dr Vineya Rai Department of Anesthesiology University of Malaya 1 What is Sepsis? Whole Body Inflammatory State + Infection 2 Incidence and Burden of Sepsis in US In
The Usefulness of Sepsis Biomarkers Dr Vineya Rai Department of Anesthesiology University of Malaya 1 What is Sepsis? Whole Body Inflammatory State + Infection 2 Incidence and Burden of Sepsis in US In
Assessing Adrenal Function in Ill, Hospitalized Patients. Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism
 Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
A BRIEF HISTORY OF SEPSIS. Euan Mackay
 A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK
 THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK Older people carry the burden of sepsis Older people carry the burden of sepsis Immunosenescence Co-morbidity Endothelial / mucosal atrophy Dependence
THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK Older people carry the burden of sepsis Older people carry the burden of sepsis Immunosenescence Co-morbidity Endothelial / mucosal atrophy Dependence
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Update on Sepsis Diagnosis and Management
 CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
CHAPTER 12 Update on Sepsis Diagnosis and Management Kevin Alexander, DPM INTRODUCTION Sepsis and septic shock have become a large problem in the health care system that affects at least 1 million people
pat hways Medtech innovation briefing Published: 29 November 2016 nice.org.uk/guidance/mib87
 pat hways CytoSorb therapy for sepsis Medtech innovation briefing Published: 29 November 2016 nice.org.uk/guidance/mib87 Summary The technology described in this briefing is CytoSorb therapy. It is an
pat hways CytoSorb therapy for sepsis Medtech innovation briefing Published: 29 November 2016 nice.org.uk/guidance/mib87 Summary The technology described in this briefing is CytoSorb therapy. It is an
Top 5 (Topics) Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008
 Papers In GIM Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008") Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
Top 5 (Topics) Papers In GIM 2008 Rocky Mountain ACP Internal Medicine Meeting Raj Padwal November 13, 2008 Methods Searched ACPJC/EBM, TOC of top medical journals, MEDSCAPE Best Evidence, consultation
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
SEPSIS-3: THE NEW DEFINITIONS
 SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine