ISCHEMIC STROKE & TIA main etiologies
|
|
|
- Alannah Norman
- 5 years ago
- Views:
Transcription
1 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון
2 תאריך בדיקה
3 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease - atherothromboembolism Cardiac source of embolism Small vessel (artery) disease
4 LARGE ARTERY DISEASE pathophysiology of ischemic insults Thrombo-embolism originating from an atheromatous, ulcerated plaque Thrombosis in situ at the site of the stenosed (by plaques) artery leading to occlusion Critical diminishing blood flow distal to a severely stenosed artery
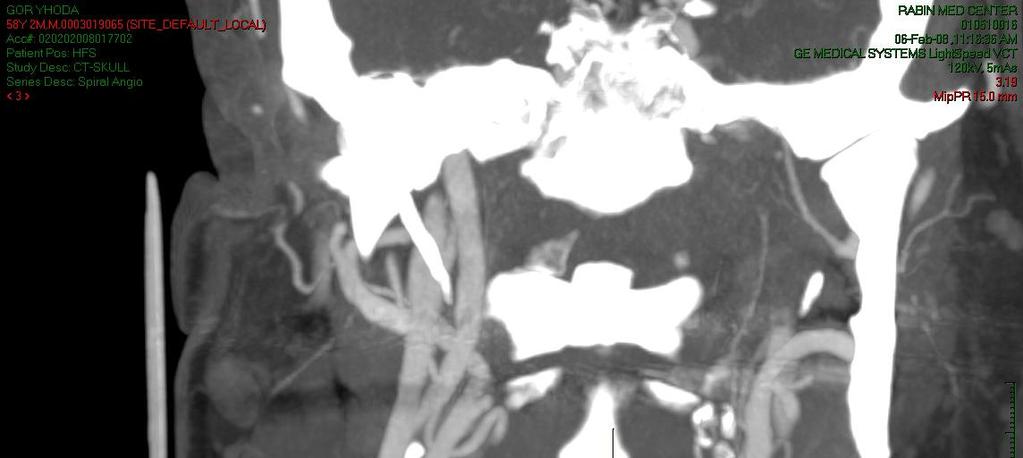




5 CT Angiography Carotid occlusion Carotid stenosis + ulcer
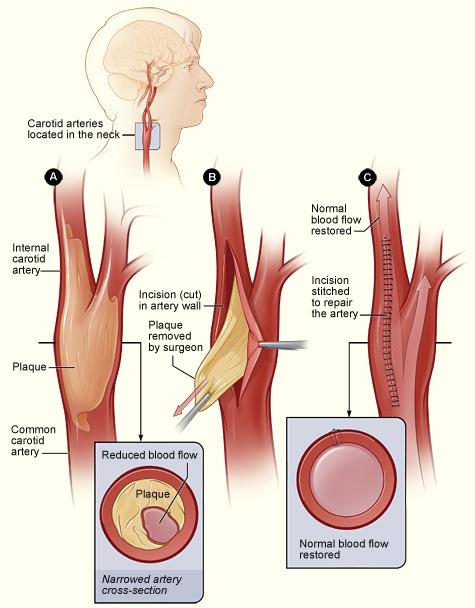
6 Carotid endarterectomy
 Barnett, H. J.M.")
7 Kaplan-Meier survival curves showing probability of surviving severe symptomatic carotid stenosis in NASCET (1991) Barnett, H. J.M. Stroke 2009;40:e53-e65
8 Kaplan-Meier survival curves to show survival free of major stroke in surgery and control patients with 80 99% stenosis in ECST (1991) (non-stroke deaths occurring more than 30 days after surgery censored) ECST collaborators, Lancet 1998;351:

9
10 Risk factors associated with symptomatic carotid stenosis Severity of the stenosis Time of symptoms Hemispheric TIA s (vs. retinal TIA s) Intracranial stenosis, No collateral circulation Contralateral carotid occlusion Plaque ulceration Presence of leukoaraiosis
 Lancet")
11 5 year risk Rothwell P. M. (based on ECST) Lancet 2005;365:256-65

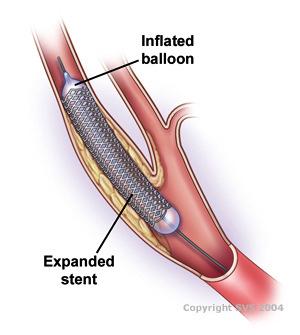


12 CAROTID STENTS & PROTECTIVE DEVICES
13 ICSS interim: meta- analysis CEA vs. stent Lancet 2.10
14 CREST - Primary End Point*, According to Treatment Group Symptomatic & asymptomatic Pts. * Stroke + periprocedural MI & death Brott T et al. N Engl J Med 2010; /NEJMoa
15 ICSS long-term outcome Courtesy of Prof. Martin Brown, UCL & Queen Square, London U.K.
16 Conclusions Carotid endarterectomy remains the treatment of choice for symptomatic carotid stenosis Rates of long-term stroke are low after both treatments ICSS results, ESC Lisbon 5.12
17 Cumulative Proportions of Patients with the Primary Composite End Point, Stroke or Death, and Any Stroke, According to Treatment Group. CREST (Symptomatic & asymptomatic Pts.) - long term follow-up Brott TG et al. N Engl J Med 2016.
18 הצרות קרוטידית אסימפטומטית Asymptomatic significant (>50%) carotid stenosis (ASCS) - גישה טיפולית
19 Prevalence of ASCS ( 50% stenosis) 4.2% in total 9.3% in people 70 years de Weerd, M. et al. Stroke 2009;40:
20 ASCS estimated annual risks of vascular events Stroke 2% Coronary events 7% Stroke mortality 0.6% Overall mortality 4-7%
21 ACAS: Carotid endarterectomy in asymptomatic men p= NS p= patients with an asymptomatic carotid stenosis 60 %. randomized to medical therapy with aspirin or CEA. mean follow up 2.2 years. Executive Committee for the Asymptomatic Carotid Atherosclerosis Trial. JAMA 1995; 273:1421.
22 ACST Asymptomatic Carotid Surgery Trial results Any type of stroke or perioperative death P< Fatal or disabling stroke or perioperative death P= ACST collaborators, Lancet 2004;363:
23 ACST 10 years follow up Of 3120 patients: % have died - 90% non stroke death Risk of stroke and peri-operative (PO) death: - Immediate surgery 13.4% - Deferred surgery 17.9% Peri-operative complications: Stroke, MI or death 3.2% Disabling stroke or death 1.7% Sept. 2008
24 Meta-analysis of ipsilateral stroke (including any stroke within 30 days) in RCTs and NRCSs of CEA versus medical therapy. Annual ipsilateral stroke risk on medical therapy = 1.68% Raman G, et al Ann Intern Med. 2013;158(9):
25 Temporal changes in the annual ipsilateral stroke risk in patients with ASCS treated medically. Naylor AR, Bell PRF, Semin Vasc Surg 2008;21:100-7

26 Use of medical treatments in the ACST study The use of lipid lowering drugs rose from 17 to 58% in last randomization period. Patient numbers reflect year of randomization. ACST collaborators, Lancet 2004;363:

27 Pleiotropic effect of statins on the vasculature DeGraba, T. J. Stroke 2004;35: Statins therapy was shown to arrest/ regress carotid atherosclerosis progression in randomized controlled trials Kang S. et al, Atherosclerosis 2004;177:433-42
28 Guidelines
29 Patients with high risk of stroke, i.e. men with stenosis of more than 80% and a life expectancy of more than 5 years, may derive some benefit from surgery in appropriate centers, i.e. peri-operative complications of less than 3% Chambers & Donnan, Cochrane Database 2005
30 Carotid endarterectomy--an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. For asymptomatic patients with 60 to 99% stenosis, the benefit/risk ratio is smaller compared to symptomatic patients and individual decisions must be made. Endarterectomy can reduce the future stroke rate if the perioperative stroke/death rate is kept low (<3%). Neurology Sep 27;65(6):
31 ESVS guidelines. Invasive treatment for carotid stenosis: indications, techniques, CEA is (also) recommended in asymptomatic men <75 years old with 70-99% stenosis if the perioperative stroke/death risk is <3%. The benefit from CEA in asymptomatic women is significantly less than in men. CEA should therefore be considered only in younger, fit women. The European Society for Vascular Surgery Eur J Vasc Endovasc Surg Apr;37(4 Suppl):1-19
32 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Recommendations for Selection of Patients for Carotid Revascularization Class I 3. Selection of asymptomatic patients for carotid revascularization should be guided by an assessment of comorbid conditions, life expectancy, and other individual factors and should include a thorough discussion of the risks and benefits of the procedure with an understanding of patient preferences. (Level of Evidence: C) Class IIa 1. It is reasonable to perform CEA in asymptomatic patients who have more than 70% stenosis of the internal carotid artery if the risk of perioperative stroke, MI, and death is low. (Level of Evidence: A)
33 Asymptomatic Carotid Stenosis: Recommendations 1. Patients with asymptomatic carotid stenosis should be prescribed daily aspirin and a statin. Patients should also be screened for other treatable risk factors for stroke, and appropriate medical therapies and lifestyle changes should be instituted (Class I; Level of Evidence C). 2. In patients who are to undergo CEA, aspirin is recommended perioperatively and postoperatively unless contraindicated (Class I; Level of Evidence C). 3. It is reasonable to consider performing CEA in asymptomatic patients who have >70% stenosis of the internal carotid artery if the risk of perioperative stroke, MI, and death is low (<3%). However, its effectiveness compared with contemporary best medical management alone is not well established (Class IIa; Level of Evidence A). Guidelines for the Primary Prevention of Stroke : A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association Stroke.2014; 45:
34 Asymptomatic Carotid Stenosis: Recommendations - continue 4. It is reasonable to repeat duplex ultrasonography annually by a qualified technologist in a certified laboratory to assess the progression or regression of disease and response to therapeutic interventions in patients with atherosclerotic stenosis >50% (Class IIa; Level of Evidence C). 5. Prophylactic CAS might be considered in highly selected patients with asymptomatic carotid stenosis (minimum, 60% by angiography, 70% by validated Doppler ultrasound), but its effectiveness compared with medical therapy alone in this situation is not well established (Class IIb; Level of Evidence B). 6. In asymptomatic patients at high risk of complications for carotid revascularization by either CEA or CAS, the effectiveness of revascularization versus medical therapy alone is not well established (Class IIb; Level of Evidence B). 7. Screening low-risk populations for asymptomatic carotid artery stenosis is not recommended (Class III; Level of Evidence C).



35 Algorithm for the management of extracranial carotid artery disease. The European Society of Cardiology Tendera M et al. Eur Heart J 2011;32:
36 7.1. Recommendations for Selection of Patients for Carotid Revascularization* Class I 1. Patients at average or low surgical risk who experience nondisabling ischemic stroke or transient cerebral ischemic symptoms, including hemispheric events or amaurosis fugax, within 6 months (symptomatic patients) should undergo CEA if the diameter of the lumen of the ipsilateral internal carotid artery is reduced more than 70% as documented by noninvasive imaging (Level of Evidence: A) or more than 50% as documented by catheter angiography (Level of Evidence: B) and the anticipated rate of perioperative stroke or mortality is less than 6%. 2. CAS is indicated as an alternative to CEA for symptomatic patients at average or low risk of complications associated with endovascular intervention when the diameter of the lumen of the internal carotid artery is reduced by more than 70% as documented by noninvasive imaging or more than 50% as documented by catheter angiography and the anticipated rate of periprocedural stroke or mortality is less than 6%. (Level of Evidence: B) ASA, AANN, AHA, etc guidelines
37 Class IIa 2. It is reasonable to choose CEA over CAS when revascularization is indicated in older patients, particularly when arterial pathoanatomy is unfavorable for endovascular intervention (Level of Evidence: B) 3. It is reasonable to choose CAS over CEA when revascularization is indicated in patients with neck anatomy unfavorable for arterial surgery. (Level of Evidence: B) 4. When revascularization is indicated for patients with TIA or stroke and there are no contraindications to early revascularization, intervention within 2 weeks of the index event is reasonable rather than delaying surgery. (Level of Evidence: B Class IIb 2. In symptomatic or asymptomatic patients at high risk of complications for carotid revascularization by either CEA or CAS because of comorbidities, the effectiveness of revascularization versus medical therapy alone is not well established. (Level of Evidence: B)
38 סיבות מקובלות לטיפול בצנתור הורית נגד לניתוח מיקום בלתי נגיש בצוואר הצרות חוזרת לאחר ניתוח CEA הצרות לאחר הקרנות לצוואר התוויה חדשה חולים צעירים (אך הגברת סיכון להצרות חוזרת)
39 Class IIb 2. In symptomatic or asymptomatic patients at high risk of complications for carotid revascularization by either CEA or CAS because of comorbidities, the effectiveness of revascularization versus medical therapy alone is not well established. (Level of Evidence: B)

40 Screening for Asymptomatic Carotid Artery Stenosis: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. Sep 2014: 356.
41 Risk factors associated with asymptomatic carotid stenosis Severity of the stenosis? no!? Stenosis progression -?? Age questionable for elderly patients (because they don t live long enough to show benefit!) Gender males, questionable for females Clinical circumstances -?? Patients characteristics -?? Plaque characteristics -!?
42 Relevant indicators (for higher risk) 1. Identification of a vulnerable plaque -New modalities under investigation include functional imaging of the plaque using positron emission tomography (PET) with CT, MRI, ultrasonic plaque texture analysis,16 contrast enhanced ultrasound (CEUS) techniques etc. -Analysis of plasma biomarkers 2. Measuring cerebrovascular reactivity (CVR) 3. Micro-embolic signals (MES) 4. Associated silent brain infarcts (SBI)
43 impaired CVR and stroke risk Meta-analysis of the Asymptomatic Carotid Emboli Study (ACES) data with previous studies, impaired CVR was associated with increased risk of: - ipsilateral stroke alone (OR, 6.14; 95% CI, ; P=0.02), - ipsilateral stroke or TIA (OR, 4.76; 95% CI, ; P=0.001), and - any stroke (OR, 4.66; 95% CI, ; P=0.003). King A et al, ACES Investigators: Stroke; 2011;42:1550-5


44 Micro-Embolic Signals (MES)
. Jayasooriya G et al.")
45 Prevalence of HITS in 70% and 70% asymptomatic stenosis. HITS, High intensity transient signals (= MES). Jayasooriya G et al. Review, J Vasc Surg 2011;54:227-36
46 Stroke risk in TCD emboli positive and negative subjects with asymptomatic carotid stenosis. Jayasooriya G et al. Review, J Vasc Surg 2011;54:227-36

47 Silent brain infarcts (SBI) SBI s are common in patients at increased risk of stroke The presence of silent infarcts more than doubles the risk of subsequent stroke and dementia. Similar adverse associations were found in patients with asymptomatic significant carotid stenosis. (SBI+) (SBI-)

48 LEUKO-ARAIOSIS (LA) Radiological Term of Greek Roots 1. LEUKO = White 2. ARAIOSIS = Rarefaction, of loose texture
49 אין אפשרות להציג תמונה זו כעת.
50 Freedom from Any Stroke by Degree of Leukoaraiosis 1.0 Proportion Event-Free Degree of Leukoaraiosis None Mild Moderate to Severe Study Time (Years)
51 Influence of Cerebral Infarcts & White Matter Lesions in Patients with Carotid Stenosis Both cerebral infarcts (silent, watershed internal borderzone or cortical) and WML (leukoaraiosis) are frequently found in patients with significant carotid stenosis. As these lesions are associated with a worse outcome especially in the perioperative period, they should be recognized and taken into account before deciding on any therapeutic approach (especially invasive interventions). Preventive measures and early recognition and treatment of carotid disease may, on the other hand, reduce this increased risk.
LARGE ARTERY DISEASE pathophysiology of ischemic insults. ISCHEMIC STROKE & TIA main etiologies
 תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Carotid Artery Disease How the Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient
 Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
ESC Heart & Brain Workshop
 ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE
Fast-track CEA: a 3-year experience
 Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
The Great Swedish Debate. Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund
 The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS
 TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
TCAR: TransCarotid Artery Revascularization Angela A. Kokkosis, MD, RPVI, FACS Assistant Professor of Surgery Director of Carotid Interventions Division of Vascular & Endovascular Surgery Stony Brook University
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention
 How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Internal carotid artery near-total occlusions: Is it justified to operate on them?
 Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Internal carotid artery near-total occlusions: Is it justified to operate on them? Christos D. Liapis Professor (Em) of Vascular Surgery Athens University Medical School Director Vascular & Endovascular
Stroke prevention in asymptomatic carotid stenosis. ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ
 Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
MEET Θ symptomatic patients. K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany
 MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Emboli detection to evaluate risk of stroke
 Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
Alma Mater Studiorum Università di Bologna
 Alma Mater Studiorum Università di Bologna S.Orsola-Malpighi, Bologna, Italia Chirurgia Vascolare The volume of cerebral ischaemic lesion predicts the outcome after symptomatic carotid revascularisation
Alma Mater Studiorum Università di Bologna S.Orsola-Malpighi, Bologna, Italia Chirurgia Vascolare The volume of cerebral ischaemic lesion predicts the outcome after symptomatic carotid revascularisation
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
FRANK J. VEITH MAC TH MUNICH VASCULAR CONF
 UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Prise en charge du polyvasculaire
 Prise en charge du polyvasculaire Dépistage et prise en charge des sténoses carotidiennes Serge Kownator Centre cardiologique et Vasculaire - Thionville Disclosure Statement of Financial Interest I currently
Prise en charge du polyvasculaire Dépistage et prise en charge des sténoses carotidiennes Serge Kownator Centre cardiologique et Vasculaire - Thionville Disclosure Statement of Financial Interest I currently
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk
 Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk Amy B. Reed, MD, a Peter Gaccione, MA, b Michael Belkin, MD, b Magruder C. Donaldson, MD, b John A. Mannick, MD,
Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk Amy B. Reed, MD, a Peter Gaccione, MA, b Michael Belkin, MD, b Magruder C. Donaldson, MD, b John A. Mannick, MD,
My Latest Take on RCT Data: When is CEA or CAS the Best Option? The Interventional Position
 LINC 2016 Leipzig, Jan 26-29, 2016 My Latest Take on RCT Data: When is CEA or CAS the Best Option? The Interventional Position Horst Sievert, Iris Grunwald CardioVasculäres Centrum Frankfurt - CVC, Frankfurt
LINC 2016 Leipzig, Jan 26-29, 2016 My Latest Take on RCT Data: When is CEA or CAS the Best Option? The Interventional Position Horst Sievert, Iris Grunwald CardioVasculäres Centrum Frankfurt - CVC, Frankfurt
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
DESCRIPTION: Percent of asymptomatic patients undergoing CEA who are discharged to home no later than post-operative day #2
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Clinical experience amongst surgeons in the Asymptomatic Carotid Surgery Trial-1 (ACST-1)
") Clinical experience amongst surgeons in the Asymptomatic Carotid Surgery Trial-1 (ACST-1) Short Title: Clinical experience in the Asymptomatic Carotid Surgery Trial-1 (ACST-1) Authors: Anne Huibers 1,2,
Clinical experience amongst surgeons in the Asymptomatic Carotid Surgery Trial-1 (ACST-1) Short Title: Clinical experience in the Asymptomatic Carotid Surgery Trial-1 (ACST-1) Authors: Anne Huibers 1,2,
AN ASSESSMENT OF INTER-RATER RELIABILITY IN THE TREATMENT OF CAROTID ARTERY STENOSIS
 Pak Heart J ORIGINAL ARTICLE AN ASSESSMENT OF INTER-RATER RELIABILITY IN THE TREATMENT OF CAROTID ARTERY STENOSIS 1 2 3 4 5 Abhishek Nemani, Arshad Ali, Arshad Rehan, Ali Aboufaris, Jabar Ali 1-4 Guthrie
Pak Heart J ORIGINAL ARTICLE AN ASSESSMENT OF INTER-RATER RELIABILITY IN THE TREATMENT OF CAROTID ARTERY STENOSIS 1 2 3 4 5 Abhishek Nemani, Arshad Ali, Arshad Rehan, Ali Aboufaris, Jabar Ali 1-4 Guthrie
a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers
 The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
The study a physician-initiated study investigating the RoadSaver stent in carotid lesions Dr. Michel Bosiers Conflict of interest have the following potential conflicts of interest to report: Consulting
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
Measure #260: Rate of Carotid Endarterectomy (CEA) for Asymptomatic Patients, without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Patient Safety
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Coutts S, Wein T (Writing Group Chairs) on Behalf of the PREVENTION of STROKE Writing
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Management of Extracranial Carotid Disease and Intracranial Atherosclerosis Coutts S, Wein T (Writing Group Chairs) on Behalf of the PREVENTION of STROKE Writing
Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy
 13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side
 Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
Debata II: Carotidal stenting v.s. carotidal endatherectomy- surgical side Academician Mitrev Z, Special hospital for surgery Filip Vtori Skopje - Macedonija Oktomvri, 2008 History Hippocrates, 400 B.C.
International Journal of Stroke
 10-year risk of stroke in patients with previous cerebral infarction and the impact of carotid surgery in the Asymptomatic Carotid Surgery Trial (ACST-1) Journal: International Journal of Stroke Manuscript
10-year risk of stroke in patients with previous cerebral infarction and the impact of carotid surgery in the Asymptomatic Carotid Surgery Trial (ACST-1) Journal: International Journal of Stroke Manuscript
Endovascular treatment for pseudoocclusion of the internal carotid artery
 Endovascular treatment for pseudoocclusion of the internal carotid artery Daqiao Guo, Xiao Tang, Weiguo Fu Institute of Vascular Surgery, Fudan University, Department of Vascular Surgery, Zhongshan Hospital
Endovascular treatment for pseudoocclusion of the internal carotid artery Daqiao Guo, Xiao Tang, Weiguo Fu Institute of Vascular Surgery, Fudan University, Department of Vascular Surgery, Zhongshan Hospital
More than strokes occur
 Surgery vs Stent: Treatment for Carotid Artery Disease Imad A. Alhaddad, MD ABSTRACT PURPOSE: This article summarizes and compares the roles of surgery and stent in the management of carotid artery disease.
Surgery vs Stent: Treatment for Carotid Artery Disease Imad A. Alhaddad, MD ABSTRACT PURPOSE: This article summarizes and compares the roles of surgery and stent in the management of carotid artery disease.
Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China
 Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting Employment
Carotid stenosis management: CAS or CEA? Yaoguo Yang, Chen Zhong Beijing Anzhen Hospital,China Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting Employment
Carotid artery percutaneous treatment: back to the future Alberto Cremonesi MD, FESC
 Carotid artery percutaneous treatment: back to the future Alberto Cremonesi MD, FESC GVM Care & Research - Cardiovascular Department (Cotignola Italy) Hypothesis: Does CAS present similar outcomes than
Carotid artery percutaneous treatment: back to the future Alberto Cremonesi MD, FESC GVM Care & Research - Cardiovascular Department (Cotignola Italy) Hypothesis: Does CAS present similar outcomes than
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH
 ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
Assessment of the procedural etiology of stroke resulting from carotid artery stenting
 Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
Assessment of the procedural etiology of stroke resulting from carotid artery stenting 1. Study Purpose and Rationale: A. Background Stroke is the 3 rd leading cause of death in the United States and carries
Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC
 CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
Extracranial Carotid Artery/Stenting
 Extracranial Carotid Artery/Stenting Policy Number: 7.01.68 Last Review: 6/2018 Origination: 4/2005 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Extracranial Carotid Artery/Stenting Policy Number: 7.01.68 Last Review: 6/2018 Origination: 4/2005 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Spontaneous embolisation on TCD and carotid plaque features
 Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
CEA or CAS for asymptomatic carotid stenosis which patients benefit most?
 CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
CLINICAL TIMELINE EVA-3S CREST ICSS SPACE SAPPHIRE
 Normal Risk Symptomatic Patients: Ongoing Debate CAS vs CEA John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center University of California, Davis CLINICAL TIMELINE Randomized
Normal Risk Symptomatic Patients: Ongoing Debate CAS vs CEA John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center University of California, Davis CLINICAL TIMELINE Randomized
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards
 Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Extracranial Carotid Artery Stenting Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Extracranial Carotid Artery Stenting Professional Institutional
Extracranial Carotid Artery Stenting Page 1 of 23 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Extracranial Carotid Artery Stenting Professional Institutional
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
CAROTID STENTING A 2009 UPDATE. Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital
 CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea
 TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
TIA SINGOLO E IN CRESCENDO: due diversi scenari della rivascolarizzazione urgente carotidea R. Pini, G.L. Faggioli, M. Gargiulo, E. Pisano, A. Pilato, E. Gallitto, C. Mascoli, L.M. Cacioppa, A. Vacirca,
The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered?
 TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
Carotid Artery Stenting
 Carotid Artery Stenting Policy Number: Original Effective Date: MM.06.005 01/10/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/23/2017 Section: Surgery Place(s) of Service:
Carotid Artery Stenting Policy Number: Original Effective Date: MM.06.005 01/10/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/23/2017 Section: Surgery Place(s) of Service:
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS. Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford
 Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Carotid Imaging. Dr Andrew Farrall. Consultant Neuroradiologist
 20121123 SSCA http://www.neuroimage.co.uk/network Andrew Farrall Carotid Imaging Dr Andrew Farrall Consultant Neuroradiologist SFC Brain Imaging Research Centre (www.sbirc.ed.ac.uk), SINAPSE Collaboration
20121123 SSCA http://www.neuroimage.co.uk/network Andrew Farrall Carotid Imaging Dr Andrew Farrall Consultant Neuroradiologist SFC Brain Imaging Research Centre (www.sbirc.ed.ac.uk), SINAPSE Collaboration
The New England Journal of Medicine PROGNOSIS AFTER TRANSIENT MONOCULAR BLINDNESS ASSOCIATED WITH CAROTID-ARTERY STENOSIS
 PROGNOSIS AFTER TRANSIENT MONOCULAR BLINDNESS ASSOCIATED WITH CAROTID-ARTERY STENOSIS OSCAR BENAVENTE, M.D., MICHAEL ELIASZIW, PH.D., JONATHAN Y. STREIFLER, M.D., ALLAN J. FOX, M.D., HENRY J.M. BARNETT,
PROGNOSIS AFTER TRANSIENT MONOCULAR BLINDNESS ASSOCIATED WITH CAROTID-ARTERY STENOSIS OSCAR BENAVENTE, M.D., MICHAEL ELIASZIW, PH.D., JONATHAN Y. STREIFLER, M.D., ALLAN J. FOX, M.D., HENRY J.M. BARNETT,
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
I have the following potential conflicts of interest to report. honorarium: 1. St Jude Medical 2. Biotronik 3. Boston Scientific
 Stenting carotideo nel paziente sintomatico alla luce dei nuovi trials Savona, 11 Aprile 2015 Gioel GabrioSecco, MD, PhD Emodinamica e CardiologiaInterventistica Ospedale SantiAntonio e Biagio e Cesare
Stenting carotideo nel paziente sintomatico alla luce dei nuovi trials Savona, 11 Aprile 2015 Gioel GabrioSecco, MD, PhD Emodinamica e CardiologiaInterventistica Ospedale SantiAntonio e Biagio e Cesare
Extracranial Carotid Artery/Stenting
 Extracranial Carotid Artery/Stenting Policy Number: 7.01.68 Last Review: 6/2017 Origination: 4/2005 Next Review: 6/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Extracranial Carotid Artery/Stenting Policy Number: 7.01.68 Last Review: 6/2017 Origination: 4/2005 Next Review: 6/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis?
 for stroke prevention in patients with asymptomatic carotid stenosis?") How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2
 Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
Special Topic Section
 Special Topic Section Cerebrovasc Dis 2004;18:69 74 DOI: 10.1159/000078753 Received: March 8, 2004 Accepted: March 8, 2004 Published online: June 1, 2004 International Carotid Stenting Study: Protocol
Special Topic Section Cerebrovasc Dis 2004;18:69 74 DOI: 10.1159/000078753 Received: March 8, 2004 Accepted: March 8, 2004 Published online: June 1, 2004 International Carotid Stenting Study: Protocol
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Quality ID #345 (NQF 1543): Rate of Asymptomatic Patients Undergoing Carotid Artery Stenting (CAS) Who Are Stroke Free or Discharged Alive National Quality Strategy Domain: Effective Clinical Care 2018
Quality ID #345 (NQF 1543): Rate of Asymptomatic Patients Undergoing Carotid Artery Stenting (CAS) Who Are Stroke Free or Discharged Alive National Quality Strategy Domain: Effective Clinical Care 2018
Will guidelines and clinical practice for asymptomatic stenosis change in the near future?
 Will guidelines and clinical practice for asymptomatic stenosis change in the near future? M Storck, MD, PhD Director Dept. Vascular and Thoracic Surgery Klinikum Karlsruhe Academic Teaching Hospital,
Will guidelines and clinical practice for asymptomatic stenosis change in the near future? M Storck, MD, PhD Director Dept. Vascular and Thoracic Surgery Klinikum Karlsruhe Academic Teaching Hospital,
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Open heart surgery or carotid endarterectomy. Which procedure should be done first?
 Open heart surgery or carotid endarterectomy. Which procedure should be done first? Pedro Pinto Sousa 1, Gabriela Teixeira 2, João Gonçalves 2 ; Luís Vouga 1, Rui Almeida 2 ; Pedro Sá Pinto 2 1 Centro
Open heart surgery or carotid endarterectomy. Which procedure should be done first? Pedro Pinto Sousa 1, Gabriela Teixeira 2, João Gonçalves 2 ; Luís Vouga 1, Rui Almeida 2 ; Pedro Sá Pinto 2 1 Centro
Provider Led Entity. CDI Quality Institute PLE Stroke AUC 07/31/2018
 Provider Led Entity CDI Quality Institute PLE Stroke AUC 07/31/2018 Appropriateness of advanced imaging procedures* in patients with stroke/cerebrovascular accident (CVA) and the following clinical presentations
Provider Led Entity CDI Quality Institute PLE Stroke AUC 07/31/2018 Appropriateness of advanced imaging procedures* in patients with stroke/cerebrovascular accident (CVA) and the following clinical presentations
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None