Professor of Cardiac Surgery Director, Department of Adult Cardiac Surgery Prince. Sultan Cardiac Center Riyadh Kingdom of Saudi Arabia
|
|
|
- Julian Nicholas Allen
- 5 years ago
- Views:
Transcription



1 Results of surgical ventricular restoration An ntonio Maria CALAFIORE Professor of Cardiac Surgery Director, Department of Adult Cardiac Surgery Prince Sultan Cardiac Center Riyadh Kingdom of Saudi Arabia
2 STICH trial: conclusions The STICH trial definitively shows that adding SVR to CABG provides no clinical benefit be yond that of CABG alone in the study population.
3 STICH trial: conclusions The STICH trial definitively shows that adding SVR to CABG provides no clinical benefit be yond that of CABG alone in the study population. Both operative str rategies provided d similar short- and long-term relief of angina and HF and improvement in 6-minute walk te est performance.
4 Criticisms The eligibility criteria were changed during the study and in 2003 the heart failure symptoms were abolished.
5 Criticisms The eligibility criteria were changed during the study and in 2003 the heart failure symptoms were abolished. The LV volume was not anymore an eligibility criterion. Only the EF 35% was kept. The study then switched from heart fail lure patients to ischemicc patients.
6 Chronic dyssynergy per se is sufficient to induce ischemic LV remodeling in patients. Carluccio E et al. Patients with hibernating myocardium show altered left ventricular volumes and shape, which revert after revas cularization: evidence that dyssynergy might directly induce cardiac remodeling g. J Am Coll Cardiol 2006;47:
7 preop Chronic dyssynergy per se is end diastole sufficient to induce ischemic LV remodeling in patients. end systole Carluccio E et al. Patients with hibernating myocardium show altered left ventricular volumes and shape, which revert after revas cularization: evidence that dyssynergy might directly induce cardiac remodeling g. J Am Coll Cardiol 2006;47:
8 preop postop Chronic CABG dyssynergy per se is sufficient to end diastole end diastole induce ischemic LV remodeling in patients. end systole end systole Carluccio E et al. Patients with hibernating myocardium show altered left ventricular volumes and shape, which revert after revas cularization: evidence that dyssynergy might directly induce cardiac remodeling g. J Am Coll Cardiol 2006;47:
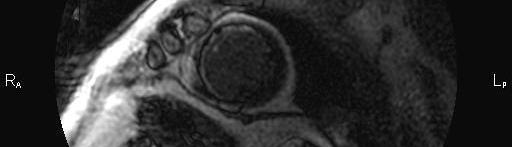
9 EDVI 160 ml/m² ESVI 148 ml/m² EF 7% Ogawa M et al. Reverse-remodeling after coronary artery bypass grafting in ischemic cardiomyopathy: assessment of myocardial viability by delayedenhanced magnetic resonance imaging can help cardiac surgeons. Interact CardioVasc Thorac Surg 2007;6:673-5
10 EDVI 160 ml/m² ESVI 148 ml/m² EF 7% <25% <25% Ogawa M et al. Reverse-remodeling after coronary artery bypass grafting in ischemic cardiomyopathy: assessment of myocardial viability by delayedenhanced magnetic resonance imaging can help cardiac surgeons. Interact CardioVasc Thorac Surg 2007;6:673-5
11 EDVI 160 ml/m² ESVI 148 ml/m² EF 7% EDVI 127 ml/m² ESVI 83 ml/m² <25% <25% EF 36% Ogawa M et al. Reverse-remodeling after coronary artery bypass grafting in ischemic cardiomyopathy: assessment of myocardial viability by delayedenhanced magnetic resonance imaging can help cardiac surgeons. Interact CardioVasc Thorac Surg 2007;6:673-5
12 The dilemma of surgery for left ventricu ular scars is still not solved.
13 The dilemma of surgery for left ventricu ular scars is still not solved. What is more important, the vo olume or the sh hape?
14 The STICH trial had, as basic surgical technique, the Dor procedure, volume-related and not shape- related.





15 Surgical technique: Dor operation The STICH trial had, as basic surgical technique, the Dor procedure, volume-related and not shape- related. Eisen HJ. Surgical ventricular reconstruction for heart failure. N Eng J Med 2009;360:1781-4
16 When the purse string and the patch insertion are limited to the scar rim, the result is surely a smaller cavity, bu ut the heart can become more spherical than th he baseline.
17 When the purse string and the patch insertion are limited to the scar rim, the result is surely a smaller cavity, bu ut pre HR (b/min) 66 EDV (ml) 175 ESV (ml) 148 EF (%) 15 CO (l/min) 1.78 the heart can become more spherical than th he baseline. Doenst T et al. Fluid-dynamic dynamic modeling of the human left ventricle: methodology and application to surgical ventricular restoration. Ann Thorac Surg 2009;87:
18 When the purse string and the patch insertion are limited to the scar rim, the result is surely a smaller cavity, bu ut pre post HR (b/min) EDV (ml) ESV (ml) EF (%) CO (l/min) the heart can become more spherical than th he baseline. Doenst T et al. Fluid-dynamic dynamic modeling of the human left ventricle: methodology and application to surgical ventricular restoration. Ann Thorac Surg 2009;87:
19 Aspect Ratio = Short/Long Axis = Sphericity Index courtesy of dr Lorenzo Menicanti Sallin EA. Fiber orientation and ejectio on fraction in the human left ventricle. Biophys J 1969;9:
20 In the most recent years morpholo ogy of fth the anterose ptal scars changed dinmany patie ents.
21 In the most recent years morpholo ogy of fth the anterose ptal scars changed dinmany patie ents. In the past dilation was predomi inant and surgical re emodeling was relativ vely easier.
22
23 This anatomic as pect prevents the involved region ntobedyskinetic and to collaps se after cardiac decompress ion in the OR.
24 This anatomic as pect prevents the involved region ntobedyskinetic and to collaps se after cardiac decompress ion in the OR. Akinesia is the most diffuse morpholog gical aspect.






25 This anatomic as pect prevents the involved region ntobedyskinetic and to collaps se after cardiac decompress ion in the OR. Akinesia is the most diffuse morpholog gical aspect.
26 As a cons sequence, nowadays volumes are not as large as bef fore.






27 As a cons sequence, nowadays volumes are not as large as bef fore.
28 The septum is oft ten more involved than the free wall and bulges toward the right ventricle, minimizing the external dilation.






29 The septum is oft ten more involved than the free wall and bulges toward the right ventricle, minimizing the external dilation.
30 In such cases pu rpose of surgery is to address the correction mainly to the septum, thatis rebuilt and mo oved anteriorly.
31 In such cases pu rpose of surgery is to address the correction mainly to the septum, thatis rebuilt and mo oved anteriorly. The longitud dinal axis is maintained similar to the preoperative o ne, to avoid any change in sph hericity, even if some apical scar has to be included in th he correction.






32 The longitud dinal axis is maintained similar to the preoperative o ne, to avoid any change in sph hericity, even if some apical scar has to be included in th he correction.
33 Calafio ore et al Left ventricula ar restoration for anteros septal scars: s volume ver rsus shape J Thorac Cardiovasc Surg 2010;139:
34 popul lation January 1988 to February patients underwent LVR for anteroseptal scars

35 popul lation January 1988 to February patients underwent LVR for anteroseptal scars Dor procedure n=107 (34.7%)
36 popul lation January 1988 to February patients underwent LVR for anteroseptal scars Guilmet procedure n=32 (10.4%) Dor procedure n=107 (34.7%)
37 popul lation January 1988 to February patients underwent LVR for anteroseptal scars Guilmet procedure septal reshaping n=32 (10.4%) n=140 (45.6%) Dor procedure n=107 (34.7%)
38 popul lation January 1988 to February patients underwent LVR for anteroseptal scars Guilmet procedure septal reshaping n=32 (10.4%) n=140 (45.6%) Dor procedure n=107 (34.7%) septoapical Dor procedure n=29 (9.3%)
39 popul lation January 1988 to February patients underwent LVR for anteroseptal scars Target of the procedure was: LV volume n= =107 (34.7%) LV shape n= =201 (65.3%)











40 current surgical indica ation to septoapical Dor procedure , 2008, n=29










41 current surgical indica ation to septal reshaping , 2008, n=140 S A
42
43 The patch is as long as necessary (m median 6 cm). Its height varie es according to the ED volumes.
44 The patch is as long as necessary (m median 6 cm). Its height varie es according to the ED volumes. If <80 ml/m m², the ratio length/he eight is 2:1
45 The patch is as long as necessary (m median 6 cm). Its height varie es according to the ED volumes. If <80 ml/m m², the ratio length/he eight is 2:1 If 80 ml/m², t he ratio is 3:1
46 The patch is as long as necessary (m median 6 cm). Its height varie es according to the ED volumes. If <80 ml/m m², the ratio length/he eight is 2:1 If 80 ml/m², t he ratio is 3:1 In case of sev vere diastolic dysfunction n, the ratio is alway ys 2:1
47 late re esults Mean follo ow up was 77±50 months
48 Su urvival pro obability (%) ±2.5 Freedom from death any cause 66.7± Number at risk months
49 ity (%) Survival probabil ± Freedom from cardiac death Freedom from death any cause 73.2± Number at risk Group: Group: months
50 Surviv val probab bility (%) ±2.8 Freedom from cardiac death Freedom from death any cause Freedom from cardiac event Number at risk Group: Group: Group: months 54.3±
51 Sur rvival prob bability (% %) ±2.8 Freedom from cardiac death Freedom from death any cause Freedom from cardiac event Freedom from any event Number at risk Group: Group: Group: Group: ± months
52 late re esults Curves were cut at 5y years to allow groups comparison.
53 freedom from cardiac death Su urvival prob bability (%) Group S 86.6±2.6 Group V 76.3± Number at risk Group: S Group: V months
54 freedom from cardiac death Su urvival prob bability (%) p= =0.032 Group S 86.6±2.6 Group V 76.3± Number at risk Group: S Group: V months
55 freedom from cardiac death Su urvival prob bability (%) HR=2.4 95CI= p=0.011 p= =0.032 Group S 86.6±2.6 Group V 76.3± Number at risk Group: S Group: V months
56 freedom from cardiac events Survival pro obability (% %) Group S 77.9±3.3 Group V 63.9± Number at risk Group: S Group: V months
57 freedom from cardiac events Survival pro obability (% %) p= =0.011 Group S 77.9±3.3 Group V 63.9± Number at risk Group: S Group: V months
58 freedom from cardiac events Survival pro obability (% %) HR=2.4 95CI= p= Number at risk Group: S Group: V p= =0.011 months Group S 77.9±3.3 Group V 63.9±
59 freedom from cardiac events (1 st month excluded) 100 Survival pro obability (% %) Group S 81.1±3.3 Group V 71.2± Number at risk Group: S Group: V months
60 freedom from cardiac events (1 st month excluded) Survival pro obability (% %) p= =0.039 Group S 81.1±3.3 Group V 71.2± Number at risk Group: S Group: V months
61 freedom from cardiac events (1 st month excluded) Survival pro obability (% %) HR=2.2 95CI= p= Number at risk Group: S Group: V p= =0.039 months Group S 81.1±3.3 Group V 71.2±
62 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling
63 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling septal reshaping n=30


64 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling septal reshaping n=30 septoapical Dor n=15

65 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling septal reshaping n=30 septoapical Dor n=15 lateral resection n=8
66 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling septal reshaping n=30 septoapical Dor n=15 in nferior resection n=3 lateral resection n=8
67 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling mitral valve surgery yes n=41, 73.2% no n=15, 27.8%
68 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling mitral valve surgery yes n=41, 73.2% mitral valve procedure repair n=41, 73.2% no n=15, 27.8% prosthesis insertion n=15, 27.8%
69 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling mitral valve surgery yes n=41, 73.2% mitral valve procedure repair n=41, 73.2% tricuspid valve surgery no n=15, 27.8% yes n=24 4, 42.8% prosthesis insertion n=15, 27.8% no n=32, 57.2%
70 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling No patient die ed during the first 30 days 3 to 6 months after surgery 3 patients (5.3 3%) died due to septi icemia i (dyalisis catheter, d efibrillator wire and pacema aker wire)
71 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling EF modification before surgery and at discharge


72 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling EF modification before surgery and at discharge % 27±9




73 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling EF modification before surgery and at discharge % 27±9 p< < ±8
74 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge

75 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m²

76 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m² 85±44
77 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m² p<00 < ±44
78 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m² 83±3131 p<00 < end systole 85±44


79 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m² 83±3131 p<00 < end systole 85±44 57±36
80 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge 113±3131 end diastole ml/m² 83±3131 p<00 < end systole 85±44 p < ±36

81 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge %
82 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge % -26.5
83 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling volumes modification befor re surgery and at discharge %
84 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling After a median follow up of 10 months, we wer re able to contact only 31 of the 53 survivors (60%).
85 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling After a median follow up of 10 months, we wer re able to contact only 31 of the 53 survivors (60%). One patient (3.2%) was unchanged and the remain ning 30 (96.8%) improved of at lea ast 1 NYHA Class.
86 Department of Adult Cardiac Surgery Prince Sultan Cardiac Cen nter, Riyadh, Saudi Arabia June 2009 to December elective or urgent patients underwent LV surgical remod deling After a median follow up of 10 months, we wer re able to contact only 31 of the 53 survivors (60%). One patient (3.2%) was unchanged and the remain ning 30 (96.8%) improved of at lea ast 1 NYHA Class. One patient had a late CVA, but fully recov vered.
87 conclu usions Long term outc come after left ventricular ti surg gical remodeling is good.
88 conclu usions Long term outc come after left ventricular ti surg gical remodeling is good. In our experience e better results, in particular freed dom from cardiac events, are achieved when purpose of surg gery is to recover a conica al shape.
CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή;
 LV Aneurysm and VSD in Ischaemic Heart Failure / Στεφανιαία νόσος, ανεύρυσμα αριστεράς κοιλίας και VSD CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή; THEODOROS KARAISKOS CONSULTANT
LV Aneurysm and VSD in Ischaemic Heart Failure / Στεφανιαία νόσος, ανεύρυσμα αριστεράς κοιλίας και VSD CABG alone. It s enough? / Μόνο η αορτοστεφανιαία παράκαμψη είναι αρκετή; THEODOROS KARAISKOS CONSULTANT
SAUDI HEART ASSOCIATION
 SAUDI HEART ASSOCIATION LV aneurysm repair: reflections on the STICH trial John Pepper Royal Brompton Hospital Monday 21st February 2011 Riyaddh, Saudi Arabia. Surgical Options in Advanced Heart Failure
SAUDI HEART ASSOCIATION LV aneurysm repair: reflections on the STICH trial John Pepper Royal Brompton Hospital Monday 21st February 2011 Riyaddh, Saudi Arabia. Surgical Options in Advanced Heart Failure
MEDICAL POLICY SUBJECT: SURGICAL VENTRICULAR RESTORATION
 MEDICAL POLICY SUBJECT: SURGICAL VENTRICULAR PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: SURGICAL VENTRICULAR PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
Modifications of the Dor Procedure Introduction
 Modifications of the Dor Procedure Introduction Left ventricular aneurysms (LVAs) occur in up to 40% of patients after myocardial infarction. The majority of these aneurysms are caused by occlusion of
Modifications of the Dor Procedure Introduction Left ventricular aneurysms (LVAs) occur in up to 40% of patients after myocardial infarction. The majority of these aneurysms are caused by occlusion of
Surgical Ventricular Restoration. Description
 Subject: Surgical Ventricular Restoration Page: 1 of 8 Last Review Status/Date: December 2013 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Surgical
Subject: Surgical Ventricular Restoration Page: 1 of 8 Last Review Status/Date: December 2013 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Surgical
Surgical Ventricular Restoration
 Surgical Ventricular Restoration Policy Number: 7.01.103 Last Review: 9/2014 Origination: 3/2006 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
Surgical Ventricular Restoration Policy Number: 7.01.103 Last Review: 9/2014 Origination: 3/2006 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies
 Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Surgical Ventricular Restoration
 Medical Policy Manual Surgery, Policy No. 149 Surgical Ventricular Restoration Next Review: July 2018 Last Review: July 2017 Effective: August 1, 2017 IMPORTANT REMINDER Medical Policies are developed
Medical Policy Manual Surgery, Policy No. 149 Surgical Ventricular Restoration Next Review: July 2018 Last Review: July 2017 Effective: August 1, 2017 IMPORTANT REMINDER Medical Policies are developed
Surgical Ventricular Restoration
 Surgical Ventricular Restoration Policy Number: 7.01.103 Last Review: 3/2018 Origination: 3/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
Surgical Ventricular Restoration Policy Number: 7.01.103 Last Review: 3/2018 Origination: 3/2006 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
Preoperative Parameters Predicting the Postoperative Course of Endoventricular Circular Patch Plasty
 Original Article Preoperative Parameters Predicting the Postoperative Course of Endoventricular Circular Patch Plasty Keiichiro Kondo, MD, Yoshihide Sawada, MD, and Shinjiro Sasaki, MD, PhD It is necessary
Original Article Preoperative Parameters Predicting the Postoperative Course of Endoventricular Circular Patch Plasty Keiichiro Kondo, MD, Yoshihide Sawada, MD, and Shinjiro Sasaki, MD, PhD It is necessary
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Impact of Surgical Ventricular Restoration on Diastolic Function: Implications of Shape and Residual Ventricular Size
 Impact of Surgical Ventricular Restoration on Diastolic Function: Implications of Shape and Residual Ventricular Size Serenella Castelvecchio, MD, Lorenzo Menicanti, MD, Marco Ranucci, MD, and Marisa Di
Impact of Surgical Ventricular Restoration on Diastolic Function: Implications of Shape and Residual Ventricular Size Serenella Castelvecchio, MD, Lorenzo Menicanti, MD, Marco Ranucci, MD, and Marisa Di
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Medical Policy Surgical Ventricular Restoration. Description. Related Policies. Policy. Policy Guidelines. Benefit Application
 7.01.103 Surgical Ventricular Restoration Section 7.0 Surgery Subsection Effective Date November 26, 2014 Original Policy Date November 26, 2014 Next Review Date November 2015 Description Surgical ventricular
7.01.103 Surgical Ventricular Restoration Section 7.0 Surgery Subsection Effective Date November 26, 2014 Original Policy Date November 26, 2014 Next Review Date November 2015 Description Surgical ventricular
Department of Cardiothoracic Surgery, Cardiology and Medicine, St Vincent s Hospital, University of Melbourne, Melbourne, Victoria, Australia
 Surgical Ventricular Restoration Procedure: Single- Center Comparison of Surgical Treatment of Ischemic Heart Failure (STICH) Versus Non-STICH Patients Siew Goh, MBChB, David Prior, PhD, Andrew Newcomb,
Surgical Ventricular Restoration Procedure: Single- Center Comparison of Surgical Treatment of Ischemic Heart Failure (STICH) Versus Non-STICH Patients Siew Goh, MBChB, David Prior, PhD, Andrew Newcomb,
Surgical Management of Heart Failure. Walid Abukhudair MD, FRCSc Head of Cardiac Surgery Department KFAFH Jeddah
 Surgical Management of Heart Failure Walid Abukhudair MD, FRCSc Head of Cardiac Surgery Department KFAFH Jeddah SURGICAL TREATMENT OF HEART FAILURE CABG.Curative Valve repair or Replacement..Curative??
Surgical Management of Heart Failure Walid Abukhudair MD, FRCSc Head of Cardiac Surgery Department KFAFH Jeddah SURGICAL TREATMENT OF HEART FAILURE CABG.Curative Valve repair or Replacement..Curative??
Steven F Bolling Professor of Cardiac Surgery University of Michigan
 Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
The Additional Prognostic Value of Left Atrial Volume on the Outcome of Patients After Surgical Ventricular Reconstruction
 The Additional Prognostic Value of Left Atrial Volume on the Outcome of Patients After Surgical Ventricular Reconstruction Serenella Castelvecchio, MD, Marco Ranucci, MD, Francesco Bandera, MD, Ekaterina
The Additional Prognostic Value of Left Atrial Volume on the Outcome of Patients After Surgical Ventricular Reconstruction Serenella Castelvecchio, MD, Marco Ranucci, MD, Francesco Bandera, MD, Ekaterina
marked increase in thickness of walls of heart in patient with HCM.
 Surgical Management of Hypertrophic Obstructive Cardiomyopathy Hani K. Najm MD, Msc, FRCSC, FRCS (Glasg Glasg), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi
Surgical Management of Hypertrophic Obstructive Cardiomyopathy Hani K. Najm MD, Msc, FRCSC, FRCS (Glasg Glasg), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Debate in CHD - When Should We
 Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Systolic and Diastolic Function After Patch Reconstruction of Left Ventricular Aneurysms
 Systolic and Diastolic Function After Patch Reconstruction of Left Ventricular Aneurysms Tetsuji Kawata, MD, Soichiro Kitamura, MD, Kanji Kawachi, MD, Ryuichi Morita, MD, Yoshitsugu Yoshida, MD, and Junichi
Systolic and Diastolic Function After Patch Reconstruction of Left Ventricular Aneurysms Tetsuji Kawata, MD, Soichiro Kitamura, MD, Kanji Kawachi, MD, Ryuichi Morita, MD, Yoshitsugu Yoshida, MD, and Junichi
Ischemic Mitral Valve Disease: Repair, Replace or Ignore?
 Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Ischemic Ventricular Septal Rupture
 Ischemic Ventricular Septal Rupture Optimal Management Strategies Juan P. Umaña, M.D. Chief Medical Officer FCI Institute of Cardiology Disclosures Abbott Mitraclip Royalties Johnson & Johnson Proctor
Ischemic Ventricular Septal Rupture Optimal Management Strategies Juan P. Umaña, M.D. Chief Medical Officer FCI Institute of Cardiology Disclosures Abbott Mitraclip Royalties Johnson & Johnson Proctor
Surgical Ventricular Restoration
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Anew era for exclusion of dyskinetic or akinetic areas
 Septal Reshaping for Exclusion of Anteroseptal Dyskinetic or Akinetic Areas Antonio M. Calafiore, MD, Michele Di Mauro, MD, Gabriele Di Giammarco, MD, Sabina Gallina, MD, Angela L. Iacò, MD, Marco Contini,
Septal Reshaping for Exclusion of Anteroseptal Dyskinetic or Akinetic Areas Antonio M. Calafiore, MD, Michele Di Mauro, MD, Gabriele Di Giammarco, MD, Sabina Gallina, MD, Angela L. Iacò, MD, Marco Contini,
Role of Surgical Ventricular Restoration in the Treatment of Ischemic Cardiomyopathy
 Role of Surgical Ventricular Restoration in the Treatment of Ischemic Cardiomyopathy Jun Liu, MD, Zixiong Liu, MD, Qiang Zhao, MD, Anqing Chen, MD, Zhe Wang, MD, and Dan Zhu, MD Department of Cardiovascular
Role of Surgical Ventricular Restoration in the Treatment of Ischemic Cardiomyopathy Jun Liu, MD, Zixiong Liu, MD, Qiang Zhao, MD, Anqing Chen, MD, Zhe Wang, MD, and Dan Zhu, MD Department of Cardiovascular
Management of Tricuspid Regurgitation
 Management of Tricuspid Regurgitation Antonis A. Pitsis, FETCS, FESC Thessaloniki Heart Institute, St. Luke s Hospital, Thessaloniki, GREECE HEART FAILURE 2012 BELGRADE SERBIA Does Tricuspid Regurgitation
Management of Tricuspid Regurgitation Antonis A. Pitsis, FETCS, FESC Thessaloniki Heart Institute, St. Luke s Hospital, Thessaloniki, GREECE HEART FAILURE 2012 BELGRADE SERBIA Does Tricuspid Regurgitation
Patterns of Left Ventricular Remodeling in Chronic Heart Failure: The Role of Inadequate Ventricular Hypertrophy
 Abstract ESC 82445 Patterns of Left Ventricular Remodeling in Chronic Heart Failure: The Role of Inadequate Ventricular Hypertrophy FL. Dini 1, P. Capozza 1, P. Fontanive 2, MG. Delle Donne 1, V. Santonato
Abstract ESC 82445 Patterns of Left Ventricular Remodeling in Chronic Heart Failure: The Role of Inadequate Ventricular Hypertrophy FL. Dini 1, P. Capozza 1, P. Fontanive 2, MG. Delle Donne 1, V. Santonato
Revascularization In HFrEF: Are We Close To The Truth. Ali Almasood
 Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death
 Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Nontransplant cardiac surgery for congestive heart. Septal Anterior Ventricular Exclusion Procedure for Idiopathic Dilated Cardiomyopathy
 Septal Anterior Ventricular Exclusion Procedure for Idiopathic Dilated Cardiomyopathy Hisayoshi Suma, MD, Tadashi Isomura, MD, Taiko Horii, MD, and Fumikazu Nomura, MD The Cardiovascular Institute, Tokyo,
Septal Anterior Ventricular Exclusion Procedure for Idiopathic Dilated Cardiomyopathy Hisayoshi Suma, MD, Tadashi Isomura, MD, Taiko Horii, MD, and Fumikazu Nomura, MD The Cardiovascular Institute, Tokyo,
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Left Ventricular Wall Resection for Aneurysm and Akinesia due to Coronary Artery Disease: Fifty Consecutive Patients
 Left Ventricular Wall Resection for Aneurysm and Akinesia due to Coronary Artery Disease: Fifty Consecutive Patients Armand A. Lefemine, M.D., Rajagopalan Govindarajan, M.D., K. Ramaswamy, M.D., Harrison
Left Ventricular Wall Resection for Aneurysm and Akinesia due to Coronary Artery Disease: Fifty Consecutive Patients Armand A. Lefemine, M.D., Rajagopalan Govindarajan, M.D., K. Ramaswamy, M.D., Harrison
DELAYED ENHANCEMENT IMAGING IN CHILDREN
 NASCI 38 TH ANNUAL MEENG, SEATLE October 3-5, 21 1. DELAYED ENHANCEMENT IN CHILDREN Shi-Joon Yoo, MD Lars Grosse-Wortmann, MD University of Toronto Canada -1. 1. 1. Magnitude image Magnitude images -1.
NASCI 38 TH ANNUAL MEENG, SEATLE October 3-5, 21 1. DELAYED ENHANCEMENT IN CHILDREN Shi-Joon Yoo, MD Lars Grosse-Wortmann, MD University of Toronto Canada -1. 1. 1. Magnitude image Magnitude images -1.
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Left Ventricular Reconstruction with or without Mitral Annuloplasty
 Original Article Left Ventricular Reconstruction with or without Mitral Annuloplasty Tetsuya Ueno, MD, 1 Ryuzo Sakata, MD, 3 Yoshifumi Iguro, MD, 1 Hiroyuki Yamamoto, MD, 1 Masahiro Ueno, MD, 1 Takayuki
Original Article Left Ventricular Reconstruction with or without Mitral Annuloplasty Tetsuya Ueno, MD, 1 Ryuzo Sakata, MD, 3 Yoshifumi Iguro, MD, 1 Hiroyuki Yamamoto, MD, 1 Masahiro Ueno, MD, 1 Takayuki
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Surgical Management of Left Ventricular Aneurysms by the Jatene Technique
 Surgical Management of Left Ventricular Aneurysms by the Jatene Technique James L. Cox Few significant improvements in left ventricular aneurysm (LVA) surgery occurred from the time of Cooley s report
Surgical Management of Left Ventricular Aneurysms by the Jatene Technique James L. Cox Few significant improvements in left ventricular aneurysm (LVA) surgery occurred from the time of Cooley s report
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Viability Testing Using Dynamic Echocardiography
 Viability Testing Using Dynamic Echocardiography Theodora A Zaglavara, MD, PhD Director of Echocardiography EUROMEDICA KYANOUS STAVROS HOSPITAL Thessaloniki GREECE Goals of Cardiac Imaging in Coronary
Viability Testing Using Dynamic Echocardiography Theodora A Zaglavara, MD, PhD Director of Echocardiography EUROMEDICA KYANOUS STAVROS HOSPITAL Thessaloniki GREECE Goals of Cardiac Imaging in Coronary
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Surgical Ventricular Restoration for Patients With Ischemic Heart Failure: Determinants of Two-Year Survival
 Surgical for Patients With Ischemic Heart Failure: Determinants of Two-Year Survival Tomasz G. Witkowski, MD, Ellen A. ten Brinke, MD, Victoria Delgado, MD, Arnold C.T. Ng, MBBS, Matteo Bertini, MD, Nina
Surgical for Patients With Ischemic Heart Failure: Determinants of Two-Year Survival Tomasz G. Witkowski, MD, Ellen A. ten Brinke, MD, Victoria Delgado, MD, Arnold C.T. Ng, MBBS, Matteo Bertini, MD, Nina
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous pulmonary valve replacement after different duration of free pulmonary regurgitation in a porcine model: effects on the right ventricle
 Percutaneous pulmonary valve replacement after different duration of free pulmonary regurgitation in a porcine model: effects on the right ventricle Mads Ersboll a, Niels Vejlstrup a, Jens Christian Nilsson
Percutaneous pulmonary valve replacement after different duration of free pulmonary regurgitation in a porcine model: effects on the right ventricle Mads Ersboll a, Niels Vejlstrup a, Jens Christian Nilsson
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Ischemic Mitral Regurgitation 1 / 6 2 / 6 3 / 6 Ischemic Mitral Regurgitation Background Myocardial infarction (MI) can directly cause (IMR), which has been touted as an indicator of poor prognosis in
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability
 Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Surgical Options for Advanced Heart Failure
 Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
Surgical Options for Advanced Heart Failure Benjamin Medalion, MD Director, Transplantation and Heart Failure Surgery Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Hospital Heart
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Measure #445 (NQF 0119): Risk-Adjusted Operative Mortality for Coronary Artery Bypass Graft (CABG) National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #445 (NQF 0119): Risk-Adjusted Operative Mortality for Coronary Artery Bypass Graft (CABG) National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
The Beating Heart Approach is Not Necessary for the Dor Procedure
 The Beating Heart Approach is Not Necessary for the Dor Procedure Thomas S. Maxey, MD, T. Brett Reece, MD, Peter I. Ellman, MD, John A. Kern, MD, Curtis G. Tribble, MD, and Irving L. Kron, MD Division
The Beating Heart Approach is Not Necessary for the Dor Procedure Thomas S. Maxey, MD, T. Brett Reece, MD, Peter I. Ellman, MD, John A. Kern, MD, Curtis G. Tribble, MD, and Irving L. Kron, MD Division
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
CT for Myocardial Characterization of Cardiomyopathy. Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea
 CT for Myocardial Characterization of Cardiomyopathy Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea Cardiomyopathy Elliott P et al. Eur Heart J 2008;29:270-276 The European Society
CT for Myocardial Characterization of Cardiomyopathy Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea Cardiomyopathy Elliott P et al. Eur Heart J 2008;29:270-276 The European Society
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
The Who, How and When of Advanced Heart Failure Therapies. Disclosures. What is Advanced Heart Failure?
 The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
Mitral valve treatment in advanced heart failure: Repair, Replacement, MitraClip. Nicola Buzzatti, MD San Raffaele Scientific Institute Milan, Italy
 Mitral valve treatment in advanced heart failure: Repair, Replacement, MitraClip Nicola Buzzatti, MD San Raffaele Scientific Institute Milan, Italy Disclosures I have nothing to disclose FMR: a ventricular
Mitral valve treatment in advanced heart failure: Repair, Replacement, MitraClip Nicola Buzzatti, MD San Raffaele Scientific Institute Milan, Italy Disclosures I have nothing to disclose FMR: a ventricular
Surgical Treatment of Ischemic Heart Failure
 REVIEW Cardiovascular Surgery Circ J 2009; Suppl A: A-1 A-5 Surgical Treatment of Ischemic Heart Failure The Dor Procedure Marisa Di Donato, MD*, **; Serenella Castelvecchio, MD*; Lorenzo Menicanti, MD*
REVIEW Cardiovascular Surgery Circ J 2009; Suppl A: A-1 A-5 Surgical Treatment of Ischemic Heart Failure The Dor Procedure Marisa Di Donato, MD*, **; Serenella Castelvecchio, MD*; Lorenzo Menicanti, MD*
Surgical repair techniques for IMR: future percutaneous options?
 Surgical repair techniques for IMR: can this teach us about future percutaneous options? Genk - Belgium Prof. Dr. R. Dion KULeu Disclosure slide Robert A. Dion I disclose the following financial relationships:
Surgical repair techniques for IMR: can this teach us about future percutaneous options? Genk - Belgium Prof. Dr. R. Dion KULeu Disclosure slide Robert A. Dion I disclose the following financial relationships:
Why do patients with ischemic cardiomyopathy and a substantial amount of viable myocardium not always recover in function after revascularization?
 Surgery for Acquired Cardiovascular Disease Why do patients with ischemic cardiomyopathy and a substantial amount of viable myocardium not always recover in function after revascularization? Arend F. L.
Surgery for Acquired Cardiovascular Disease Why do patients with ischemic cardiomyopathy and a substantial amount of viable myocardium not always recover in function after revascularization? Arend F. L.
Use of Cardiac Computed Tomography for Ventricular Volumetry in Late Postoperative Patients with Tetralogy of Fallot
 Korean J Thorac Cardiovasc Surg 2017;50:71-77 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.71 Use of Cardiac Computed Tomography for Ventricular
Korean J Thorac Cardiovasc Surg 2017;50:71-77 ISSN: 2233-601X (Print) ISSN: 2093-6516 (Online) CLINICAL RESEARCH https://doi.org/10.5090/kjtcs.2017.50.2.71 Use of Cardiac Computed Tomography for Ventricular
Less Invasive Ventricular Enhancement For Heart Attack Patients. Revivent TC TransCatheter Ventricular Enhancement System
 For Heart Attack Patients Revivent TC TransCatheter Ventricular Enhancement System This patient booklet is for those who have suffered a heart attack resulting in damage to the left side of the heart causing
For Heart Attack Patients Revivent TC TransCatheter Ventricular Enhancement System This patient booklet is for those who have suffered a heart attack resulting in damage to the left side of the heart causing
ARVD/C and the athlete s heart: Application of revised Task Force Criteria
 ARVD/C and the athlete s heart: Application of revised Task Force Criteria T. Luijkx MD, B.K. Velthuis MD PhD, N.H.J. Prakken MD PhD, M.G.P.J. Cox MD, R.N.W. Hauer MD PhD, M.J.M. Cramer MD PhD Stockholm,
ARVD/C and the athlete s heart: Application of revised Task Force Criteria T. Luijkx MD, B.K. Velthuis MD PhD, N.H.J. Prakken MD PhD, M.G.P.J. Cox MD, R.N.W. Hauer MD PhD, M.J.M. Cramer MD PhD Stockholm,
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Acquired Cardiovascular Disease
 Holly et al Acquired Cardiovascular Disease Myocardial viability and impact of surgical ventricular reconstruction on outcomes of patients with severe left ventricular dysfunction undergoing coronary artery
Holly et al Acquired Cardiovascular Disease Myocardial viability and impact of surgical ventricular reconstruction on outcomes of patients with severe left ventricular dysfunction undergoing coronary artery
Revascularization Strategies in Patients with Severe LV Dysfunction
 Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
A new concept of ventricular restoration for nonischemic dilated cardiomyopathy
 European Journal of Cardio-thoracic Surgery 29S (2006) S207 S212 www.elsevier.com/locate/ejcts A new concept of ventricular restoration for nonischemic dilated cardiomyopathy Hisayoshi Suma a, Taiko Horii
European Journal of Cardio-thoracic Surgery 29S (2006) S207 S212 www.elsevier.com/locate/ejcts A new concept of ventricular restoration for nonischemic dilated cardiomyopathy Hisayoshi Suma a, Taiko Horii
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
For Personal Use. Copyright HMP 2013
 12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
Left Ventricular Reconstruction in Ischemic Heart Disease
 Department of Molecular Medicine and Surgery Karolinska Institutet Stockholm, Sweden Left Ventricular Reconstruction in Ischemic Heart Disease Ulrik Sartipy Stockholm 2007 All previously published papers
Department of Molecular Medicine and Surgery Karolinska Institutet Stockholm, Sweden Left Ventricular Reconstruction in Ischemic Heart Disease Ulrik Sartipy Stockholm 2007 All previously published papers
Gd-enhanced cardiovascular MR imaging to identify left ventricular pseudoaneurysm
 Journal of Cardiovascular Magnetic Resonance (2005) 7, 717 721 Copyright D 2005 Taylor & Francis Inc. ISSN: 1097-6647 print / 1532-429X online DOI: 10.1081/JCMR-200065641 CASE REPORT Gd-enhanced cardiovascular
Journal of Cardiovascular Magnetic Resonance (2005) 7, 717 721 Copyright D 2005 Taylor & Francis Inc. ISSN: 1097-6647 print / 1532-429X online DOI: 10.1081/JCMR-200065641 CASE REPORT Gd-enhanced cardiovascular
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
(Ann Thorac Surg 2008;85:845 53)
") I Made Adi Parmana The utility of intraoperative TEE has become increasingly more evident as anesthesiologists, cardiologists, and surgeons continue to appreciate its potential application as an invaluable
I Made Adi Parmana The utility of intraoperative TEE has become increasingly more evident as anesthesiologists, cardiologists, and surgeons continue to appreciate its potential application as an invaluable
The Key Questions in Mitral Valve Interventions. Where Are We in 2018?
 The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Komplikationen des akuten Myokardinfarktes Klaus Holper Paul Libera Rüdiger Lange
 Deutsches Herzzentrum München Klinik an der TU München Komplikationen des akuten Myokardinfarktes Klaus Holper Paul Libera Rüdiger Lange Übersicht Globale Herzinsuffizienz Ventrikelseptumdefekt Ventrikelaneurysma
Deutsches Herzzentrum München Klinik an der TU München Komplikationen des akuten Myokardinfarktes Klaus Holper Paul Libera Rüdiger Lange Übersicht Globale Herzinsuffizienz Ventrikelseptumdefekt Ventrikelaneurysma
Septal Myectomy, Papillary Muscle Resection, and Mitral Valve Replacement for Hypertrophic Obstructive Cardiomyopathy: A Case Report
 Case Report Septal Myectomy, Papillary Muscle Resection, and Mitral Valve Replacement for Hypertrophic Obstructive Cardiomyopathy: A Case Report Junichiro Takahashi, MD, 1 Yutaka Wakamatsu, MD, 1 Jun Okude,
Case Report Septal Myectomy, Papillary Muscle Resection, and Mitral Valve Replacement for Hypertrophic Obstructive Cardiomyopathy: A Case Report Junichiro Takahashi, MD, 1 Yutaka Wakamatsu, MD, 1 Jun Okude,
Significance of Left Ventricular Diastolic Function on Outcomes After Surgical Ventricular Restoration
 Significance of Left Ventricular Diastolic Function on Outcomes After Surgical Ventricular Restoration Akira Marui, MD, PhD, Takeshi Nishina, MD, PhD, Yoshiaki Saji, MD, Kazuhiro Yamazaki, MD, PhD, Takeshi
Significance of Left Ventricular Diastolic Function on Outcomes After Surgical Ventricular Restoration Akira Marui, MD, PhD, Takeshi Nishina, MD, PhD, Yoshiaki Saji, MD, Kazuhiro Yamazaki, MD, PhD, Takeshi
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD
 New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
What is Ebstein Anomaly?
 Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
FEV1 predicts length of stay and in-hospital mortality in patients undergoing cardiac surgery
 EUROPEAN SOCIETY OF CARDIOLOGY CONGRESS 2010 FEV1 predicts length of stay and in-hospital mortality in patients undergoing cardiac surgery Nicholas L Mills, David A McAllister, Sarah Wild, John D MacLay,
EUROPEAN SOCIETY OF CARDIOLOGY CONGRESS 2010 FEV1 predicts length of stay and in-hospital mortality in patients undergoing cardiac surgery Nicholas L Mills, David A McAllister, Sarah Wild, John D MacLay,
Xiaorong Chen 1,2, Hongjie Hu 2, Yue Qian 2, Jiner Shu 1. Introduction
 Original Article Relation of late gadolinium enhancement in cardiac magnetic resonance on the diastolic volume recovery of left ventricle with hypertrophic cardiomyopathy Xiaorong Chen 1,2, Hongjie Hu
Original Article Relation of late gadolinium enhancement in cardiac magnetic resonance on the diastolic volume recovery of left ventricle with hypertrophic cardiomyopathy Xiaorong Chen 1,2, Hongjie Hu
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
Importance of the Area of Fibrosis at the Midterm Evolution of Patients Submitted to Ventricular Reconstruction
 Importance of the Area of Fibrosis at the Midterm Evolution of Patients Submitted to Ventricular Reconstruction Gustavo Calado de Aguiar Ribeiro, Mauricio Lopes, Fernando Antoniali, Ana Nunes, Cledicyon
Importance of the Area of Fibrosis at the Midterm Evolution of Patients Submitted to Ventricular Reconstruction Gustavo Calado de Aguiar Ribeiro, Mauricio Lopes, Fernando Antoniali, Ana Nunes, Cledicyon
The Ross Procedure: Outcomes at 20 Years
 The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Ross Procedure: Outcomes at 20 Years Tirone David Carolyn David Anna Woo Cedric Manlhiot University of Toronto Conflict of Interest None The Ross Procedure 1990 to 2004 212 patients: 66% 34% Mean age:
The Impact of Volume Reduction on Early and Long-Term Outcomes in Surgical Ventricular Restoration for Severe Heart Failure
 The Impact of Volume Reduction on Early and Long-Term Outcomes in Surgical Ventricular Restoration for Severe Heart Failure Nathan Wm. Skelley, BS, Jeremiah G. Allen, MD, George J. Arnaoutakis, MD, Eric
The Impact of Volume Reduction on Early and Long-Term Outcomes in Surgical Ventricular Restoration for Severe Heart Failure Nathan Wm. Skelley, BS, Jeremiah G. Allen, MD, George J. Arnaoutakis, MD, Eric
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiovascular magnetic resonance for timing pulmonary valve replacement E.Valsangiacomo Buechel University Children s Hospital Zurich Outline Introduction Pulmonary
DECLARATION OF CONFLICT OF INTEREST Cardiovascular magnetic resonance for timing pulmonary valve replacement E.Valsangiacomo Buechel University Children s Hospital Zurich Outline Introduction Pulmonary
Concomitant mitral valve surgery in patients undergoing surgical ventricular reconstruction for ischaemic cardiomyopathy
 European Journal of Cardio-Thoracic Surgery 43 (2013) 1000 1005 doi:10.1093/ejcts/ezs499 Advance Access publication 14 September 2012 ORIGINAL ARTICLE Concomitant mitral valve surgery in patients undergoing
European Journal of Cardio-Thoracic Surgery 43 (2013) 1000 1005 doi:10.1093/ejcts/ezs499 Advance Access publication 14 September 2012 ORIGINAL ARTICLE Concomitant mitral valve surgery in patients undergoing